


Abstract
Brown adipose tissue (BAT) is retained into adulthood in some patients. It has been imaged using several radiopharmaceuticals, including 18F-FDG. Using SPECT/CT, we assessed whether and how frequently uptake of 99mTc-methoxyisobutylisonitrile (99mTc-MIBI) was present in expected locations of BAT. Methods: A total of 205 SPECT/CT scans using 99mTc-MIBI for parathyroid imaging were reviewed for the presence of 99mTc-MIBI uptake in expected locations of BAT. Results: We detected 99mTc-MIBI uptake in BAT in 13 of 205 patients (6.3%). When BAT was visualized, it was detected on both early and delayed scans. The patients with 99mTc-MIBI uptake in BAT were younger than the patients with no 99mTc-MIBI uptake (P = 0.044). Conclusion: Uptake of 99mTc-MIBI in BAT is relatively common in this adult patient population and should not be confused with 99mTc-MIBI-avid–tumors. SPECT/CT can be useful for defining such tracer uptake as a normal physiologic variant.
Brown adipose tissue (BAT) is metabolically active in some adults and can cause inaccurate diagnoses on several types of nuclear scans because of substantial tracer uptake, which can be confused with or mask disease. Previously, BAT has been visualized by PET using 18F-FDG (1,2), and by single-photon imaging using 123I-metaiodobenzylguanidine (3,4) or 99mTc-tetrofosmin (5) in humans. 99mTc-methoxyisobutylisonitrile (99mTc-MIBI) is widely used for many imaging applications, most notably for both cardiac and parathyroid imaging. To our knowledge, there have been 2 case reports (6,7) describing the possible uptake of 99mTc-MIBI into brown fat in humans. Studies in rodents show clearly an increased uptake of 99mTc-MIBI into BAT relative to background blood levels (8). Thorough examination of a 99mTc-MIBI scan of the heart or parathyroid glands includes assessment of the visualized body to exclude incidental incremental tumor involvement, which may be 99mTc-MIBI-avid. This is particularly important in instances when 99mTc-MIBI is used for tumor imaging. We suspected that 99mTc-MIBI might accumulate in BAT and evaluated this possibility, reviewing consecutive SPECT/CT scans.
MATERIALS AND METHODS
Patient Population
We retrospectively reviewed scintigrams of consecutive patients who were evaluated for parathyroid adenomas from May 2004 to July 2005, using dual-phase (early and late) planar imaging and SPECT/CT. We identified 205 patients (153 female, 52 male; mean age, 59.7 ± 13.1 y, range, 23–94 y). Our retrospective study was approved by the Institutional Review Board, and informed consent was waived.
Imaging Protocol and Analysis
All patients were injected intravenously with 925–1,110 MBq of 99mTc-MIBI.
Planar Imaging
At 15 min and 2 h after injection, 10-min anterior, 35° right anterior oblique, and 35° left anterior oblique planar images were acquired in a 128 × 128 matrix, with a 20% window centered around the 140-keV photopeak, using a low-energy, high-resolution parallel collimator.
SPECT/CT
Neither oral nor intravenous contrast material was used. Hybrid SPECT/CT images of the neck and chest were obtained on 1 of 2 SPECT/CT systems (Millennium VG Hawkeye; GE Healthcare, or Infinia Hawkeye; GE Healthcare) immediately after planar imaging (at approximately 30 min and 2.5 h after 99mTc-MIBI injection). Both SPECT/CT systems used a step-and-shoot protocol of 25 s/3° for a total of 60 views per camera head. SPECT images were reconstructed on a 128 × 128 matrix. The CT (x-ray tube current, 2.5 mA; voltage, 140 kVp) had a slice thickness of 10 mm with a scan time of approximately 10 min for an average 40-cm field of view. The anonymous SPECT/CT images were reviewed on an imaging workstation (Xeleris; GE Healthcare) by 2 nuclear medicine physicians (2 and >20 y of experience) and qualitatively assessed for the presence or absence of radiotracer uptake in areas known to commonly contain BAT. These areas included the neck, supraclavicular region, mediastinum, and paraspinal tissues. Before we could render a “brown fat present” reading, however, 2 parameters had to be met: the CT image of the expected region had to show fat tissue density and the reviewers had to agree BAT was present or absent. Planar- and SPECT-only images of the patients categorized as having “BAT present” were reviewed also, and the radiotracer distribution was noted. The frequency of BAT visualization was calculated; differences in BAT visualization frequency for age and sex were analyzed using the Student t test and Fisher exact test, respectively.
RESULTS
We detected the presence of 99mTc-MIBI uptake in BAT in 13 of 205 patients (6.3%). When BAT was visualized, it was detected on both early and delayed scans. With fused SPECT/CT images, BAT could be clearly distinguished from muscle, bone, thyroid, parathyroids, myocardium, and other structures in the neck and chest. In 12 patients, 99mTc-MIBI was localized to BAT in the supraclavicular area (Fig. 1). This localization was symmetric in 11 patients and asymmetric in 1 patient. Uptake in the supraclavicular areas was seen on planar- and SPECT-only images, but without CT fusion it was indistinguishable from possible muscle or lymph node uptake. In 6 patients, the supraclavicular area was the only area of 99mTc-MIBI uptake in BAT. In the other 6 patients, different areas of 99mTc-MIBI-avid–BAT were noted. In addition, 2 patients demonstrated further 99mTc-MIBI uptake in the paraspinal areas (Fig. 2). The paraspinal uptake was not noted on planar-only images (likely because the paraspinal areas are posterior) but could be seen on SPECT-only images. Four patients exhibited additional neck uptake of 99mTc-MIBI that fused to areas of BAT on SPECT/CT (symmetric in 3 cases). None of the areas was seen on planar images (likely because intense 99mTc-MIBI uptake in the anterior parotid and salivary glands obscured the more posterior BAT). Although 99mTc-MIBI uptake in the posterior neck could be seen on SPECT-only images, again, a clear association to an anatomic structure (muscle, lymph node, BAT) could not be made. In 1 patient, 99mTc-MIBI uptake was seen solely in the region of the interatrial septa fusing to an area of fat density, possibly representing lipomatous hypertrophy of the interatrial septum (LHIS) (Fig. 3). Both planar- and SPECT-only images showed a mediastinal focus of 99mTc-MIBI uptake.

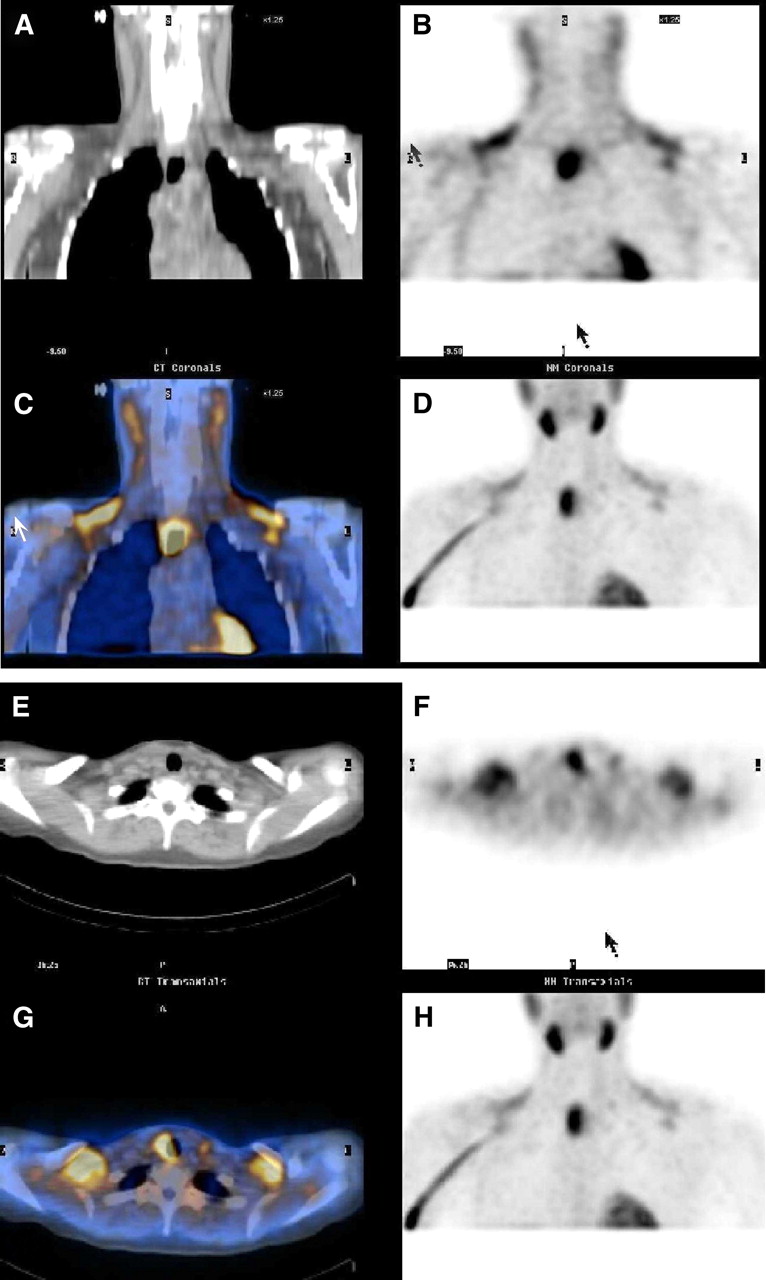
Scans performed on a 26-y-old woman with primary hyperparathyroidism with supraclavicular BAT in addition to right superior mediastinal parathyroid adenoma (confirmed at time of surgery). 99mTc-MIBI uptake seen on SPECT clearly fuses to BAT. Selected coronal (A–D) and transaxial (E–H) slices of CT (A and E), SPECT (B and F), fused SPECT/CT (C and G), and maximum-intensity projection (MIP) (D and H) using 99mTc-MIBI.
Early coronal slices of CT (A), SPECT (B), fused SPECT/CT (C), and maximum-intensity projection (MIP) (D) of a 60-y-old woman with primary hyperparathyroidism. 99mTc-MIBI–avid BAT is seen in the supraclavicular area (MIP) and in the paraspinal area (MIP, SPECT/CT).

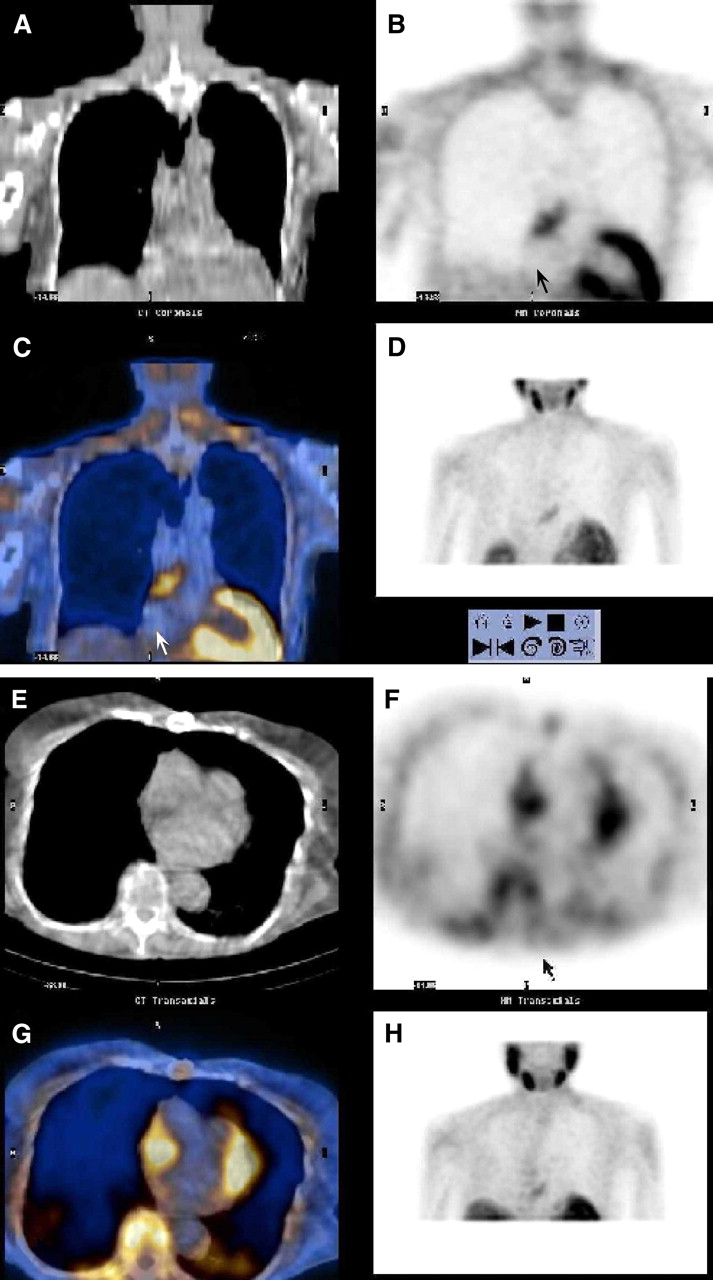
Scans performed on an 84-y-old woman with primary hyperparathyroidism. 99mTc-MIBI uptake fusing to fat in the area of the interatrial septum possibly represents LHIS. Selected coronal (A–D) and transaxial (E–H) slices of CT (A and E), SPECT (B and F), fused SPECT/CT (C and G), and maximum-intensity projection (MIP) (D, H).
The patients with 99mTc-MIBI uptake in BAT were significantly younger (mean age, 50.5 ± 19.1 y, range, 23–84 y) than the patients with no 99mTc-MIBI uptake (mean age, 60.4 ± 12.4 y, range, 28–94 y [t test, P = 0.044]). Although the percentage of female patients with BAT detection was higher (11/153 patients; 7.2%) than that of the male population (2/52 patients; 3.8%), this difference was not statistically significant (P = 0.52).
DISCUSSION
BAT is a metabolically active tissue and, on the basis of our study, often actively accumulates 99mTc-MIBI. BAT that has been localized with 99mTc-MIBI should not be confused with disease, such as abnormal uptake in lymph nodes, tumors, thyroid cancer, parathyroid adenomas, or muscle. Although there are reports of 99mTc-MIBI uptake in BAT in rats (8,9), to our knowledge only 2 case reports exist in the literature describing 99mTc-MIBI uptake in BAT in a human, using SPECT (or SPECT/CT) (6,7). The cardiac uptake of 99mTc-MIBI, a lipophilic cationic radiotracer that concentrates in mitochondria, is substantially proportional to regional blood flow in the myocardium. BAT, which appears to play a role in thermo- and energy regulation, is characterized by abundant vasculature and high mitochondrial metabolic activity. Though the precise mechanism of uptake needs further study, 99mTc-MIBI uptake in BAT is likely related to relatively high blood flow, possibly even more than to increased mitochondrial density and function (6,8–10).
In our study, BAT visualization by 99mTc-MIBI included areas commonly known to contain BAT: the supraclavicular region, neck (Fig. 4), and paraspinal tissues. We also found 1 patient with a more unusual pattern of tracer uptake in what appeared to be LHIS (11). This finding correlates to the observation that LHIS can be 18F-FDG–avid as well (12,13), which is likely related to the fact that LHIS is composed of both mature adipocytes and, to a variable degree, fetal fat cells or brown fat. It should not be misdiagnosed as tumor or ectopic parathyroid adenoma. The frequency of BAT visualization in our study is similar to the frequency reported in studies with 18F-FDG PET in adults (6.3% for MIBI vs. 4%–7% for 18F-FDG PET). A higher frequency of BAT visualization with 99mTc-tetrofosmin was reported but might be related to the pediatric population and to the fact that no CT was obtained to ascertain that the tracer accumulation definitely is in BAT.
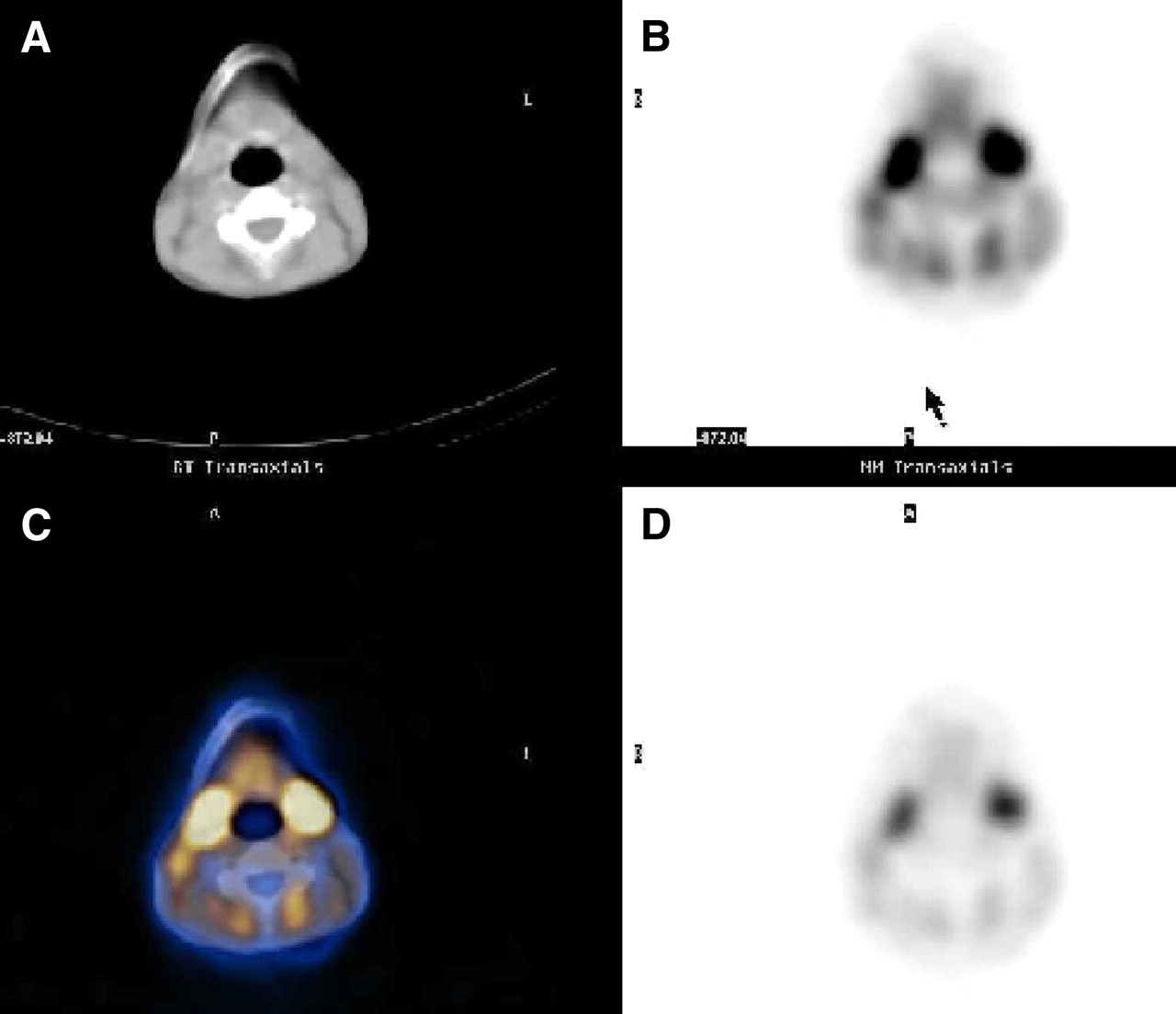
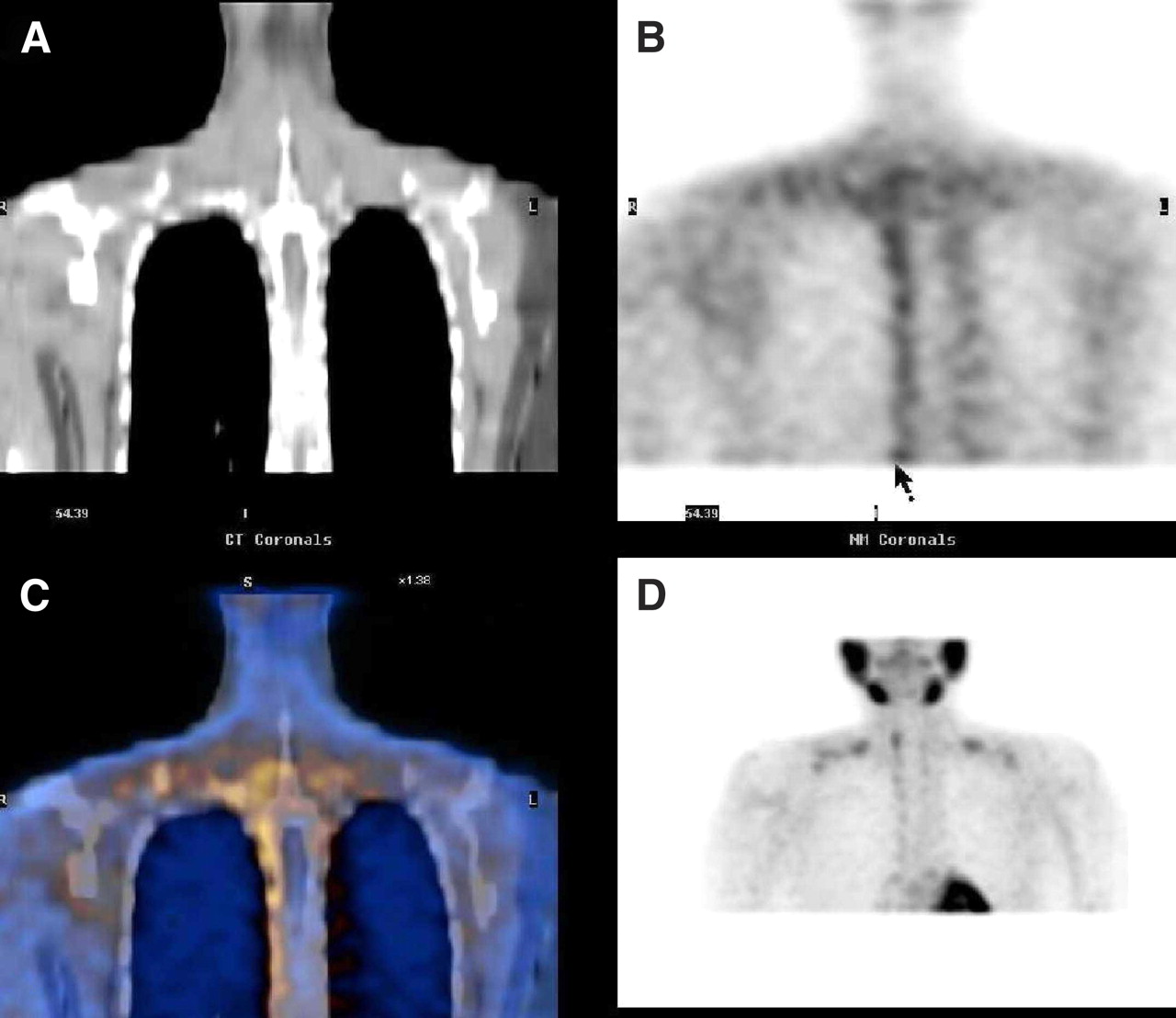
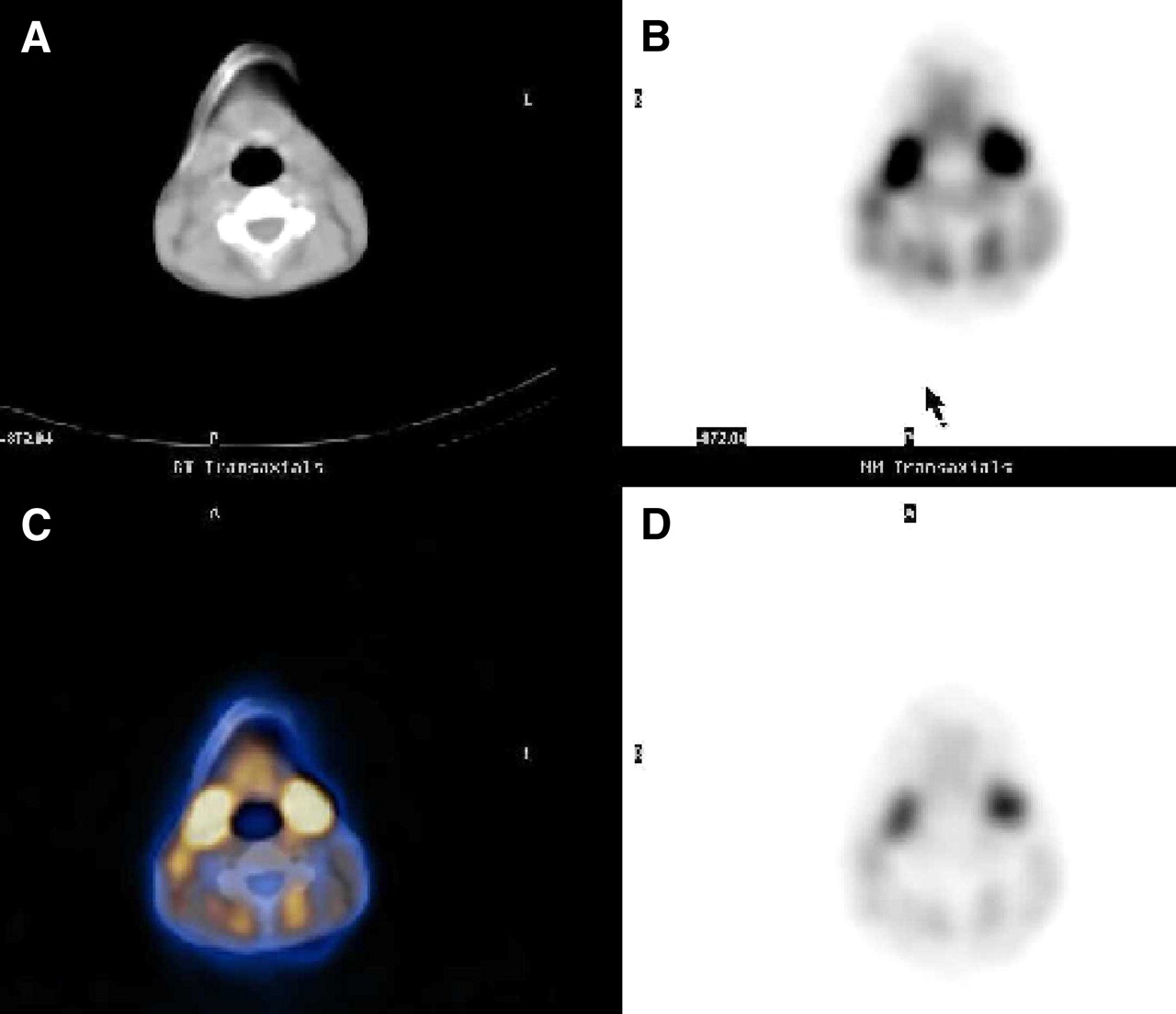
Selected slices of CT (A), attenuation-corrected SPECT (B), fused SPECT/CT (C), and noncorrected SPECT (D). 99mTc-MIBI uptake is fusing to areas of BAT in the neck area.
CONCLUSION
As we gain more understanding about the role of BAT (especially its possible role regarding glucose metabolism and obesity), 99mTc-MIBI might prove to be a good tracer to visualize BAT for research or clinical purposes. For the present, recognizing this normal finding and avoiding confusion with 99mTc-MIBI-avid–disease, including through the use of SPECT/CT, are most salient.
Acknowledgments
This study was presented in part at the 2005 annual meeting of the Radiological Society of North America.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 9, 2007.
- Accepted for publication January 3, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Perspectives on Brown Adipose Tissue Imaging: Insights from Preclinical and Clinical Observations from the Last and Current Century
- Quantification of Human and Rodent Brown Adipose Tissue Function Using 99mTc-Methoxyisobutylisonitrile SPECT/CT and 18F-FDG PET/CT
- 18F-Fluorobenzyl Triphenyl Phosphonium: A Noninvasive Sensor of Brown Adipose Tissue Thermogenesis