


Abstract
In 1%–5% of all acute Q fever infections, chronic Q fever develops, mostly manifesting as endocarditis, infected aneurysms, or infected vascular prostheses. In this study, we investigated the diagnostic value of 18F-FDG PET/CT in chronic Q fever at diagnosis and during follow-up. Methods: All adult Dutch patients suspected of chronic Q fever who were diagnosed since 2007 were retrospectively included until March 2015, when at least one 18F-FDG PET/CT scan was obtained. Clinical data and results from 18F-FDG PET/CT at diagnosis and during follow-up were collected. 18F-FDG PET/CT scans were prospectively reevaluated by 3 nuclear medicine physicians using a structured scoring system. Results: In total, 273 patients with possible, probable, or proven chronic Q fever were included. Of all 18F-FDG PET/CT scans performed at diagnosis, 13.5% led to a change in diagnosis. Q fever–related mortality rate in patients with and without vascular infection based on 18F-FDG PET/CT was 23.8% and 2.1%, respectively (P = 0.001). When 18F-FDG PET/CT was added as a major criterion to the modified Duke criteria, 17 patients (1.9-fold increase) had definite endocarditis. At diagnosis, 19.6% of 18F-FDG PET/CT scans led to treatment modification. During follow-up, 57.3% of 18F-FDG PET/CT scans resulted in treatment modification. Conclusion: 18F-FDG PET/CT is a valuable technique in diagnosis of chronic Q fever and during follow-up, often leading to a change in diagnosis or treatment modification and providing important prognostic information on patient survival.
Q fever is a zoonosis with a worldwide distribution caused by the intracellular bacterium Coxiella burnetii. In The Netherlands, a large Q fever outbreak occurred between 2007 and 2010 with over 4,000 notified cases of acute Q fever and more than 40,000 infected patients (1). In 1%–5% of infections with C. burnetii, chronic Q fever infection develops (2,3). In most patients, manifestations of chronic Q fever are endocarditis, infected aneurysms, or infected vascular prostheses. Even if adequate treatment is started, chronic Q fever causes high morbidity and mortality. Many patients with chronic Q fever present when severe complications develop, such as a ruptured aneurysm, with an associated high mortality (4). Therefore, it is important to diagnose chronic Q fever early and start treatment as soon as possible. However, diagnosing chronic Q fever is often difficult.
18F-FDG PET/CT is effective in localizing metastatic infection in cases of bacteremia (5,6). In endocarditis, the diagnosis is made using the modified Duke criteria, with evidence of endocardial involvement on echocardiography as one of the major criteria (7). The value of 18F-FDG PET/CT for diagnosing native valve endocarditis has been investigated, but sensitivity is not optimal (8,9). For prosthetic valve endocarditis, 18F-FDG PET/CT has shown promising results, and recently 18F-FDG PET/CT was added to the European Society of Cardiology criteria as a major criterion for diagnosing prosthetic valve endocarditis (10). In diagnosing vascular infection, 18F-FDG PET/CT has proven its effectiveness (11,12) also in chronic Q fever vascular infection (13,14).
In this study, we investigated the diagnostic value of 18F-FDG PET/CT in patients with chronic Q fever at the time of diagnosis and during follow-up, as well as the effect on treatment modification. We also studied whether the addition of 18F-FDG PET/CT to the modified Duke criteria can improve diagnosis of chronic Q fever endocarditis.
MATERIALS AND METHODS
Patients and Study Design
All Dutch patients who were at least 18 y old and had possible, probable, or proven chronic Q fever according to the Dutch consensus guidelines (Table 1) (15) were included when one or more 18F-FDG PET/CT scans were obtained. All Dutch hospitals treating chronic Q fever patients were actively approached to include all chronic Q fever patients who were detected since the start of the Dutch Q fever epidemic in 2007. Patients were included in this study until March 2015. Data on patient characteristics, signs and symptoms, microbiologic results, 18F-FDG PET/CT results and their consequences, echocardiography, type and duration of antibiotic therapy, and outcome were collected from patient records. The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived.
Dutch Consensus Guidelines on Chronic Q Fever Diagnosis (15)
Diagnostic Work-up
The patients included in this study underwent 18F-FDG PET/CT in the hospital where they were evaluated or treated for their chronic Q fever. For this study, Siemens Biograph (16, 20, or mCT40) and Philips Gemini (GXL16, TF16, or TF64) PET/CT scanners were used. Before 18F-FDG injection, all patients fasted and any glucose- or insulin-containing infusions were discontinued for at least 6 h. In 22.5% of patients, a low-carbohydrate fat-allowed diet was followed 24 h before 18F-FDG PET/CT. One hour after injection of 18F-FDG, a low-dose CT scan of the area between the proximal femora and skull base was acquired for anatomic correlation and attenuation correction of the PET data. To avoid interpretation bias, the retrospectively acquired 18F-FDG PET/CT images were prospectively reevaluated by 3 nuclear medicine physicians without knowledge of the prior clinical evaluation and masked to any clinical information or patient history. For evaluation, specific criteria for assessment of vascular infection and endocarditis were used (Table 2). 18F-FDG PET/CT assessed by this structured scoring system was compared with the final clinical diagnoses, which were based on medical history, physical examination, laboratory and microbiologic results, and imaging. Microbiologic analysis for the diagnosis of chronic Q fever consisted of serology and polymerase chain reaction (PCR) for C. burnetii DNA on plasma, serum, and tissue. An indirect fluorescent-antibody assay (Focus Diagnostics, Inc.) was used for serologic analysis in all patients. The modified Duke criteria were used for diagnosing infective endocarditis (7). Whether the sensitivity of these criteria could be improved by adding the result of the 18F-FDG PET/CT was studied in an attempt to improve the diagnostic criteria for chronic Q fever endocarditis. The impact of 18F-FDG PET/CT on treatment modification was determined by 2 study coauthors for all cases based on all available clinical information as registered in the patient records and classified as follows: initiation of antibiotic treatment, discontinuation of antibiotic treatment, changing of the type of antibiotic treatment, continuation of antibiotic treatment, and surgical intervention. If the result of 18F-FDG PET/CT did not result in any modification, this was also reported.
Interpretation of 18F-FDG PET/CT Combining Visual Grading Score and Uptake Pattern
Statistical Methods
All data were analyzed using SPSS, version 20 (SPSS, Inc.). Two-tailed χ2 tests or Wilcoxon tests were used to compare qualitative data. Mean values were analyzed by Student t tests.
RESULTS
In total, 379 patients had a diagnosis of proven, probable, or possible chronic Q fever according to the Dutch consensus guidelines (15). 18F-FDG PET/CT was performed on 273 patients, and in 230 of these patients, 18F-FDG PET/CT was performed at diagnosis of chronic Q fever. During follow-up, 218 18F-FDG PET/CT scans were obtained on 143 patients. The reasons for follow-up 18F-FDG PET/CT were suspected new complications (175, 80.3%) or end-of-treatment evaluation (43, 19.7%). New complications in chronic Q fever patients, such as new abscesses, new spondylodiskitis, or progression of the primary infection during treatment, were suspected in cases of new positive serum PCR, no change in antibody titer after 1 y of treatment, or increasing titers, as well as in cases of new or increasing complaints. In 43 patients, only follow-up 18F-FDG PET/CT was performed, without baseline 18F-FDG PET/CT at diagnosis. In these patients, diagnosis of chronic Q fever was based on a combination of serology, PCR, or CT imaging. Of all 273 patients (199 men [72.9%] and 74 women [27.1%]), 147 were eventually diagnosed with proven chronic Q fever, 60 with probable chronic Q fever, and 66 with possible chronic Q fever. The mean age of the patients at diagnosis was 65.0 y. A known history of acute Q fever was identified in 105 patients (38.5%). Risk factors and outcome for all patients are shown in Table 3. Overall, in 93 patients (63.3%) with proven chronic Q fever, infectious foci were seen on 18F-FDG PET/CT. Of the 448 18F-FDG PET/CT scans obtained in this study, 438 scans could be reevaluated (10 scans were not available for reevaluation).
Risk Factors and Outcome of All Patients with Proven, Probable, and Possible Chronic Q Fever
Vascular Infection
Of all 142 18F-FDG PET/CT scans obtained at diagnosis of chronic Q fever with grade 1 or grade 2 vascular patterns (Table 2), 3 (2.1%) were from patients with a clinical diagnosis of vascular infection. Reevaluation of follow-up 18F-FDG PET/CT confirmed this diagnosis in 2 patients; in the third patient, follow-up 18F-FDG PET/CT was missing but the diagnosis was confirmed by positive PCR on tissue of the aneurysm. The results of all reevaluated 18F-FDG PET/CT scans obtained at diagnosis of chronic Q fever for vascular infection (Fig. 1) and Q fever–related mortality are shown in Table 4. Of 29 scans with a homogeneous 18F-FDG uptake pattern, 16 (55.2%) were considered to show inflammation without infection and 13 (44.8%) to show vascular infection due to perigraft soft-tissue involvement, of which 9 cases had positive PCR on vascular tissue. Q fever–related mortality rates in patients with and without vascular infection based on this scoring system were 23.8% and 2.1%, respectively (P = 0.001).

18F-FDG PET/CT scan of 72-y-old man with proven chronic Q fever, infected endovascular aortic graft, and psoas abscess (arrows). Patient had vascular surgery 6 mo after initiation of antibiotic therapy with doxycycline and hydroxychloroquine because of severity of infection. Four years later, patient was still on antibiotic treatment because of persisting chronic Q fever infection.
Results of 221 Reevaluated 18F-FDG PET/CT Scans at Diagnosis of Chronic Q Fever
Endocarditis
Of all chronic Q fever patients, 9 (3.3%) had definite endocarditis according to the modified Duke criteria and 59 (21.6%) had possible endocarditis. In 36 of all patients, no echocardiography was performed. On reevaluation of 18F-FDG PET/CT scans, the heart showed diffuse 18F-FDG uptake (grade 2) on 300 18F-FDG PET/CT scans in 193 patients, making a reliable assessment of the heart impossible. In 92.3% of these scans, no prior low-carbohydrate fat-allowed diet had been followed. Of all 80 patients in whom 18F-FDG PET/CT scans were assessable for the heart region, 10 18F-FDG PET/CT scans (12.5%) showed focal 18F-FDG uptake indicating endocarditis (grade 3) (Fig. 2). Of these 10 patients, 2 (20.0%) had a diagnosis of definite endocarditis according to the modified Duke criteria. Of all 70 patients without relevant 18F-FDG uptake by the heart valve (grade 1), 2 (2.9%) had definite endocarditis according to the modified Duke criteria. Of all 237 patients who underwent echocardiography, 9 had valve vegetations on echocardiography. Of these 9 patients, evaluation of 18F-FDG PET/CT scans showed grade 1 18F-FDG uptake in 2 patients, grade 2 in 4 patients, and grade 3 in 3 patients.

18F-FDG PET/CT scan of 67-y-old man with history of acute Q fever and analysis because of severe fatigue. Serology for C. burnetii showed increased antiphase 1 IgG; PCR on blood was negative for C. burnetii. Transesophageal echocardiography was negative for endocarditis, but 18F-FDG PET/CT showed highly increased 18F-FDG uptake of patient’s native mitral valve (arrows). Patient was treated for almost 2 y with antibiotic therapy because of chronic Q fever endocarditis.
When 18F-FDG PET/CT was added as a major criterion to the Duke criteria, 17 patients (7.2%) had definite endocarditis. In Table 5, the modified Duke criteria were compared with the Duke criteria including 18F-FDG PET/CT as a major criterion by a 2-tailed Wilcoxon test, which showed a significant difference in the number of patients with proven endocarditis (P = 0.008). Of the 8 patients who had a diagnosis of definite endocarditis based on the 18F-FDG PET/CT result, 5 had a positive PCR on blood, 2 had a valve prosthesis, and 6 had no other infectious foci. Of these 8 patients, 2 were originally diagnosed with possible endocarditis and 6 with rejected endocarditis according to the modified Duke criteria.
Comparison of 18F-FDG PET/CT to Modified Duke Criteria for Diagnosing Endocarditis
18F-FDG PET/CT and Treatment Modification
At diagnosis, after a negative PCR result on blood or tissue was obtained, 18F-FDG PET/CT contributed to a change in diagnosis in 31 patients (13.5%). In all these patients, the diagnosis of probable chronic Q fever was changed to proven chronic Q fever. At diagnosis, 18F-FDG PET/CT contributed to treatment modification in 45 patients (19.6%). In 37 patients (16.1%), 18F-FDG PET/CT led to a start of antibiotic treatment, and in 2 patients (0.9%), antibiotic treatment was changed. In 6 patients (2.6%), the 18F-FDG PET/CT result led to surgical intervention.
At follow-up, 18F-FDG PET/CT performed to make a decision on stopping antibiotic treatment was negative in 31 patients (72.1%) and suggested ongoing infectious foci in 12 patients (27.9%). Of the 175 follow-up 18F-FDG PET/CT scans performed because of suspected new complications, 84 (48.0%) were negative. Of all follow-up 18F-FDG PET/CT scans, 125 (57.3%) led to treatment modification, 21 (9.6%) led to discontinuation of antibiotic treatment (Fig. 3), and 7 (3.2%) led to a change in antibiotic treatment. In 97 scans (44.5%), the result of 18F-FDG PET/CT contributed to the decision to continue antibiotic treatment. In 6 patients (3.4%), 18F-FDG PET/CT led also to surgical intervention.
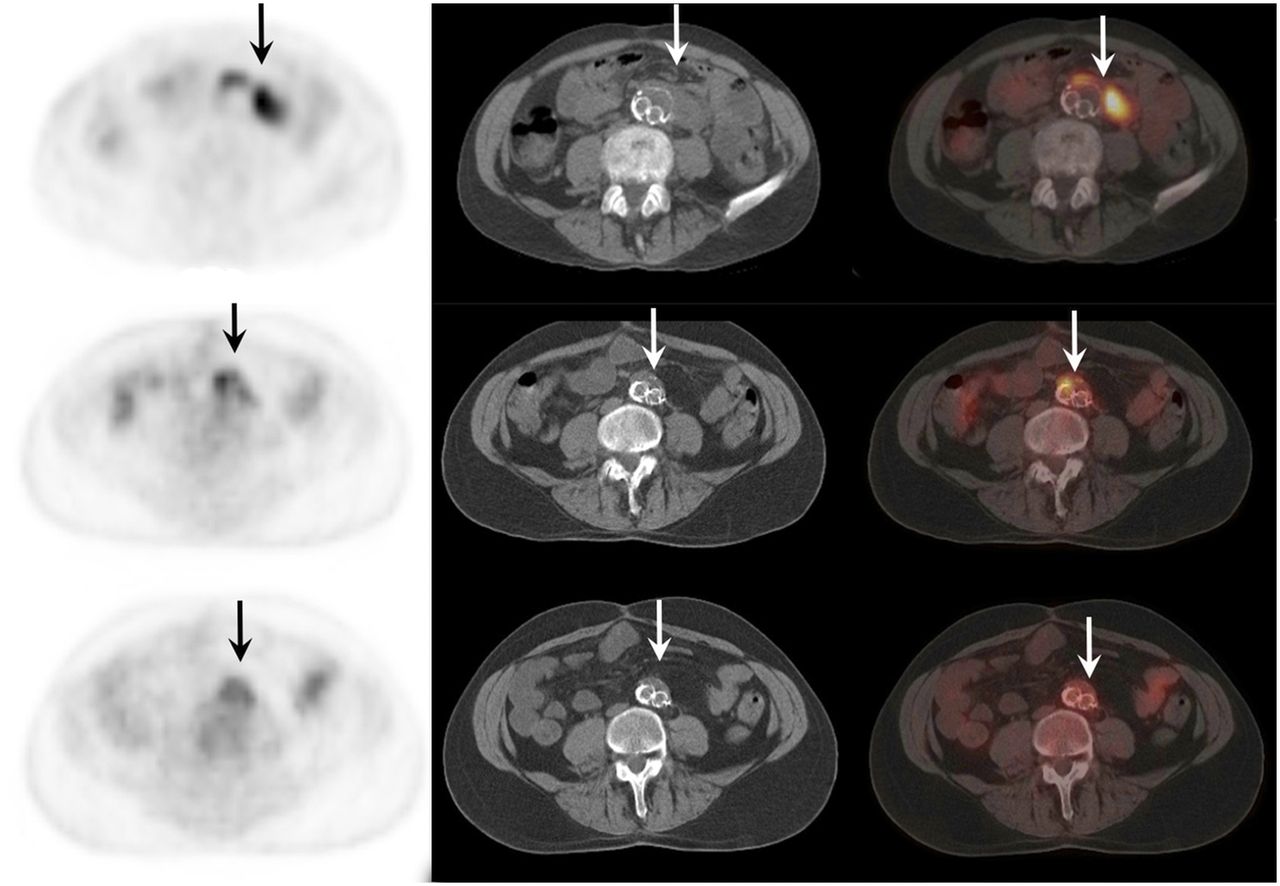
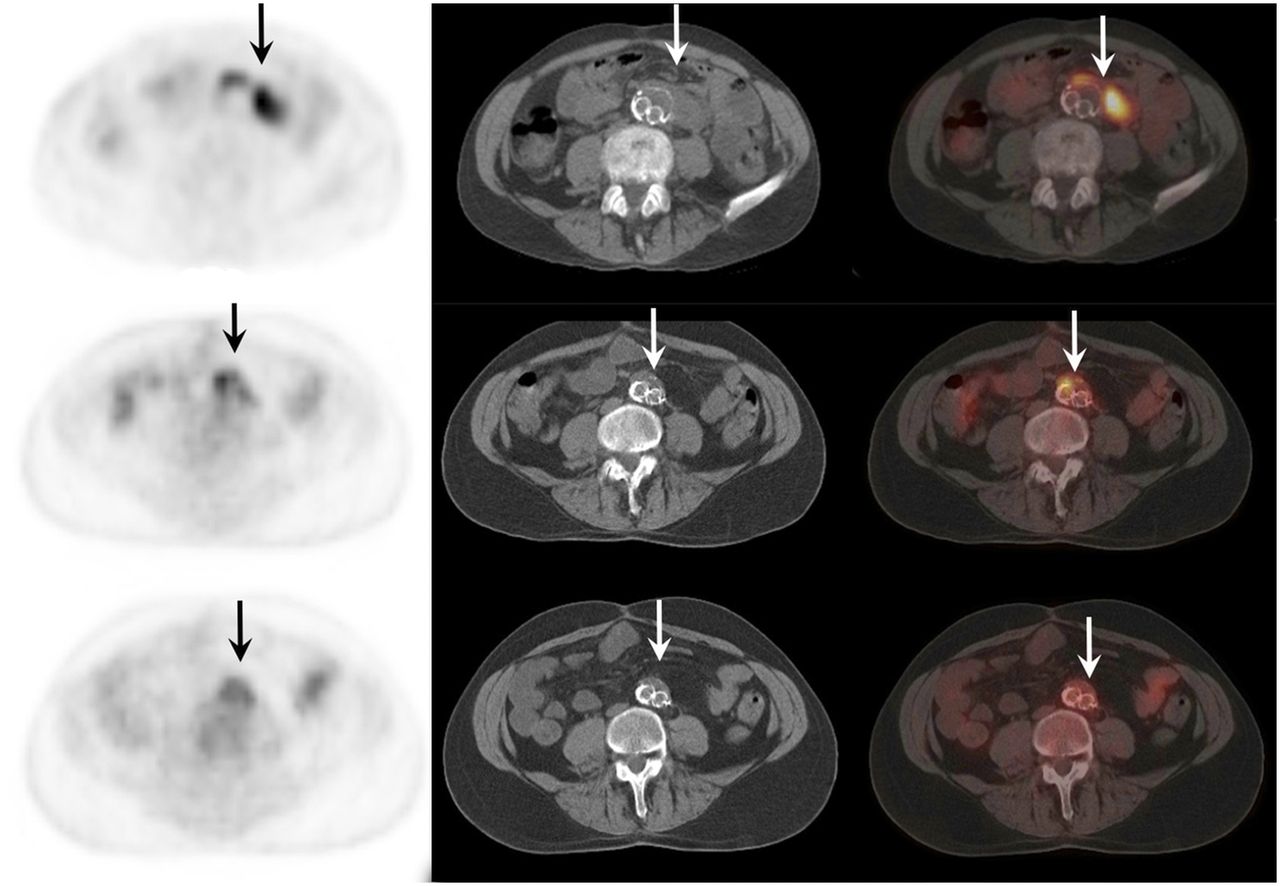
18F-FDG PET/CT scan of 64-y-old man with proven chronic Q fever, infected aneurysm, and infected vascular graft in aorta (arrows). Upper scan shows vascular infection before initiation of antibiotic treatment with doxycycline and hydroxychloroquine. Middle scan shows same area after 1 y of treatment. Lower scan, obtained 2 y after start of treatment, no longer shows vascular infection and therefore antibiotic treatment was discontinued. Four years later, patient died because of septic cholangitis. Autopsy did not show any Q fever foci, and PCR on several tissues, including aorta, was negative for C. burnetii.
DISCUSSION
In this study, we investigated the value of 18F-FDG PET/CT in diagnosis and during follow-up in patients with chronic Q fever. Specific guidelines on when to perform 18F-FDG PET/CT are lacking. Because of the largest Q fever outbreak ever reported in The Netherlands, between 2007 and 2010, it was possible to analyze the value of 18F-FDG PET/CT in a large cohort of 273 patients with chronic Q fever.
The results of our study show that 18F-FDG PET/CT is a valuable diagnostic technique, with a contribution to the diagnosis of chronic Q fever in 13.5% of patients after serology and PCR have already been performed. In follow-up of chronic Q fever, 18F-FDG PET/CT performed for decision making in stopping antibiotic treatment showed persisting focal infection in 27.9%, although patients had low serologic titers and were asymptomatic. This result emphasizes the importance of 18F-FDG PET/CT in follow-up of chronic Q fever. 18F-FDG PET/CT is also valuable for decision making in treatment of chronic Q fever patients, with treatment modification in 19.6% at diagnosis and 57.3% during follow-up. Moreover, 18F-FDG PET/CT provided important prognostic information on patient survival.
Several case reports indicated that 18F-FDG PET/CT could be valuable in diagnosing chronic Q fever (16–18). One study on a screening program in patients with chronic Q fever reported that 18F-FDG PET/CT showed vascular infection in 5 of 10 patients (19). In a retrospective study on 52 patients with chronic Q fever, 18F-FDG PET/CT was performed on 13 of 18 patients with proven chronic Q fever and was helpful in 77%, showing 7 infected vascular prostheses and 3 infected aneurysms (13). Recently, a Dutch study reported that 18F-FDG PET/CT showed a vascular infection in 6 of 13 patients with proven chronic Q fever based on positive PCR for C. burnetii and known aneurysm or vascular prosthesis (14).
Very recently, Eldin et al. (20) reported on a case series of 99 patients with abnormalities seen on 18F-FDG PET/CT performed after diagnosis of both acute and chronic Q fever. 18F-FDG PET/CT contributed to a change in diagnosis in 62.6% of patients. Limitations of the study of Eldin et al. are the fact that only 18F-FDG PET/CT scans showing signs of infection were included and that no central reevaluation of 18F-FDG PET/CT scans was performed. Also, because both acute and chronic Q fever patients were included in the study of Eldin et al., a comparison with our study is difficult. Furthermore, the change in diagnosis in 62.6% of patients was based only on a new abnormality seen on 18F-FDG PET/CT; it is not clear whether these abnormalities were Q fever foci, because the exact clinical context of the patients was not mentioned.
In vascular chronic Q fever infection, a structured protocol for assessment of 18F-FDG PET/CT is lacking. Also, noninfected vascular prostheses may show increased 18F-FDG uptake due to postsurgical inflammation (21,22). In our study, we used a structured grading score for prospective reevaluation of the 18F-FDG PET/CT scans, which is a modified adaptation of scoring systems used in other studies on vascular infection (12,22). The value of this score as shown in Table 2 was endorsed by the fact that patients with grade 1 or 2 had no vascular infection in 97.9% and a significantly lower Q fever–related mortality rate. Our score shows that a homogeneous uptake pattern does not exclude vascular infection, especially when the surrounding tissue is involved, and also considering the high amount of positive PCR on vascular tissue in this group. It is important that interpretation of 18F-FDG PET/CT be multidisciplinary and based on the individual clinical context.
In prosthetic valve endocarditis (not caused by Q fever), the diagnostic value of 18F-FDG PET/CT has been investigated and shown promising results (23). Recently, 18F-FDG PET/CT was added to the European Society of Cardiology modified diagnostic criteria as a major criterion for prosthetic valve endocarditis (10). The sensitivity of 18F-FDG PET/CT in diagnosing native valve endocarditis is not optimal (8,9). In chronic Q fever endocarditis, vegetations are small and often not seen on echocardiography (24). As endocardial involvement seen on echocardiography is a major criterion of the modified Duke criteria, many patients with chronic Q fever endocarditis are missed using these criteria. Therefore, a high antiphase I IgG titer was added earlier to the modified Duke criteria as a major criterion (24). Our study showed that adding increased 18F-FDG valve uptake as a major criterion to the modified Duke criteria led to a 1.9-fold increase in diagnoses of proven endocarditis. Thus, adding 18F-FDG PET/CT to the modified Duke criteria for diagnosing chronic Q fever endocarditis could be a valuable improvement since missed diagnoses have always been expected in this disease.
Potential limitations of our study are the fact that only chronic Q fever patients who underwent 18F-FDG PET/CT were included. This criterion could lead to selection bias, as patients with early death were not included in the study. Also, the lack of additional clinical context in reevaluation of 18F-FDG PET/CT could have led to less sensitive readings.
CONCLUSION
18F-FDG PET/CT is valuable in chronic Q fever. This imaging technique should be performed at diagnosis, as well as being considered during follow-up when new complications are suspected or before the end of treatment when the first 18F-FDG PET/CT scan had abnormal results. Scans should be interpreted using a structured protocol. The addition of 18F-FDG PET/CT to the modified Duke criteria in patients with chronic Q fever can be valuable.
DISCLOSURE
This work was supported by a grant from Q-Support (UMCN140926-00), a Dutch foundation for support of Q fever research and patients. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the following physicians and institutes treating chronic Q fever patients for their cooperation in this study: Shahan Shamelian, internal medicine specialist at Jeroen Bosch Hospital in ’s-Hertogenbosch, The Netherlands; Nicole H.M. Renders, medical microbiologist at Jeroen Bosch Hospital in ’s-Hertogenbosch, The Netherlands; Yvonne E.P. Soethoudt, infectious diseases specialist at Elkerliek Hospital in Helmond, The Netherlands; Brian S.N. Blank, infectious diseases specialist at Maxima Medical Center in Veldhoven, The Netherlands; Dirk Posthouwer, infectious diseases specialist at Maastricht University Medical Center in Maastricht, The Netherlands; Corine Delsing, infectious diseases specialist at Medisch Spectrum Twente Hospital in Enschede, The Netherlands; Jan-Jelrik Oosterheert, infectious diseases specialist at University Medical Center Utrecht in Utrecht, The Netherlands; Sanjay U.C. Sankatsing, infectious diseases specialist at Diakonessenhuis Hospital in Utrecht, The Netherlands.
Footnotes
Published online May 25, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 27, 2017.
- Accepted for publication May 22, 2017.





{kind=link}
{kind=link}
{kind=link}