


Abstract
The aim of this study was to use brain SPECT to differentiate vascular parkinsonism (VP) from Parkinson’s disease. Methods: Fourteen VP patients (age range, 59–87 y; mean age, 70 ± 7.5 y), 30 Parkinson’s disease patients (age range, 54–84 y; mean age, 65 ± 8.8 y), and 26 healthy (control) individuals (age range, 50–85 y; mean age, 60 ± 9 y) were examined. A 925-MBq (25 mCi) dose of 99mTc-TRODAT-1 was injected intravenously, and brain SPECT images were acquired 4 h after injection. The ratio of specific to nonspecific striatal 99mTc-TRODAT-1 binding was measured and compared. Results: After a region-of-interest analysis of the images from VP patients, Parkinson’s disease patients, and healthy volunteers was performed to obtain ratios of putamen to occipital and striatal to occipital binding as a measurement of specific binding to the dopamine transporters in these regions of the brain, where dopamine neurons are concentrated, the specific binding in the 14 VP patients was slightly lower than but not statistically different from that of the healthy individuals in both putamen and caudate areas. A significant decrease in uptake of 99mTc-TRODAT-1 in the striatum (P < 0.01) was found in Parkinson’s disease patients. Reduction of the uptake was more pronounced in the contralateral putamen of Parkinson’s disease patients than that of VP patients (P < 0.001). A significant bilateral striatal asymmetry was also observed in Parkinson’s disease patients but not in VP patients (P < 0.01). Conclusion: Our findings clearly show that, for VP patients, 99mTc-TRODAT-1 SPECT is a reliable method to differentiate VP from Parkinson’s disease. Further studies, including those to differentiate Parkinson’s disease from arteriosclerotic parkinsonism and patients with both VP and Parkinson’s disease, are needed to help rule out the possibility of Parkinson’s disease as early as possible.
Vascular parkinsonism (VP) is a term applied to patients with clinical symptoms of lower body parkinsonism, multiple cerebral infarctions in basal ganglia or white matter (or both), exclusion of other degenerative diseases that can induce parkinsonism, no prior administration of drugs that can induce parkinsonism, and no, or insufficient, response to anti-Parkinson’s disease drugs (1–3). Early diagnosis of VP is important because the VP patients’ prognosis and response to treatment are different from those of patients with Parkinson’s disease (4). Until recently, diagnosis of both Parkinson’s disease and VP has been made purely on clinical grounds by most neurologists. However, like Parkinson’s disease, VP may have a wide spectrum of clinical manifestations. According to the results of an autopsy series of 100 patients with a clinical diagnosis of Parkinson’s disease made by neurology experts, only 76% were definitively diagnosed to have Parkinson’s disease, including 3% who also had VP (5). Therefore, differentiation of VP patients from Parkinson’s disease patients on the basis of clinical information is difficult, even for a specialized neurologist. Recently, 18F-dihydroxyphenylalanine (DOPA) PET scanning was thought to be a powerful diagnostic tool to support the impression of Parkinson’s disease; however, the limitations of this examination are that it is expensive and is not readily available for common use in clinical practice (6–8).
TRODAT-1 is a cocaine analog that can bind to the dopamine transporter (DAT) sites at presynaptic neuron membrane and can easily be labeled with 99mTc in most nuclear medicine departments throughout the world (9–11). Recent research from our group showed that 99mTc-TRODAT-1 is useful in the diagnosis of Parkinson’s disease and Machado-Joseph disease (12–14). The goal of this study was to evaluate the feasibility of using 99mTc-TRODAT-1 in the diagnosis of VP and to provide a single, simple, and useful method of differentiating VP from Parkinson’s disease.
MATERIALS AND METHODS
Patients
Fourteen VP patients (age range, 59–87 y; mean age, 70 ± 7.5 y) and 30 Parkinson’s disease patients (age range, 54–84 y; mean age, 65 ± 8.8 y), referred from our Neurology Department, were included in this prospective study. The Parkinson’s disease and VP patients were both matched for age (within 5 y) and disease duration (within 5 y). The inclusion criteria for VP are clinical symptoms of lower body parkinsonism, multiple cerebral infarctions in basal ganglia or white matter (or both), exclusion of other degenerative diseases that can induce parkinsonism, no prior administration of drugs that can induce parkinsonism, and no, or insufficient, response to anti-Parkinson’s disease drugs. Lower body parkinsonism was defined as the presence of at least two of the four cardinal signs: tremor at rest, bradykinesia, rigidity, and loss of postural reflexes and predominant rigid akinesia. Evidence of multiple cerebral infarctions in the basal ganglia or white matter (or both) was assessed using a vascular score based on clinical, historic, and neuroimaging data (small, deep, or territorial infarcts and white matter lesions on MRI, CT, or both) (15–18). Parkinson’s disease was defined as existing with the criteria for possible diagnosis of Parkinson’s disease by Gelb et al. (19), exclusion of other degenerative diseases that can induce parkinsonism, and no prior administration of drugs that can induce parkinsonism. 99mTc-TRODAT-1 brain SPECT and MRI were performed with the informed consent of each patient for both quantitative analyses (imaging registration) and qualitative comparison. Twenty-six age-matched (within 5 y) healthy volunteers (age range, 50–85 y; mean age, 60 ± 9 y) were included as a control group. No significant differences in the ages of these three groups existed (t test, P > 0.10). All Parkinson’s disease patients were off dopamine replacement therapy for at least 12 h before injection. The healthy volunteers were free of any neurologic or psychiatric disease and were not taking drugs known to affect the dopaminergic system. This protocol was approved by the medical ethics committee of this hospital, and all subjects participating in this study gave informed consent.
99mTc-TRODAT-1 Brain SPECT
99mTc-TRODAT-1 was prepared by using kits from the Institute of Nuclear Energy Research of Taiwan. Each subject received a dose of 925 MBq (25 mCi) in a 2-mL volume. Imaging was performed 4 h after intravenous injection of 99mTc-TRODAT-1. SPECT images were obtained using a Siemens MultiSPECT 3 three-head rotating gamma camera (CTI/Siemens, Knoxville, TN) fitted with fanbeam collimators; 120 images were acquired over 360°, with 60 s per rotational step and a 128 × 128 matrix size. Individual images were reconstructed with backprojection using a ramp-Butterworth filter, with cutoff frequency of 0.3 per cm and an order of 10. The data were corrected for the effects of photon attenuation using the first-order Chang’s method with an attenuation coefficient of 0.12, with the attenuation ellipses defined on the summed images of the entire dataset and applied, without modification, to all images individually. No attempt was made to correct for partial-volume effects. The slice thickness and in-plane size was 2.9 mm. Three reconstructed transaxial slices were summed and reoriented in parallel, with the orbitomeatal line with the highest signal in the region of the basal ganglia as the central slice (13,14). All images were reviewed by three nuclear medicine physicians who were unaware of the clinical status of the subjects, and all decisions were confirmed by at least two of the three physicians.
MRI
VP and Parkinson’s disease patients and healthy volunteers were examined using a 0.5-T MRI scanner. T1-weighted axial images (repetition time [TR], 500 ms; echo time [TE], 25 ms) and T2-weighted axial images (TR, 3500 ms; TE, 120 ms) were obtained in the transaxial plane (6-mm slice thickness and 0.6-mm gap). Diagnoses were made separately by three neuroradiologists who were unaware of the clinical status of the subjects.
Data Processing
For analysis of the striatal binding of 99mTc-TRODAT-1, the ratio of specific to nonspecific binding was calculated by summing up three adjacent transverse slices representing the most intense striatal DAT binding. Analyses were performed by investigators who were unaware of the clinical data. A standard region-of-interest template (using a stereotactic shape obtained from an MRI atlas, including the entire striatum and occipital cortex) was placed bilaterally on the acquired images (12–14). Estimates of specific striatal binding were made by subtracting occipital counts from striatal counts. The ratio of specific to nonspecific striatal 99mTc-TRODAT-1 binding was then calculated by dividing the specific striatal uptake by the occipital binding.
Statistics
All data were analyzed using the computer software package JMP 3.0 (SAS Institute Inc., Cary, NC) on a Macintosh computer. Differences between these three groups were examined by ANOVA. Differences in binding ratios of 99mTc-TRODAT-1 in the striatum from the data of the Parkinson’s disease, VP, and healthy (control) individuals were examined by the ANOVA and Wilcoxon rank sum tests. P < 5% was considered to be significant.
RESULTS
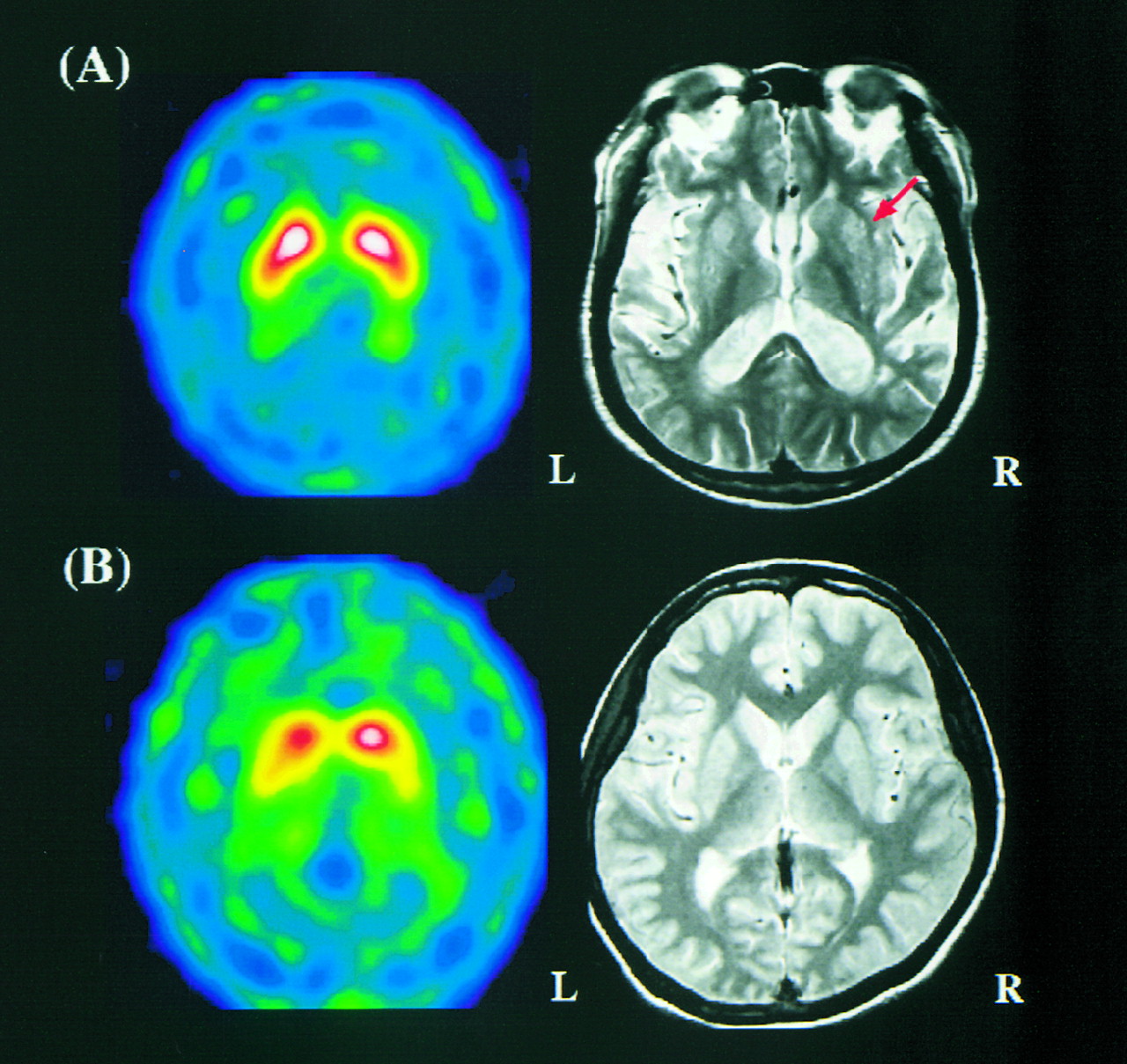
Transaxial images of 99mTc-TRODAT-1 SPECT and MRI in a VP patient and a Parkinson’s disease patient are shown in Figure 1. In the VP patient, the 99mTc-TRODAT-1 uptake in bilateral striata was nearly normal. However, multiple cerebral infarctions in both basal ganglia and white matter were observed on the MR image. In the Parkinson’s disease patient, the MRI findings were normal but the uptake of 99mTc-TRODAT-1 was significantly decreased in the left striatum, with a more noticeable decrease in the left putamen. Figure 2 shows the correlation of 99mTc-TRODAT-1 uptake ratios in the striatum of the VP patients, Parkinson’s disease patients, and healthy volunteers (control group) at different age groups. The ratios of VP patients were decreased slightly, but no significant difference was observed between VP patients and healthy volunteers. An age-related reduction of the ratios was observed in both the control group and the VP patients (P < 0.05), but it was not observed in the Parkinson’s disease patients. In VP patients, the uptake value of 99mTc-TRODAT-1 was not correlated with the severity of the symptoms of lower body parkinsonism or cerebral infarctions in the basal ganglia by the Wilcoxcon rank sum test (P > 0.10). No preferential loss of dopaminergic neurons in either the caudate or the putamen was observed in VP patients. Compared with the clinical symptoms of Parkinson’s disease patients, the uptake value of 99mTc-TRODAT-1 in the striatum not only showed significant asymmetry but also was significantly decreased in the contralateral putamen region (P < 0.001). A significantly decreased uptake of 99mTc-TRODAT-1 was found bilaterally in the striatum in Parkinson’s disease patients compared with that of VP patients (P < 0.05), and the uptake was decreased more appreciably in the contralateral putamen region (P < 0.001) (Fig. 3). The significant differences in these groups were observed with both the Mann-Whitney U test and the ANOVA.
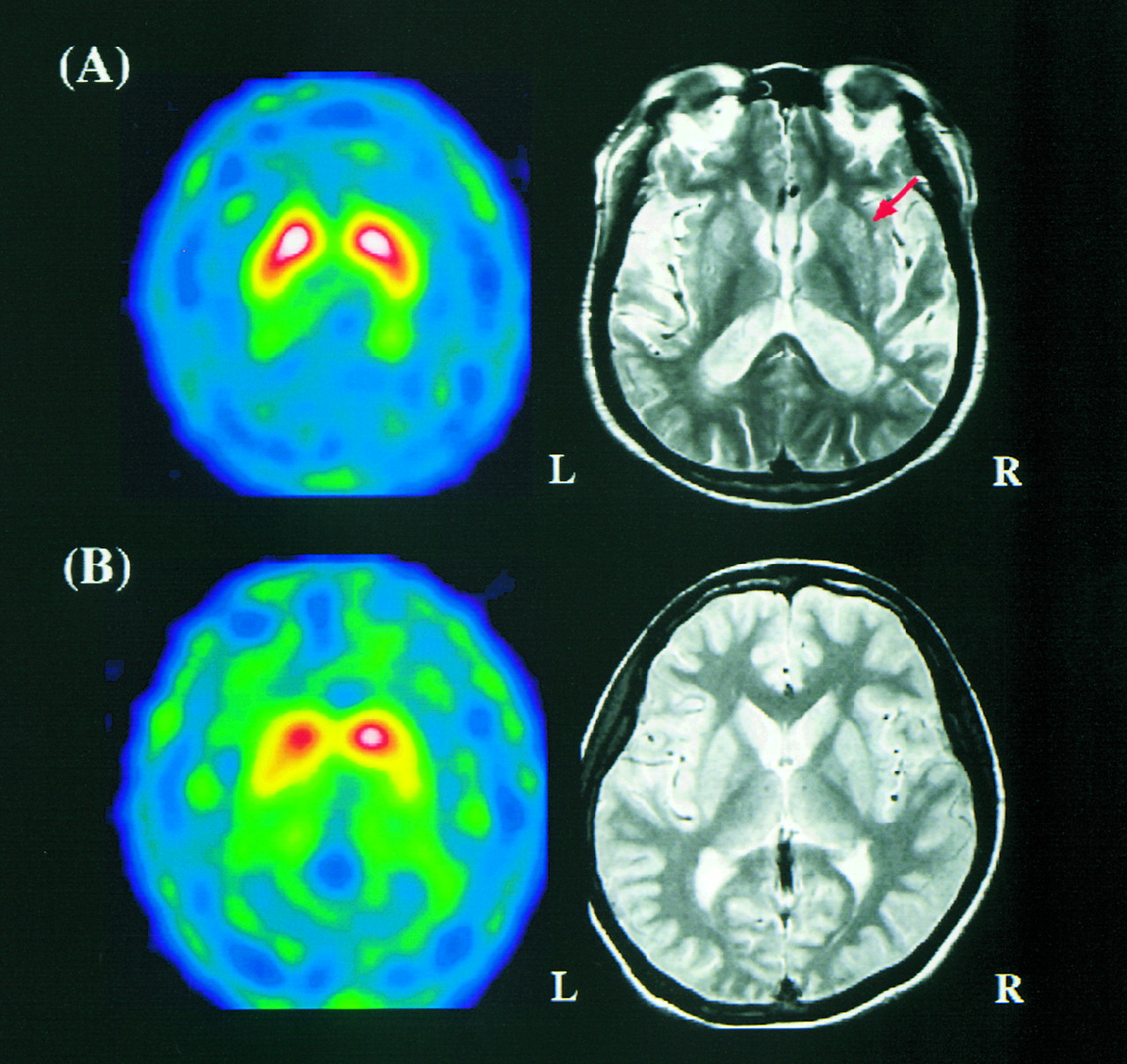
(A) 99mTc-TRODAT-1 brain SPECT and MR images of 62-y-old male VP patient. Symmetric and normal uptake of 99mTc-TRODAT-1 in bilateral basal ganglia is observed (L = left image). Multiple small infarcts are seen bilaterally in basal ganglia and white matter (arrow) on MR image (R = right image). (B) 99mTc-TRODAT-1 brain SPECT and MR images of 62-y-old male Parkinson’s disease patient. Asymmetric and low uptake of 9mTc-TRODAT-1 in right putamen is observed (L = left image). No obvious abnormality is seen bilaterally in basal ganglia and white matter on MR image (R = right image).
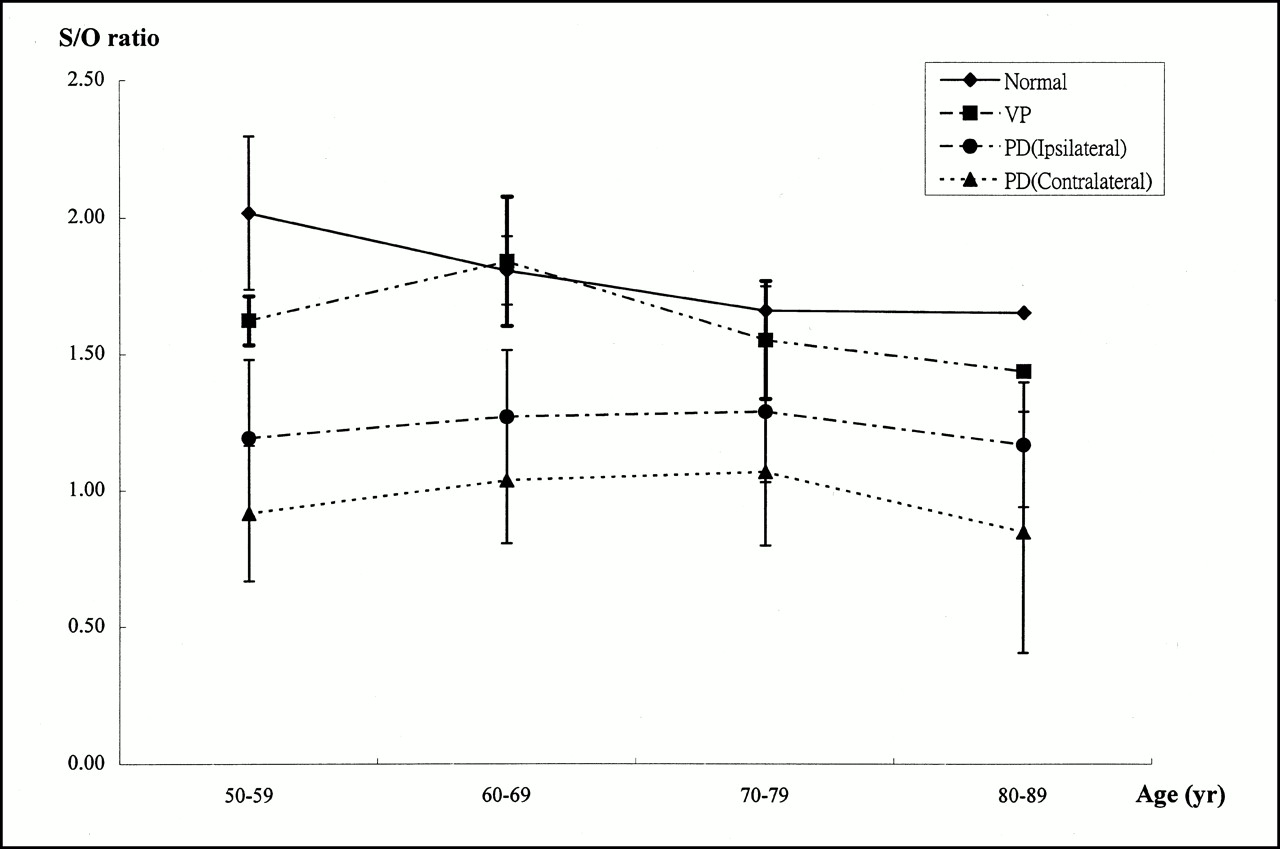
99mTc-TRODAT-1 uptake ratios in striatum in age-matched healthy (normal) individuals, VP patients, and Parkinson’s disease (PD) patients. Age-related decline of 99mTc-TRODAT-1 uptake ratios in striatum was observed in healthy individuals and in VP patients. In comparison with VP and Parkinson’s disease patients, 99mTc-TRODAT-1 uptake ratio in striatum is asymmetric and significantly decreased bilaterally in Parkinson’s disease patients. S/O ratio = striatum-to-occipital ratio.

Putamen-to-caudate uptake ratio (P/C ratio) for 99mTc-TRODAT-1 in age-matched VP and Parkinson’s disease (PD) patients. 99mTc-TRODAT-1 uptake in Parkinson’s disease patients is significantly decreased compared with that in VP patients, with uptake in contralateral putamen site more obviously decreased in Parkinson’s disease patients.
DISCUSSION
For many years, most neurologists believed VP to be lower body parkinsonism associated with multiple small infarcts in the bilateral basal ganglia or white matter (or both) with no, or poor, response to anti-Parkinson’s disease drugs. However, because of the similar symptomatology in parkinsonism patients, VP can be the result of a variety of causes. The lack of the validity of these definitions from the supporting data of clinicopathologic studies prevents a clear diagnosis, whereas the clinical characteristics and the pathologic lesions of VP remain uncertain (16–18,20,21). Differentiation of VP from Parkinson’s disease is important because of the different pathogenesis, prognosis, and responses to treatment (4). To the best of our knowledge, there is no single, useful, and convenient tool to differentiate these two diseases.
Recently, neuroimaging modalities, including CT and MRI, have provided support for the concept of arteriosclerosis-induced parkinsonism (22–28). Imaging studies showed that VP patients had more subcortical white or gray matter lesions (SCLs) than did patients with Parkinson’s disease (27). Although the location and number of infarcts did not correlate well with the clinical presentation of VP, lacunar infarcts in the basal ganglia seemed to be commonly associated with VP (28). However, because the abnormalities of SCLs on CT and MRI are observed frequently in elderly hypertensive patients, these changes are often nonspecific. Therefore, the significance of SCL abnormalities observed on CT and MRI remains controversial, and there is no consensus on the diagnostic usefulness of these imaging results (29,30).
It is well established that 18F-DOPA is a PET tracer for imaging the in situ synthesis of dopamine. As such, it is useful for measuring in vivo production of the neurotransmitter dopamine in the presynaptic neuronal sites. However, use of 18F-DOPA as a routine clinical tool for detecting the integrity of dopamine neurons has several disadvantages. The in vivo metabolism of F-DOPA is quite complicated, which requires the analysis of metabolites in arterial blood samples. Some of the peripheral metabolites may cross the blood–brain barrier, thus contributing to the background and uncertainty of PET imaging. The kinetics of brain uptake and retention of F-DOPA in the brain are relatively complex and, therefore, require extensive kinetic modeling studies. Because of its high cost and lack of availability in most nuclear medicine departments, use of this examination in daily, clinical practice is limited (6–8).
The clinical symptoms of Parkinson’s disease and VP may be similar, but the pathogenesis of these two diseases is quite different. Parkinson’s disease is one of the neurodegenerative disorders that affect the dopaminergic pathway. The most severely affected region in Parkinson’s disease is the putamen (31,32). In VP, chronic subcortical ischemia was observed secondary to hypertensive vascular disease, with partial preservation of the neurons in both the striatum and the deep white matter (33). Theoretically, the dopamine neurons have degenerated in the substantia nigra in Parkinson’s disease, but the dopamine neurons are nearly normal in VP. It is generally believed that DATs play an important role in controlling presynaptic dopamine function, including dopamine storage (34). It belongs to a family of the Na+/Cl−-coupled neurotransmitter transporters, is exclusively found in dopamine neurons, and appears to be a protein reflecting the dopamine neuronal function (35–38). In this study, we used 99mTc-TRODAT-1 to evaluate dopamine neuron density in these two disease states. Our study showed that in VP patients, the uptake of 99mTc-TRODAT-1 was bilaterally symmetric in the striatum. Age-related reduction in uptake was observed, and it was decreased slightly compared with that of the control group. No preferentially decreased uptake of 99mTc-TRODAT-1 in the putamen in VP patients was observed. In addition, the uptake of 99mTc-TRODAT-1 in VP patients was not correlated with the severity of parkinsonism or the extent of lesions of cerebral infarcts in the basal ganglia. Our results are compatible with those of the 2β-carboxymethoxy-3β-(4-[123I]iodophenyl)tropane (123I-β-CIT) studies on VP reported by Hamano et al. (39) and Bencsits et al. (40). However, 123I-β-CIT was not widely available for daily use in a general nuclear medicine department and it also requires a prolonged waiting period (>15 h) after injection before SPECT imaging (39,40). Our results are consistent with the pathologic findings in VP patients that chronic subcortical ischemia was induced by the total extent of lesions in the basal ganglia, caused by multiple infarctions or hemorrhage, but not that the damage to dopamine neurons in the substantia nigra contributed to the core symptoms in VP. Rather, in VP, the dopamine neurons in the substantia nigra were preserved (33). These findings are also compatible with the clinical observations of Thompson and Marsden (23) that the severity of lower body parkinsonism was correlated with the severity of chronic subcortical ischemia. In this study, the uptake value of 99mTc-TRODAT-1 in the striatum in Parkinson’s disease patients showed significant asymmetry and also was preferentially decreased in the contralateral putamen region. After comparison with the Unified Parkinson’s Disease Rating Scale and Hoehn and Yahr scores in Parkinson’s disease patients, the decreased uptake of 99mTc-TRODAT-1 in the striatum was correlated with the severity of symptoms. These findings are compatible with the pathologic findings that the striatum was most sensitive to dopamine neuronal damage in Parkinson’s disease, especially in the putamen, which is the most severely affected region. In comparison with Parkinson’s disease, our studies also clearly showed that the uptake ratios of 99mTc-TRODAT-1 in VP were significantly higher in the contralateral striatum and more obviously decreased in the contralateral putamen site.
CONCLUSION
Because of the different pathogenesis of VP and Parkinson’s disease, which affects the DAT on the dopamine neurons in different ways, imaging DATs provides a powerful procedure to examine the different alterations that change the dopamine neuronal functions. Our data show that the specific uptake ratios of 99mTc-TRODAT-1 in the striatum can be an effective indicator to discriminate between these two apparently similar parkinsonian diseases. The 99mTc-TRODAT-1 SPECT study has several attributes. It is based on using simple 99mTc kits, which are readily available and are as reliable as those used currently in nuclear medicine clinics. 99mTc imaging agents will likely provide a tool that is as readily assessable as that of the conventional brain scan based on regional cerebral blood flow images. Although the number of VP patients studied (n = 14) was insufficient to make a final conclusive appraisal of selectivity and sensitivity of this procedure, the data clearly show the feasibility of using this simple imaging technique to discriminate between VP and Parkinson’s disease. Further studies may be needed to examine the possible coexistence of VP and Parkinson’s disease as well as the specificity and reliability of using this imaging procedure in various VP-related parkinsonian patients who show similar clinical manifestations.
Acknowledgments
We thank Shiann-Rong Lieu and Tsu-Min Tsai for assistance with data assembly and radiopharmaceutical preparation. The work on healthy volunteers and Parkinson’s disease was supported by the National Science Council of Taiwan (grants NSC 89–2314-B-182A-108-M08 and NSC 89-NU-7–182A-003).
Footnotes
Received Jun. 5, 2000; revision accepted Sep. 29, 2000.
For correspondence or reprints contact: Kai-Yuan Tzen, MD, Department of Nuclear Medicine, Chang Gung Memorial Hospital, 199, Tung-Hwa North Road, Taipei, 105 Taiwan.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The role of DAT-SPECT in movement disorders
- Combination of Converging Collimators for High-Sensitivity Brain SPECT
- 123I-FP-CIT SPECT Imaging of Dopamine Transporters in Patients with Cerebrovascular Disease and Clinical Diagnosis of Vascular Parkinsonism
- Sensitivity and Specificity of 99mTc-TRODAT-1 SPECT Imaging in Differentiating Patients with Idiopathic Parkinson's Disease from Healthy Subjects
- 99mTc-TRODAT-1 Imaging of Multiple System Atrophy
- Dopamine Transporter Concentration Is Reduced in Asymptomatic Machado-Joseph Disease Gene Carriers
- Evaluation of Early-Stage Parkinson's Disease with 99mTc-TRODAT-1 Imaging