


Abstract
Patients with end-stage renal disease undergoing maintenance hemodialysis (MHD) are highly prone to infections. The potential clinical usefulness of 18F-FDG PET/CT for the detection of infections of unknown origin in this patient population remains unclear. This study was designed to investigate this issue. Methods: Between October 2011 and July 2014, a total of 104 adult MHD patients with sepsis underwent 18F-FDG PET/CT for the detection of unknown infection foci. Follow-up was continued until October 2014. Positive 18F-FDG PET/CT findings and mortality served as the main outcome measures. Results: Of the 104 study patients, 73 (70.2%) had positive 18F-FDG PET/CT findings, and a total of 95 major infection foci were identified. Eighteen patients (24.6%) had at least 2 infection foci on 18F-FDG PET/CT scans. Seven (53.8%) of the 13 patients with primary vascular access–related infections had concurrent metastatic foci. Twenty-eight patients (26.9%) had their treatments modified by 18F-FDG PET/CT results. Multivariate logistic regression analysis demonstrated that low hemoglobin and high C-reactive protein levels at diagnosis were the independent predictors of positive 18F-FDG PET/CT results. Twenty-seven patients (26.0%) died during their hospital stay, and 24 of them had positive 18F-FDG PET/CT findings (P = 0.014). Positive 18F-FDG PET/CT results were an independent predictor of mortality (hazard ratio, 3.896; 95% confidence interval, 1.039–14.613; P = 0.044). Conclusion: Our results suggest that 18F-FDG PET/CT may be clinically useful for detecting occult infection foci in end-stage renal disease patients undergoing MHD. In this population, positive 18F-FDG PET/CT findings may lead to a significant change in clinical management and independently predict mortality.
Taiwan has the highest rate of end-stage renal disease (ESRD) in the world (2,584 cases per million persons in 2010) (1). Data from our historical cohort of patients undergoing maintenance hemodialysis (MHD) indicate that infections account for 39.6% of all deaths, being second only to cardiovascular diseases as the most prevalent cause of mortality (52.3%) (2). Although the overall mortality rate is 100- to 300-fold higher and the sepsis-related mortality is 50-fold higher in ESRD patients with sepsis than in the general population, only a few studies have examined the epidemiology, pathogenesis, prevention, and treatment of infections in ESRD patients with MHD (3,4).
There is evidence that 18F-FDG PET/CT may be an accurate and reliable clinical tool for identifying several infectious diseases. Current guidelines suggest that the major indications for 18F-FDG PET/CT in the setting of infectious diseases include osteomyelitis, spinal infections, fever of unknown origin, and metastatic infections (5). Moreover, we have previously demonstrated the clinical utility of 18F-FDG PET/CT imaging in the detection of occult infection foci in patients with sepsis, ultimately inducing major management changes (6). Although loss of renal function is related to impaired functioning of immune defenses and increased susceptibility to infections, the potential clinical usefulness of 18F-FDG PET/CT for the detection of infection foci of unknown origin in ESRD patients undergoing MHD remains unclear (7,8). This study was designed to investigate this issue.
MATERIALS AND METHODS
Patients and Hemodialysis Management
Between October 1, 2011, and July 31, 2014, a total of 104 patients with ESRD undergoing MHD had the initial diagnosis of sepsis of unknown origin on admission to the Chang Gung Memorial Hospital at Linkou. Patients underwent 18F-FDG PET/CT imaging within 2 wk of admission in the presence of one of the following conditions: inability to identify unequivocal infection foci after an extensive evaluation; evidence of bacteremia and high suspicion of metastatic spread of infection; or suspected infection of a vascular access site of uncertain extent. All patients underwent empiric antibiotic treatment even though the focus of infection had not yet been identified. All patients received MHD for 4 h 2 or 3 times per week. Patients underwent MHD using single-use hollow-fiber dialyzers equipped with modified cellulose-based, polyamide or polysulfone membranes. The dialysis solution consisted of a standard ionic composition with bicarbonate-based buffer. All patients were followed up for at least 3 mo after discharge to determine the clinical outcome. This retrospective observational study was approved by the Institutional Review Board of the Chang Gung Memorial Hospital (approval 101-4533B). Informed consent was waived because of the retrospective nature of the study.
PET/CT Acquisition, Processing, and Interpretation
18F-FDG PET/CT was performed using a Biograph mCT PET/CT system (Global Siemens Healthcare) 60 min after intravenous administration of 18F-FDG. The injected dose ranged from 333 to 407 MBq (9–11 mCi). PET was performed with time-of-flight acquisition and 1 min per bed position in a head-to-toe direction. The PET images were reconstructed using the UltraHD method (TrueX + time-of-flight) with 2 iterations, 21 subsets, and a 3-mm gaussian filter. CT data were used for both attenuation correction and fusion with attenuation-corrected PET images. All images (PET, CT, and PET/CT) were displayed in rotating maximum-intensity projections, axial, coronal, and sagittal views. Images were interpreted by a team of 2 nuclear medicine physicians who did not know the patient’s clinical history, blood test results, and previous imaging findings. Positive PET findings were defined as any abnormal uptake higher than the background activity. In consensus with infectious disease physicians, positive PET/CT findings were defined as true-positive if confirmed by clinical data or the complementary imaging workup. In contrast, negative 18F-FDG PET/CT results were considered true-negative in the absence of either localized foci or infection recurrences at follow-up. We did not calculate accuracy because of the lack of an accepted gold standard in ESRD patients undergoing MHD and because of the pilot nature of the study.
Definitions
The general characteristics of the study patients were collected from their medical records. Age was dichotomized using 65 y as the cutoff. The severity of ESRD was staged using the National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative classification (9). Chronic liver disease or liver cirrhosis was diagnosed by an expert gastroenterologist on the basis of histologic findings from liver biopsies, imaging results from abdominal sonography or CT, clinical histories, physical examinations, and blood tests (including hepatitis B and C virus infections). Diabetes mellitus was diagnosed by typical symptoms of hyperglycemia and high plasma glucose levels either at fasting (>126 mg/dL) or after a glucose load (>200 mg/dL) and was subsequently confirmed on a separate occasion (10). All study patients had clinical evidence of the systemic inflammatory response syndrome diagnosed according to the criteria of the American College of Chest Physicians and the Society of Critical Care Medicine (11). Sepsis was defined as clinical evidence of a systemic inflammatory response syndrome accompanied by suspected or definitive evidence of infection (12). Metastatic infections were considered to be present when the entry of the microorganisms from the primary foci into the bloodstream led to the formation of distant abscesses or secondary areas of infection (13–15). In hospitalized patients, the results of all blood cultures were retrieved using the computer-assisted microbiology reporting system of our Clinical Microbiology Laboratory.
Data Analysis
Patients were not analyzed twice even though a follow-up 18F-FDG PET/CT scan was performed for monitoring response to treatment. Descriptive statistics were summarized using frequencies, percentages, means, and SDs. Continuous variables were tested for normal distributions using the Kolmogorov–Smirnov test. We used independent Student t tests and Mann–Whitney U tests to compare normally distributed and skewed continuous variables, respectively. Categoric data were compared using the Pearson χ2 test. We used logistic regression analysis to identify the variables associated with positive PET/CT findings and mortality. All variables with a P value of less than 0.05 in univariate analyses were entered into a forward multivariate logistic regression model. All calculations were performed using the SPSS software (version 16.0; IBM). Two-tailed P values of less than 0.05 were considered statistically significant.
RESULTS
The general characteristics of the study patients are summarized in Table 1. Patients older than 65 y represented 64.4% of study participants. There were no significant differences in age, sex, and MHD characteristics in patients with or without positive 18F-FDG PET/CT findings. However, chronic liver disease was significantly associated with negative 18F-FDG PET/CT findings (P = 0.020). Patients with positive 18F-FDG PET/CT findings had a higher white blood cell count and C-reactive protein (CRP) level (P = 0.016 and <0.001, respectively) but had a lower hemoglobin level (P = 0.011). Moreover, patients with positive scans had a significantly longer hospital stay (56.8 vs. 28.2 d, P < 0.001). Of the 27 patients who died during the admission, 18F-FDG PET/CT results were positive in 24 and negative in 3 (P = 0.014). At the end of follow-up, 40 (38.5%) patients had died.
Baseline Characteristics of ESRD Patients with Infections of Unknown Origin Stratified According to 18F-FDG PET/CT Results
Of the 59 patients (56.7%) with positive blood cultures, 41 (39.4%) had gram-positive bacteremia, 14 (13.5%) had gram-negative bacteremia, 1 (1.0%) had fungemia, and 3 (2.9%) had both gram-positive bacteremia and fungemia. The most common gram-positive pathogen was Staphylococcus aureus, which was isolated from 29 of the 44 patients with gram-positive bacteremia. Of them, 15 (51.7%) had infections caused by methicillin-resistant S. aureus. The most common gram-negative pathogens were Salmonella enterica and Enterobacter cloacae, each of which was isolated in 3 of the 14 patients with gram-negative bacteremia. A total of 95 septic foci were identified on 18F-FDG PET/CT scans (Table 2). Fourteen patients (13.5%) had 2 septic foci and 4 (3.8%) had 3 septic foci identified during a single image acquisition (Figs. 1 and 2). Forty-one patients (39.4%) were diagnosed as having metastatic infections. Of them, 24 (58.5%) had gram-positive bacteremia, which was identified as a significant risk factor for metastatic spread of infection (P = 0.011). In contrast, only 6 (14.6%) of the 41 patients with metastatic infections had gram-negative bacteremia (P = 0.961).
Major Infectious Foci (n = 95) Identified in 73 Patients with Positive 18F-FDG PET/CT Findings

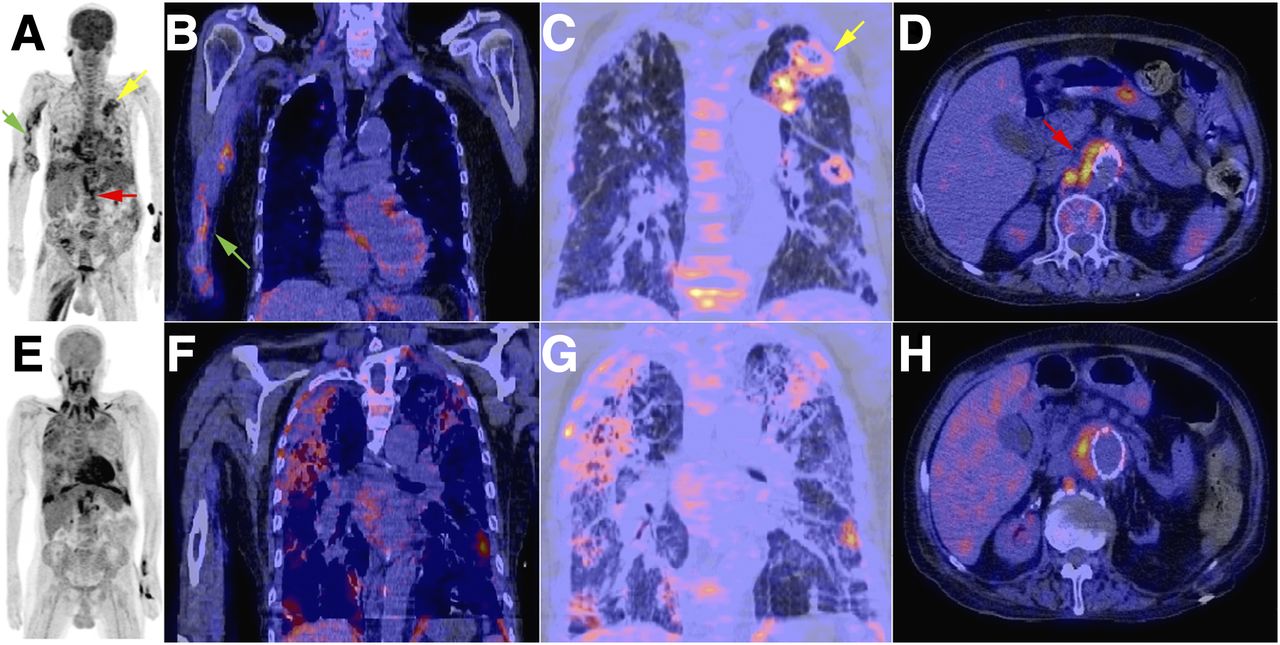
18F-FDG PET/CT images of 75-y-old man who presented with methicillin-resistant S. aureus bacteremia. Shown from left to right are maximum intensity projection of PET, fused PET/CT coronal views, and axial view. (A–D) Imaging revealed right arm arteriovenous graft–related pyomyositis (green arrow) accompanied by septic pulmonary embolism (yellow arrow) and mycotic aneurysm adjacent to vascular graft in abdominal aorta (red arrow). Despite arteriovenous graft removal and local debridement, patient died after 1 mo because of progressive respiratory failure. (F) Right-arm soft-tissue infection subsequently resolved. (E and G) Respiratory distress pattern with increased 18F-FDG uptake in respiratory muscles and marked lung fibrotic changes were noted. (H) Mycotic aneurysm remained stable and showed poor response to antibiotic treatment.

18F-FDG PET/CT images of 57-y-old woman who presented with methicillin-sensitive S. aureus bacteremia. Shown from left to right are maximum intensity projection of PET, fused PET/CT axial view of sternoclavicular joint, and fused PET/CT sagittal view of head. (A–C) Imaging revealed left arm arteriovenous graft–related phlebitis (red arrow) ascending to axillary vein, accompanied by adjacent left sternoclavicular septic arthritis (green arrow). We also identified wedge defect accompanied by increased 18F-FDG uptake in left parietal lobe (particularly beside gyrus, yellow arrow), which was interpreted as presence of brain septic emboli. (D–F) After arteriovenous graft removal and local debridement, follow-up 18F-FDG PET/CT scan after 1 mo revealed resolution of brain emboli despite persistence of left sternoclavicular lesion. Strong liver uptake may reflect presence of increased liver enzymes at time of second scan. Patient subsequently survived.
Of 73 patients with positive 18F-FDG PET/CT findings, 50 (68.4%) were identified as having musculoskeletal system infections. The most common forms included septic arthritis and infective spondylitis, followed by vascular access–related infections, pyomyositis, and appendicular bone osteomyelitis. Among the 13 patients with primary vascular access–related infections, 7 (53.8%) had concurrent metastatic infections, including septic arthritis, infective spondylitis, pyomyositis, and pulmonary and brain septic emboli. Seven patients (9.6%) were diagnosed with intraabdominal and retroperitoneal abscesses, including a liver abscess (4 patients), anal abscess (1), subphrenic abscess (1), and perinephric abscess (1). Only 2 patients were diagnosed as having infective endocarditis.
In total, 28 patients (26.9%) had their treatment modified by 18F-FDG PET/CT findings. Specifically, 15 underwent surgical debridement, 11 had CT-guided or incision drainage, and 2 received arteriovenous graft thrombectomy. Of them, 21 were successfully cured, whereas 7 died. Twenty patients with positive 18F-FDG PET/CT findings had their dialysis catheter removed during their hospital stay as compared with 6 of the 31 patients with negative results.
Univariate and multivariate logistic regression analyses were performed to identify the significant predictors of positive 18F-FDG PET/CT findings and mortality (Tables 3 and 4). As shown in Table 3, univariate analysis identified the presence of chronic liver disease as significantly associated with the likelihood of negative 18F-FDG PET/CT results (P = 0.023). In contrast, decreased hemoglobin levels, increased white blood cell count, and increased CRP levels were significantly associated with the likelihood of positive 18F-FDG PET/CT findings. Multivariate logistic regression analysis demonstrated that low hemoglobin and high CRP levels at diagnosis were the independent predictors of positive 18F-FDG PET/CT results. Old age and positive 18F-FDG PET/CT results were statistically significant predictors of death in both univariate and multivariate analyses (Table 4).
Odds Ratios for Positive 18F-FDG PET/CT Findings According to Univariate and Multivariate Logistic Regression Analyses
Hazard Ratios for Death According to Univariate and Multivariate Logistic Regression Analyses
DISCUSSION
Increased uptake of 18F-FDG at the suspected sites (which is caused mainly by enhanced glycolysis and reflects a high expression of glucose transporters in inflammatory cells) may be used to detect a variety of inflammatory and infectious disorders on PET imaging (16,17). Because ESRD patients undergoing MHD are prone to infections (7,18,19), we hypothesized that 18F-FDG PET/CT may be clinically useful to identify unknown infection foci in this complex patient population.
In the present study, 18F-FDG PET/CT successfully identified infection foci in 73 of 104 ESRD patients (70.2%) with infections of unknown origin. Anemia and high CRP levels were significantly associated with the likelihood of positive 18F-FDG PET/CT findings. Although patients with ESRD are predisposed to infections because of various immune alterations (including defective neutrophil and monocyte functions) (20), their metabolic response does not seem to be altered. Acute inflammation may result in anemia and increased CRP levels (21). Because anemia and CRP levels are known correlates of acute inflammatory reactions, their association with the likelihood of positive 18F-FDG PET/CT findings is not surprising.
Another important finding from this study is that chronic liver disease was identified as a significant predictor of negative 18F-FDG PET/CT findings, which is consistent with our previous results obtained in septic patients without overt kidney disease (6). It should be noted that Taiwan has a unique background, with the highest prevalence of uremia and endemic hepatitis B virus and hepatitis C virus infections (22). However, because MHD represents the major risk factor for ESRD patients, our findings are probably generalizable to other areas. Patients with cirrhosis have altered nonoxidative glucose disposal, impaired glycogen synthesis, and dysregulated glucose-transporter expression, ultimately resulting in a reduced uptake of 18F-FDG and a higher likelihood of negative 18F-FDG PET/CT findings (23,24). Theoretically, such disadvantages in patients with chronic liver diseases may be avoided by using different PET tracers (e.g., 68Ga-citrate). Further research is needed to address this issue.
The early management of sepsis in ESRD patients undergoing MHD requires identification and control of the source of infection (25). In addition to antimicrobial therapy, removal of the infected catheter, antibiotic lock therapy, and even surgery may be required to achieve an adequate level of infection control and reduce the risk of mortality (26–28). However, the management of septic ESRD patients undergoing MHD can pose several dilemmas. First, the diagnosis of sepsis in this population can be difficult, as ESRD patients may have atypical responses to infections, thus delaying therapeutic interventions that may influence their prognosis. Second, patient cooperation in acute illnesses is scarce, making acceptable diagnostic specimens poorly available. More important, attempted catheter salvage in the presence of a catheter-related infection is invariably associated with an increased risk of progressive infections, metastatic complications, and relapses. The guidelines of the Infectious Disease Society of America suggest catheter removal when complicated or metastatic infections are present (e.g., suppurative thrombophlebitis, septic thrombosis, endocarditis, or osteomyelitis) (29). Under these circumstances, 18F-FDG PET/CT imaging may be useful for diagnosing suspected catheter infections when there are diagnostic dilemmas.
Several previous studies have shown the clinical utility of 18F-FDG PET/CT in the detection of unknown sites of infection and metastatic foci (6,13,30). In the current study, 18 (24.6%) of the 73 patients with positive 18F-FDG PET/CT findings had more than one site of infection identified during a single image acquisition. Seven (53.8%) of the 13 patients with primary vascular access–related infections had concurrent metastatic foci. Importantly, 28 (26.9%) patients had their treatment modified by the results of 18F-FDG PET/CT imaging, including the decision to perform surgical interventions. Conventional imaging modalities lack metabolic information and do not provide whole-body coverage in the detection of unknown foci of infection in ESRD patients receiving MHD. In this patient group, 18F-FDG PET/CT is an ideal imaging modality and has significant prognostic value.
The term malnutrition–inflammation complex syndrome in ESRD patients undergoing MHD indicates the concomitant presence of both malnutrition and inflammation, which are highly correlated with morbidity and mortality (31,32). In our study, low hemoglobin levels and high CRP values were significant risk factors for positive 18F-FDG PET/CT findings. These data may suggest a link between severe malnutrition–inflammation complex syndrome and positive 18F-FDG PET/CT results, which may in turn explain the observed association between positive 18F-FDG PET/CT findings and mortality (hazard ratio, 3.896; 95% confidence interval, 1.039–14.613; P = 0.044). It is not surprising that old age was identified as another prominent risk factor for mortality. Specifically, 23 of the 51 patients who carried both risk factors died during their hospital stay (mortality rate, 45.1%). Close monitoring and aggressive infection control measures are required to reduce mortality in this high-risk group.
To our knowledge, this study was the first to investigate the clinical value of 18F-FDG PET/CT in ESRD patients undergoing MHD and presenting with sepsis of unknown origin. The results of our report have several important clinical implications. First, we have shown that 18F-FDG PET/CT imaging may correctly identify the infection foci in up to 70.2% of cases with unknown origin. Second, 18F-FDG PET/CT can significantly modify clinical management in this patient group (e.g., change to surgical intervention or catheter removal). Third, we were able to define the impact of different clinical characteristics (i.e., chronic liver disease, anemia, CRP levels, and old age) both on the likelihood of positive 18F-FDG PET/CT findings and on mortality. Finally and most important, we have shown that 18F-FDG PET/CT itself has prognostic value in this group of patients (i.e., patients with positive results had longer hospital stays and poorer clinical outcomes).
Some limitations of the current report merit consideration. The caveats of the retrospective nature of the study can be addressed only through future prospective investigations. The absence of patient preparation with a low carbohydrate but fat-allowed diet reduced the diagnostic sensitivity for the detection of infective endocarditis (33). Moreover, we cannot rule out a selection bias because 18F-FDG PET/CT imaging was performed at the discretion of the attending physician. Finally, further research is needed to investigate the exact relations between positive 18F-FDG PET/CT results, the presence and severity of malnutrition–inflammation complex syndrome, and the excess risk of death observed in this study.
CONCLUSION
Our results suggest that 18F-FDG PET/CT may be clinically useful for detecting occult infection sites in patients with ESRD undergoing MHD. In this patient population, positive 18F-FDG PET/CT findings may lead to a significant change in clinical management and independently predict mortality.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 12, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 14, 2014.
- Accepted for publication January 19, 2015.





{kind=link}
{kind=link}