


Abstract
The management for totally thyroidectomized differentiated thyroid cancer (TT-DTC) patients with unexplained hyperthyroglobulinemia remains indeterminate because of evidence scarcity. This multicenter study aimed at prospectively evaluating the response to radioiodine (131I) adjuvant therapy (RAT) and its potential role in risk stratification and causal clarification. Methods: TT-DTC patients with stimulated serum thyroglobulin levels greater than 10 ng/mL but no structurally evident disease were consecutively enrolled in 5 tertiary-care institutions. After the administration of 5.55 GBq of 131I, the risk of persistent, recurrent, or metastatic differentiated thyroid cancer (prmDTC) was compared with that before RAT. The causes of hyperthyroglobulinemia were explored—and the response to RAT assessed—6–12 mo after RAT. The change in suppressed thyroglobulin level was reported. Results: A cohort of 254 subjects with a median stimulated thyroglobulin level of 27.1 ng/mL was enrolled for the analyses. Immediately after RAT, low, intermediate, and high risk were identified in 5.9%, 88.6%, and 5.5% patients, respectively, with no significant difference in risk stratification compared with that before RAT (P = 0.952). During the follow-up (median, 10.6 mo), hyperthyroglobulinemia was ultimately attributed to a thyroid remnant, biochemical disease, and structural or functional disease in 17.3%, 54.3%, and 28.4% of subjects, respectively. In addition, responses that were excellent, indeterminate, biochemically incomplete, and structurally or functionally incomplete were achieved in 18.1%, 27.2%, 36.2%, and 18.5% of patients, respectively. Notably, the distribution for either cause of hyperthyroglobulinemia or response to RAT was comparable among the 3 postoperative risk groups. Suppressed thyroglobulin levels in patients who merely received RAT declined significantly over time. Conclusion: Our study demonstrated that over 90% of TT-DTC patients with unexplained hyperthyroglobulinemia are stratified as being at intermediate to high risk, and RAT using 5.55 GBq of 131I reveals biochemical, functional, or structural disease and yields a non–structurally or –functionally incomplete response in more than 80% patients, suggesting that TT-DTC patients with unexplained hyperthyroglobulinemia are explicit candidates for RAT.
With the exception of active surveillance and thermal ablation in patients with low-risk microscopic papillary thyroid cancer, the initial management of differentiated thyroid cancer relies mainly on surgery followed by radioiodine (131I) remnant ablation (RRA), radioiodine adjuvant therapy (RAT) of potential residual thyroid cancer, or radioiodine treatment (RT) of known disease, under thyroid-stimulating hormone (TSH) suppression (1–3).
Before 131I administration, the postoperative serum thyroglobulin level measured at either the stimulated (Tgoff) or the suppressed (Tgon) TSH level is of great value in both disease monitoring and management decision making, since hyperthyroglobulinemia a few weeks after total thyroidectomy is highly associated with persistent, recurrent, or metastatic differentiated thyroid cancer (prmDTC) and survival (4–8). The 2015 American Thyroid Association (ATA) guidelines pointed out that patients with postoperative Tgoff levels of more than 10 ng/mL will likely need additional evaluations and possibly even complementary therapies (1). Unfortunately, although it has been over 10 y since the term thyroglobulinemia was initially raised by the well-acknowledged 2009 ATA guidelines (9), few dedicated data exist for totally thyroidectomized differentiated thyroid cancer (TT-DTC) patients with unexplained hyperthyroglobulinemia, partially because of inclusion of patients with structural disease in previous studies (7,10). Consequently, the relationship between hyperthyroglobulinemia and the risk of carrying prmDTC, the primary cause of unexplained hyperthyroglobulinemia, and the response to 131I administration in such patients remains largely unknown.
Aiming at facilitating initial staging and follow-up, improving disease-specific survival and progression-free survival, and decreasing recurrence, RAT should be considered or routinely recommended in intermediate- or high-risk patients but not in low-risk patients, with regard to guidelines issued by the ATA (1). However, the implications of serum thyroglobulin level in risk stratification have not been fully clarified, and the attempt to define the indications for RAT has been retarded, since a precise thyroglobulin cutoff has not been firmly established for distinguishing intermediate- from low- or high-risk patients or for distinguishing RAT from RRA or RT. Hence, we conducted this prospective multicenter study to assess the response to RAT and its potential role in risk stratification and causal clarification in a dedicated cohort of TT-DTC patients with unexplained hyperthyroglobulinemia regardless of postoperative risk stratification, to establish a potential indication for RAT.
MATERIALS AND METHODS
Patients
TT-DTC patients with hyperthyroglobulinemia, whose Tgoff levels at more than 4 wk after total thyroidectomy and just before RAT were more than 10 ng/mL, were consecutively recruited from June 2009 in 5 tertiary-care institutions. Patients with a prmDTC lesion identified by neck ultrasonography (1), chest CT, 99mTc-methylene diphosphonate whole-body scanning, MRI, or 18F-FDG PET/CT were excluded. Consequently, a Tgoff level of over 10 ng/mL in TT-DTC patients without structurally evident prmDTC was defined as unexplained hyperthyroglobulinemia and comprehensively analyzed.
Just before RAT, patients with radioiodine uptake greater than 15% were excluded to ensure the success of RRA as previously described by our group (11). Serum TSH, thyroglobulin, and antithyroglobulin antibody (TgAb) levels were measured by electrochemiluminescence immunoassay on a Cobas analyzer (Roche Diagnostics Gmbh). The upper detection limit of the TSH assay was 100 mIU/L, and TSH levels higher than that were counted as 100 mIU/L. Similarly, thyroglobulin and TgAb levels lower than their thresholds were counted as 0.04 ng/mL and 10 IU/mL, respectively. Neck ultrasonography and chest CT were conducted on all patients before RAT.
For RAT, an activity of 5.55 GBq of 131I was orally administered. Three days later, a planar whole-body scan was performed with SPECT/CT if needed (12). RT was performed 6 mo after RAT in patients if 131I-avid prmDTC lesions were identified by post-RAT scanning; conversely, patients without overt structural or functional disease were regularly followed up for more than 1 y under TSH suppression. Tgon levels were tested and neck ultrasonography performed at each follow-up visit. The follow-up visit, and possible modulation of levothyroxine dosage, were done at 1, 4, and 12 mo after RAT except as otherwise indicated, then every 6–12 mo. The assessment of therapeutic response to RAT and the primary cause of hyperthyroglobulinemia were revealed 6–12 mo after RAT.
The institutional review boards approved this study, and all subjects gave written informed consent.
Risk Stratification
According to the 2009 ATA guidelines, the 3-tiered system, including a low, intermediate, and high risk of prmDTC, was used with minor revisions (9). Low-risk patients were characterized by intrathyroidal differentiated thyroid cancer with no evidence of extrathyroidal extension, vascular invasion, aggressive histology, or metastases. Intermediate-risk patients were featured by either microscopic extrathyroidal extension, cervical lymph node metastases, 131I-avid disease in the neck outside the thyroid bed, vascular invasion, or aggressive tumor histology. High-risk patients were distinguished by either gross extrathyroidal extension, incomplete tumor resection, or distant metastases.
Causal Categorization
The primary causes of postoperative unexplained hyperthyroglobulinemia were based on the findings of post-RAT scanning, consecutive serum thyroglobulin tests, medical imaging, ultrasonography-guided fine-needle aspiration in combination with pathologic examination, and correlation with clinical follow-up within 6–12 mo after RAT.
Determination of a thyroid remnant was based on visible uptake in the normal thyroid bed or ectopia on post-RAT scanning, absence of prmDTC, and a Tgon level of less than 0.2 ng/mL. Biochemical disease was affirmed by the absence of structural or functional evidence of prmDTC but a Tgon level of at least 0.2 ng/mL. Structural or functional disease was defined as any evidence of prmDTC lesions identified by post-RAT scanning or other imaging examinations during surveillance.
Response to RAT
According to the 2015 ATA guidelines, a response evaluation scheme with 4 categories was adopted with minor modifications 6–12 mo after RAT (1). The definitions of excellent response, indeterminate response, and biochemically incomplete response remained. A structurally or functionally incomplete response (S/FIR) endorsed positive anatomic or metabolic imaging evidence of disease with any thyroglobulin level. Indeterminate response, biochemically incomplete response, and S/FIR were collectively assigned as a nonexcellent response, whereas an excellent response, an indeterminate response, and a biochemically incomplete response were grouped as non-S/FIR.
Statistical Analyses
All analyses were conducted using SPSS (version 20; IBM) software. Continuous data are presented as means with SDs or medians with interquartile ranges for normal and abnormal distributions, respectively. Categoric variables are displayed as number with percentage. Categoric variables were compared using the χ2 test or Fisher exact test. Variance was analyzed for continuous data with a normal distribution. The predictive value of Tgoff for the primary cause of hyperthyroglobulinemia was evaluated by univariate receiver-operating-characteristic analysis in combination with the DeLong test for comparing the area under the curve. The Wilcoxon signed-rank test for thyroglobulin level was performed at multiple time points. Two-tailed probabilities were reported, and a P value of less than 0.05 was considered statistically significant.
RESULTS
Baseline Characteristics
From June 2009 through August 2018, 469 TT-DTC patients with a Tgoff level of more than 10 ng/mL were enrolled. After the exclusion of 215 patients (8 patients with TgAb > 100 IU/mL, 55 patients with radioiodine uptake > 15%, 114 patients with suspected cervical locoregional disease, and 38 patients with possible distant metastases), 54.2% (254/469) of patients deemed as having unexplained hyperthyroglobulinemia were eligible for further analyses.
The baseline characteristics of the 254 subjects are summarized in Table 1. The mean age at diagnosis was 38.3 ± 11.8 y, with a male-to-female ratio of 1:1.65. In total, 252 (99.2%) patients were classified as stage I or II. None of the enrolled patients had undergone RRA before RAT. The mean interval between surgery and RAT was 4.2 ± 3.3 mo. The postoperative median Tgon level was 3.7 ng/mL, while thyroglobulin level increased up to 27.1 ng/mL just before RAT, when the median TSH level was 100 mIU/mL at 4 wk after thyroid hormone withdrawal.
Baseline Characteristics of TT-DTC Patients with Postoperative Unexplained Hyperthyroglobulinemia (n = 254)
Risk Stratification
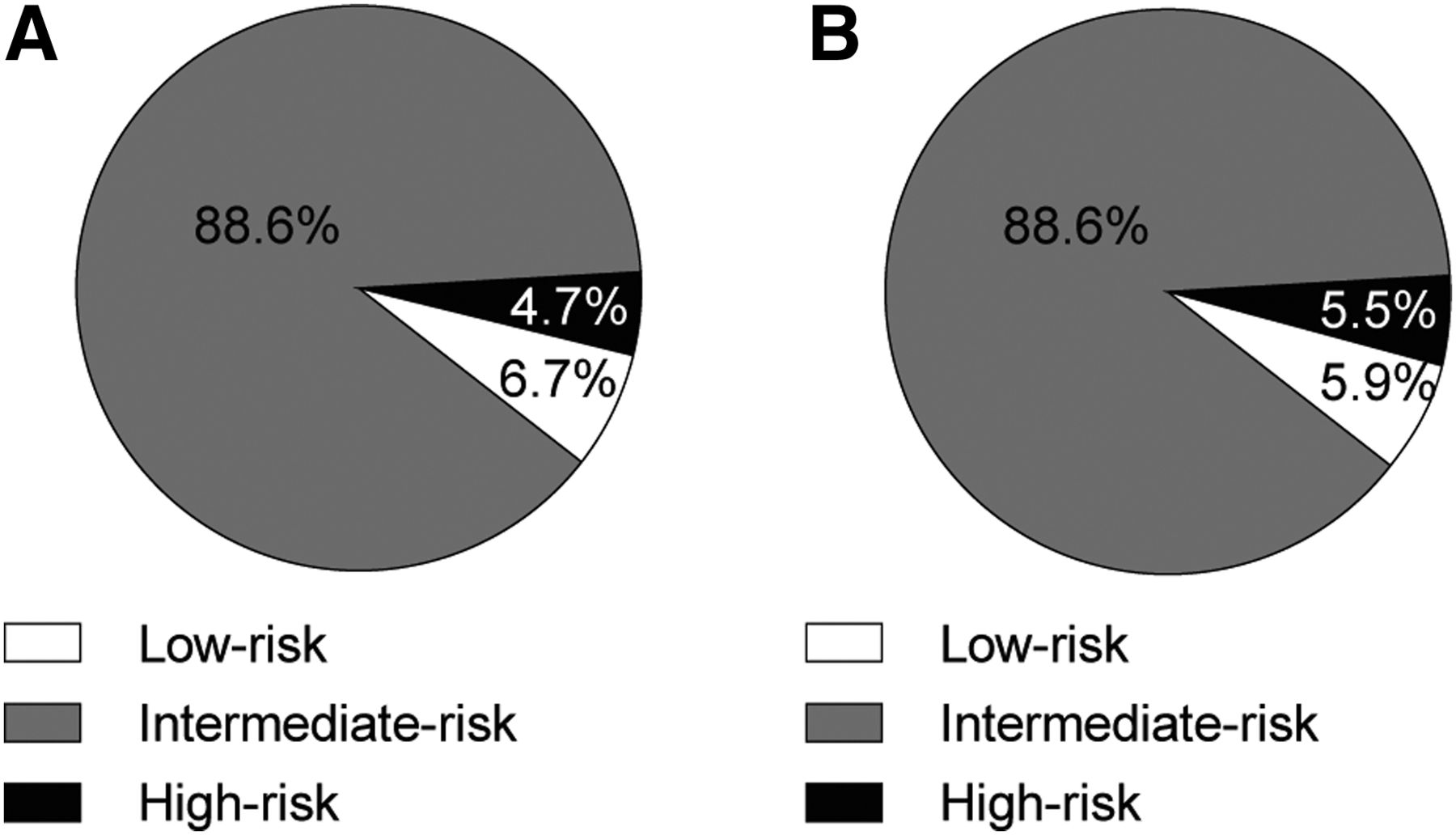
In the postoperative risk stratification, only 17 (6.7%) of the 254 eligible patients were categorized into the low-risk group. In total, 225 (88.6%) and 12 (4.7%) patients were classified as having an intermediate and high risk, respectively, of harboring prmDTC. Once post-RAT scan findings were obtained, 11.8% (2/17) of postoperative low-risk patients switched to the intermediate-risk group for the identification of nodule disease, replacing another 2 intermediate-risk patients who were transferred to the high-risk group because of distant metastasis. Thus, the number of patients with intermediate risk remained at 225. No significant difference in the risk distribution between the 2 time points (before and after RAT) was achieved (P = 0.952) (Fig. 1).
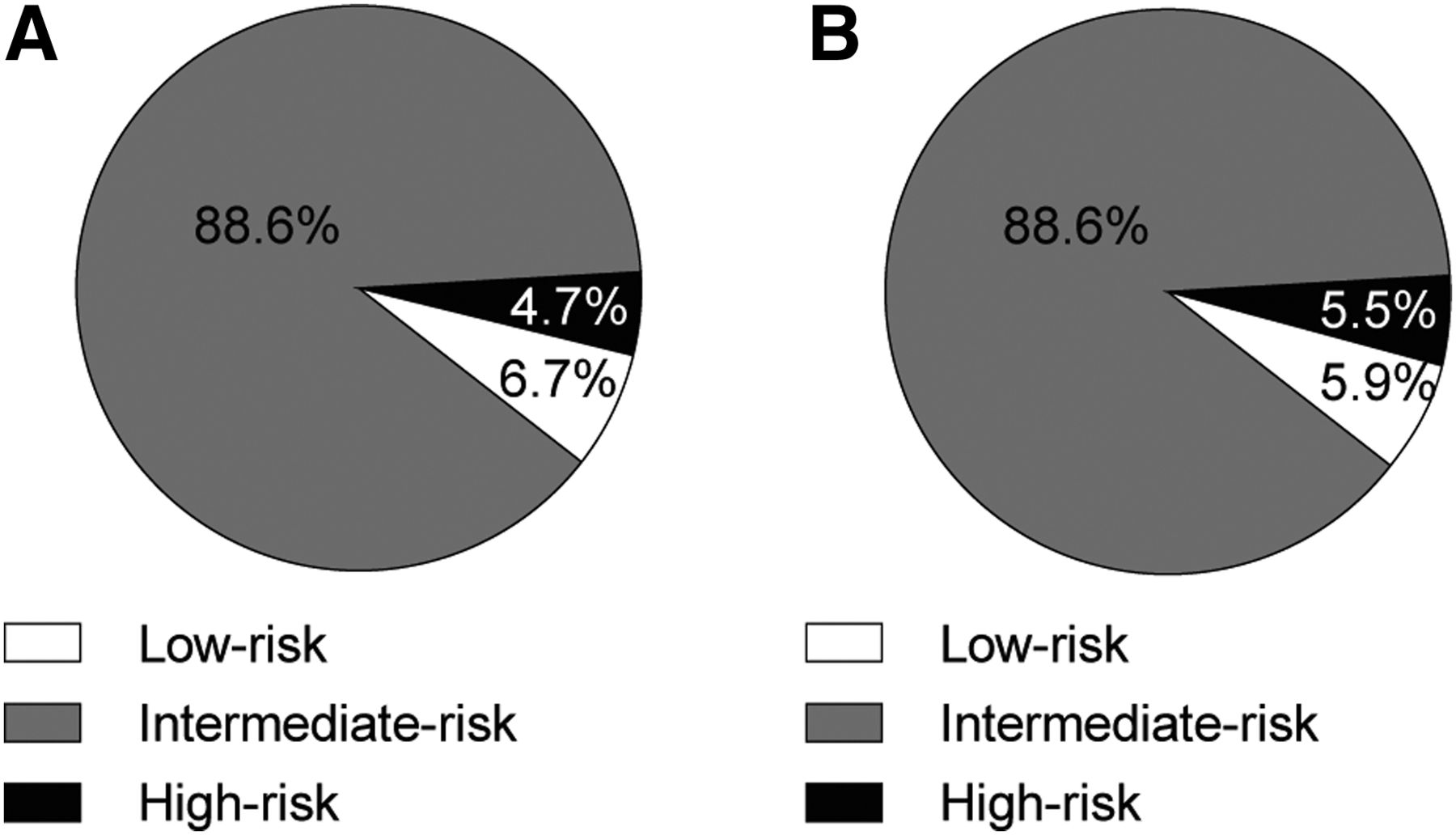
Risk stratifications in patients with unexplained hyperthyroglobulinemia before (A) and just after (B) RAT (n = 254).
Causal Categorization
According to the findings in a median follow-up of 10.6 mo (range, 7.3–13.8 mo), the unexplained postoperative hyperthyroglobulinemia could ultimately be attributed to a thyroid remnant in 17.3% (Fig. 2), biochemical disease in 54.3%, and structural or functional disease in 28.4% (Figs. 3 and 4) of the 254 patients (Fig. 5).
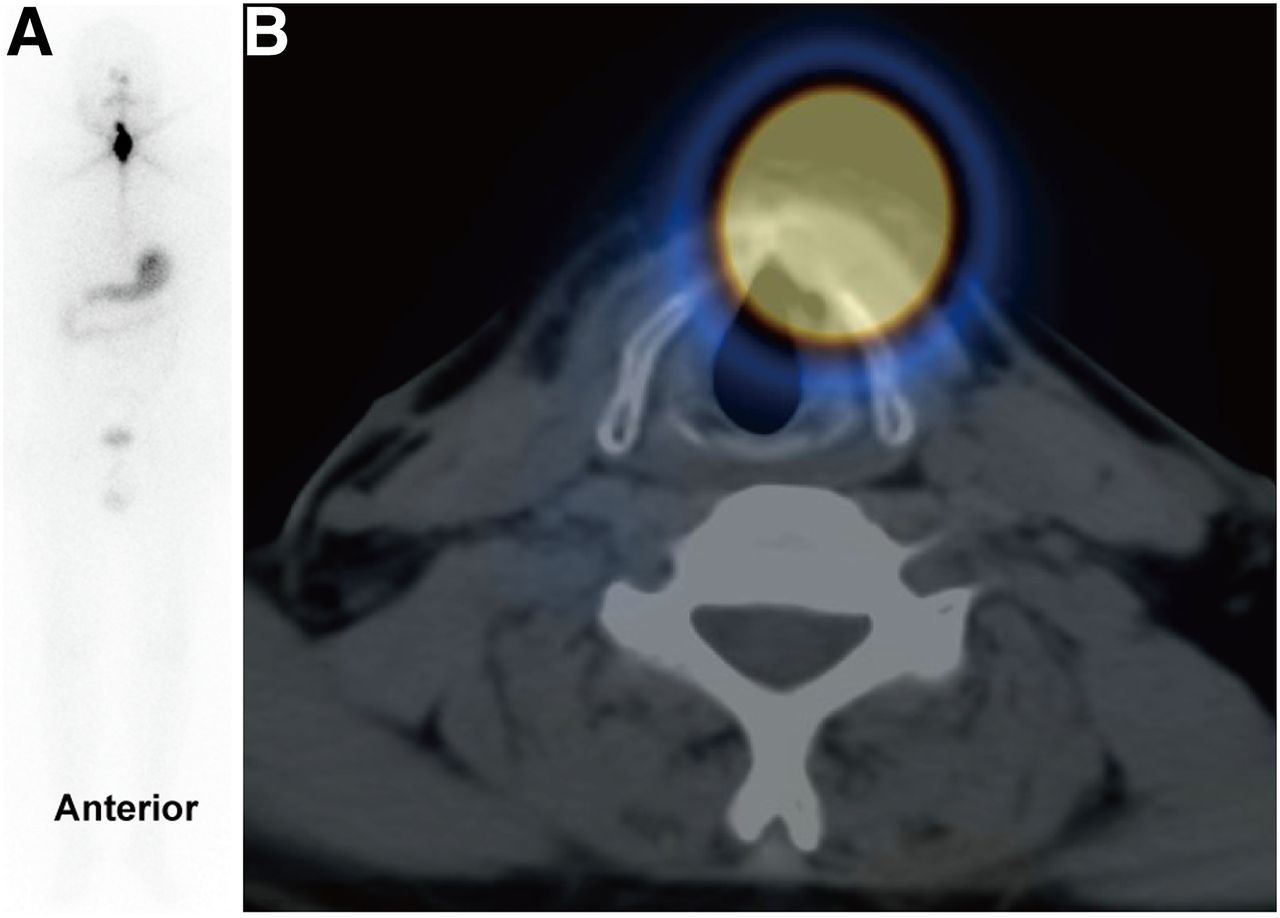
Post-RAT whole-body scan (A) and SPECT/CT image (B) of papillary thyroid carcinoma patient with unexplained hyperthyroglobulinemia causally attributed to thyroid remnant.

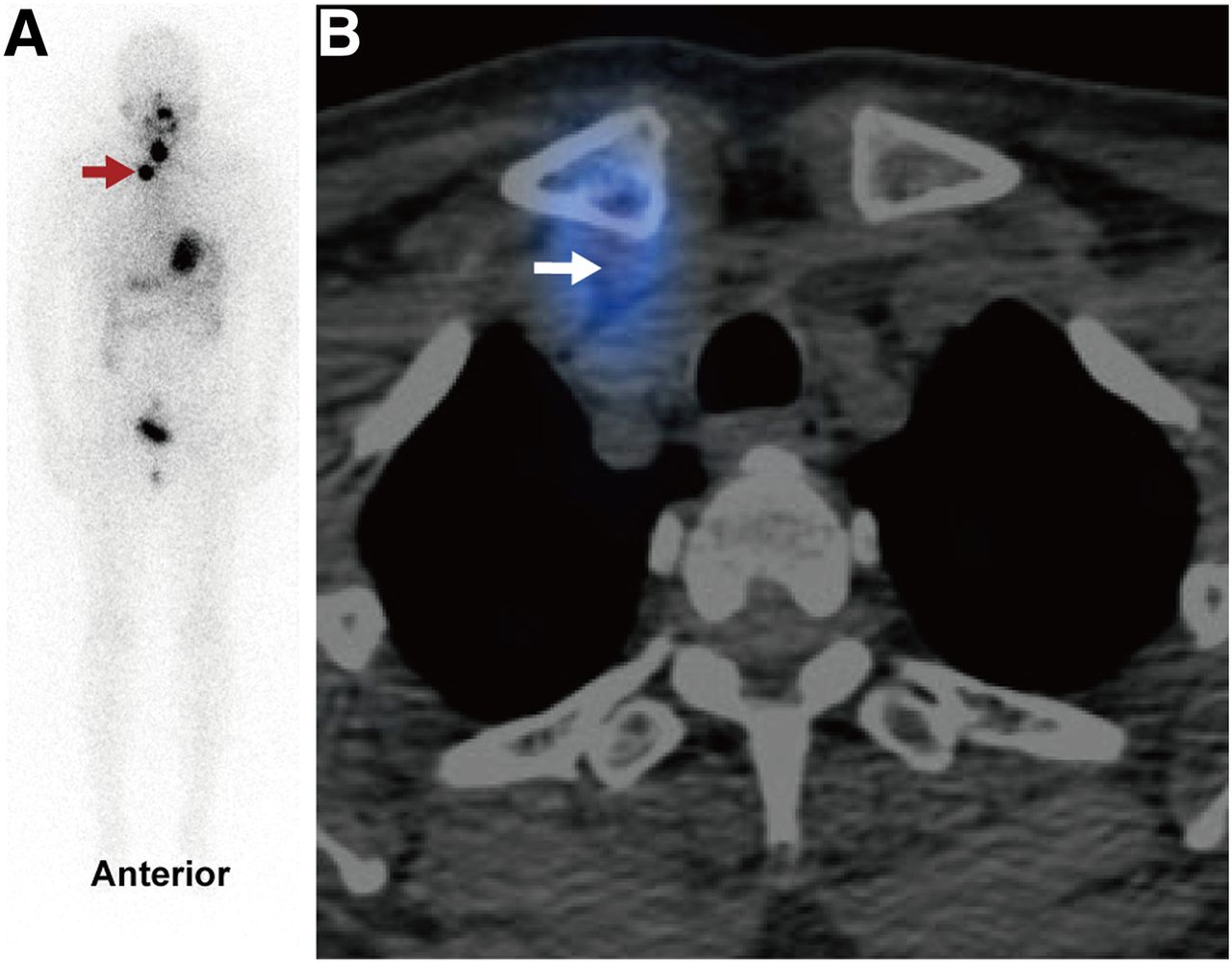
Post-RAT whole-body scan (A) and SPECT/CT image (B) of papillary thyroid carcinoma patient with unexplained hyperthyroglobulinemia causally attributed to metastatic lymph node (arrows) unable to be diagnosed by ultrasonography and CT before RAT.

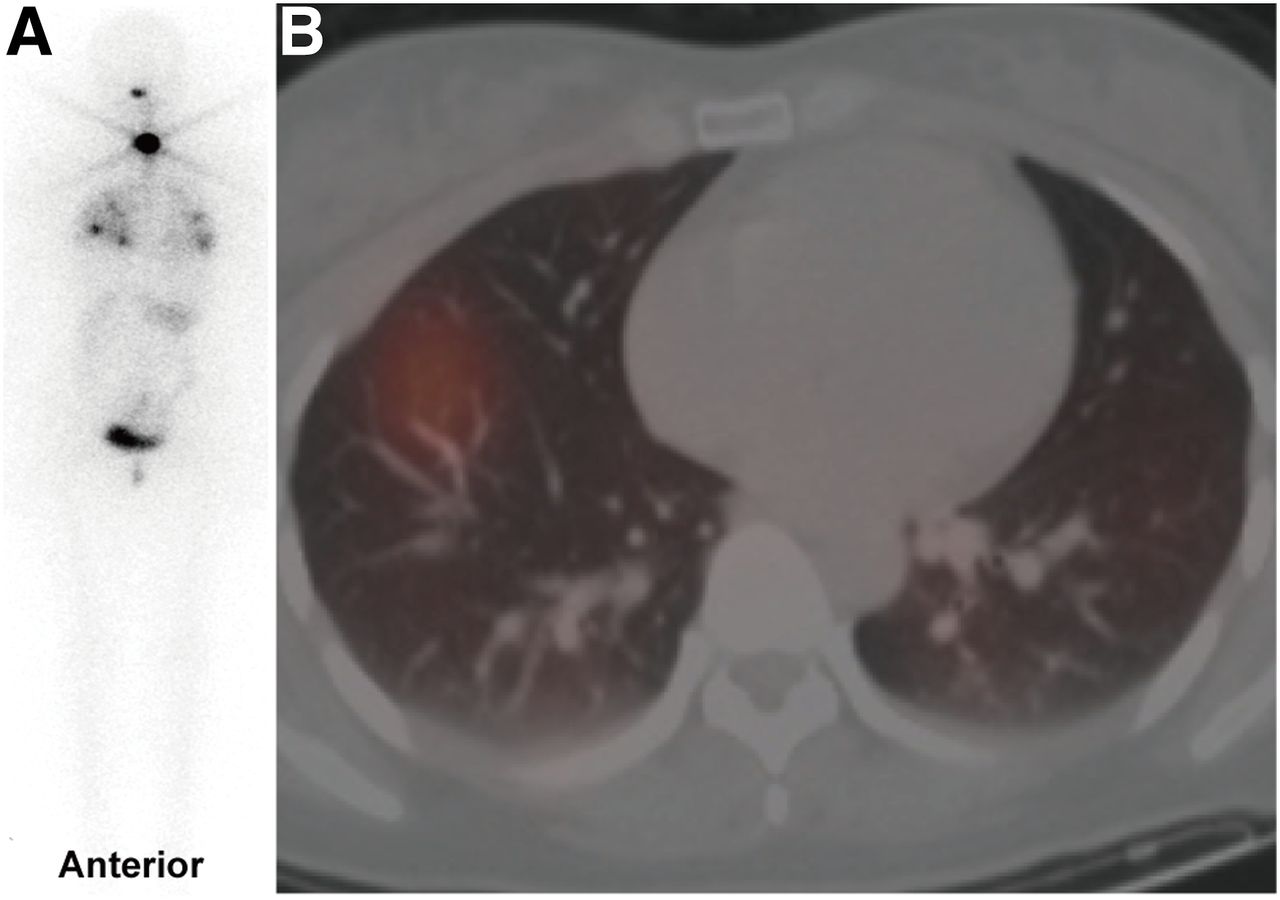
Post-RAT whole-body scan (A) and SPECT/CT image (B) of follicular thyroid carcinoma patient with unexplained hyperthyroglobulinemia causally attributed to lung metastases unable to be identified by CT before RAT.

Causal distribution of unexplained postoperative hyperthyroglobulinemia after RAT (A) and therapeutic response to RAT (B) (n = 254).
The causal classification of the postoperative risk of prmDTC is shown in Table 2. Again, no significant difference in causal proportion was achieved among the 3 risk groups (P = 0.526). Moreover, the proportion of either biochemical or structural or functional disease in the intermediate- to high-risk group was comparable with that in the low-risk group (P = 0.465).
Causal Classification Regarding Postoperative Risk of prmDTC in TT-DTC Patients with Unexplained Hyperthyroglobulinemia (n = 254)
Furthermore, the comparisons of factors potentially associated with the cause of unexplained hyperthyroglobulinemia in TT-DTC patients are shown in Table 3. The median Tgoff level significantly differed among the 3 causal groups (P = 0.000). The Tgoff cutoff for distinguishing a thyroid remnant from biochemical, structural, or functional disease was 19.5 ng/mL, with an area under the curve of 0.714, a sensitivity of 68.2%, and a specificity of 70.0% (P < 0.0001). In addition, a Tgoff level of 27.9 ng/mL was obtained as the cutoff for isolating structural or functional disease from a thyroid remnant and biochemical disease, with an area under the curve of 0.630, a sensitivity of 68.2%, and a specificity of 58.8% (P = 0.0009). However, no significant difference in radioiodine uptake, TSH, or TgAb level was achieved among the 3 causal groups, with a comparable proportion of patients having a TSH of more than 100 mIU/mL or a TgAb of less than 10 IU/mL.
Comparisons of RAIU, TSH, Tgoff, and TgAb Levels Among 3 Primary Causes of Unexplained Hyperthyroglobulinemia in TT-DTC Patients (n = 254)
Of the 72 patients causally attributed to structural or functional disease, 38 (52.8%) received RT because of the 131I avidity of prmDTCs as demonstrated by post-RAT scanning, in which 1, 2, and 3 courses of RT were given in 33 (86.8%), 3 (7.9%), and 2 (5.3%) patients, respectively. Thirty-four patients were identified with prmDTC during the 6- to 12-mo follow-up, in which 3 underwent cervical lymph node resection and the remaining 31 (43.1%) were under active surveillance with TSH suppression.
Additionally, 2 patients with anatomically negative but functionally positive disease were identified. One with pulmonary metastases achieved negative results on 131I whole-body scanning after the second therapeutic dose, and one with iliac metastasis, who received RT followed by bone lesion resection, obtained a disease-free status in the subsequent 1-y follow-up.
Response to RAT
Overall, 46 (18.1%), 69 (27.2%), 92 (36.2%), and 47 (18.5%) of the 254 eligible patients achieved excellent response, indeterminate response, biochemical incomplete response, and S/FIR, respectively (Fig. 5).
Regarding postoperative risk stratification, an excellent response was achieved in 35.3% (6/17) of low-risk patients, 16.4% (37/225) of intermediate-risk patients, and 25.0% (3/12) of high-risk patients (P = 0.119). Besides, S/FIR was obtained in 11.8% (2/17) of low-risk patients, 19.6% (44/225) of intermediate-risk patients, and 8.3% (1/12) of high-risk patients (P = 0.632).
After exclusion of 41 patients with more rounds of 131I administration or surgery, which might additionally affect the change in thyroglobulin level caused by RAT, the median Tgon level in the remaining 213 patients significantly decreased over time. Similar trends for change in median Tgon level in patients with hyperthyroglobulinemia primarily caused by thyroid remnant, biochemical disease, and structural or functional disease were found (Fig. 6).

Change in suppressed thyroglobulin level in patients with unexplained hyperthyroglobulinemia who received only RAT. (A) All patients (n = 213). (B, C, and D) Patients with unexplained hyperthyroglobulinemia causally attributed to thyroid remnant (n = 44), biochemical disease (n = 138), and structural or functional disease (n = 31), respectively. Data are expressed as median with interquartile range. *P < 0.05.
DISCUSSION
In this prospective multicenter study, we comprehensively reported the outcomes of RAT in a cohort of 254 TT-DTC patients with unexplained postoperative hyperthyroglobulinemia. Along with the non-S/FIR rate of 81.5%, a cause of biochemical, functional, or structural disease and an intermediate to high risk were deemed present in 82.7% and 94.1% of all eligible subjects, respectively, which was reached by a sufficient follow-up after RAT with an initial administration of 5.55 GBq of 131I. These novel findings may play a vital role in elucidating the indication for RAT, facilitating nuclear medicine practice and interdisciplinary communications.
Instead of the latest version, the original risk stratification protocol derived from the 2009 ATA guidelines was adopted and feasibly applied in this study, avoiding commonly insufficient detailed data on lymph node involvement and molecular features, which have been additionally suggested by the 2015 ATA guidelines. In addition, the risks were merely assessed before and soon after RAT, evading potential replacement by response categorization—the so-called dynamic risk stratification in some previous studies (13,14). As a result, up to 93.3% of TT-DTC patients with unexplained postoperative hyperthyroglobulinemia were initially classified as being at intermediate to high risk by the ATA guidelines during the interval between surgery and RAT. Unexpectedly, the distributions of risk before and after RAT were similar, indicating a stable and predominantly intermediate- to high-risk stratification in this commonly encountered entity. This finding may be interpreted in the light of the strictly controlled indications for total thyroidectomy, the rigorous exclusion criteria of this study, and a pathologic feature–predominant risk stratification scheme. Notably, although fewer than 1% of patients initially ranked as at intermediate risk were reclassified as being at high risk immediately after RAT, as many as 11.8% of patients initially classified as at low risk were reclassified as being at intermediate risk via post-RAT scanning. This modulation suggests that initially low-risk TT-DTC patients with hyperthyroglobulinemia may need more active monitoring and aggressive intervention instead of observation or RRA—a possibility that necessitates randomized controlled studies to evaluate the impact of RAT on prognosis (15).
During a median follow-up of 10.6 mo, hyperthyroglobulinemia was attributed to 3 well-defined causes. When 5.55 GBq of 131I were used, hyperthyroglobulinemia was finally attributed to a thyroid remnant in only 17.3% of patients. Considering the high efficacy of 131I in RRA as recently demonstrated by our team (11), we believe that such a dose is more competent for smaller thyroid remnants in the current study. Meanwhile, more than half the patients with unexplained hyperthyroglobulinemia were causally categorized as having biochemical disease, indicating the existence of subclinical lesions, which are most suitable for RAT and regular follow-up under TSH suppression (16). Although a significant difference in median Tgoff level was found among the 3 causal groups, it is currently difficult to use thyroglobulin level to efficiently separate patients with structural or functional disease from those with a thyroid remnant or biochemical disease before RAT, much less to use radioiodine uptake. In addition, distant metastases were identified by post-RAT scanning in fewer than 1% of patients with no apparent anatomic abnormalities, but a favorable status after active treatment was noted. We tentatively conclude that the total tumor burden might be relatively light and that RAT with 5.55 GBq of 131I can identify and treat the lesions competently.
It has been acknowledged that patients with S/FIR require a more intensive follow-up than those with non-S/FIR (1,17,18). Conversely, a non-S/FIR means a less than 1% rate of disease-specific death (1,19). The current study revealed no significant difference in response to RAT among the 3 risk groups, demonstrating that RAT using a high activity of 5.55 GBq can yield similar short-term efficacies among the 3-tiered risk groups.
In addition to acting as an efficient biomarker for postoperative disease status, thyroglobulin has long been recognized as a reliable therapeutic response evaluation tool (15,20,21). In our study, a significant decline in thyroglobulin level during as long as 1 y of follow-up in RAT-treated patients was found regardless of the cause of hyperthyroglobulinemia, as may be explained by both the sustained destroying effect of 131I on the thyroid remnant or invisible 131I-avid prmDTC lesions and the continuously sufficient suppression of TSH (18,22). Since it has been reported that patients who had negative findings on posttherapeutic 131I scanning, ultrasonography, CT, and 18F-FDG PET/CT but elevated thyroglobulin rarely showed positive findings on the second 131I scan (23), we recommended that patients without visualized 131I-avid lesions be monitored under continued TSH suppression in the first year after RAT. Moreover, since the thyroglobulin level just before RAT might be influenced by both TSH level and interval between total thyroidectomy and RAT, thyroid hormone withdrawal for 4 wk after total thyroidectomy when the median TSH level had climbed up to 100 mIU/mL (range, 49.5–100 mIU/mL) adequately ensured both cleanup of existing serum thyroglobulin immediately after total thyroidectomy and exposure of thyroglobulin deriving from a microscopic thyroid remnant or prmDTC lesion (1).
Although the term RAT has been raised for decades and attempts were recently made to define it as “131I administered to destroy subclinical tumor deposits after surgical resection of all known primary tumor tissue and metastatic foci,” a clear definition of “subclinical tumor deposits” was not achieved by the joint statement (24). Even more confusingly, the statement has also mentioned that patients with biochemical evidence of disease can also be candidates for RT, as are patients with structural or functional disease (1,24). The above difficulties and inconsistencies may be caused by the severe overlap in thyroglobulin level and potentially simultaneous goals among the 3 clinical scenarios (RRA, RAT, and RT) and the absence of precisely differential techniques, necessitating diagnostic radioiodine scanning and other imaging modalities (25). As was demonstrated by the current study, unexplained hyperthyroglobulinemia in TT-DTC patients represents an apparent indicator for RAT irrespective of the initial risk stratification, since over 90% of patients with this entity were stratified as being at intermediate to high risk and 82.7% of patients were finally attributed to have biochemical, functional, or structural disease. Therefore, we believe that our findings may ameliorate the relatively vague indication of RAT compared with those of RRA and RT and constructively promote scientific dialogue.
The study had some limitations. First, because of long-term controversies, diagnostic radioiodine imaging, which might have explained the cause of hyperthyroglobulinemia in part before RAT, was not incorporated in our study. Second, since the optimal administered activity of 131I in RAT had not been determined, our patients received a fixed activity of 131I; thus, studies comparing the outcomes and side effects of multiple doses are still needed. Third, a forthcoming randomized control study assessing long-term outcomes may strengthen the significance of RAT by compensating this single-arm study.
CONCLUSION
Our prospective multicenter study demonstrated that unexplained hyperthyroglobulinemia in TT-DTC patients represents an appropriate indicator for RAT, since there was found to be an intermediate to high risk of carrying prmDTC in greater than 90% of patients, and RAT with an activity of 5.55 GBq revealed biochemical, functional, or structural disease and yielded non-S/FIR in more than 80% of patients.
DISCLOSURE
This work was supported by the National Natural Science Foundation of China (grant 81671711). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How should TT-DTC patients with unexplained hyperthyroglobulinemia be treated?
PERTINENT FINDINGS: Our prospective multicenter cohort study demonstrated that over 90% of TT-DTC patients with unexplained hyperthyroglobulinemia were stratified as being at intermediate to high risk, and RAT at a dose of 5.55 GBq revealed biochemical, functional, or structural disease and yielded a non–structurally or functionally incomplete response in more than 80% of subjects. Distribution for either cause of hyperthyroglobulinemia or response to RAT was comparable among the 3 postoperative risk groups.
IMPLICATIONS FOR PATIENT CARE: These findings recommend TT-DTC patients with unexplained hyperthyroglobulinemia as candidates for RAT irrespective of postoperative risk stratification.
Footnotes
Published online May 1, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCE
- Received for publication February 20, 2020.
- Accepted for publication April 9, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.