


Abstract
The timely detection of metastatic infectious foci in gram-positive bacteremia is crucial, because these foci often require prolonged antibiotic treatment or drainage. The diagnosis of metastatic infectious foci is difficult because localizing symptoms are often absent. We investigated whether 18F-FDG PET/CT was able to detect such foci and whether detection influenced clinical outcome. Methods: One hundred fifteen nonneutropenic patients with gram-positive bacteremia were prospectively included. Patients with positive blood cultures growing Staphylococcus aureus, Streptococcus species, or Enterococcus species were eligible when a risk factor for developing metastatic infectious foci was present. 18F-FDG PET/CT was performed within 2 wk after the first positive blood culture. Abnormal 18F-FDG uptake had to be confirmed by radiologic, microbiologic, or pathologic studies. Results were compared with a matched historical control group of 230 patients in whom no 18F-FDG PET/CT was performed. Results: Significantly more patients were diagnosed with metastatic foci in the study group (67.8% vs. 35.7%). Of the imaging investigations performed, 18F-FDG PET/CT was the first to delineate infectious foci in 35 patients (30%). In the remaining 70%, either symptoms on physical examination or other imaging techniques first revealed infectious foci. The sensitivity, specificity, negative predictive value, and positive predictive value of 18F-FDG PET/CT were 100%, 87%, 100%, and 89%, respectively. Relapse rates decreased from 7.4% to 2.6% among study patients (P = 0.09) and from 8.9% to 1.4% in patients with S. aureus (P = 0.04). Overall mortality after 6 mo decreased from 32.2% to 19.1% in the 18F-FDG PET/CT group (P = 0.014). Conclusion: In the diagnostic work-up of high-risk patients with gram-positive bacteremia, 18F-FDG PET/CT is a valuable technique that results in lower mortality rates. In patients with S. aureus bacteremia, relapse rates decreased significantly after the addition of 18F-FDG PET/CT.
The timely detection of metastatic infectious foci in gram-positive bacteremia is crucial, because these foci require prolonged antibiotic treatment and, in some cases, drainage. Insufficiently eradicated infectious foci result in relapse of infection after cessation of antibiotic treatment in 12%–16% of patients (1,2). Mortality rates are significantly higher in patients with metastatic complications or relapse (3,4). The diagnosis of complicating infectious foci is often difficult because up to 32% of these foci do not have any localizing symptoms and signs (5,6). To date, no guidelines addressing the diagnostic work-up of patients with gram-positive bacteremia are available, except for the advice to perform echocardiography in patients with Staphylococcus aureus bacteremia (7).
A sensitive imaging technique suitable for screening of complicating infectious foci might be helpful in identifying patients in need of prolonged antibiotic treatment. CT, MRI, and ultrasonography are less suitable as screening methods when clues for specific sites of infection are absent (8,9). 18F-FDG accumulates in metabolically active cells, including activated leukocytes at the site of infection, enabling imaging of inflammatory processes (10). Therefore, whole-body 18F-FDG PET/CT is potentially useful in delineating metastatic infectious foci. In a retrospective study in a selected patient population with bacteremia, 18F-FDG PET/CT diagnosed, with a high negative predictive value, clinically relevant new infectious complications in 45% of patients (11). To date, there are limited data on infection imaging by 18F-FDG PET/CT in deeply neutropenic patients. The present prospective study investigated whether 18F-FDG PET/CT enabled the early and accurate diagnosis of metastatic infectious complications in patients with gram-positive bacteremia and risk factors for complicating infectious foci and whether the detection of metastatic foci influenced clinical outcome by enabling early and more accurate diagnosis of those foci.
MATERIALS AND METHODS
Study Design and Patients
From November 2005 to January 2008, patients were prospectively recruited from the Radboud University Nijmegen Medical Centre, a 950-bed university hospital. All nonneutropenic (neutrophil count ≥ 0.5 × 109) adult patients (age, ≥18 y) were eligible when at least 1 of the following known risk factors for the presence of complicating infectious foci was present: community acquisition, signs of infection more than 48 h before initiation of appropriate treatment, fever more than 72 h after initiation of appropriate treatment, and positive blood cultures more than 48 h after initiation of appropriate treatment (3,5,12). Patients primarily admitted to the intensive care unit were included only when transferred to regular patient wards within 14 d after the first positive blood culture. Exclusion criteria were polymicrobial infection and pregnancy. The records of all patients with positive blood cultures growing S. aureus, Streptococcus species (excluding S. pneumoniae), or Enterococcus species were reviewed for eligibility as soon as blood culture results were available. The protocol was approved by the institutional review board. Written informed consent was obtained from all patients. The study has been registered in the ISRCTN database (no. 76425553).
A historical control group was defined using the electronic database of the Department of Microbiology, in which all culture results of clinical specimens are available. A pool of 456 patients diagnosed with gram-positive bacteremia between January 2000 and December 2004 in whom 18F-FDG PET/CT was not performed was identified. Patients having at least 1 of the known risk factors for developing complicating infectious foci were eligible for inclusion in the control group. For every prospectively included patient, 2 control patients were matched for the type of microorganism, site of acquisition of the infection, and the presence or absence of additional risk factors (treatment delay, persistent fever, or both). Because blood cultures had not been obtained in a standardized way in the retrospective cohort, the presence of persistently positive blood cultures more than 48 h after the initiation of treatment was not included as a risk factor in the matching strategy.
Clinical Features
The portal of entry was defined as a localized site of infection preceding bacteremia. A central venous catheter was considered a portal of entry if there was evidence of inflammation at the insertion site or if culture of the catheter tip grew the same microorganism as the blood culture in the absence of evidence for another source of infection. Respiratory or urinary tract infections were diagnosed as portals of entry only when specific symptoms and signs were present in addition to positive culture results. Phlebitis due to peripheral intravascular catheters and cellulitis, categorized as skin infections, were considered portals of entry.
Bacteremia was considered to be nosocomial if only blood cultures taken after more than 48 h of hospitalization were positive and clinical signs of the infection were absent at the time of admission. All other infections were considered community-acquired. Both infectious foci without anatomic relation to the portal of entry and direct extension of the infection beyond the primary focus of infection were defined as complicating infectious foci. Endocarditis was defined according to the Duke criteria (7).
Metastatic infectious foci not diagnosed during the first period of infection, or a second period of bacteremia with the same microorganism—either occurring within 3 mo of the first positive blood culture—was defined as relapse of infection. Patients were considered cured if no symptoms or signs of infection were present at 3 mo after the discontinuation of antibiotic treatment. Infection was considered contributory to death using the criteria described elsewhere (12,13). The outcome was assessed in a masked fashion, independent of the predicting variables and imaging results.
Diagnostic Work-up
18F-FDG PET/CT was performed as soon as possible after inclusion. The maximum time between the first positive blood culture and 18F-FDG PET/CT was 2 wk. Because antibiotic treatment can be stopped after 2 wk in uncomplicated bacteremia, the decision to prolong treatment because of infectious complications should be made within those 14 d.
An integrated PET/CT scanner (Biograph; Siemens) was used for data acquisition. Before 18F-FDG injection, patients fasted, and glucose or insulin-containing intravenous infusions were discontinued for at least 6 h. In all diabetic patients at the time of 18F-FDG injection, glucose was below 12.0 mmol/L. One hour after intravenous injection of 200–220 MBq of 18F-FDG (Covidien), a low-dose CT scan, without contrast enhancement, of the area between the proximal femora and base of the skull was acquired for anatomic correlation and attenuation correction of the PET data. Subsequently, emission images of the same area were acquired. 18F-FDG PET/CT images were evaluated by physicians without knowledge of prior clinical evaluation and imaging results. When 18F-FDG uptake was abnormal, conventional radiologic, microbiologic, or pathologic studies were performed when possible, to confirm the diagnosis. All confirmed infectious foci were reported to the attending physician.
Except for 18F-FDG PET/CT and the diagnostic procedures needed for confirmation of abnormal 18F-FDG PET/CT results, standard diagnostic and therapeutic procedures were followed. Conventional radiologic techniques before 18F-FDG PET/CT were performed only at the discretion of the attending physician. Transthoracic echocardiography, followed by transesophageal echocardiography, was to be performed in all patients. In the study group, additional blood cultures were taken at 24, 48, and 72 h after the first positive blood culture and 48 h thereafter when subsequent blood cultures were positive. C-reactive protein and leukocyte counts were ordered twice weekly. 18F-FDG PET/CT results were considered abnormal if focal accumulation of 18F-FDG was detected. Results were considered to be true-positive when abnormal 18F-FDG uptake pointed to the organ or tissue in which infection was eventually diagnosed. Abnormal results were categorized as false-positive when the abnormality could not be confirmed. Normal test results were true-negative when no complicating infectious foci were diagnosed within 2 wk after 18F-FDG PET/CT. Abnormal test results not related to metastatic infection that were caused by a confirmed alternative diagnosis (i.e., cancer) were also considered true-negative. Antibiotic treatment was not influenced by these foci. Normal test results were considered false-negative when a localized infectious focus was diagnosed. Because of the high physiologic 18F-FDG uptake within the brain, heart, and kidneys, 18F-FDG PET/CT was unsuitable for the detection of infectious foci and was not evaluated for metastatic foci in these organs. Within the study period (2000–2008), the diagnostic work-up or treatment of patients with gram-positive bacteremia remained unchanged in our hospital. If no complicating infectious foci were detected, the standard duration of treatment was 14 d. Treatment was prolonged to 6–12 wk in patients with complicating infectious foci, depending on the site of infection and clinical response according to clinical practice. Endocarditis was treated according to international guidelines (14).
Diagnosis and Patient Follow-up
The final diagnosis served as a standard of reference and was based on microbiologic and pathologic results. If these results were not available, the probable final diagnosis was based on conventional radiologic procedures and clinical follow-up. The final diagnosis was never based on the results of the 18F-FDG PET/CT scan alone. Patient follow-up was performed for 6 mo after the first positive blood culture. Epidemiologic data, number, type, and results of all diagnostic tests and treatment data were registered in a structured database (Access; Microsoft). Mortality data were obtained for all patients at 3 and 6 mo after diagnosis.
Outcome Parameters
The primary outcome parameter was relapse of infection. Secondary outcome measures were overall and attributable mortality after 3 and 6 mo, duration of antibiotic treatment, and number of diagnostic procedures performed to confirm 18F-FDG PET/CT results.
Statistical Analysis
The study was designed to detect a statistically significant difference of 10% between the study group and a historic control group (α, 0.05; power, 0.80; 2-group χ2 test, 2-sided). This design required 115 evaluable study patients and 230 patients in the historic control group. An intention-to-treat analysis was performed. Differences between groups were tested with Fisher exact tests for categoric variables. Differences were considered to be statistically significant at a P value less than 0.05 (2-sided). Cox proportional hazard models were used to analyze the relationship between durations (survival, duration of therapy) and exploratory variables after adjustment for potential confounding variables. When no statistically significant confounding variables were detected, Kaplan–Meier curves were estimated. We used SPSS (version 16.0; SPSS, Inc.) for the analyses.
RESULTS
One hundred fifteen study patients and 230 control patients were included in the study (Fig. 1). For 102 of 115 (89%) study patients, 2 perfectly matching controls were found (Table 1). The remaining 13 study patients were always matched with control patients with the same type of microorganism. Overall, the control patients had fewer additional risk factors than did the study patients (89% vs. 80%, P < 0.05). Treatment delay was added as a covariate (confounder) in the final analysis but was insignificant in all Cox proportional hazards models; therefore, Kaplan–Meier analyses were performed. The identification of the portal of entry of infection was similar for study and control patients.

Enrollment of prospectively included study patients and historical control patients from database of Department of Medical Microbiology. False-positive 18F-FDG PET/CT scan results were found in 7 patients. Localized colonic uptake, followed by normal colonoscopy results, was seen in 2 patients. In 1 patient, shoulder uptake was not accompanied by hydrops on ultrasound, but no puncture was performed. Confirmed mediastinal lymphadenopathy on CT was seen in 1 patient, but no further diagnostic tests were performed. Lymphadenopathy had disappeared after 6 mo of follow-up. Pleural uptake without pleural effusion on chest radiography was seen in 1 patient. She died before further investigations could be performed. In 1 patient, uptake in psoas was thought to be due to recent bleeding seen on CT. No cultures were taken in this patient, and she was treated for 6 mo because of infected knee prosthesis. Abnormalities on CT disappeared. In 1 patient, 18F-FDG uptake was present at site of pacemaker lead. He refused transesophageal echocardiography and was treated for 6 wk until presumed infected kidney stone was removed. Infection did not recur.
Baseline Characteristics of Study Patients and Historical Controls
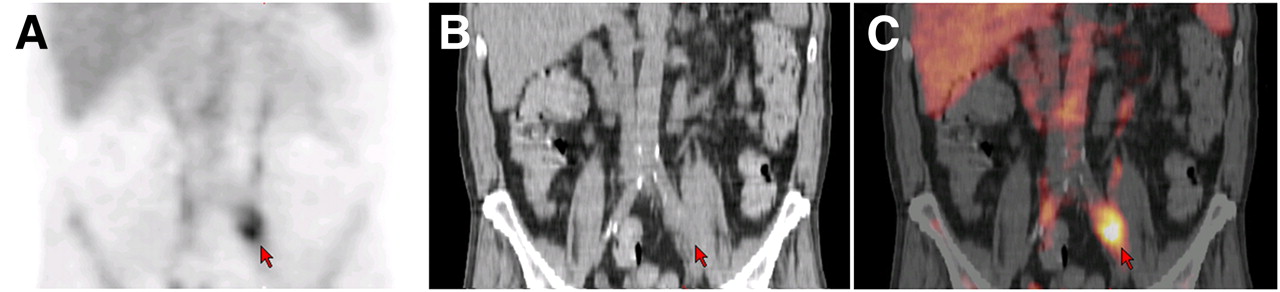
18F-FDG PET/CT was performed in 111 of 115 study patients at a median of 7 d (mean, 6.8 d) after the first blood culture became positive. Significantly more metastatic foci were identified in study patients than in control patients: 67.8% versus 35.7% (P < 0.05, Table 2). Compared with 27% of the controls, almost 40% of the study patients with metastatic foci had more than 1 localization. More than half of the patients with endocarditis in both groups also had another metastatic localization. Figure 2 shows an example of a CT-confirmed mycotic aneurysm that was asymptomatic. In 50% of all patients eventually diagnosed with metastatic infection, no signs and symptoms suggesting metastatic complications were present before 18F-FDG PET/CT was performed. Of the imaging investigations performed, 18F-FDG PET/CT was the first to delineate 44 of all 124 (35%) metastatic infectious foci in 35 patients (30% of all patients; in the remaining 70%, either symptoms on physical examination or other imaging techniques first revealed infectious foci). In 26 of these 35 patients, the metastatic foci were not associated with clinical signs guiding the attending physician. Nevertheless, in 7 of those patients, prior investigations were performed (5 ultrasounds, 1 CT scan, and 1 MRI). In 5 of the 9 remaining patients who did have guiding symptoms, prior diagnostic procedures (4 CT scans and 1 MRI scan) had not revealed the focus of infection. In the remaining 4 patients with guiding symptoms, conventional diagnostic procedures were delayed because of logistic reasons in 2 patients and symptoms had not led to ordering additional imaging in the remaining 2 patients. To confirm 18F-FDG PET/CT findings, 24 ultrasounds, 16 CT scans, and 7 MRI scans were obtained. Echocardiography was performed significantly more often in the study group (83% vs. 29%, P = 0.001). The difference in patients with metastatic foci between both groups remains significant (P < 0.001) when patients with endocarditis alone are excluded from the analysis. For delineating metastatic infectious foci, 18F-FDG PET/CT had a sensitivity of 100%, specificity of 87%, negative predictive value of 100%, and positive predictive value of 89%. Information regarding the 7 patients with false-positive 18F-FDG PET/CT results is shown in Figure 1.
Localization of Metastatic Foci and Number of Foci First Detected by 18F-FDG PET/CT

18F-FDG PET/CT of patient with community-acquired S. aureus bacteremia and proven endocarditis, presenting with fever, heart failure, and new cardiac murmur (aortic valve insufficiency). 18F-FDG PET/CT detected accumulation in left common iliac artery (arrow) due to clinically silent mycotic aneurysm. This finding resulted in prolonged treatment with antibiotics and monitoring of aneurysm size. Coronal sections are shown for 18F-FDG PET (A), CT (B), and integrated 18F-FDG PET/CT (C).
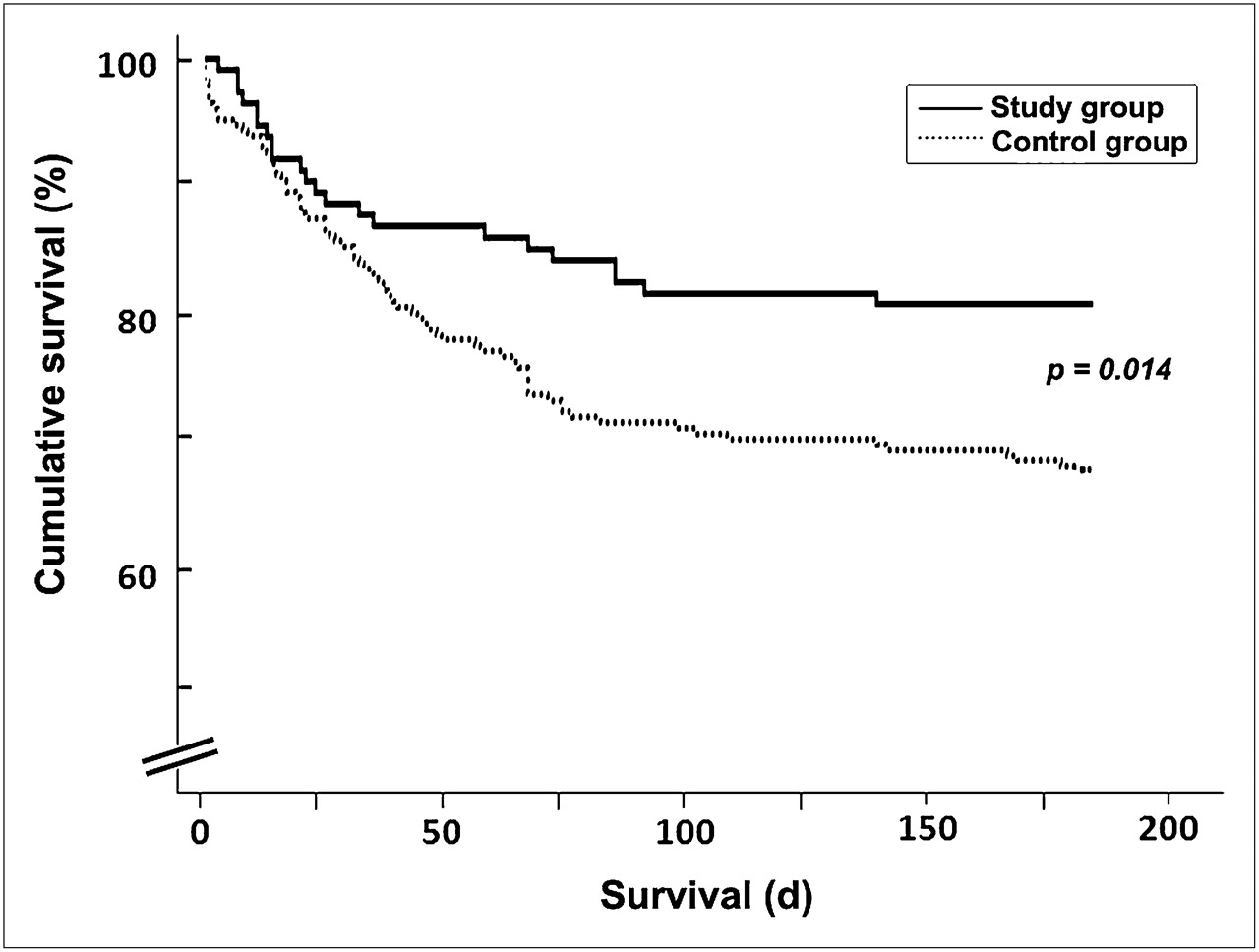
The relapse rate was 7.4% in controls and 2.6% in the study group (Table 3). In the S. aureus subgroup, however, significantly fewer study patients had a relapse of infection than controls (P = 0.04). Overall mortality rate was 16.6% in the study group at 3 mo of follow-up and 25.7% in the control group (P = 0.06). Eight patients had died after relapse of infection in the control group versus 2 study patients. The difference in overall mortality rate remained significant during 6 mo of follow-up (19.1% in the study group vs. 32.2% in the control group, P = 0.014) in the Kaplan–Meier models (Fig. 3). Infection contributed to death in 80% of study patients and 74% of controls (P = 0.7). After 6 mo of follow-up, infection-related mortality decreased from 24.3% in controls to 14.8% in study patients (P = 0.049). In all but 2 patients in each group, 6-mo follow-up data were available. In the study group, the median duration of treatment was longer. The median duration of treatment of patients without metastatic foci of infection was 14 d in both groups (Fig. 4). When metastatic infectious foci were present, study patients and controls were treated significantly longer in both groups (median, 45 and 36 d, respectively). In the study group, 73 of 78 patients with metastatic foci were treated for more than 14 d. After the diagnosis of infectious complications, percutaneous or surgical drainage was performed in 30 of these patients. Another 6 patients underwent cardiac valve replacement. In 5 patients, treatment was not prolonged. Three of those patients died. Six of the study patients were still being treated at the end of follow-up.
Clinical Endpoints at 3- and 6-Month Follow-up
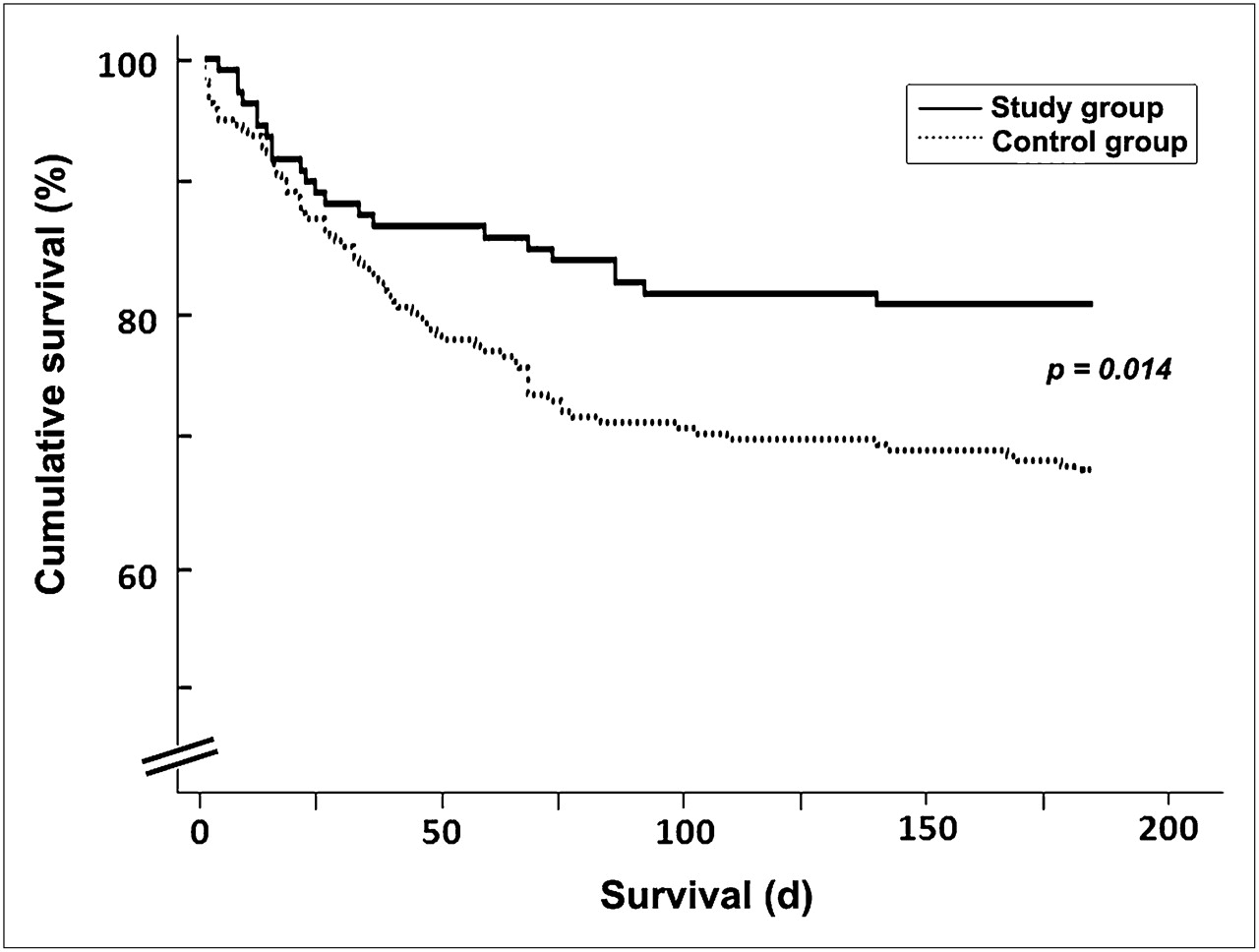
Kaplan–Meier curve for survival at 6-mo follow-up in study and control groups.

Kaplan–Meier curves for duration of treatment. (A) Duration of treatment between study and control groups when metastatic foci were present. (B) Duration of treatment between study and control group when metastatic foci were absent.
DISCUSSION
This prospective study with matched historical controls showed that relapse rate and mortality decreased when 18F-FDG PET/CT was performed in patients with gram-positive bacteremia and at least 1 risk factor for developing complicating infectious foci. Metastatic foci were found in a larger proportion of study patients than in control patients (P < 0.001) using 18F-FDG PET/CT. In previous studies investigating gram-positive bacteremia, the reported incidence of complicating foci varies between 16% and 35%, which is comparable to the percentage of complicating foci in the control group (36%) (1,3,12,15). The percentage of complicating infectious foci delineated in the 18F-FDG PET/CT group, however, is much higher: 68%. In 35 patients (30% of all patients), metastatic infectious foci were first revealed by 18F-FDG PET/CT, despite the fact that 18F-FDG PET/CT was considered experimental. Priority was given to other clinically indicated diagnostic procedures, and 18F-FDG PET/CT was sometimes postponed, as long as the 14-d time limit was not reached. The fact that 18F-FDG PET/CT delineated significantly more endovascular, pulmonary, and spinal infections in the study group than in the controls, in whom no 18F-FDG PET/CT was performed, is not surprising because these infections often lack localizing symptoms. These sites of infection, however, should not be missed because treatment should be prolonged, and surgical intervention is indicated in a proportion of these patients. Remarkably, the duration of treatment in 6 of the 22 patients with endocarditis was dictated by a second complicating infectious focus requiring prolongation of antibiotic treatment. As expected, endocarditis was not detected by 18F-FDG PET/CT because of physiologic uptake in the myocardium (16). In line with international guidelines, echocardiography was strongly advocated in our protocol, as it was in clinical practice in previous years (7,14). Nevertheless, echocardiography was performed significantly more often in the study group, resulting in a more frequent diagnosis of endocarditis. However, when patients with endocarditis alone were excluded, metastatic foci were still found significantly more often in the study group. These findings indicate that the higher incidence of patients with metastatic infections in the study group was not caused by the increased use of echocardiography, because significantly more metastatic infections at other anatomic sites were also diagnosed.
The early detection of metastatic infectious foci facilitated the adaptation of treatment in patients at high risk of relapse. In the study group, the overall relapse rate was only 2.6%. This did not differ significantly from the 7.4% among controls. The study was designed to detect a 10% decrease in relapse rate. In the subgroup with S. aureus bacteremia, however, a significant improvement in relapse rate from 8.9% to 1.4% was found. Compared with other rates given in the literature, our historic relapse rate in S. aureus bacteremia is low (8.9 vs. 12%–16%), possibly because of the low number of methicillin-resistant S. aureus infections (<2%) and concomitant vancomycin use in our study (17). It was hypothesized that early mortality due to sepsis could not be prevented by the early detection of metastatic infection; thus, total mortality was regarded as only a secondary outcome parameter. However, overall and infection-related mortality proved to be significantly lower in the study group after follow-up of 6 mo.
A limitation of our study is the use of a historical control group. However, the control group was both large and matched for the risk profile for developing metastatic infectious complications (3,5,12,18,19). Furthermore, the study patients had more additional risk factors than the control patients, taking into account the larger number of persisting positive blood cultures. Thus, the overall risk for relapse of infection should have been higher in the study group. Because treatment delay might have been an important confounder—being significantly more prevalent among control patients—it was added as a covariate in the final analysis. But adding treatment delay as a covariate did not influence the outcome on survival at 6 mo of follow-up. Because protocols for diagnostic evaluation and treatment did not change within the period 2000–2008, there were no differences in the management of patients with gram-positive infections. The median duration of treatment was significantly longer in the presence of metastatic infectious foci, with a difference between study and control patients. This difference was probably due to the greater number of endovascular infections (17% vs. 4%)—which require prolonged antibiotic treatment—that were found in the study group. As stated, most of these infections were delineated first by 18F-FDG PET/CT because of the lack of guiding symptoms. Therefore, it is highly likely that the difference in the number of metastatic foci and the reduced relapse rate and mortality rates can be attributed to the addition of 18F-FDG PET/CT to the diagnostic regimen.
CONCLUSION
18F-FDG PET/CT detected clinically relevant new complicating infectious foci in 30% of all study patients, with a high negative predictive value. The addition of 18F-FDG PET/CT to the diagnostic work-up led to a decrease of relapse rates and overall and infection-related mortality of gram-positive bacteremia by early detection and treatment of metastatic infectious foci. 18F-FDG PET/CT is thus a valuable technique in the diagnostic work-up of all patients with gram-positive bacteremia and at least 1 risk factor for developing metastatic complications.
Acknowledgments
This study was supported in part by a grant from the Netherlands Organization for Health Research and Development (ZonMw). The funding source had no influence on study design, data collection, analysis, interpretation of data, and writing of the report or in the decision to submit the paper. All authors had full access to the data and held the final responsibility for the decision to submit the report for publication.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication November 3, 2009.
- Accepted for publication April 28, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Importance of Blood Glucose Management Before 18F-FDG PET/CT in 322 Patients with Bacteremia of Unknown Origin
- Sterile endogenous panophthalmitis with uncontrolled diabetes
- 18F-FDG PET/CT-Guided Treatment Duration in Patients with High-Risk Staphylococcus Aureus Bacteremia: A Proof of Principle
- The Value of 18F-FDG PET/CT in Diagnosis and During Follow-up in 273 Patients with Chronic Q Fever
- 18F-FDG PET/CT Optimizes Treatment in Staphylococcus Aureus Bacteremia and Is Associated with Reduced Mortality
- Characterization of 18F-Fluorodeoxyglucose Uptake Pattern in Noninfected Prosthetic Heart Valves
- Clinical Usefulness of 18F-FDG PET/CT for the Detection of Infections of Unknown Origin in Patients Undergoing Maintenance Hemodialysis
- 18F-FDG PET/CT for the Detection of Septic Embolisms in Patients with Infectious Endocarditis
- Role of 18F-FDG PET in Patients with Infectious Endocarditis
- Imaging of Inflammation by PET, Conventional Scintigraphy, and Other Imaging Techniques
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- Cost-Effectiveness of Routine 18F-FDG PET/CT in High-Risk Patients with Gram-Positive Bacteremia
- Nuclear Medicine Imaging of Infection in Cancer Patients (With Emphasis on FDG-PET)
- Imaging of Inflammation by PET, Conventional Scintigraphy, and Other Imaging Techniques