


Abstract
Gram-positive bacteremia has a high morbidity and mortality rate of approximately 30%. Delayed diagnosis of clinically silent metastatic infectious foci is an important indicator for a complicated outcome. 18F-FDG PET/CT allows detection of focal infection, resulting in lower relapse rates and mortality. Here, we present a cost-effectiveness analysis associated with introduction of 18F-FDG PET/CT for patients with gram-positive bacteremia. Methods: A cost-effectiveness analysis in a prospective 18F-FDG PET/CT group (n = 115) and matched control group (n = 230) was performed alongside a clinical study, the results of which were previously published. Mortality at 6 mo was considered the final effect outcome and was used in the denominator of the incremental cost-effectiveness ratio. Results: Mortality in the 18F-FDG PET/CT group was 19%, compared with 32% in the control group (P < 0.01). Incremental costs of 18F-FDG PET/CT were $9,454 (95% confidence interval [CI], $3,963–$14,947), mainly because of admission (mean, $6,631; 95% CI, $1,449–$11,814). Additional costs were related to echocardiography (P < 0.01), not to 18F-FDG PET/CT (P = 0.8). The mean incremental costs of the 18F-FDG PET/CT strategy estimated by stratification for endocarditis were $5,277 per patient (95% CI, $429–$10,123; P = 0.03). The point estimate of the incremental cost-effectiveness ratio is $72,487 per prevented death (95% CI, $11,388–$323,379). Conclusion: Introduction of a diagnostic regimen including routine 18F-FDG PET/CT decreases morbidity and mortality. The cost increase is due to in-hospital treatment of metastatic infectious foci. Costs per prevented death, $72,487, are within the range that is considered to be efficient by Dutch guidelines. Patients with high-risk gram-positive bacteremia therefore should have easy access to 18F-FDG PET/CT to enable early detection of metastatic infectious disease.
Gram-positive bacteremia is a serious and growing health care problem known for its high morbidity and a mortality rate of approximately 30% (1–5). In several European studies, the incidence of Staphylococcus aureus bacteremia (SAB) increased to 17–19 per 100,000 inhabitants over the past few decades (6,7). In the same time frame, both community-acquired and nosocomial SAB increased more than 2- to 3-fold to approximately 250 per 100,000 hospital discharges in the United States (8,9). Among survivors of nosocomial bloodstream infections at a surgical intensive care unit, the median hospital stay of surgical patients was extended by 14–24 d once admission was complicated by a bloodstream infection (10,11). Delayed diagnosis of disease activity and subsequent treatment is one of the most important indicators for a complicated outcome (12). Incomplete eradication of either the primary infection or secondary metastatic infectious foci appears to be the most important contributor to worse outcome and relapse of infection, specifically in gram-positive bacteremia (13). A substantial part of metastatic infectious foci (32%) is clinically silent because the foci lack guiding symptoms (14). To date, diagnostic strategies after gram-positive bacteremia are mainly symptom-based, even though metastatic infectious foci are described in 16%–36% of patients in daily clinical practice (2–5). Extra costs attributable to infection averaged $30,000–$40,000 in the 1990s and may be higher at present (10,11). Routine echocardiography in SAB to assess endocarditis is the only imaging technique that has been studied extensively. Routine echocardiography proved to be cost-effective and is recommended in international guidelines to rule out infective endocarditis in patients with high-risk bacteremia (15,16).
It has been hypothesized that scintigraphic whole-body imaging techniques are helpful in detecting clinically silent infectious foci other than endocarditis (17). In an earlier study, 18F-FDG PET/CT proved to reveal clinically relevant metastatic foci, despite the fact that a median of 3 conventional imaging techniques had been performed before 18F-FDG PET/CT had been ordered (18). Because uncomplicated bacteremia can be cured with 2 wk of antibiotic treatment, metastatic foci ideally should be revealed within the first 2 wk after admission to enable the physician to adjust treatment, for example, either to prolong antibiotic treatment or to perform surgical drainage (19–21). Most metastatic foci require at least 6 wk or longer of antibiotic treatment to be cured.
In a prospective matched-control study published before in this The Journal of Nuclear Medicine, we showed that introduction of 18F-FDG PET/CT for detection of metastatic infectious foci in patients with SAB or Streptococcus spp. bacteremia (SSB) reduced both relapse rates and mortality due to SAB and SSB (1). In the present study, performed alongside our previous clinical study (1), we assessed costs associated with the introduction of 18F-FDG PET/CT for this indication, resulting in information about the efficiency or cost-effectiveness of the addition of 18F-FDG PET/CT in high-risk patients with gram-positive bacteremia. The cost-effectiveness analysis was performed from a health care perspective, meaning only direct medical costs related to diagnosis, treatment, and admission were analyzed. We hypothesized that early detection and treatment of metastatic foci would be cost-effective because fewer patients would be readmitted and treated for relapse of infection, or delayed cure.
MATERIALS AND METHODS
Design
The methodology of the clinical study was published earlier (1). In brief, between 2005 and 2008 18F-FDG PET/CT was performed in the first 2 wk after admission for 111 of 115 prospectively included study patients with gram-positive bacteremia and at least one of the following risk factors for the development of metastatic infectious foci: community acquisition, signs of infection longer than 48 h before initiation of appropriate treatment, fever more than 72 h after initiation of appropriate treatment, or positive blood cultures more than 48 h after initiation of appropriate treatment. Study patients were matched for microorganism and risk profile for the presence of metastatic infectious foci with 230 historic control patients in the same hospital in the 4 y preceding the prospective study for whom no 18F-FDG PET/CT was performed. Echocardiography was facilitated routinely in the 18F-FDG PET/CT group and was performed only in the historic control group at the discretion of the attending physician. Metastatic infectious foci included those localized infectious foci without anatomic relation to the portal of entry of bacteremia (i.e., hematogenous spreading) or direct extension beyond the anatomic borders of the primary source of infection (e.g., abscess formation after wound infections). Endocarditis was defined according to the Duke criteria (22).
Besides clinical data, cost data were collected using the principles of a cost-effectiveness analysis. An electronic case record form was used to collect resource consumption data (Access 2003; Microsoft). Both in the prospectively acquired study population and in the historic control group, only health care variables and medical costs were collected, using a microcosting approach, meaning all relevant cost components were defined at the most detailed level (23).
Effect measures that were collected and considered relevant to the cost-effectiveness analysis were relapse rate, defined as confirmed relapse of infection within 3 mo after completion of antibiotic treatment and mortality at 6 mo of follow-up. Mortality was considered the final outcome (together with costs) and was used in the denominator of the incremental cost-effectiveness ratio. Differences in relapse rate were reported on comparison of the 18F-FDG PET/CT group and the historic controls. The cost-effectiveness ratio was expressed as costs per prevented death. Potential confounders between both study groups in the clinical study were considered in the analysis by substratification or by adding the confounders as a covariate to the linear regression model.
Cost Analysis
All medical costs associated with the experimental strategy were recorded prospectively in Euros (1 Euro = 1.5 U.S. Dollars). Also, the costs related to more accurate diagnostics resulting in more appropriate treatment of patients were recorded. Direct costs related to the diagnosis and treatment of patients with a complicated bloodstream infection included admission days in the intensive care unit and general ward, all imaging techniques, antibiotic treatment, specialist consultation, and surgical interventions. Costs of the primary visit to the emergency room department, routine blood examinations, blood cultures, and chest radiographs were not included in the analysis because they belong to regular care and there were no differences on a per-patient basis in either study group. The cost analysis had 2 main parts. First, at the patient level, the duration of hospital admission, length of antibiotic treatment, and numbers and types of procedures were considered in both the historic control group and the prospective study group. In the second part of the cost analysis, prices were determined for each unit of health care consumed. Subsequently, these were used for multiplying the volumes registered for each patient. In the case of relapse of infection, the same set of items was collected, and costs were added to the total costs of the first admission. The prices per item were retrieved from various sources (Table 1). The costs of antibiotic treatment were assessed using a standardized method of full-cost calculation (including administration and monitoring costs) as published before (24,25). The Dutch guidelines for conducting pharmacoeconomic studies and the guidelines for cost analyses were used (26,27). Costs were adjusted to the price level of the first quarter of 2007 based on the consumer price index as presented by the Central Bureau of Statistics (www.statline.nl). Mean, median, range, and SD of the total medical costs per patient were determined for each of the 2 groups. Depending on the skewness of the distribution, costs were either log-transformed or not. On costs, parametric statistical testing was done.
Unit Costs and Sources
The incremental costs of 18F-FDG PET/CT alone were estimated by excluding all patients with endocarditis, because echocardiography is the preferred imaging technique to detect endocarditis. Because of physiologic 18F-FDG uptake in the myocardium, 18F-FDG PET/CT scans were not analyzed for possible endocarditis. Therefore, both 18F-FDG PET/CT and echocardiography should be considered as having the potential to independently bring about an improvement in patient management by detecting clinically relevant infectious metastatic foci. In the 18F-FDG PET/CT group, besides 18F-FDG PET/CT, also echocardiography had been performed significantly more often than in the control group (P < 0.01), resulting in the detection of significantly more patients having endocarditis
Cost-Effectiveness Analysis
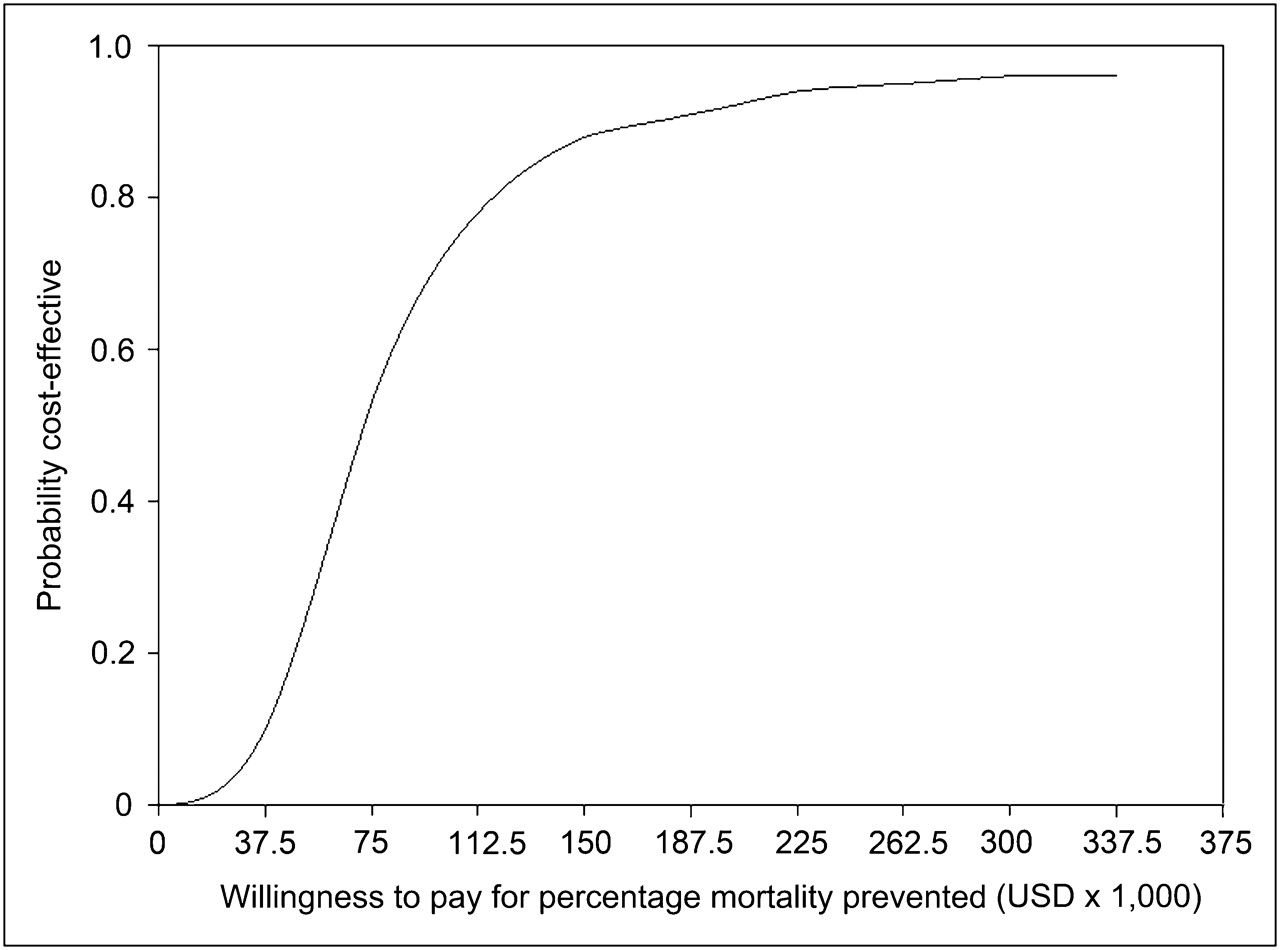
Uncertainty surrounding the incremental cost-effectiveness ratio (ICER), expressed as costs per percentage mortality prevented, was determined with the bootstrap method, resulting in a mean and confidence interval (CI), which are presented in a cost-effectiveness plane. The 95% confidence interval is estimated using the percentile method. Finally a cost-effectiveness acceptability curve was derived, enabling us to evaluate efficiency by exploring a range of thresholds (willingness to pay for a percentage mortality prevented). The graph shows how many of the bootstrap replications fall to the right of some line with the slope equal to the ICER, given a certain willingness to pay for a percentage mortality prevented. For an increasing willingness to pay for a percentage mortality prevented, the probability that the addition of the PET scan becomes cost-effective increases according to the shape of the acceptability curve.
RESULTS
Clinical Trial
Patient characteristics and results of the clinical trial have been reported earlier (1). The main results of the clinical study are presented in Table 2. Both relapse rate (2.6% vs. 7.4%, P = 0.07) and mortality (19% vs. 32%, P < 0.01) were favorable in the 18F-FDG PET/CT group, compared with the matched historic control group (1).
Main Results of Clinical Study
The length of hospital stay was similar in both the 18F-FDG PET/CT and the control group (27 and 28 d, respectively, in the presence of metastatic infection and 14 d in both groups in the absence of metastatic infection). Duration of treatment also depended on the presence or absence of metastatic infectious foci in both groups. During follow-up, no additional foci became apparent in the study group, indicating that no clinically relevant lesions were missed. To confirm 18F-FDG PET/CT findings, 24 ultrasound examinations, 16 CT scans, and 7 MRI scans were obtained.
Echocardiography, however, was a potential confounder as it was performed in 29% in the control group and in 83% in the 18F-FDG PET/CT group. Because of this difference, endocarditis was diagnosed significantly more often in the 18F-FDG PET/CT group (P = 0.01). Endocarditis was never diagnosed by 18F-FDG PET/CT. After correction for the effect of echocardiography, the mortality of the 18F-FDG PET/CT group was still favorable as compared with the control group (P < 0.01).
Cost Analysis
Mean total costs per patient were higher in the 18F-FDG PET/CT group ($3,1710; 95% CI, $25,954–$37,465) than in the control group ($22,255; 95% CI, $19,623–$24,888). The incremental costs of the 18F-FDG PET/CT group were $9,454 (95% CI, $3,963–$14,947). Mean total costs of relapse of infection were $23,979 per patient in the 3 patients with a relapse in the 18F-FDG PET/CT group and $20,679 per patient in 17 patients with a relapse in the control group. Admission days accounted for the largest part of the incremental costs, with a mean of $6,631 per patient (95% CI, $1,449–$11,814) (Table 3). When echocardiography was analyzed as a potential confounder, costs in the 18F-FDG PET/CT group were not related to 18F-FDG PET/CT (P = 0.8) but to echocardiography (P < 0.01). The mean incremental costs due to 18F-FDG PET/CT estimated by stratification for endocarditis were $5,277 per patient (95% CI, $429–$10,123; P = 0.03).
Mean Incremental Costs of 18F-FDG PET Group, Compared with Control Group per Volume
Cost-Effectiveness Analysis
Figure 1 shows the cost-effectiveness plane where 1,000 bootstrapped ICERs (cost per percentage mortality prevented) are presented. The estimated ICER is $72,487 per mortality prevented death (95% CI, $11,388–$323,379), indicating that prevention of a single fatality by the addition of 18F-FDG PET/CT requires an additional investment in health care of $72,487.

Cost-effectiveness plane with bootstrap replicates of ICER expressed as cost per percentage mortality prevented. USD = U.S. dollars.
Figure 2 shows the acceptability curve based on the analysis described in the “Cost Analysis” section. Figure 2 indicates that, given an 80% chance of being cost-effective, the willingness to pay for a prevented death approaches $112,500, indicating that the costs to prevent a death due to the addition of 18F-FDG PET/CT ($72,487) is within the generally accepted limit of the willingness to pay.
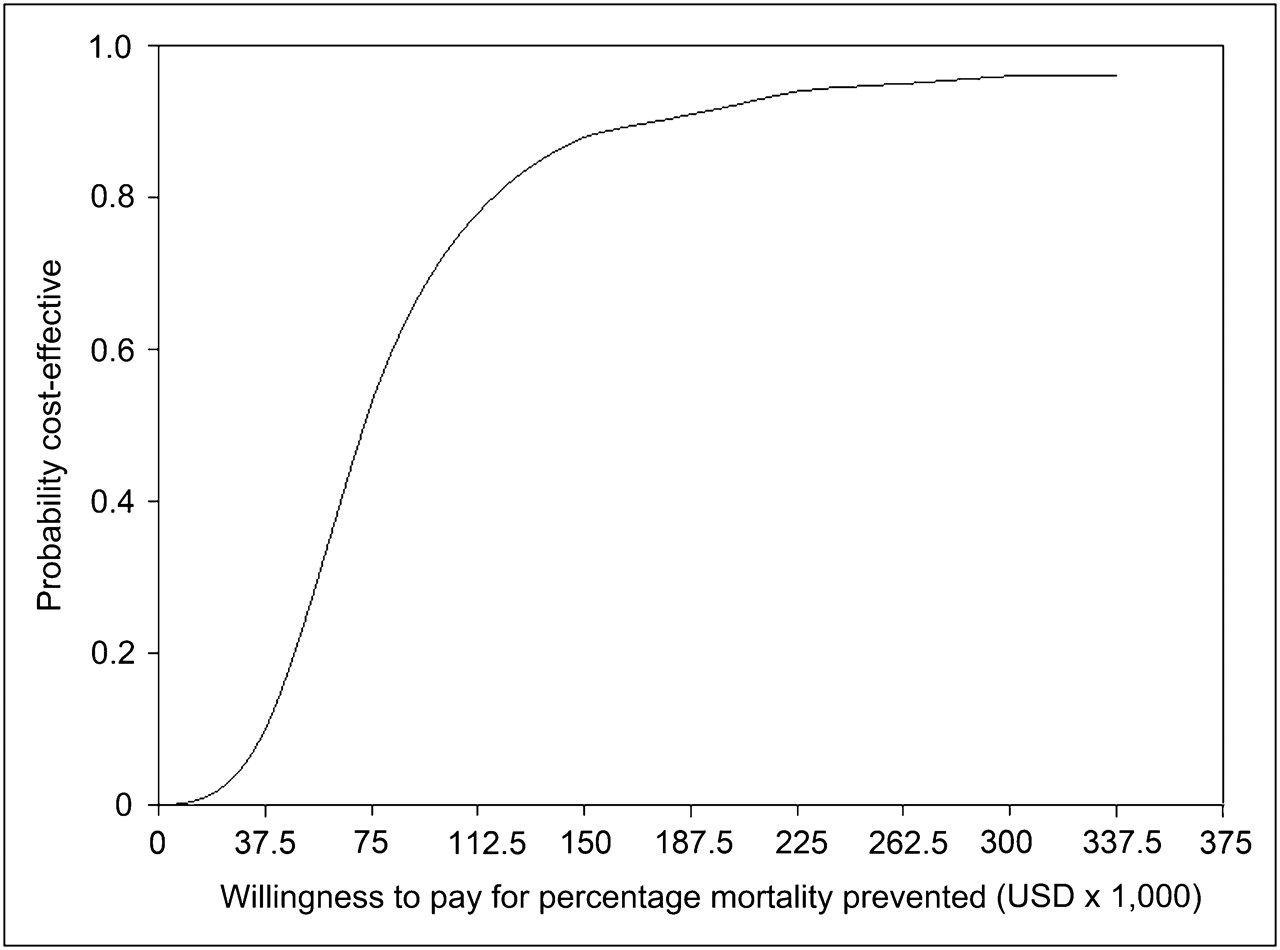
Willingness to pay for percentage mortality prevented. Acceptability curve can be interpreted as probability that 18F-FDG PET/CT will be cost-effective for certain willingness to pay for percentage mortality prevented. USD = U.S. dollars.
DISCUSSION
This study reports on the cost-effectiveness of routine performance of 18F-FDG PET/CT in patients with high-risk gram-positive bacteremia. We demonstrated that this strategy identified significantly more clinically relevant infectious foci, enabling early adjustment of treatment and a consequent decrease in mortality rates. Associated costs resulted in a point-estimate of $72,487 per prevented death—an investment that is well within the acceptable range (26). In-hospital treatment, prolongation of antibiotic treatment, and surgical procedures are the most important cost drivers.
To date, no direct comparison is available on this subject. In patients with pneumococcal pneumonia, in whom disease burden is considered high (0.82), acceptable costs per quality-adjusted life-year were estimated at $96,000 (26,28). In the present study, however, because we did not measure quality-adjusted life-years, a comparison with the point-estimate of costs per prevented death was hampered ($72,487). In-hospital treatment is not needed for a substantial number of patients with pneumococcal pneumonia, in contrast to SAB and SSB, for which many patients are admitted to the hospital (1,14,26). Therefore, disease burden and the related impact on quality-adjusted life-years might be higher in SAB and SSB. Following this line of reasoning, it seems appropriate to state that 18F-FDG PET/CT is an efficient modality.
In the 18F-FDG PET/CT group, both echocardiography and 18F-FDG PET/CT had been performed more often, resulting in an increase in the number of patients with metastatic infectious foci. The number of patients diagnosed with endocarditis doubled in the 18F-FDG PET/CT group. As patients were carefully matched for their risk for infectious complications, the incidence of endocarditis can be considered to be equal in both groups. The increase in the number of patients diagnosed with endocarditis in this group therefore was explained by the performance of echocardiography. Treatment of endocarditis seemed to be the main driver of costs when echocardiography was added in the cost-effectiveness analysis. The consequence of excluding all patients with endocarditis from the analysis is a decrease in incremental costs from $9,454 (95% CI, $3,963–$14,947) to $5,277 (95% CI, $429–$10,123). This figure cannot be translated into real costs contributed by 18F-FDG PET/CT because in a subgroup of patients both endocarditis and other clinically relevant metastatic infectious foci requiring prolonged antibiotic treatment were present. It shows, however, that both echocardiography and, in lesser part, 18F-FDG PET/CT are cost drivers.
A potential weakness of the study is the fact that the cost-effectiveness analysis was based on the Dutch health care system. If the provision of care differs, then transferability becomes more limited. The price difference, on the other hand, does not jeopardize the transferability of the cost-effectiveness conclusion, as it is a constant factor, with the unit costs and differences in relapse rates and duration of treatment provided in the “Results” section.
Although confirmation of 18F-FDG PET/CT findings is still daily clinical practice, it might be reasonable to anticipate that decisions made solely on the basis of 18F-FDG PET/CT will result in lower incremental costs than in the present study group, in which confirmation 18F-FDG PET results by conventional techniques was required per protocol. The positive predictive value of 18F-FDG PET/CT for the detection of localized infectious foci when performed in patients at high risk for metastatic infectious foci was around 90% in previous studies (1,18). This high predictive value leads to efficiency gains, especially when 18F-FDG PET/CT is performed in high-risk patients, because conventional radiologic techniques may subsequently be restricted to delineating the extent of infection if necessary (such as the epidural extent in patients with spondylodiskitis) or to evaluating those patients with persistent complaints despite adequate treatment.
CONCLUSION
Routine 18F-FDG PET/CT in patients with high-risk gram-positive bacteremia is an important tool to reduce morbidity and mortality. Introduction of a diagnostic regimen that incorporates routine 18F-FDG PET/CT results in an increase in costs due to more in-hospital treatment of clinically relevant metastatic infectious foci. Still, the costs per prevented death, $72,487, are considered to be well within the range that is generally accepted as efficient. Cost-effectiveness would further improve if patient management were based on 18F-FDG PET/CT abnormalities without the addition of noncontributing confirmatory tests. Patients with high-risk gram-positive bacteremia therefore should have easy access to 18F-FDG PET/CT when available, to enable early detection of metastatic infectious disease.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
This study was supported in part by a grant from the Netherlands Organization for Health Research and Development (ZonMw). The funding source had no influence on study design, data collection, analysis, interpretation of data, writing of the report, or in the decision to submit the paper. All authors had full access to the data and held the final responsibility for the decision to submit the report for publication. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 7, 2011.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication February 23, 2011.
- Accepted for publication July 14, 2011.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Infective endocarditis: Beyond the usual tests
- 18F-FDG PET/CT-Guided Treatment Duration in Patients with High-Risk Staphylococcus Aureus Bacteremia: A Proof of Principle
- The Value of 18F-FDG PET/CT in Diagnosis and During Follow-up in 273 Patients with Chronic Q Fever
- 18F-FDG PET/CT Optimizes Treatment in Staphylococcus Aureus Bacteremia and Is Associated with Reduced Mortality
- 18F-FDG PET/CT in the Diagnostic Workup of Infective Endocarditis and Related Intracardiac Prosthetic Material: A Clear Message
- 18F-FDG PET/CT for the Detection of Septic Embolisms in Patients with Infectious Endocarditis
- Role of 18F-FDG PET in Patients with Infectious Endocarditis
- Radiolabeled WBC Scintigraphy in the Diagnostic Workup of Patients With Suspected Device-Related Infections
- Imaging for Infected Cardiac Implantable Electronic Devices: A New Trick for Your Pet