


Abstract
Preclinical data suggest a negative correlation between brown adipose tissue (BAT) and the degree of coronary atherosclerosis. We sought to evaluate the relationship between 18F-FDG uptake in supraclavicular BAT in relation to arterial inflammation and subsequent cardiovascular disease (CVD) events in humans. Methods: Individuals who underwent 18F-FDG PET/CT for clinical indications but who did not have either cancer or known atherosclerotic disease at the time of imaging were included. A radiologist masked to clinical data measured 18F-FDG uptake within BAT (in the supraclavicular region) as well as in subcutaneous adipose tissues. Tissue density was evaluated using CT (Hounsfield units). Arterial inflammation was assessed by measuring arterial 18F-FDG uptake and calculating target-to-background ratio. CVD events were independently adjudicated by masked cardiologists. Thereafter, the relationship between BAT activity and CVD events was evaluated. Results: A total of 443 patients (age, 55 y [44–66 y]; 44% men; body mass index [BMI], 26 [range, 23–31]) were included, and 30 patients experienced a cardiovascular event during a median follow-up of 4 y. BAT activity negatively correlated with arterial inflammation (r = −0.178, P < 0.01), a relationship that persisted after correcting for age and BMI (r = −0.147, P < 0.01). When either high sensitivity or high accuracy thresholds (from receiver-operating curve analyses) were used to define elevated BAT, high BAT was associated with a reduced risk of CVD events (P = 0.048), even after correcting for age (P = 0.037). Conclusion: Our results suggest that increased supraclavicular BAT activity is inversely associated with arterial inflammation, independently of age and BMI. Additionally, increased BAT may be associated with fewer cardiovascular events.
Brown adipose tissue (BAT) is primarily observed in young children and regresses with increasing age (1). Several studies found a high incidence of metabolically active BAT in the supraclavicular and paraspinal regions in adults, an observation that is accentuated after cold activation (2–7). Studies furthermore suggest that BAT activation is associated with improved regulation of energy expenditure. Further evidence for a role of BAT in energy metabolism is that BAT activation is associated with improved whole-body glucose homeostasis and heightened insulin sensitivity (8). BAT activity may also have a beneficial impact on atherosclerosis, which is a chronic inflammatory condition (9). A postmortem study in humans (10) demonstrated a negative correlation between BAT and coronary atherosclerosis (as luminal narrowing). Thus, we hypothesized that supraclavicular BAT might play an important protective role against atherosclerosis.
The combination of PET and CT (PET/CT) allows for the identification of BAT, because BAT demonstrates high 18F-FDG uptake on PET and CT allows for the identification of fat tissue using Hounsfield units (HU) (11,12). Moreover, 18F-FDG uptake in the aortic wall can be used as a reliable imaging biomarker of inflammation in atherosclerotic plaques (13). Hence, the aim of this study was to evaluate the relation between 18F-FDG uptake in supraclavicular BAT and arterial inflammation in humans using PET/CT imaging. As a secondary aim, we sought to evaluate the relation between supraclavicular BAT uptake and subsequent cardiovascular events.
MATERIALS AND METHODS
In this retrospective observational study, participants who underwent PET/CT imaging for clinical reasons at the Massachusetts General Hospital between 2005 and 2008 were included. Predefined inclusion criteria were the absence of prior cancer diagnosis or clinical remission of cancer throughout the follow-up period, age 30 y or older, the absence of known cardiovascular disease at the time of imaging, and the absence of inflammatory or autoimmune disease or use of chronic antiinflammatory therapy. Additionally, to ensure adequacy of follow-up clinical information, the study participants had to have at least 3 subsequent medical visit notes spanning more than 1 y. The study protocol was approved by the local institutional review board; informed consent was waived because of the study’s retrospective nature.
18F-FDG PET/CT Imaging
18F-FDG PET/CT imaging was performed using previously described and validated methods (14). All subjects fasted for at least 8 h before intravenous 18F-FDG injection (∼370 MBq for a 70-kg patient). PET/CT images were acquired approximately 60–90 min after 18F-FDG injection, on a Biograph 64 scanner (Siemens Healthcare).
18F-FDG PET/CT Image Analysis
The images were analyzed by masked interpreters at a core laboratory using TrueD (MMWP VE40A; Siemens Healthcare), using previously described methods (14). 18F-FDG uptake was measured within the wall of the ascending aorta in the axial plane from 1 cm above the origin of coronary vessels and up to the bottom of the aortic arch in 5-mm increments. Arterial 18F-FDG uptake was recorded as the mean of SUVmax of all slices. For background correction, SUVmean was measured in the superior vena cava. Arterial target-to-background ratio (TBR) was calculated as aortic SUVmax divided by venous blood SUV. The predictive role of arterial inflammation in this cohort was evaluated in a previous publication (15).
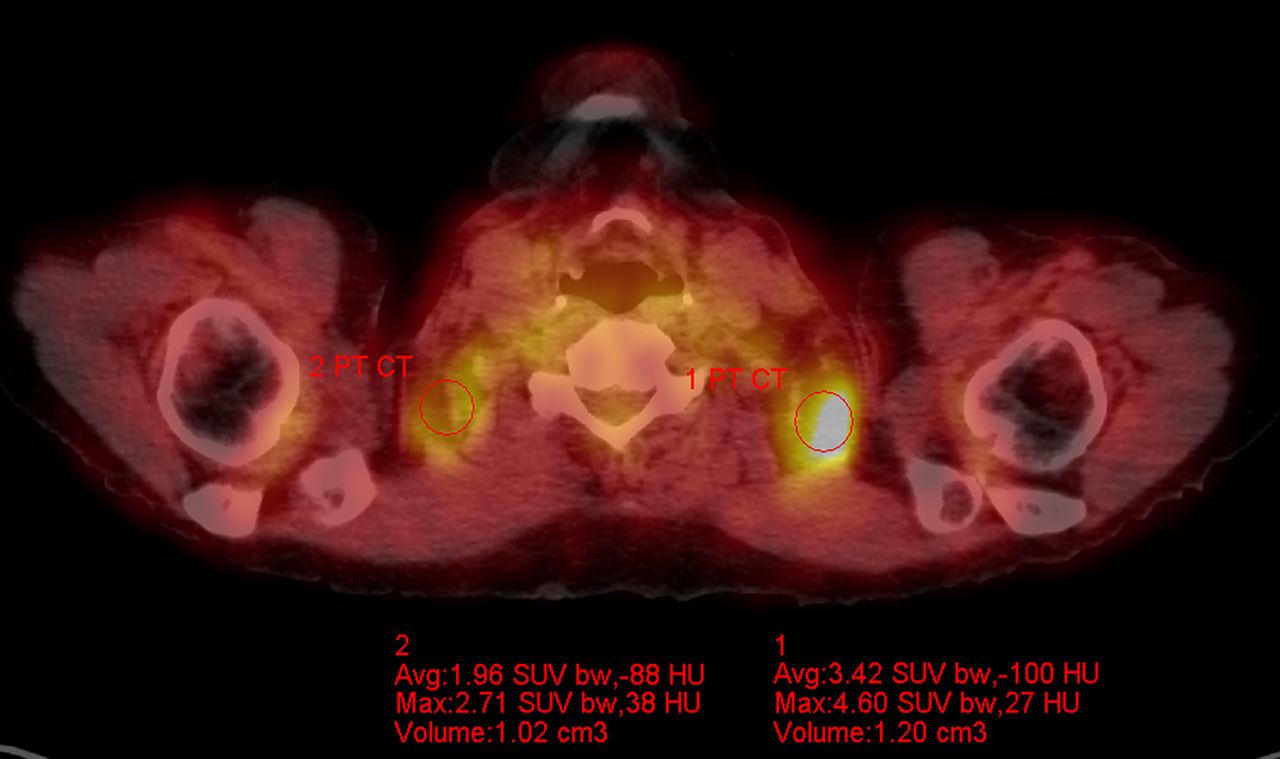
BAT 18F-FDG activity was quantified by an experienced radiologist within the supraclavicular region as previously described by Cohade et al. (11). First, the right and left supraclavicular fossae were identified and the supraclavicular fat depots (wherein BAT resides) were identified using CT density information (−250 to −50 HU, Fig. 1) (16). Subsequently, a region of interest was placed within the supraclavicular fossae adipose depots, and the SUV data were recorded. The average of the mean BAT SUV was calculated as the average of the bilateral recorded BAT SUVmean. The average HU values for supraclavicular BAT were recorded simultaneously with the SUVs. As a control fat tissue, 18F-FDG uptake was measured in the subcutaneous adipose tissue (SAT SUV).
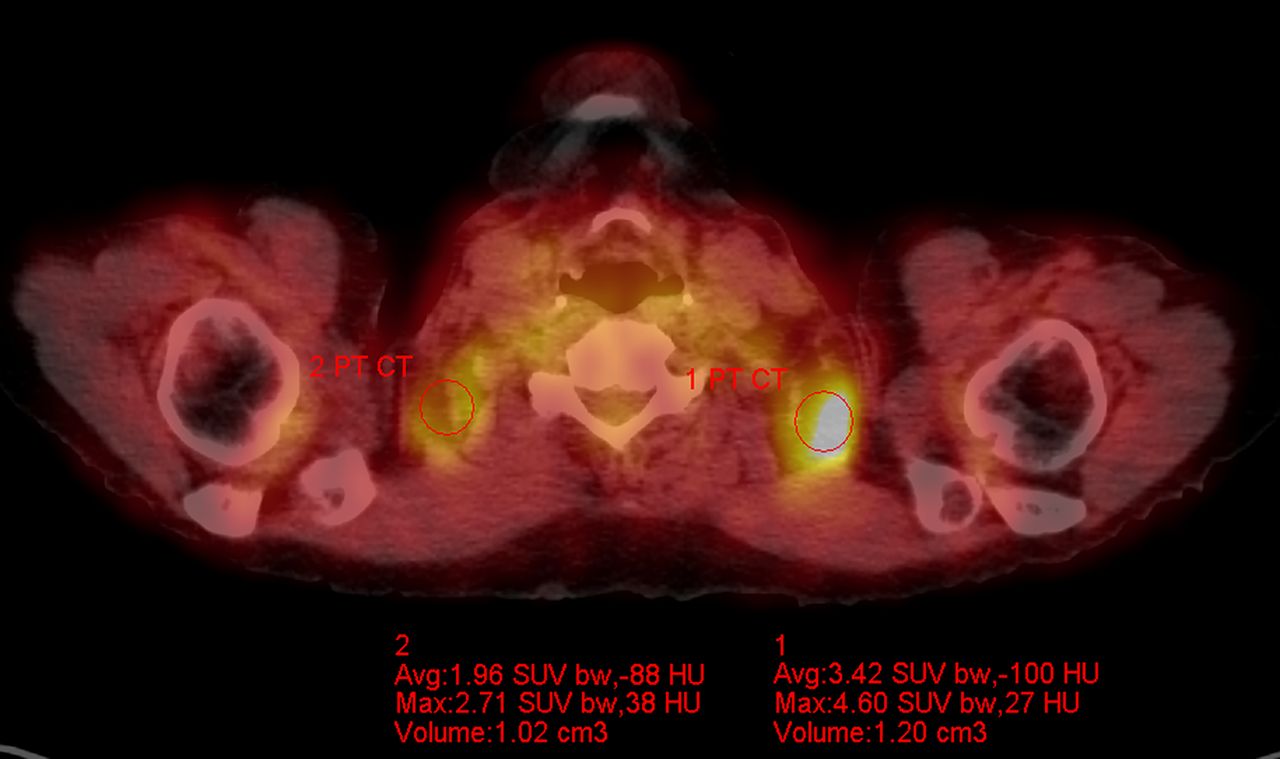
Measurement of BAT uptake. Supraclavicular fat was identified using CT density thresholds (HU −50 to −250). BAT 18F-FDG uptake was assessed by manually drawing region of interest within supraclavicular fat in axial plane. SUVmean was recorded bilaterally.
In adult humans imaged under ambient conditions, the incidence of BAT activation, if defined using the classic criterion of an SUV greater than 2, is low (<2% of cases) (17). Because such a definition of activated BAT would severely limit power for analyses, we sought alternative methods to describe relative BAT activation in our population. Thus, we defined relative BAT activation using 2 main methods. The first method to define relative BAT activation that was used measured absolute BAT SUV. The second method to define relative BAT activation used a ratio of BAT SUV to SAT SUV. For each method, we identified 2 separate thresholds to identify high BAT activity: a threshold derived using the receiver-operating curve (ROC) to determine the lowest value associated with 100% sensitivity to detect cardiovascular disease (CVD) events, and a threshold derived using the ROC curve to determine the value associated with highest accuracy. Of the 4 resultant thresholds to define activated BAT, we prospectively chose the absolute BAT SUV associated with 100% sensitivity for the primary analysis.
Cardiovascular Events
CVD events were adjudicated using medical records by 2 independent cardiologists who were masked to all imaging data. Incident cardiovascular events included ischemic stroke or transient ischemic attack, acute coronary syndrome, revascularization (coronary, carotid, or peripheral), unstable angina pectoris, heart failure, and cardiovascular death. For the exact definition of events, we refer to the online supplement of a previous publication (18).
Statistical Analysis
Continuous variables were expressed as mean (±SD), and nonnormally distributed variables were expressed as median (P25, P75). Quantile–quantile plots were evaluated to determine normal distribution. Categoric variables were expressed as frequencies and percentages. To assess for statistically significant differences in continuous variables, the independent-samples Student t test was applied. Levene’s test was used to assess the equality of variances for a variable. In the case of nonnormal distribution, the Mann–Whitney U test was used. Univariate associations were evaluated using Pearson correlation coefficients. ROC curves and areas under the curve were generated to determine cut-points. Kaplan–Meier estimates of free cardiovascular events of patients were calculated, and the log-rank test was applied to test for statistical significance. P values were 2-sided, and a P value of 0.05 was considered statistically significant. Statistical analyses were performed using SPSS (version 22; IBM) and R version 3.12 combined with the package survival (R Foundation for Statistical Computing).
RESULTS
We were able to measure BAT activity in 443 subjects; patient demographics are shown in Table 1.
Baseline Characteristics of Study Subjects
Cardiovascular Outcomes
The median follow-up period was 3.7 y, and 30 patients experienced an incidental cardiovascular event. Nine developed acute coronary syndrome, 4 underwent coronary revascularization, 6 experienced a stroke, 2 had a transient ischemic attack, 1 underwent carotid revascularization, 5 had new-onset angina pectoris, 2 were diagnosed with peripheral artery disease and underwent peripheral revascularization, and 1 experienced cardiovascular death.
BAT Metabolic Activity Versus Arterial Inflammation
BAT metabolic activity (SUV) negatively correlated with arterial inflammation (arterial TBR), age, and body mass index (BMI) (Figs. 2A–2C). Further, BAT SUV was significantly higher in women than in men (Fig. 3). The relationship between BAT SUV and arterial inflammation remained significant after controlling for age and BMI (r = −0.147, P = 0.002), as well as for sex (r = −0.148, P = 0.002). Additionally, BAT SUV modestly correlated with BAT CT density (HU, Fig. 2D). Generally similar correlations were observed when the BAT-to-SAT ratio was substituted for the absolute BAT SUV (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
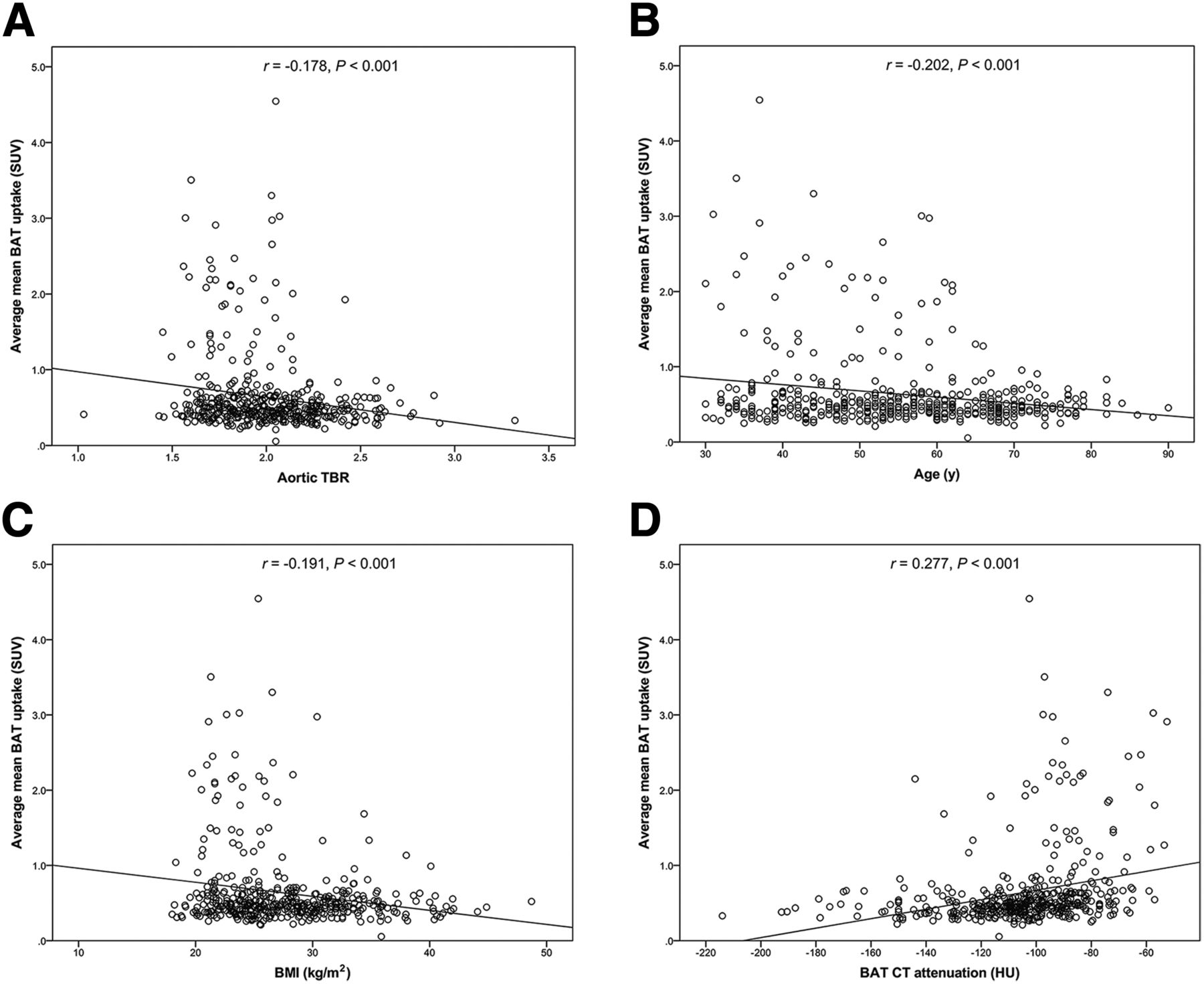
Scatterplot between average mean BAT uptake and aortic TBR (A), age (B), BMI (C), and CT assessment (HU) of BAT (D).
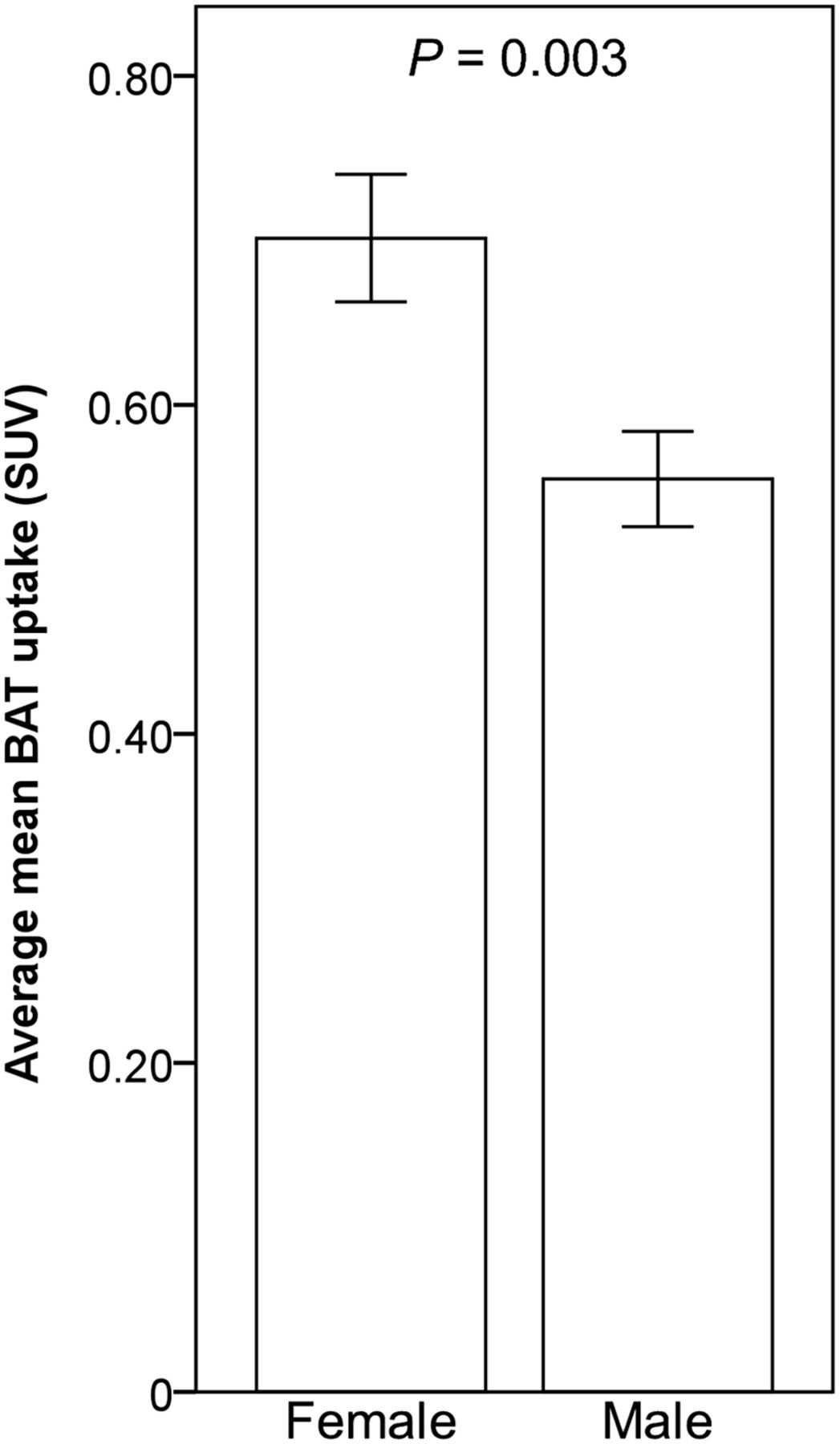
Bar plot comparing average mean BAT uptake in women and men. Error bars represent ±SE.
BAT Metabolic Activity Versus CVD Events
BAT metabolic activity (SUV) was lower in individuals who subsequently experienced a cardiovascular event (0.65 ± 0.55 vs. 0.51 ± 0.14, P < 0.001, Table 2). Similarly, the BAT–to–SAT activity ratio was also lower in those who subsequently experienced a cardiovascular event (3.89 ± 3.41 vs. 3.04 ± 1.29, P = 0.004). In contrast, there was no difference in SAT SUV between patients with and without a CVD event (Table 2).
18F-FDG Uptake
BAT Uptake and Event-Free Survival
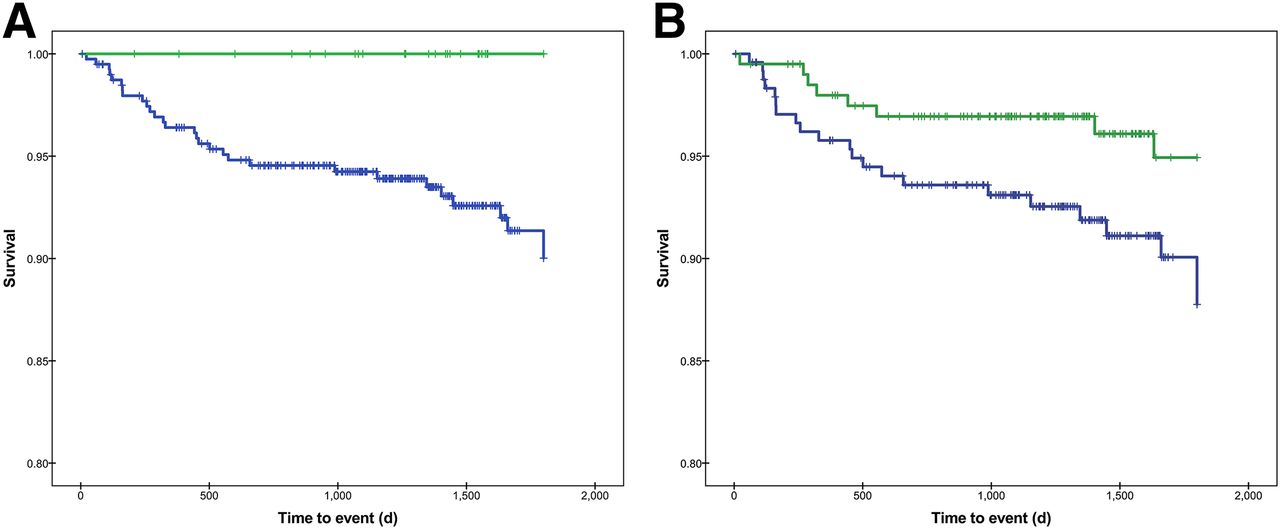
The relationship between BAT activation and events was evaluated using 4 separate thresholds to define activated BAT (Table 3). The prospectively defined primary analysis defined activated BAT according to the lowest BAT SUV that identified 100% of individuals who experienced a CVD event (a BAT SUV of > 1.0) (Fig. 4). Using that threshold, we observed significantly greater arterial inflammation in those with lower BAT metabolic activity (TBR, 2.02 ± 0.29 vs. 1.84 ± 0.20, P < 0.001). Moreover, individuals with lower BAT metabolic activity had more CVD events during the subsequent follow-up period (Fig. 5A). These differences in survival remained significant after correcting for BMI, though became nonsignificant after correcting for age. However, when a high-accuracy threshold to define activated BAT was used, the inverse relationship between BAT SUV and events remained significant even after correcting for age (Table 3). Similar inverse relationships between BAT activation and events were observed when BAT activity was assessed in relation to SAT activity (using BAT-to-SAT ratios; Table 3; Fig. 5B).
BAT Activation Versus Events
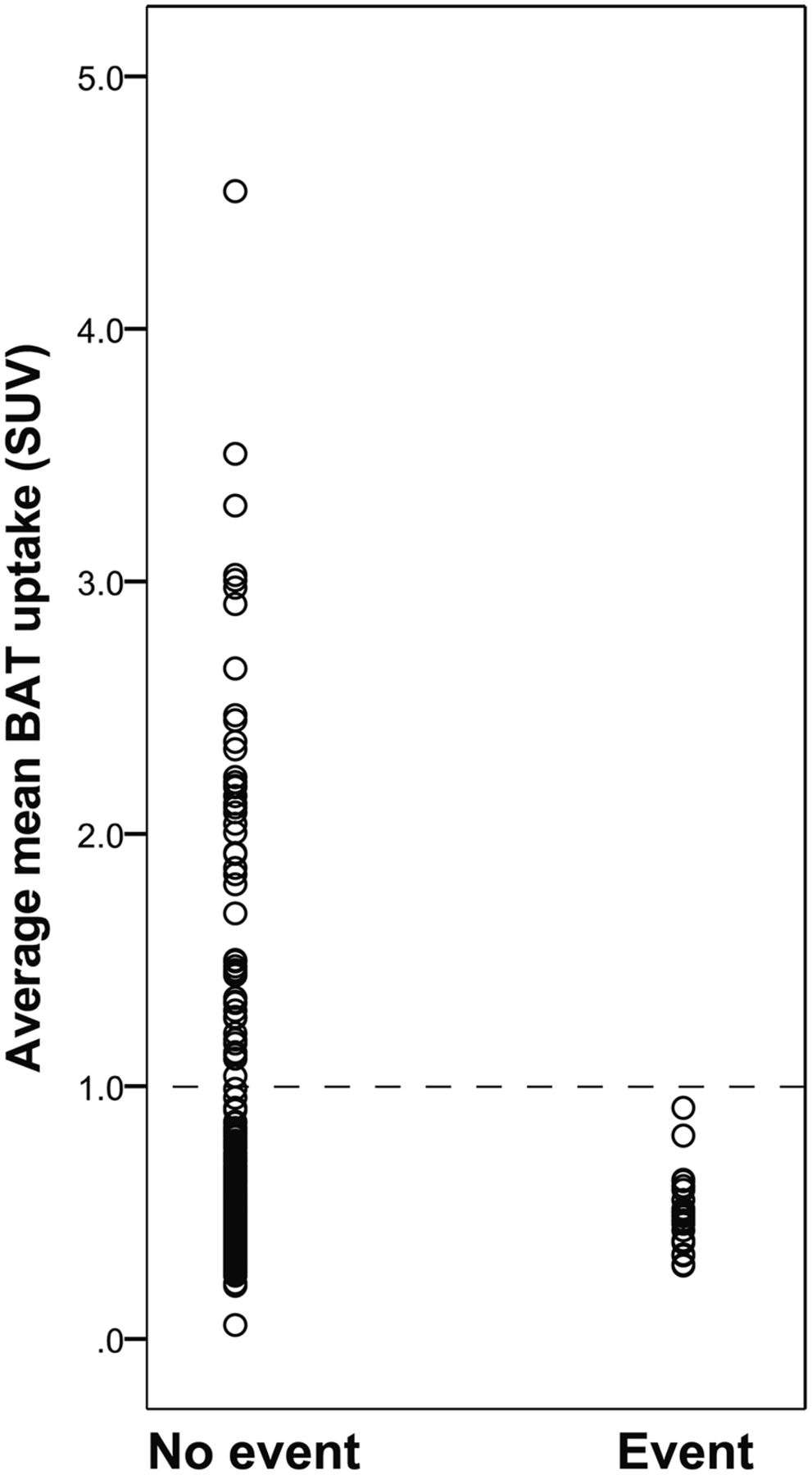
Scatterplot in average mean BAT SUV and cardiovascular event.
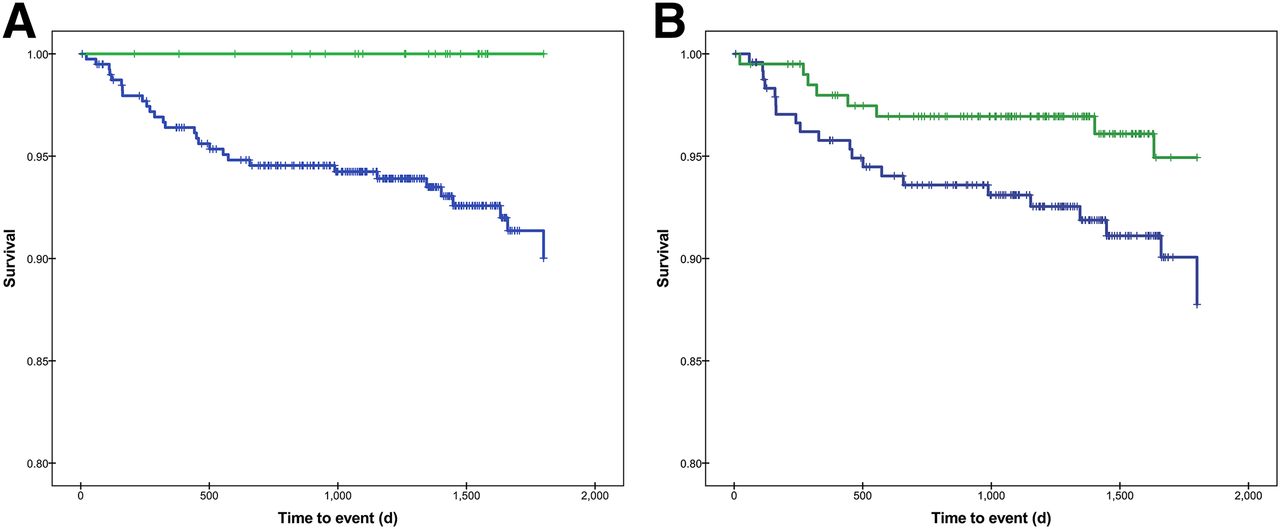
Kaplan–Meier plot displaying proportion free of CVD events in individuals with vs. without BAT activation. (A) Activated BAT was identified using threshold BAT SUV of 1.0. (B) Activated BAT was identified as a BAT SUV that had 3 times activity of SAT SUV. When either definition was used, individuals with activated BAT (green) had fewer CVD events than those without activated BAT (blue).
DISCUSSION
To our knowledge, our study is the first to evaluate the relation between BAT activity, arterial inflammation, and CVD events. We found that BAT was moderately, inversely associated with arterial inflammation independent of age and BMI. Furthermore, we observed that cardiovascular events were more frequent in patients with low BAT activity. Our data suggest that BAT activity is inversely associated with arterial inflammation and that a high BAT activity may be predictive for subsequent CVD events.
BAT is an active metabolic organ and potentially plays an important role in the basal metabolic rate and inflammation (19,20). Atherosclerosis is a chronic inflammatory disorder characterized by an accumulation of lipids, collagen, foam macrophages, and proliferated smooth muscle cells (21–23). 18F-FDG PET allows for the quantification of arterial inflammation and improves CVD risk prediction beyond traditional clinical risk prediction models (e.g., Framingham Risk Score) (15). In this study, we observed a modest inverse relationship between BAT activity and arterial inflammation. Given that PET/CT measures of arterial inflammation have repeatedly been shown to predict CVD events (13,15,24), we hypothesized that BAT activation would also be associated with CVD events. Indeed, we observed that in individuals who experienced CVD events, arterial 18F-FDG uptake was higher whereas BAT uptake was significantly lower. Further, no events were observed in subjects with high BAT activity, raising the possibility that BAT could have an important role in vasoprotection.
The relationship between BAT activity and CVD events became nonsignificant in the primary analysis after correcting for age. However, on secondary analyses, using a different threshold for BAT activation, we found that BAT activity remained significantly inversely associated with CVD events even after adjusting for age. Moreover, we observed a robust inverse association between BAT activity and arterial inflammation, which persisted after correcting for age and other covariates. Taken together, the observations support the hypothesis that BAT activation is cardioprotective.
In many previous studies, the identification of BAT is further facilitated through cold stimulation (which provokes BAT thermogenesis and increases BAT 18F-FDG uptake) (3,4,25). In our study, however, patients were imaged under ambient conditions; cold stimulation was not performed, because of the retrospective design of the study. Hence, it is important to consider the results of this study under this light. Nonetheless, unstimulated BAT might yield important information regarding its potential antiatherogenic impact. Notably, BAT presumably exists primarily in its unstimulated state (in the absence of cold provocation), hence evaluation of BAT under ambient conditions might provide insights into the more typical metabolic state of that tissue. Thus, unstimulated BAT activity may even better reflect the salutary contributions of that tissue on long-term health. Future studies will need to compare the value of cold-activated measures with ambient BAT measures for predicting its atheroprotective impact. Other limitations also deserve mention. The study consisted primarily of patients who had a prior history of treated cancer, which may hamper the generalizability of our results. Also, we did not adjust for the effect of β-blockers, which could reduce BAT activity (26).
Although the findings of this study underscore a link between BAT activation and better cardiovascular health, the data do not denote causation and indeed several important questions remain. Among them, although BAT activity can be increased pharmacologically (27) or through cold exposure (28), it is not clear if modulation of BAT activity will translate to improved CVD outcomes. Further, consistent with previous research (24), we also found that BAT activity tends to be lower in elderly subjects. It is unknown to what degree BAT activity can be upregulated in older adults, in whom its potentially protective effects are needed the most. Consistent with prior research, we observed higher BAT activity in women (2,16). Though the mechanisms underlying this observed difference are unclear, it is possible that sex hormones play a role (29).
CONCLUSION
The study demonstrates that supraclavicular BAT activity is inversely associated with arterial inflammation (independent of age and BMI). Furthermore, we observed that higher BAT activity is associated with significantly fewer CVD events and that no cardiovascular events occurred in individuals with a high BAT activity. These observations provide support for the concept that BAT activation may be associated with better cardiovascular health.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 21, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 26, 2015.
- Accepted for publication December 7, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}