


Abstract
The supraclavicular region is a common site for lymph node metastases. A commonly reported type of nonmalignant 18F-FDG uptake on PET imaging in the supraclavicular region is “muscle uptake” purportedly due to muscle contraction in tense patients during the 18F-FDG uptake phase. PET/CT offers the unique opportunity to correlate PET findings with CT anatomy in the supraclavicular region. Methods: Images from the first 359 consecutive clinical whole-body studies (in 347 patients) using 18F-FDG and a PET/CT scanner (with CT attenuation correction and ordered-subsets expectation maximization [OSEM] reconstruction) were retrospectively reviewed. The supraclavicular region was evaluated for the presence of abnormal uptake on PET images, and the corresponding CT findings were assessed. Three distinct patterns of abnormal 18F-FDG uptake were noted: pattern A (uptake localizing to supraclavicular area fat [USA-fat], i.e., without corresponding lymph node or muscle uptake on CT), pattern B (uptake localizing to muscle on CT), and pattern C (uptake localizing to lymph nodes or soft-tissue masses on CT). Results: Forty-nine patients (14.1%) (32 female, 17 male; mean age, 51.4 ± 15.6 y; age range, 12–77 y) showed abnormal 18F-FDG uptake in the supraclavicular region. Twenty patients (5.8%) had muscle uptake (group B); 15 (4.3%) had definite abnormal lymph nodes (group C). However, 14 patients (4.0%) had USA-fat (group A) and foci of very low Hounsfield units on CT. These foci were also present on 68Ge attenuation-corrected images (when obtained) and non-attenuation-corrected images. Uptake in USA-fat was typically bilateral and symmetric, intense, more often multifocal than linear, and located in fat on PET/CT. Age was not significantly different for group C versus the 2 other groups. Intensity; mean standardized uptake value, lean (SUVL MEAN); or maximum standardized uptake value, lean (SUVL MAX), did not allow differentiation between patterns A and C (P > 0.05). Standardized uptake values (SUVL MAX, 3.1; SUVL MEAN, 2.1) were significantly lower in group B than in the 2 other groups (P < 0.005). Conclusion: So-called muscle uptake in the supraclavicular region may be caused in a significant proportion of cases by an unrelated process we call the USA-fat finding, with 18F-FDG uptake in tissues of low-Hounsfield (fat) density. This finding most likely reflects an underlying nonpathologic process that we hypothesize to be in foci of brown fat. This intense supraclavicular uptake should be recognized and should not be misinterpreted as a malignant metastatic process or as muscle uptake.
The supraclavicular region can be involved by malignancy, commonly by metastatic diseases to lymph nodes. Lymphoma and cancers of the esophagus, stomach, lung, and breast commonly affect the supraclavicular region. Other nonmalignant conditions, inflammatory or infectious, can cause pathologic supraclavicular lymph node involvement as well.
18F-FDG PET is well suited to the evaluation of malignant involvement in the supraclavicular region. The typical appearance of a malignant lymph node on 18F-FDG PET images is a round focus of intense metabolic activity that can be single, multiple, or bilateral and is sometimes accompanied by other distant abnormal foci of uptake. Nonpathologic supraclavicular uptake is well known and often attributed to muscle uptake. Muscle uptake of 18F-FDG is a well-known cause of findings on PET imaging (1,2) and is a potential cause of false-positive findings on images of patients with cancer (3,4). Uptake can affect virtually all muscles. It is increased by increased endogenous or exogenous insulin, recent muscle activity (voluntary or not), and clinical orthopedic conditions. Segregating pathologic from normal variant 18F-FDG uptake can sometimes be challenging (5). The use of muscle relaxants and sedatives such as diazepam has been proposed to reduce such uptake. However, in some patients imaged with PET/CT, we observed that 18F-FDG activity in the supraclavicular area did not have a corresponding soft-tissue mass or lymph node or muscle uptake on the CT scan.
The recent introduction of PET/CT scanners (6), combining both PET and CT scanning devices, offers a unique opportunity to evaluate how patterns of 18F-FDG uptake in the supraclavicular region relate to CT findings.
MATERIALS AND METHODS
A total of 365 consecutive clinical scans were obtained with PET/CT and 18F-FDG from June to December 2001. Six brain studies were excluded. Of the scans, 359 were obtained using whole-body 18F-FDG imaging on 347 patients (188 male, 159 female; mean age ± SD, 56.6 ± 15 y; age range, 8–92 y). Eleven patients had a total of 12 repeated scans. All whole-body scans were obtained with the Discovery LS PET/CT scanner (General Electric Medical Systems, Waukesha, WI). All patients were referred for oncologic imaging. Patients fasted at least 4 h before the PET acquisition and received an intravenous injection of 555–740 MBq of 18F-FDG. A tracer uptake phase of about 60 min was allowed, during which the patients sat in a quiet injection room without talking. They were allowed to breathe normally during the PET and CT acquisitions. No specific breathing or breath-holding instructions were given to the patients, and scanning was performed during quiet tidal breathing.
CT Scanning
The CT portion of the Discovery LS scanner consists of a multidetector helical CT scanner (LightSpeed Plus; General Electric Medical Systems). The parameters for CT for a typical 5-bed-position acquisition were as follows: 140 kV, 80 mA, 0.8 s per CT rotation, a pitch of 6, a table speed of 22.5 mm/s, a 722.5-mm coverage, a 31.9-s acquisition time, and positioning of patients with their arms at their sides. The CT acquisition was done before the emission acquisition. Images were acquired with the patients positioned the same as for the emission scan by adjusting the table in linear increments. CT data were resized from a 512 × 512 matrix to a 128 × 128 matrix and were smoothed to match the PET data so that the images could be fused and the CT transmission map generated.
68Ge Transmission Scanning
68Ge transmissions scans were used to generate a transmission map. The transmission time for each bed position was 3 min. A segmented attenuation map was then generated. Emission PET images corrected with maps from 68Ge transmission scans were available for 250 patients.
PET Scanning
Emission data was acquired for 5–7 bed positions, typically from the base of the skull through the mid thigh. For patients referred because of melanoma, 2 sets of emission data were acquired, one from the vertex of the head through the mid thigh and another from the mid thigh to the toes. Emission data were acquired for 5 min at each bed position. Each bed had 35 scanning planes, with a 14.6-cm longitudinal field of view and a 1-slice overlap. PET images were reconstructed using CT for attenuation correction with the OSEM algorithm (2 iterations, 28 subsets) and an 8-mm gaussian filter using a 128 × 128 matrix.
Image Analysis
All PET scans were reviewed retrospectively by a single observer who was aware of the clinical data and the findings of other anatomic imaging modalities. All PET images were analyzed on an interactive computer display using commercial fusion software (eNTEGRA; ELGEMS, Haifa, Israel), which allowed review of PET, CT, and fused-image data.
PET images were first assessed visually, using transaxial, sagittal, and coronal displays, for any obviously abnormal foci of increased 18F-FDG uptake in the supraclavicular region. The intensity of uptake relative to the mediastinal blood pool was classified using 4 grades: 0 = no uptake, 1+ = faint uptake, 2+ = moderate uptake, and 3+ = intense uptake. Abnormal uptake was defined as any focus of increased uptake that was clearly grade 1+ or greater. With the fusion software, abnormal-uptake foci of grade 1+ or greater were classified according to their anatomic correlation using 3 patterns: A = uptake with no corresponding abnormal lymph nodes or soft-tissue mass on CT, B = muscle uptake, and C = abnormal uptake in lymph nodes or a soft-tissue mass. Uptake was also classified according to its appearance: focal or linear; unilateral or bilateral.
For each abnormal supraclavicular region, 18F-FDG uptake was evaluated semiquantitatively for the most 18F-FDG-avid abnormal focus using standardized uptake value, lean (SUVL), which represents decay-corrected tissue activity divided by the injected dose per patient lean body weight (as described previously (7)). SUVL was calculated from regions of interest (ROIs) that were placed manually on the maximal area (14-pixel circular area) of 18F-FDG uptake in the focus. Partial-volume effects were not systematically corrected. The maximal pixel value and average ROI value were obtained. The CT-measured density at the maximum focus of 18F-FDG uptake was obtained in Hounsfield units (HU) using the ROI drawn on the PET image superimposed on the CT image.
The CT scans of patients with abnormal supraclavicular uptake were carefully reviewed by an experienced radiologist. The review, limited to both supraclavicular regions, assessed for the presence of lymph nodes on the CT scan. Afterward, both the nuclear medicine physician and the radiologist identified the CT findings corresponding to the 18F-FDG activity (lymph node or soft-tissue mass; muscle or fat) and reached a consensus on the location of 18F-FDG uptake based on PET/CT.
Statistical Analysis
Data are expressed as mean ± SD. The unpaired t test was used to compare uptake intensity, standardized uptake value, age, and body mass index for the 3 patterns of uptake. P < 0.05 was considered statistically significant.
RESULTS
Forty-nine of the 347 patients (14.1%) showed abnormal foci of 18F-FDG uptake in the supraclavicular region. The results are summarized in Table 1.
Patient Characteristics Among the 3 Patterns of Supraclavicular Uptake
USA-Fat (Pattern A)
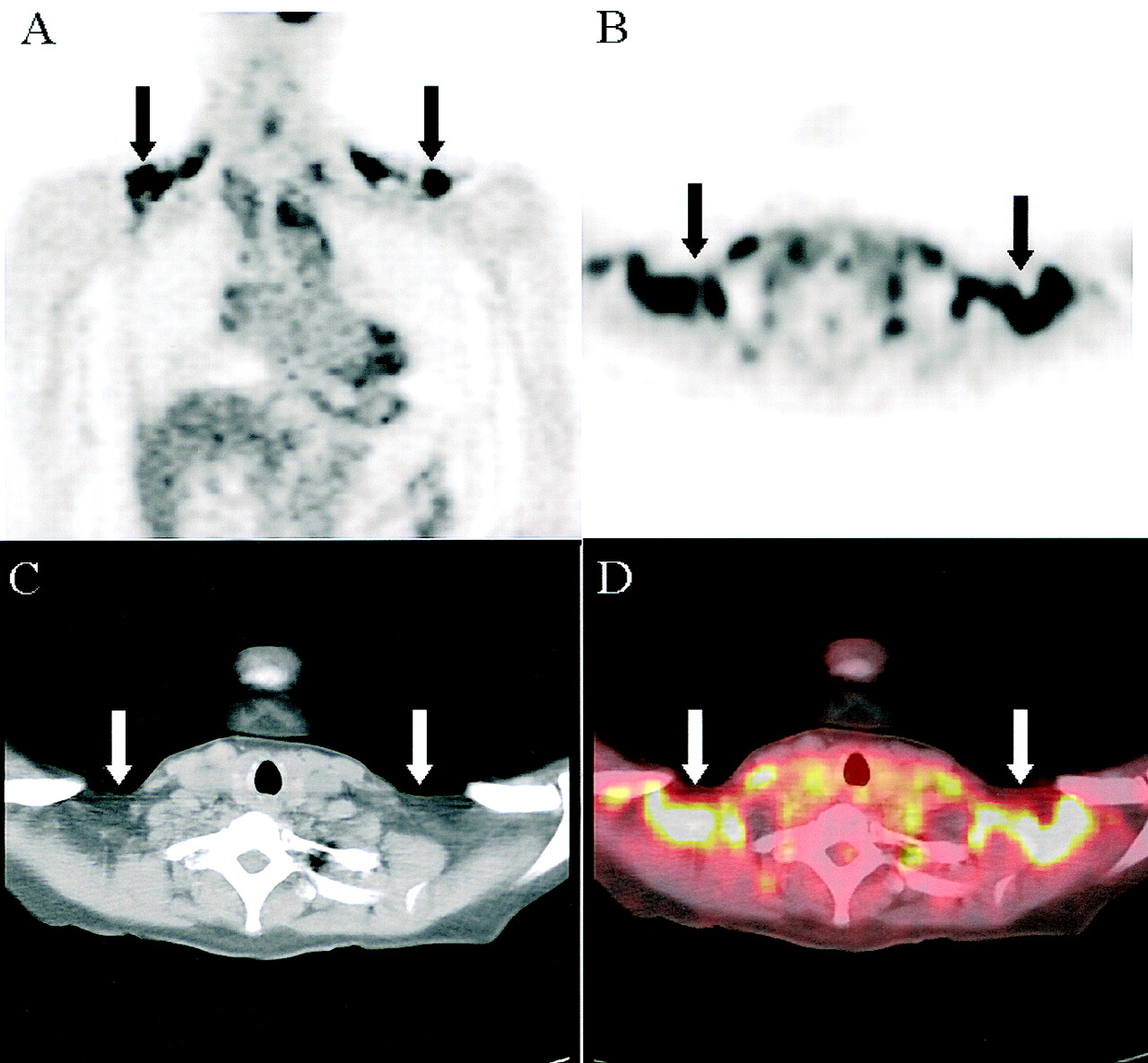
Fourteen patients showed supraclavicular foci of abnormally increased 18F-FDG uptake without any corresponding abnormalities of soft-tissue density on CT images (Fig. 1). This activity was present on both CT-corrected and 68Ge-corrected images. This represents 28.6% of patients with abnormal uptake, or 4.0% of total patients, 12 female and 2 male. Mean age was 50.7 ± 15 y (age range, 12–68 y). The mean body mass index of patients with this finding was 24.2 ± 7. In total, 28 abnormal supraclavicular regions were found. The CT density of the lesions was −75.9 ± 24 HU, consistent with fat. The uptake was bilateral in all patients (Fig. 1) and was symmetric in all but 4 patients. Two of these patients had slightly asymmetric uptake, and 2 had markedly asymmetric but still bilateral uptake. A large area of tracer uptake was seen in 12 patients, of whom 4 had a linear component. It was mainly linear, without a clear focus, in 1 patient and was focal in another patient. In this latter patient, PET/CT allowed differentiation from muscle or lymph node uptake.
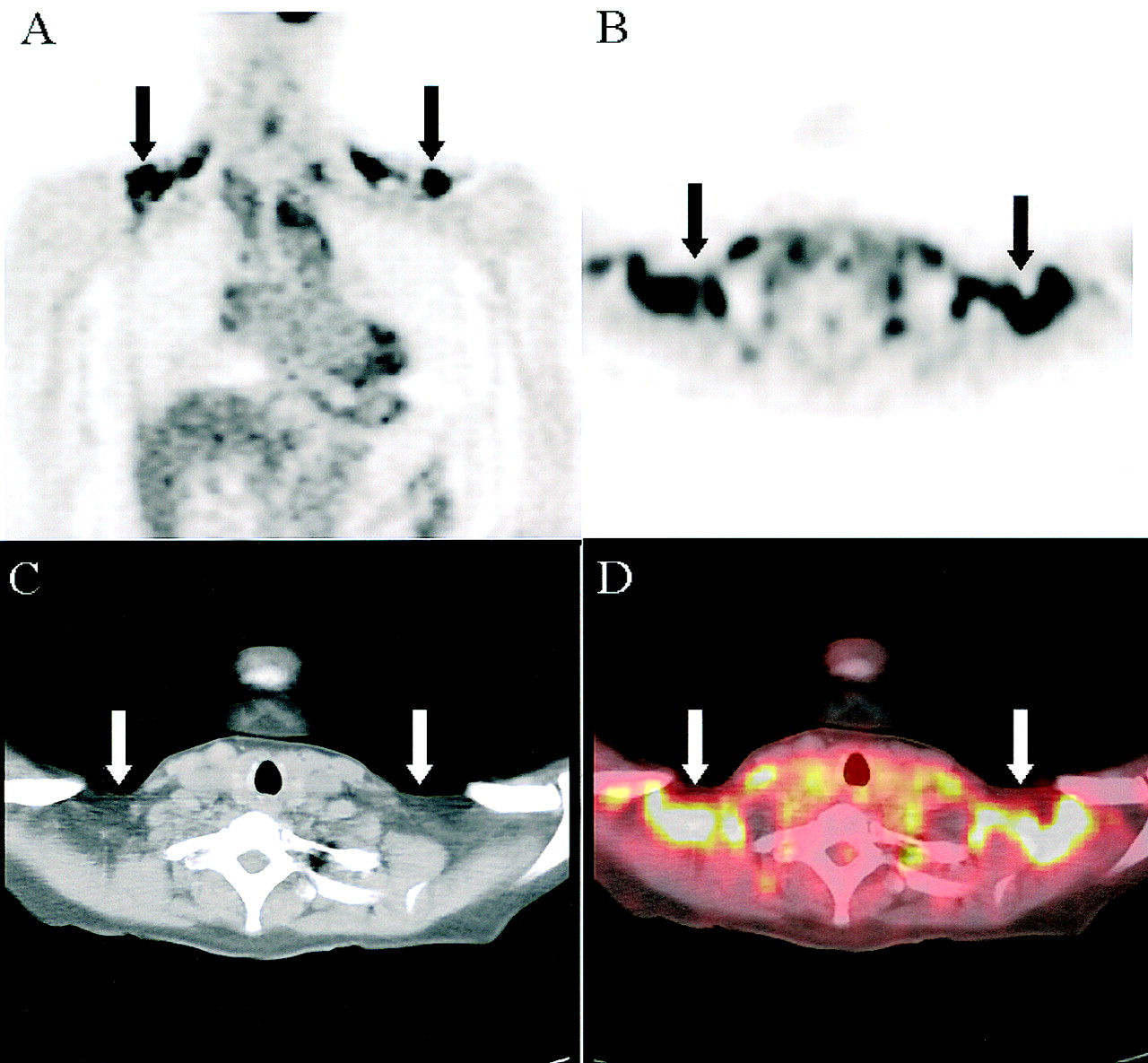
Pattern A: USA-fat. A 59-y-old woman with endometrial carcinoma evaluated after chemotherapy. (A and B) PET images in coronal (A) and transverse (B) planes show bilateral intense uptake in both supraclavicular regions (arrows). (C) Corresponding CT scan shows no abnormal lymph node or muscle uptake in supraclavicular region (arrows). (D) 18F-FDG uptake appears to fuse predominantly into fat (arrows); hence, finding is described as uptake in supraclavicular area fat (USA-fat).
Uptake was intense in 10 patients, moderate to intense in 3 patients, and mild to moderate in 1 patient, the patient with a small region of focal uptake. The intensity of tracer uptake was 2.79 ± 0.4 on a semiquantitative scale (0–3). In 3 patients, coexisting muscle uptake was found. Muscle uptake was linear and easily distinguishable from the supraclavicular artifact (USA-fat).
All patients but 1 had known cancer. One patient had lung nodules that were most likely benign. Maximum SUVL (SUVL MAX) of the USA-fat was 7.1 ± 4 (range, 2.08–17.35), and mean SUVL (SUVL MEAN) was 4.8 ± 3 (range, 1.43–12.44). Review of the CT portion of the PET/CT scan showed no supraclavicular lymphadenopathy in 13 patients. In 1 patient, a small lymph node was noted in the supraclavicular region, without corresponding increased 18F-FDG activity. In all 14 patients, PET supraclavicular activity clearly localized into fatty tissue. In 10 of the 14 patients, PET showed active metabolic lesions suggestive of active cancer in other locations.
Follow-up, albeit of limited duration, was available for USA-fat patients. No pathologic involvement of the supraclavicular region was clinically demonstrated. Of the 10 patients who were followed up, 9 had positive PET findings elsewhere in the body. Six of these 9 patients underwent chemotherapy, 1 underwent surgery and was scheduled to receive chemotherapy, 1 had suspected recurrent ovarian cancer but no cancer revealed by surgery, and 1 had suspected recurrent thyroid cancer but was followed up before additional treatment. Two patients had no active disease during the follow-up. All patients with gynecologic cancers were postmenopausal.
Muscle Uptake (Pattern B)
Twenty patients showed abnormal foci of 18F-FDG uptake corresponding to muscle on the CT scan (Fig. 2). This represents 40.8% of patients with abnormal uptake, or 5.8% of total patients, 15 female and 5 male. Mean age was 54.7 ± 17 y (age range, 18–77 y). The mean body mass index of patients with this finding was 23 ± 5. All but 1 patient had a history of cancer. In total, 34 abnormal regions were found. Uptake was typically bilateral (13 symmetric and 1 asymmetric) but was unilateral in 6 cases. Uptake was linear in 14 patients, but with some foci in 6 patients. Uptake was mild or mild to moderate in 8 patients, moderate in 8 patients, and moderate to intense or intense in 4 patients. The intensity of uptake was 1.66 ± 0.5 on a semiquantitative scale. SUVL MAX was 3.1 ± 1 (range, 1.45–6.17), and SUVL MEAN was 2.1 ± 0.7 (range, 1.03–3.82). The density of the muscles on CT was 31.9 ± 14 HU.

Pattern B: muscle uptake. A 57-y-old woman with history of mediastinal adenocarcinoma from unknown primary, who was evaluated after chemotherapy. Coronal and transaxial PET images show linear bilateral uptake with fusion of uptake to corresponding muscle in CT images. Uptake is slightly asymmetric. Display is same as in Figure 1.
Review of the CT portion of the PET/CT scan showed that 1 patient had a lymph node smaller than 1 cm in the supraclavicular region, but without corresponding metabolic activity. In all patients, the metabolic activity fused to muscles. Clinical follow-up was available for 11 patients. On review of patient charts, no mention of active neoplastic involvement of the supraclavicular region was found for these 11 patients.
Lymph Nodes or Soft-Tissue Uptake (Pattern C)
Fifteen patients showed abnormal focal 18F-FDG uptake with corresponding lymph nodes on the CT scan (Fig. 3). This represents 30.6% of patients with abnormal uptake, or 4.3% of total patients, 5 female and 10 male. Mean age was 47.8 ± 15 y (age range, 13–75 y). The mean body mass index of patients with this finding was 27.2 ± 6. All patients had cancer. In total, 19 abnormal regions were identified. Uptake was unilateral in 11 patients and bilateral in 4 (2 symmetric and 2 asymmetric). The pattern was typically focal (5 single and 10 multiple). Uptake was intense in 12 patients and mild to moderate or moderate to intense in the 3 other patients. The intensity of uptake was 2.82 ± 0.4 on a semiquantitative scale (0–3).

Pattern C: supraclavicular lymph nodes. A 28-y-old man with stage II Hodgkin’s disease. Coronal and transverse PET images, CT scan, and fused images show multiple metabolically active foci, which fuse to location of lymph nodes in left supraclavicular region. Coronal images show mediastinal involvement. Display is same as in Figure 1.
SUVL MAX was 9.0 ± 5 (range, 1.92–21.83), and SUVL MEAN was 5.9 ± 4 (range, 1.29–16.64). The density of the lymph nodes and soft-tissue masses was 29.8 ± 12 HU. CT review showed that all activity was projected in lymph nodes or soft-tissue masses.
Abnormal pathologic uptake was confirmed in 7 of these patients by histopathology (4 biopsies, 3 surgeries). Two patients had no direct pathologic confirmation of the supraclavicular uptake; however, other positive sites underwent biopsy and revealed metastatic disease. One patient with known metastatic melanoma showed extensive metastatic disease including the supraclavicular area. None of the sites underwent biopsy. Five other patients had no confirmatory biopsy.
Comparison of the 3 Groups
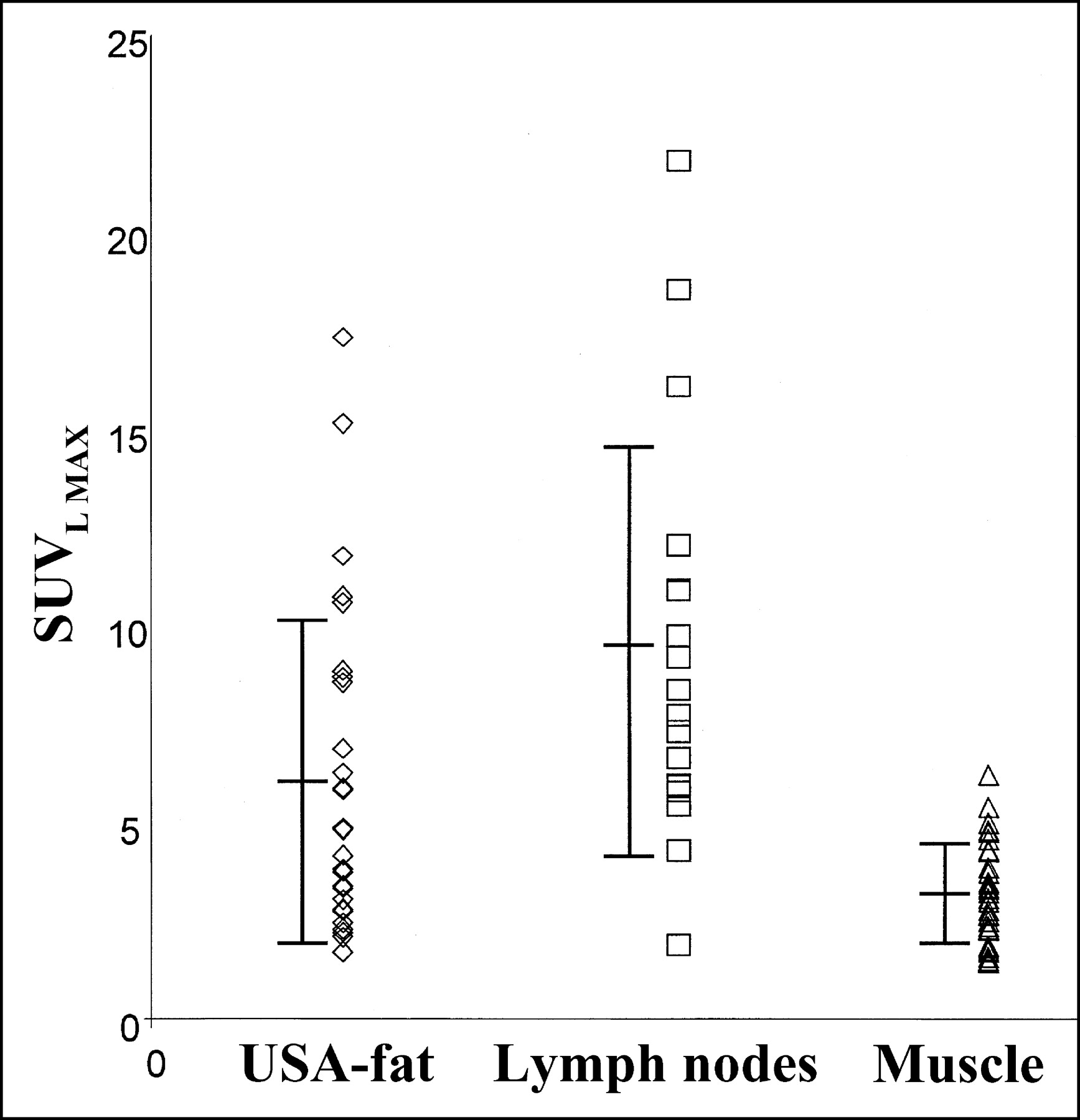
Patient age was not significantly different among the 3 groups of patients (P > 0.05). Body mass index was not significantly different between group A and the 2 other groups (P > 0.05). However, body mass index was different between groups B and C (P = 0.02). The intensity of visual uptake did not allow differentiation between USA-fat and lymph node uptake (P = 0.4), but muscle uptake was significantly lower than USA-fat and lymph node uptake (P < 0.00001). SUVL MAX and SUVL MEAN tended to be higher for lymph nodes than for USA-fat, but the difference was not significant (P > 0.05) (Fig. 4). SUVL MAX and SUVL MEAN were significantly lower for muscle than for the 2 other patterns (P < 0.001). The measured CT density of lesions was not significantly different between the muscle and lymph node patterns (P = 0.28) but was significantly different between these 2 patterns and USA-fat (P < 0.0001) (Fig. 5).

Comparison of SUVL MAX activity among the 3 patterns of uptake (mean ± SD). SUVL MAX is lower in muscle than in USA-fat or lymph nodes.

Comparison of measured density on CT in HU among the 3 patterns of uptake (mean ± SD). CT HU are significantly lower in USA-fat than in lymph nodes or muscle.
DISCUSSION
Abnormal supraclavicular 18F-FDG uptake is not an infrequent finding in 18F-FDG PET imaging (14.1% of patients in this study). Metastases are the most ominous cause for this finding. Muscle uptake is the other usual explanation for most nonpathologic supraclavicular uptake. However, this report clearly shows that for half the instances of non-lymph node uptake, muscle uptake could not be retained as an acceptable explanation. The USA-fat of, to date, unknown etiology but fusing to “fat” in PET/CT was found in 4% of a population referred for oncologic evaluation. It is an important scintigraphic finding to recognize and to avoid confusing with tumor.
PET/CT allowed us to verify that these foci had no corresponding anatomic soft-tissue mass detectable by CT scanning. Rather, the 18F-FDG-avid focus fused to tissues of fat density. The corresponding measured HU were within the reported fat-density range (−150 to −50) (8). It seems improbable that malignant pathologic foci of this intensity and size shown by PET imaging could have no corresponding CT findings. The PET findings could help in recognizing this artifact. The intensity and standardized uptake value were not reliable tools for differentiating among these categories. Muscle uptake was more often linear and mild to moderate in intensity but could be intense, focal, and unilateral. Lymph node uptake was usually round, could be intense, and could be single or multiple. The supraclavicular artifact was more likely to be bilateral and symmetric and usually was intense. The exact etiology of the supraclavicular artifact is unknown. That it is pathologic is highly improbable. No corresponding soft-tissue abnormalities were found in these patients. The CT density corresponding to these foci was that of fat.
Brown-fat benign tumors, “hibernomas,” have been reported in the supraclavicular region (9). However, these lesions are infrequent, with fewer than 100 cases reported in the literature. A recent case report showed intense 18F-FDG uptake in a hibernoma (10). A more likely explanation is that this activity is a reflection of an underlying physiologic process. Our hypothesis is that the uptake reflects the metabolic activity of brown fat. Brown fat has the ability to increase its blood flow with norepinephrine stimulation, has extensive β-adrenergic innervation, and has a high content of mitochondria. In contrast to white fat, which stores energy, the main purpose of brown fat is to produce heat. This heat production is caused by an uncoupling protein, which produces heat in opposition to energy storage with adenosine triphosphate production. This tissue is highly metabolically active. Glucose is not the major energy supply for brown fat. However, glucose use by brown fat increases during cold stimulation (11). Glucose transporter 4 is increased in brown fat after exposure to cold (12). Insulin stimulation in rats can drastically increase glucose use by brown fat (13).
Brown fat is present in hibernating rodents and neonates. The typical site of deposition in rodents is interscapular. The presence of brown fat in adult humans is controversial. However, its having been reported in patients with pheochromocytomas (14,15) is perhaps understandable, since adrenergic stimulation causes thermogenesis in brown fat and its hyperplasia. Brown fat has also been reported in other adults on the basis of both general necropsy studies (16) and necropsy studies of outdoor workers who were exposed to the cold (17), in patients who died from chronic congestive heart failure (18), and in perirenal fat from donors operated on for nonmalignant conditions (19). Brown-fat-deprived mice are genetically prone to obesity. Our study did not show that USA-fat patients were leaner than the 2 other groups of patients. Activation of brown fat has been suggested as an explanation for cancer-induced cachexia (20). A study in rats showed that tumor necrosis factor increased the thermogenic activity of brown adipose tissue by stimulating sympathetic outflow to it (21). However, another study showed that tumor necrosis factor induced insulin resistance in fetal brown adipocytes in culture, decreased insulin-stimulated glucose uptake, but upregulated uncoupling protein gene expression (22). Ten of the 14 patients with USA-fat had active cancer according to PET imaging.
We observed a high female-to-male ratio (6:1) in the USA-fat group. In cold-exposed rats, the increase in glucose use by brown fat was less in adult male rats than in female rats because of the smaller amount of brown fat in older male rats (23). Female rats had an increased mass of brown fat with increasing age, whereas male rats showed a decreased mass (24). Female rats in a postcafeteria period (model of dietary obesity) showed a greater loss of body weight and a higher activation of thermogenic brown fat with increased expression of uncoupling proteins (25). Aged women have been reported to maintain higher rectal temperatures during exposure to cold than have men of similar age (26).
The in vivo demonstration of brown fat using noninvasive methods is difficult. The present study did not conclusively show that the activity seen in the supraclavicular area corresponded to brown fat, but on the basis of CT findings the tracer was clearly present in the fat. Two patients had a possible hyperthyroid state (1 patient with thyroid cancer, who is receiving levothyroxine sodium for suppression of thyroid-stimulating hormone, and 1 patient with Graves’ disease, who was treated with 131I therapy a few months before PET and is receiving methimazole). Hyperthyroidism is associated with a hyperadrenergic status.
A potential limitation of this study is that the patients were followed up over only the short term to confirm the benignity of the USA-fat. An additional limitation is that the pathologic etiology was not confirmed for all lymph nodes (pattern C). Increased tracer uptake did correspond to the CT observation of abnormal lymph nodes, almost certainly of inflammatory, infectious, or malignant etiology.
CONCLUSION
Supraclavicular 18F-FDG uptake is quite frequent in a population referred for oncologic PET imaging (14.1% of patients in this study). Uptake in lymph nodes, tumor, or muscle is a common cause, but 18F-FDG PET/CT imaging revealed that 28.6% of abnormal foci of supraclavicular uptake were caused by a previously undescribed finding, USA-fat. USA-fat is characterized by increased 18F-FDG uptake in the supraclavicular region without corresponding muscle or lymph node uptake present on the CT scan and with localization of uptake to fat. The physiologic etiology of this uptake remains unknown but may be related to brown fat. Such uptake should be recognized and not be misinterpreted as pathologic.
Footnotes
Received May 13, 2002; revision accepted Sep. 17, 2002.
For correspondence or reprints contact: Richard L. Wahl, MD, Division of Nuclear Medicine, The Russell H. Morgan Department of Radiology and Radiological Sciences, The Johns Hopkins Hospital, 601 N. Caroline St., Room 3223, Baltimore, MD 21287-0817.
E-mail: Rwahl{at}jhmi.edu
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Brown Adipose Tissue: A Protective Mechanism Against "Preprediabetes"?
- Perspectives on Brown Adipose Tissue Imaging: Insights from Preclinical and Clinical Observations from the Last and Current Century
- Repeatability of Radiomic Features of Brown Adipose Tissue
- Assessing PET Parameters in Oncologic 18F-FDG Studies
- Brown Adipose Tissue is Associated with Improved Cardiometabolic Health and Regulates Blood Pressure
- Assessment of the aging of the brown adipose tissue by 18F-FDG PET/CT imaging in the progeria mouse model LmnaG609G/G609G
- Brown adipocyte glucose metabolism: a heated subject
- Measurement of Brown Adipose Tissue Activity Using Microwave Radiometry and 18F-FDG PET/CT
- The Gift of Light: Using Multiplexed Optical Imaging to Probe Cardiac Metabolism in Health and Disease
- The significance of beige and brown fat in humans
- Pediatric Brown Adipose Tissue on 18F-FDG PET: Diazepam Intervention
- Supraclavicular Brown Adipose Tissue 18F-FDG Uptake and Cardiovascular Disease
- Increased Energy Expenditure, Ucp1 Expression, and Resistance to Diet-induced Obesity in Mice Lacking Nuclear Factor-Erythroid-2-related Transcription Factor-2 (Nrf2)
- Quantification of Human and Rodent Brown Adipose Tissue Function Using 99mTc-Methoxyisobutylisonitrile SPECT/CT and 18F-FDG PET/CT
- Assessment of incidental and clinically unsuspected fluorodeoxyglucose-avid foci detected on oncological positron emission tomography/CT
- Brown adipose tissue: development, metabolism and beyond
- Anatomical Locations of Human Brown Adipose Tissue: Functional Relevance and Implications in Obesity and Type 2 Diabetes
- Stability in Brain Glucose Metabolism Following Brown Adipose Tissue Inactivation in Chinese Adults
- Brown Adipose Tissue: Mechanisms and Potential Therapeutic Targets
- Thermal Control of Brown Adipose Tissue in 18F-FDG PET
- The adipose organ of obesity-prone C57BL/6J mice is composed of mixed white and brown adipocytes
- 18F-Fluorobenzyl Triphenyl Phosphonium: A Noninvasive Sensor of Brown Adipose Tissue Thermogenesis
- Restaging: Should We PERCIST Without Pattern Recognition?
- Prevention of Brown Adipose Tissue Activation in 18F-FDG PET/CT of Breast Cancer Patients Receiving Neoadjuvant Systemic Therapy
- CT Hounsfield Units of Brown Adipose Tissue Increase with Activation: Preclinical and Clinical Studies
- Hybrid SPECT-CT and PET-CT imaging of differentiated thyroid carcinoma
- A novel approach for reduction of brown fat uptake on FDG PET
- High Incidence of Metabolically Active Brown Adipose Tissue in Healthy Adult Humans: Effects of Cold Exposure and Adiposity
- Preliminary PET/CT Study of 18F-FDG Uptake in Cervical and Supraclavicular Brown Adipose Tissue
- Visualization of Brown Adipose Tissue with 99mTc-Methoxyisobutylisonitrile on SPECT/CT
- Presence of Specific 11C-meta-Hydroxyephedrine Retention in Heart, Lung, Pancreas, and Brown Adipose Tissue
- Comparison of Uptake of Multiple Clinical Radiotracers into Brown Adipose Tissue Under Cold-Stimulated and Nonstimulated Conditions
- Brown Fat Imaging with 18F-6-Fluorodopamine PET/CT, 18F-FDG PET/CT, and 123I-MIBG SPECT: A Study of Patients Being Evaluated for Pheochromocytoma
- Integrating PET and PET/CT into the Risk-Adapted Therapy of Lymphoma
- Prevalence and Patterns of Physiologic Muscle Uptake Detected with Whole-Body 18F-FDG PET.
- 18F-FDG Imaging: Pitfalls and Artifacts
- Extensive Skeletal Muscle Uptake of 18F-FDG: Relation to Immunosuppressants?
- Intense 18F-FDG Uptake in Brown Fat Can Be Reduced Pharmacologically
- Brown Adipose Tissue and Nuclear Medicine Imaging
- Tetraphenylphosphonium as a Novel Molecular Probe for Imaging Tumors
- 18F-FLT PET for Visualization of Laryngeal Cancer: Comparison with 18F-FDG PET
- PET/CT in Oncology: Integration into Clinical Management of Lymphoma, Melanoma, and Gastrointestinal Malignancies
- Patterns of 18F-FDG Uptake in Adipose Tissue and Muscle: A Potential Source of False-Positives for PET
- PET/CT in Colorectal Cancer
- Visualization of Interscapular Brown Adipose Tissue Using 99mTc-Tetrofosmin in Pediatric Patients
- 123I-Metaiodobenzylguanidine Uptake in the Nape of the Neck of Children: Likely Visualization of Brown Adipose Tissue
- "USA-Fat": Prevalence Is Related to Ambient Outdoor Temperature--Evaluation with 18F-FDG PET/CT