


Abstract
Current guidelines recommend intravenous antibiotic therapy for at least 4 wk in patients with high-risk Staphylococcus aureus bacteremia (SAB), because of the risk for metastatic infection. We evaluated the safety of a shorter duration of treatment in patients with high-risk SAB without signs of metastatic infection at presentation, using standard 18F-FDG PET/CT and echocardiography. Methods: Retrospective analyses were performed of patients with SAB admitted between 2013 and 2017 in 2 medical centers. Patients with risk factors for complicated bacteremia (community acquisition, persistently positive blood cultures, >72 h of fever, or foreign body materials present), a normal echocardiography result, and 18F-FDG PET/CT without signs of metastatic infection were included (cases) and compared with patients with uncomplicated bacteremia (absence of any of the risk factors and no known metastatic disease, controls). Primary outcomes were 3-mo SAB-specific mortality rate and recurrent infection. The secondary outcome was overall mortality. Results: We included 36 cases and 40 controls. Both groups had a similar treatment duration (15.9 vs. 15.4 d). No deaths occurred as a consequence of SAB in the cases, compared with 1 in the control group. One relapse occurred in the case group and 2 in the control group. Overall mortality did not differ between the groups (19.4% vs. 15.0%, P = 0.64). Conclusion: This study suggests that intravenous treatment for 2 wk in high-risk patients with SAB without endocarditis and absence of metastatic infection on 18F-FDG PET/CT is safe. A diagnostic-driven approach using 18F-FDG PET/CT to determine treatment duration in high-risk SAB seems feasible and allows tailoring treatment to individual patients.
Staphylococcus aureus bacteremia (SAB) is a serious infection, associated with a 30-d overall mortality of 20% (1). Metastatic infection, occurring in 16%–73% of patients, is the most important determinant of morbidity and mortality (2–8). Prolonged bacteremia, delayed clinical response to antibiotic treatment, and the presence of foreign body materials are associated with a complicated course. Current guidelines consider both patients with risk factors for metastatic infection and patients with proven metastatic infection as “complicated bacteremia” and recommend intravenous treatment for 4–6 wk. Only a selected group of patients who fulfill the criteria for uncomplicated bacteremia may be treated with a short course of treatment (2 wk) of intravenous antibiotics (9,10). However, these recommendations have not been formally evaluated in clinical studies, and using this approach for all patients with SAB is expensive and may result in complications of unnecessary prolonged therapy for those patients who do not have metastatic infection despite having risk factors (3,10). Unfortunately, metastatic infectious foci often lack signs or symptoms (11).
18F-FDG PET/CT has been increasingly used in diagnosing infectious diseases (12–14). Previous studies on the value of 18F-FDG PET/CT for diagnosing metastatic infection have shown that 18F-FDG PET/CT is able to detect infectious foci in patients with bacteremia and infective endocarditis and is associated with a decrease in relapse and mortality rates (8,13). The diagnostic performance of 18F-FDG PET/CT for detecting metastatic infection is high, with a reported sensitivity approaching 100% (13,15), making it an accurate diagnostic modality to rule out metastatic infection. Therefore, the purpose of this study was to assess the safety of a shorter duration of treatment in patients with risk factors for metastatic disease with normal 18F-FDG PET/CT results and no signs of endocarditis using echocardiography, and to compare this group with patients with uncomplicated SAB, hypothesizing that both groups have a similar outcome of short-term therapy.
MATERIALS AND METHODS
Study Design and Patients
This retrospective observational cohort study was performed at Radboud University Medical Center, Nijmegen, and at Bernhoven Hospital, Uden, The Netherlands. All patients diagnosed with SAB between January 1, 2013, and December 31, 2017, were recorded in an online registry (Castor EDC), using an electronic case report form. Castor EDC complies with the good-clinical-practice standards for recoding data that involve the participation of human subjects. SAB was defined as one or more blood cultures positive for S. aureus. SAB was considered hospital-acquired if patients had been admitted for at least 48 h before the first positive blood culture, and as community-acquired in all other cases. Two groups of patients were included: cases and controls. Cases were patients with one or more risk factors for complicated bacteremia without signs of metastatic infection on 18F-FDG PET/CT and a normal echocardiography result. Controls were patients without any of the risk factors for complicated bacteremia or proven metastatic disease. Inclusion into the case group was restricted to patients with SAB and one or more of the risk factors for complications defined previously (3,9,11): community acquisition of the bacteremia, fever for more than 72 h after initiating appropriate antibiotic treatment, positive follow-up blood cultures obtained 2–4 d after the initial positive blood culture, or the presence of implanted prostheses. Furthermore, case patients had to have no signs of endocarditis on echocardiography and no signs of metastatic infection on 18F-FDG PET/CT. Exclusion criteria for both groups were an intravenous treatment duration of less than 7 d, a persistent primary focus of infection (e.g., a central venous catheter that was not removed), no follow-up 3 mo after treatment completion, or poor-quality 18F-FDG PET/CT, hampering proper interpretation.
According to Dutch law, this study was exempt from approval by an ethics committee because of the retrospective character of this study and the anonymous processing of data. The regional institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived.
Data Collection
Every patient with SAB in the participating hospitals was recorded in the registry by the attending infectious disease physician. All data required to determine inclusion and exclusion criteria, data on patient demographic characteristics, the estimated prognosis of preexisting underlying disease, comorbidity according to the Charlson comorbidity score (16), resistance of S. aureus to methicillin, antimicrobial therapy, treatment duration, and outcomes were retrieved from the online registry.
Diagnostic Work-up
In all patients with SAB, the local antimicrobial stewardship program recommends bedside consultation by an ID specialist, and in patients with high-risk SAB, echocardiography and 18F-FDG PET/CT are also recommended. The local guideline says that echocardiography and 18F-FDG PET/CT can be omitted in low-risk patients. Transthoracic echocardiography was recommended as a first-line screening technique. In patients with persistent suspicion of endocarditis or with prosthetic cardiac valves, transesophageal echocardiography was recommended. An integrated PET/CT scanner (Biograph 40 mCT; Siemens Healthcare) was used. A low-carbohydrate, fat-allowed diet was prescribed 24 h before 18F-FDG PET/CT in all patients. A low-dose CT scan was acquired from the vertex to the bottom of the feet for anatomic correlation and attenuation correction of the PET data. Emission images of the same area were acquired. 18F-FDG PET/CT findings were considered abnormal if focal accumulation of 18F-FDG was detected, suggestive of metastatic infection (13). The primary source of the infection was defined as a localized site of infection preceding bacteremia. A central venous catheter was considered a primary source when there was evidence of inflammation at the insertion site or when culturing of the catheter tip grew S. aureus in the absence of evidence of another source of infection. Respiratory or urinary tract infections were diagnosed as the primary source only when specific symptoms and signs were present in addition to positive culture results. Other primary sources were phlebitis due to peripheral intravascular catheters, and cellulitis or postoperative skin infections. Patients with high-risk SAB and the presence of metastatic infection or endocarditis were advised to be treated for at least 4–6 wk; patients with uncomplicated bacteremia were advised to be treated for at least 2 wk (9). For patients with risk factors for complicated bacteremia without signs of metastatic infection on 18F-FDG PET/CT and echocardiography negative for endocarditis, 2 wk of antimicrobial therapy were recommended by our local guideline. The treatment algorithm used is shown in Supplemental Figure 1 (supplemental materials are available at http://jnm.snmjournals.org).
Patient Outcome
Primary outcome measures were SAB-specific mortality at 3 mo after completion of therapy (defined as clinical evidence of S. aureus infection at the time of death without an alternative cause of death) and recurrent infection (a new episode of SAB within 3 mo after treatment discontinuation). As a secondary outcome, overall mortality at 3 mo after completion of therapy was recorded. Patients were considered to be cured if no symptoms or signs of infection were present at 3 mo after the discontinuation of antibiotic treatment.
To prevent interpretation bias, 2 independent physician observers reviewed hospital records and determined causes of death. If there was no consensus, the case was discussed with a third infectious disease specialist until consensus was reached. The case group was compared with the control group for all outcome measures.
Statistical Analysis
SPSS (version 22.0; SPSS, Inc.) was used for analyzing data. Descriptive statistics for continuous variables were represented as mean ± SD. Unpaired Student t tests were used to compare normally distributed, continuous variables; otherwise, nonparametric tests were used. Categoric variables were compared by use of the χ2 test or, when the χ2 test was not appropriate, the Fisher exact test. Survival data were displayed by Kaplan–Meier curves, and groups were compared by the log-rank test. Differences were considered to be statistically significant at a 2-sided P value of less than 0.05.
RESULTS
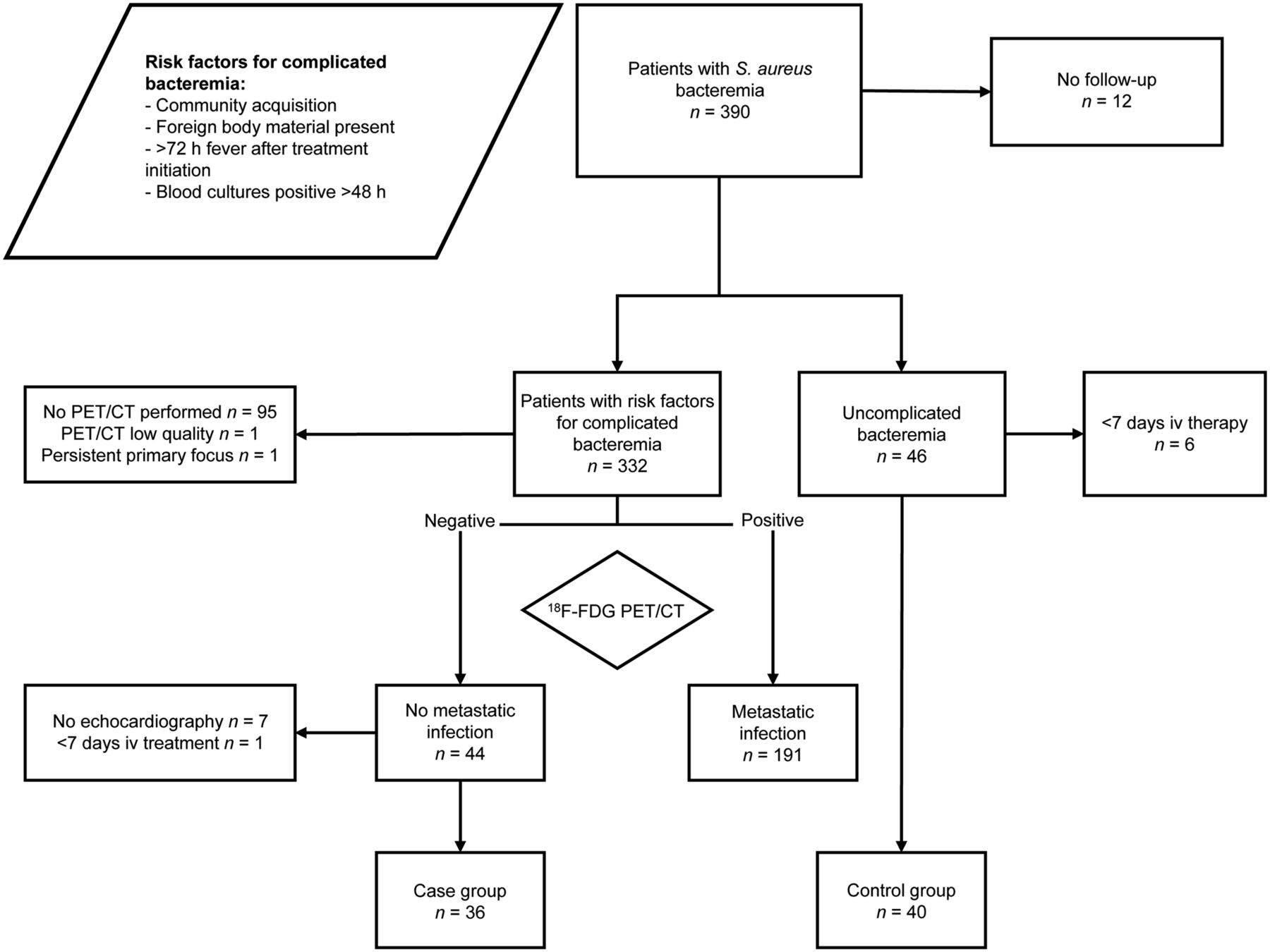
From January 2013 to December 2017, 390 patients were included in the registry (Fig. 1), of whom 265 were classified as high-risk according to the case definition. In 44 of 265 (16.6%) high-risk patients, 18F-FDG PET/CT showed no metastatic infection. Thirty-seven (84.1%) of these 44 patients had a normal echocardiography result; in 7 patients (15.9%), echocardiography was not performed. One patient (2.3%) was excluded because intravenous treatment lasted only 3 d. Thus, 36 patients were included in the case group. Forty-six patients had no risk factors for complicated bacteremia. Of these patients, 6 (13.0%) were treated for less than 7 d with intravenous therapy and were excluded, resulting in 40 patients in the control group. The mean duration from the first positive blood culture until imaging was 8.4 d (SD, 3.8 d) for 18F-FDG PET/CT and 5.9 d (SD, 3.2 d) for echocardiography. The demographics and clinical characteristics are shown in Table 1. The mean treatment duration did not differ between the cases and the controls (15.9 vs. 15.4 d, P = 0.34).

Patient inclusion.
Baseline Characteristics of Patients in Case Group (High-Risk SAB, No Metastatic Infection) and Control Group (Uncomplicated SAB)
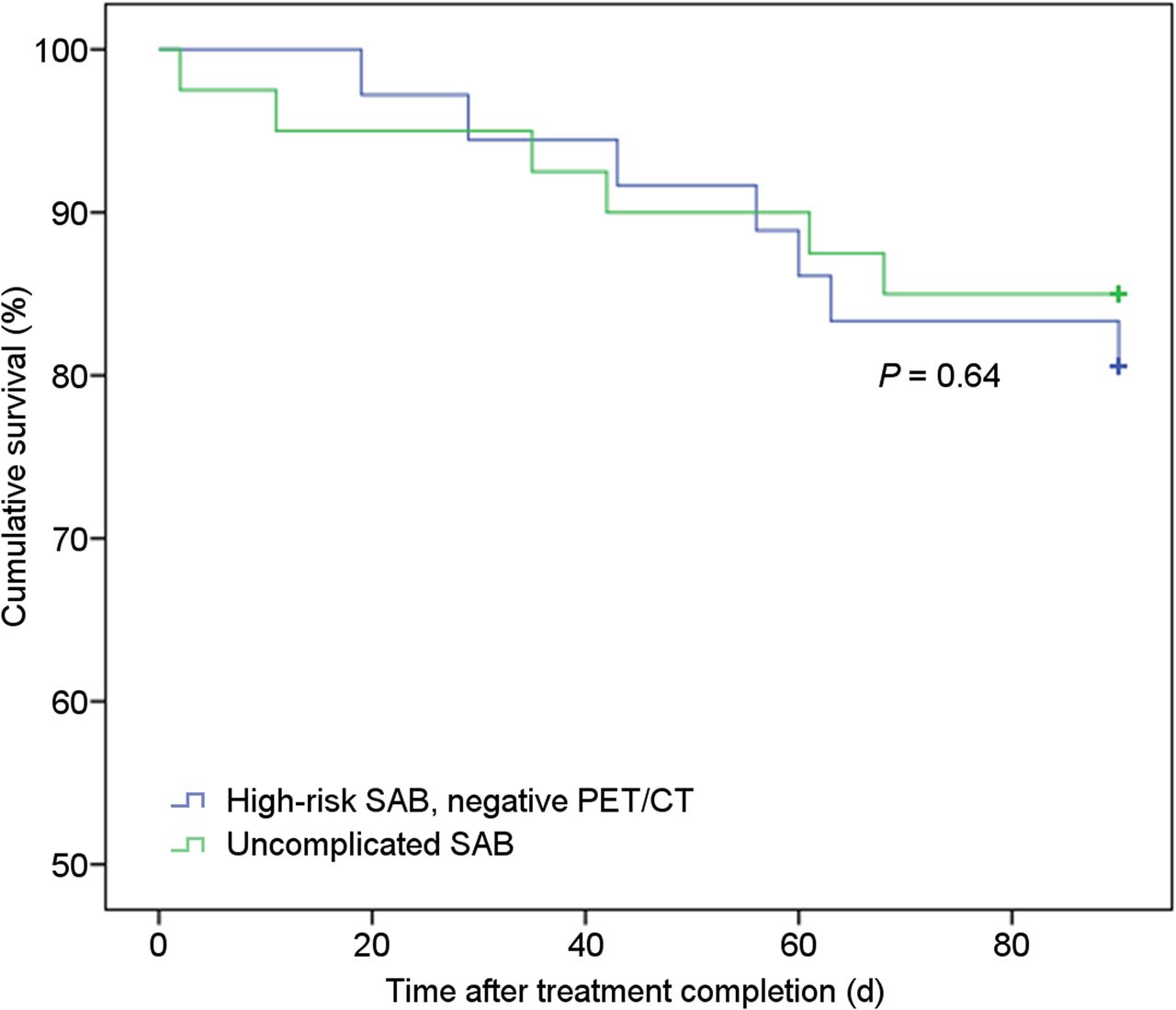
Relapses after treatment were rare in both groups: 2.5% (n = 1) in the case group versus 5.1% (n = 2) in the control group (P = 1.00) (Table 2). The single relapse that occurred in the case group was 11 d after treatment completion in a patient with cerebral lymphoma who had phlebitis and persistently positive blood cultures despite catheter removal. In the case group, no deaths were the direct consequences of SAB. In the control group, one patient died as a consequence of SAB relapse due to septic cerebral embolism. The relapse occurred 1 d after a 10-d course of antibiotic therapy. Follow-up blood cultures were negative after the relapse, but the patient unfortunately succumbed to ongoing sepsis and the consequences of stroke. Twelve patients (15.8%) with SAB died of other causes during the 3-mo follow-up period. Causes of death for the 7 cases were metastatic malignancy (2), non–S. aureus pneumonia (2), heart failure without signs of endocarditis (2), and T-cell lymphoma (1). The causes of death for the 5 control patients were malignancy (2), heart failure without signs of endocarditis (1), non–S. aureus pneumonia (1), and 1 unknown cause (this patient died at home at the age of 88 y, 42 d after treatment completion, without signs of infection). Overall mortality rates were not significantly different among the 2 groups (19.4% in the case group vs. 15.0% in the control group, log-rank test P = 0.64. Fig. 2).
Study Endpoints of Case Group (High-Risk SAB, No Metastatic Infection) and Control Group (Uncomplicated SAB)

Survival 3 mo after treatment completion for patient with high-risk SAB without metastatic infection on 18F-FDG PET/CT and echocardiography (n = 36), and uncomplicated SAB (n = 40) (P = 0.64, log-rank test).
DISCUSSION
In this cohort study, we showed that patients with SAB at high risk of complicated disease, but without signs of metastatic infection on 18F-FDG PET/CT and endocarditis, have a similar outcome to patients without risk factors for complicated SAB when treated with a 14-d course of intravenous antibiotic therapy.
To our knowledge, this was the first study that included 18F-FDG PET/CT in an algorithm to reduce treatment duration in patients with risk factors for complicated SAB. Guidelines for SAB recommend prolonged treatment for 4–6 wk in patients with risk factors for complicated SAB, whereas patients who fulfil criteria for uncomplicated SAB can be treated for 2 wk (1,9,17). The evidence for these recommendations is mainly based on observational cohort studies (10). The currently used risk-based approach to determine treatment duration has limited specificity and may lead to overtreatment. About 36%–50% of patients with one or more risk factors for complicated bacteremia do not have metastatic infection (4,8,13). The present study suggests that 18F-FDG PET/CT in addition to echocardiography can be used to differentiate patients at high risk of complicated SAB without metastatic infection (who may be cured with a short treatment course) from patients with proven complicated SAB (for whom longer treatment is necessary).
18F-FDG PET/CT has a high sensitivity for detecting metastatic infection in patients with gram-positive bacteremia and has been used in several studies for the detection of metastatic infection and subsequent treatment modification (8,13,18). In a prospective study, 115 patients with gram-positive bacteremia who underwent 18F-FDG PET/CT were compared with a historical control group of 230 patients without 18F-FDG PET/CT (13). Significantly more patients were diagnosed with metastatic foci in the study group (67.8% vs. 35.7%). Mortality rates after 6 mo were lower in the study group (19.1% vs. 32.2%, P = 0.014). Furthermore, in a subgroup of patients with SAB, recurrent infection occurred less frequently in the 18F-FDG PET/CT group (1.5% vs. 8.9%, P = 0.04) (13). In a retrospective control study, we previously showed that performing 18F-FDG PET/CT in patients with high-risk SAB detects metastatic infection in 74% of patients and leads to treatment modifications in 75% and is associated with reduced mortality (8). Our current study adds a rationale for 18F-FDG PET/CT in patients with risk factors for complicated SAB.
Our study has several limitations: it was retrospective, with a relatively small population sample. However, we proposed a novel strategy for optimizing treatment of SAB that had not been studied in this way before. The ideal design would have been randomization of patients with risk factors for complicated disease without signs of metastatic infection on 18F-FDG PET/CT to short versus long intravenous treatment. Second, we could not assess the impact of the present strategy on patients infected by methicillin-resistant Staphylococcus aureus. Some studies have suggested that methicillin-resistant S. aureus is more virulent than methicillin-susceptible S. aureus (19), whereas other studies did not find this association (20). Short-course treatment in a cohort with methicillin-resistant S. aureus bacteremia should be a subject for further investigation. Third, the most important predictor for endocarditis is the presence of a positive follow-up blood culture result (3). The case group included only 6 patients with persistent bacteremia. Clinicians should be prudent and consider repeated echocardiography in cases with positive follow-up blood cultures, and treatment duration should be determined on an individual level.
Although 18F-FDG PET/CT is an expensive investigation, its cost effectiveness has been shown in a previous study (21). The savings from a shorter treatment duration were not considered in that study. We estimate that for the group of patients we studied, savings will be larger: the costs of 2- to 4-wk prolonged intravenous treatment at home (∼2,000–4,000 euros) are higher than the costs of a single 18F-FDG PET/CT in our institution (∼900 euros). Additional visits for follow-up of outpatient parenteral antimicrobial therapy and possible treatment-related complications are not included.
CONCLUSION
In this study, the treatment duration could be safely reduced to 2 wk in patients with high-risk SAB without signs of metastatic infection on 18F-FDG PET/CT and echocardiography. The findings in this study support the potential for performing 18F-FDG PET/CT in patients with high-risk SAB. Larger prospective studies are needed to validate these findings, especially in patients with MRSA.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 14, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 16, 2018.
- Accepted for publication November 28, 2018.





{kind=link}
{kind=link}