


Abstract
Although radiation-induced mesenteritis or peritonitis can potentially exacerbate the risk of bowel obstruction, there are no data in the literature on the incidence of intestinal obstruction related to peptide receptor radionuclide therapy. Methods: The records of all patients treated with 177Lu-DOTATATE at Moffitt Cancer Center between April 2018 and October 2019 were evaluated. The number of patients who developed bowel obstruction within 3 mo of a 177Lu-DOTATATE treatment was divided by the total number of patients with preexisting peritoneal or mesenteric disease. Management strategies and outcomes were evaluated. Results: Of a total of 159 patients treated, 81 had baseline mesenteric or peritoneal disease, among whom 5 (6%) experienced at least 1 episode of bowel obstruction within 3 mo of treatment. Two of the patients underwent surgical exploration during obstruction describing a “frozen abdomen.” All 5 responded at least temporarily to high-dose corticosteroid treatment and regained bowel function, but 2 patients eventually succumbed to progressive peritoneal disease. Conclusion: Peptide receptor radionuclide therapy can lead to bowel obstruction in patients with mesenteric or peritoneal disease, likely by inducing inflammation. Corticosteroids can potentially play a role in treatment and prophylaxis.
Radiolabeled somatostatin analogs have developed into an important treatment option for patients with progressive, well-differentiated neuroendocrine tumors (NETs) (1). These radiopharmaceuticals belong to a treatment category known as peptide receptor radionuclide therapy (PRRT) and are generated through the linkage of a radioactive isotope to a somatostatin analog. This linkage enables the delivery of targeted radiation to somatostatin-receptor (SSTR)–expressing tumor cells. Several generations of radioactive isotopes, most notably the β-emitters 90Y and 177Lu, have been tested in clinical trials (2–5). With a maximum tissue penetration range of roughly 2 mm, 177Lu is associated with a favorable therapeutic index. The radiolabeled somatostatin analog 177Lu-DOTATATE has been studied extensively in single-arm studies and in the phase III NETTER-1 trial, where it was shown to significantly delay progression-free survival compared with high-dose octreotide in a population of patients with progressive midgut NETs (6). Results of the NETTER-1 study, as well as a large institutional registry (2), led to the approval of 177Lu-DOTATATE for the treatment of gastroenteropancreatic NETs in the United States and Europe in 2018.
A standard course of 177Lu-DOTATATE consists of 4 treatment cycles at a dose of 7.4 GBq (200 mCi) each, administered 8 wk apart. Past analyses of 177Lu-DOTATATE–associated side effects have focused primarily on myelotoxicity and nephrotoxicity. Severe, irreversible myelotoxicity (myelodysplastic syndrome or acute myelogenous leukemia) has been observed to occur in roughly 2.5% of treated patients, whereas the risk of significant nephrotoxicity appears to be negligible when prophylactic amino acids are used (2,7). Gastrointestinal risks, other than acute nausea or vomiting, have not been well described in the literature, possibly because treatment-related toxicities are difficult to distinguish from disease-associated complications.
Underlying mesenteric and peritoneal disease is associated with a chronic risk of bowel obstruction. Mesenteric metastases from small-bowel NETs are often characterized by surrounding desmoplasia, a fibrotic process that can tether adjacent bowel (8,9). Delivery of radiation to mesenteric or peritoneal disease could, potentially, increase the risk of bowel obstruction through an inflammatory mechanism. However, to our knowledge, there have been no descriptions in the literature of intestinal obstruction arising as a consequence of treatment with 177Lu-DOTATATE. We therefore sought to investigate the incidence of PRRT-induced bowel obstruction in a high-volume treatment center.
MATERIALS AND METHODS
The medical records of all NET patients who received treatment with 177Lu-DOTATATE at the Moffitt Cancer Center between April 2018 and October 2019 were reviewed. Institutional review board approval was obtained, and a waiver of consent was granted because of the retrospective nature of this study. Patients with underlying mesenteric or peritoneal disease were considered to be an at-risk population for bowel obstruction. The radiographic characteristics of their baseline cross-sectional scans, as well as SSTR imaging, were evaluated by a board-certified radiologist and nuclear medicine specialist. Patients with extensive peritoneal disease (defined as >10 lesions) or mesenteric disease with significant desmoplastic fibrosis tethering bowel were considered to be at high risk.
Patients who developed a bowel obstruction within 3 mo of a treatment cycle of 177Lu-DOTATATE were considered to have possible treatment-related obstruction. The timing of their symptoms in relation to treatment, the course of obstruction, and management strategies were extracted from the medical record.
The number of patients with bowel obstruction was divided by the total number of treated patients, as well as by the subset of patients with peritoneal or mesenteric disease (at-risk population) and the number of patients with extensive peritoneal carcinomatosis or desmoplastic mesenteric disease (high-risk population).
RESULTS
In total, 159 patients were treated between April 2018 (after Food and Drug Administration approval and commercial availability of 177Lu-DOTATATE) and October 2019. Eighty-one patients (51%) were at risk for bowel obstruction due to baseline mesenteric or peritoneal disease. Among the patients with mesenteric or peritoneal tumors, a majority (59 patients) had primary midgut (jejunal and ileocecal) tumors, 16 patients had primary pancreatic tumors, and 6 patients had tumors of other primary sites. Twenty-two patients were deemed to be at high risk because of extensive peritoneal disease or desmoplastic changes associated with mesenteric tumors. Among midgut NET patients with mesenteric or peritoneal disease, 80% had previously undergone resection of their primary tumor. Although 19 patients with midgut NETs had experienced prior small-bowel obstruction, 16 of those cases were related to primary tumor with or without associated mesenteric disease, and only 3 cases were related to peritoneal carcinomatosis.
After beginning PRRT, 5 patients, all falling into the high-risk category, experienced a bowel obstruction within 3 mo of a treatment with 177Lu-DOTATATE. These 5 cases represented 3% of all patients treated with 177Lu-DOTATATE, 6% of patients with mesenteric or peritoneal disease, and 22% of high-risk patients. All had primary small-intestine (midgut) NETs with mesenteric and peritoneal disease, the extent of which was best appreciated on 68Ga-DOTATATE imaging. All had undergone resection of primary small-intestine tumors, and none had experienced overt bowel obstruction within the prior decade. The patient characteristics and clinical course are summarized in Table 1 and described below.
Patient Characteristics and Clinical Course
The first patient to experience bowel obstruction had progressive hepatic, mesenteric, and peritoneal disease at the time of initiation of treatment with 177Lu-DOTATATE. The peritoneal tumor burden was exceptionally high (Fig. 1), and he had developed a progressive stabbing abdominal pain shortly before treatment. One week after initiating 177Lu-DOTATATE, he presented with bowel obstruction, and a CT scan showed peritoneal thickening consistent with peritonitis, as well as dilatation of the proximal colon. He was started on oral dexamethasone, 4 mg twice daily, and was able to resume eating but was subsequently readmitted with recurrent bowel obstruction with a transition point at the level of the sigmoid colon. Exploratory laparotomy was performed and revealed a “frozen abdomen” caused by extensive adhesions between abdominal viscera and the anterolateral abdominal wall, leading to intestinal immobility. He was restarted on high-dose steroids and again regained a temporary ability to eat. Treatment with 177Lu-DOTATATE was not resumed and his peritoneal disease progressed. He eventually developed encapsulating peritonitis and a cocoon abdomen 5 mo after treatment and died 6 mo after treatment.

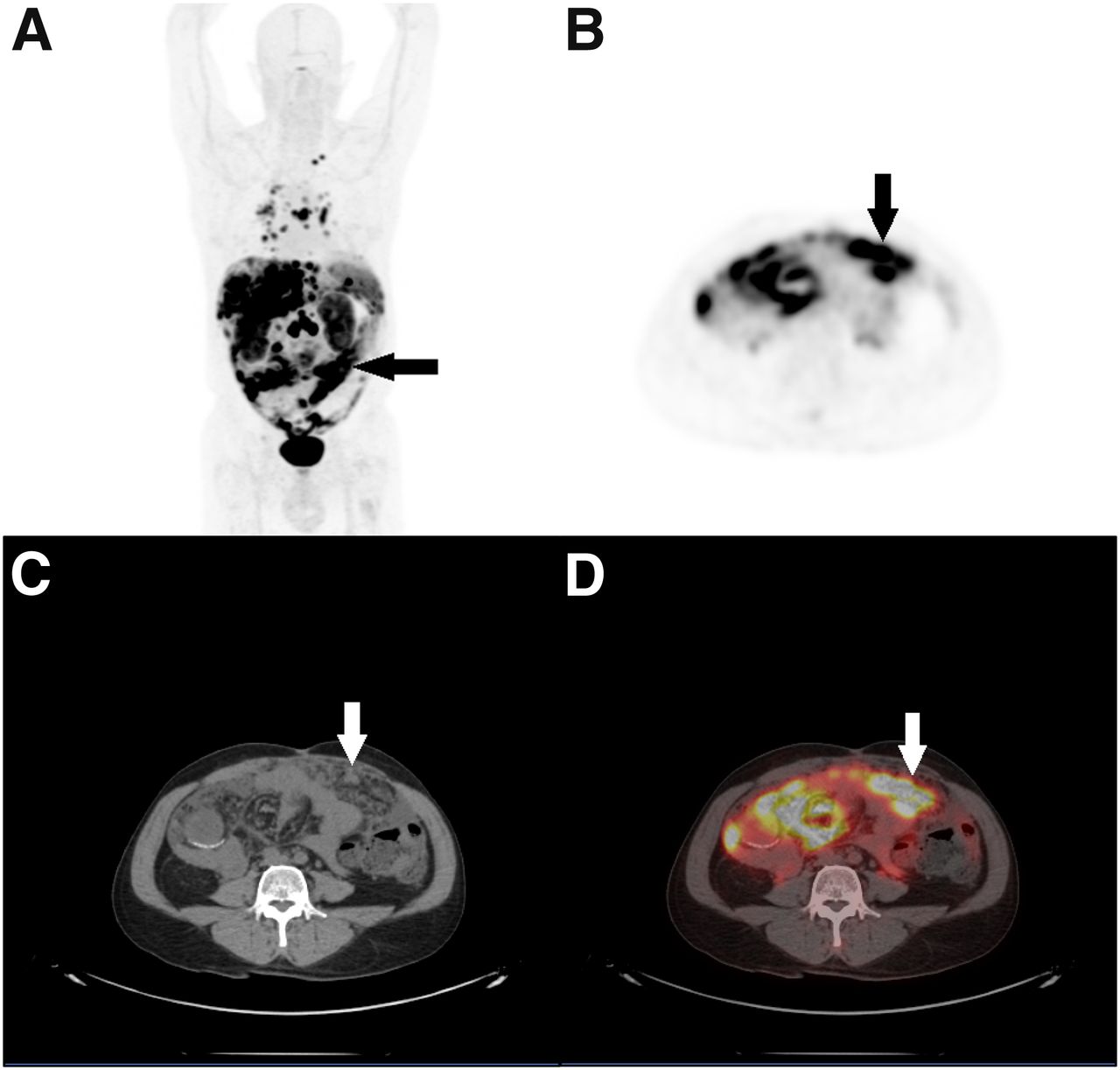
(A) Maximum-intensity projection demonstrates peritoneal carcinomatosis (arrow) and liver and mediastinal metastases in patient with progressive metastatic small-bowel NET. (B–D) Axial 68Ga-DOTATATE PET (B), attenuation-correction CT (C), and 68Ga-DOTATATE PET/CT (D) demonstrate uptake in extensive peritoneal metastatic implants (arrows).
The second patient presented with progressive hepatic, skeletal, mesenteric, and peritoneal disease (Fig. 2). Within several minutes of her first treatment with 177Lu-DOTATATE, she experienced acute nausea that resolved after administration of intravenous dexamethasone, 8 mg. She was discharged on a steroid taper but developed small-bowel obstruction 2 d after completion of steroids. The obstruction appeared to be related to tethering of bowel to a mesenteric mass (Fig. 3). She was restarted on steroids, and bowel function recovered 4 d later. She was able to tolerate her second and third 177Lu-DOTATATE treatments with prophylactic steroids (oral dexamethasone, 4 mg daily for 7 d followed by a 2-wk taper). However, she developed another bowel obstruction 3 wk after her fourth treatment and underwent exploratory laparotomy, which revealed a frozen abdomen. She was restarted on high-dose steroids and was able to resume eating 3 d after surgery. She was discharged on a prednisone taper and remained free of obstruction for 2 mo. However, at the time of data collection, she had developed recurrent small-bowel obstruction and began total parenteral nutrition.
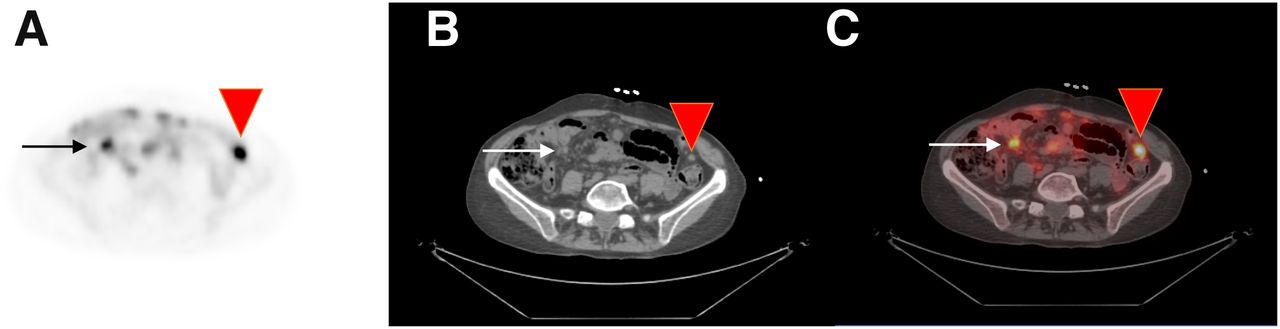
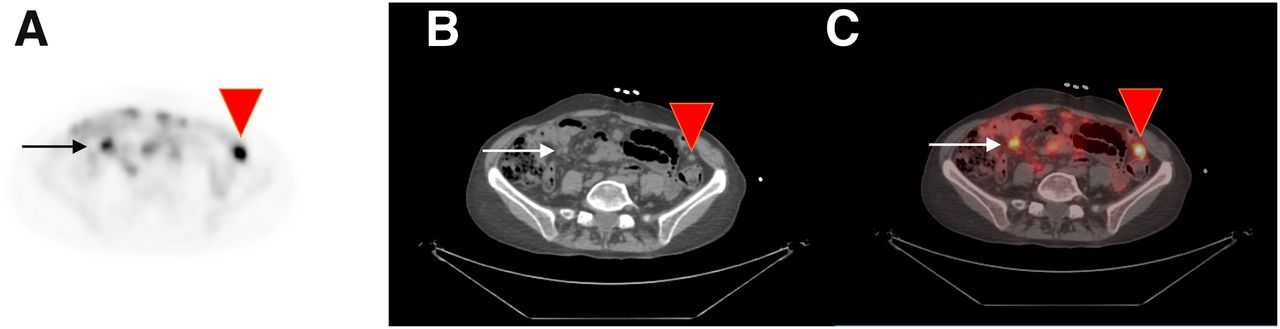
Axial 68Ga-DOTATATE PET (A), attenuation-correction CT (B), and 68Ga-DOTATATE PET/CT (C) demonstrate somatostatin-receptor–expressive mesenteric (arrows) and peritoneal (arrowheads) metastases. There is mild tethering of loops of bowel to mesenteric mass in right lower quadrant (arrows).

Coronal contrast-enhanced CT of abdomen and pelvis demonstrates small-bowel obstruction with dilated loops of bowel tethered to mesenteric lesion (arrow).
The third patient had progressive peritoneal disease at the time of 177Lu-DOTATATE initiation, as well as liver and lymph node metastases (Fig. 4). He developed crampy abdominal pain after the second treatment and was prescribed a steroid taper. He received prophylactic steroids with his third treatment but developed bowel obstruction 5 wk after therapy. A CT scan showed multilevel obstruction secondary to peritoneal carcinomatosis. His bowel function recovered 3 d after resuming steroids, and his fourth cycle of treatment was canceled. Five months later, in the setting of increasing postprandial pain and weight loss, he underwent exploratory laparotomy with extensive peritoneal surgical debulking. Over 50 tumors were resected, including numerous colon and small-bowel implants. The surgeon noted a massive desmoplastic reaction due to peritoneal carcinomatosis. He recovered well from surgery and was able to resume a normal diet.

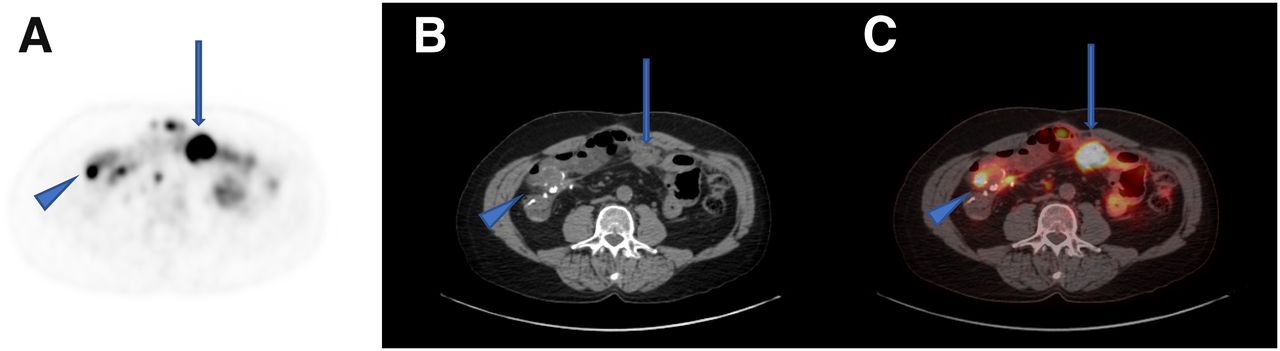
Axial 68Ga-DOTATATE PET (A), attenuation-correction CT (B), and 68Ga-DOTATATE PET/CT (C) demonstrate somatostatin-receptor–expressive peritoneal carcinomatosis (arrows), including peritoneal lesions along anastomotic suture line (arrowheads).
The fourth patient had progressive hepatic and peritoneal disease along with mesenteric and retroperitoneal disease at the time of treatment onset and complained of intermittent pelvic pain. She received 2 cycles of 177Lu-DOTATATE (with prophylactic steroids after each treatment) but discontinued it after developing increased postprandial abdominal pain and vomiting. A CT scan 2 mo after the second treatment demonstrated stable disease with no evidence of bowel obstruction, but with increased tethering of pelvic bowel to tumor. She developed overt bowel obstruction a month later, with dilated small bowel and proximal colon, likely due to pelvic implants, and died 6 mo after her last PRRT treatment.
The fifth patient had progressive hepatic and mesenteric disease at the onset of PRRT treatment. He developed transient abdominal pain and nausea and vomiting 1 wk after his first cycle of PRRT, as well as developing similar symptoms along with radiographic evidence of small-bowel obstruction 1 wk after his second cycle. He was treated with a steroid taper, and his symptoms resolved. Further treatments were held pending a surgical consult.
DISCUSSION
Our experience with intestinal obstruction among patients with mesenteric or peritoneal disease after 177Lu-DOTATATE treatment strongly suggests a cause-and-effect relationship. Radiation can induce an inflammatory response in treated tumors and exacerbate existing desmoplastic fibrosis, a process that is particularly prominent in small-bowel NETs. Intratumoral infiltration of inflammatory cells is thought to underlie the process of pseudoprogression, a phenomenon commonly observed in patients treated with PRRT (10).The development of a frozen abdomen caused by adhesions between bowel and the anterolateral abdominal wall (observed in 2 of the 5 patients in this series) strongly suggests an inflammatory etiology of obstruction. However, it is also important to note that all patients who developed obstruction in this series had increasing mesenteric or peritoneal disease at the time of treatment initiation and were therefore likely to experience bowel obstruction as a complication of disease progression. Two of the 5 patients experienced progressive intermittent abdominal pain even before initiation of treatment with 177Lu-DOTATATE.
It is important to contextualize our findings within the natural history of patients with NETs and abdominal carcinomatosis. A recent analysis of 135 NET patients with peritoneal disease found that both diffuse peritoneal carcinomatosis and the size of peritoneal metastases represented significant risk factors for obstruction, which occurred in 22% of patients during their course of disease (11). Moreover, PRRT was associated with a particularly high risk of abdominal complications such as bowel obstruction and ascites in patients with diffuse peritoneal carcinomatosis while failing to control peritoneal disease in 40% of cases.
The limited data we accumulated on treatment of post-PRRT bowel obstruction suggest that corticosteroids can contribute to the reversal or tapering of the obstructive process. Indeed, the fact that both patients who developed a frozen abdomen were able to temporarily regain oral intake supports a role for steroids in this setting. However, the optimal dose and duration of steroids are unknown. Nor is it clear whether prophylactic steroids play any role in the prevention of bowel obstruction among patients at risk. Ultimately, the benefit of steroids appeared to be transient in patients with advanced peritoneal carcinomatosis.
Limitations of this study are its retrospective, nonrandomized nature, its relatively small population, and the infrequency of the complication of interest (bowel obstruction). A very large, randomized study would be required to conclusively establish a link between 177Lu-DOTATATE treatment and bowel obstruction. In the absence of such data, a multicenter registry might be helpful to identify and quantify uncommon risks of treatment such as obstruction.
CONCLUSION
We observed a temporal relationship between treatment with 177Lu-DOTATATE and bowel obstruction in 5 patients, all of whom had underlying peritoneal and mesenteric metastases. Treating physicians and patients should be aware of this potential complication in high-risk patients. Corticosteroids should be considered as a treatment option in patients who experience bowel obstruction within a short time-frame after 177Lu-DOTATATE.
DISCLOSURE
Jonathan Strosberg has consulted for Novartis and is on the speaker’s bureau for Ipsen and Lexicon. Jason Fleming is an advisor for Glycosbio Food Sciences Inc., Bio-Path Holdings Inc., Natera, and PanTher Therapeutics Inc. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the incidence of bowel obstruction in patients treated with PRRT?
PERTINENT FINDINGS: A comprehensive records review of patients treated with 177Lu-DOTATATE at Moffitt Cancer Center was conducted, with 81 patients identified who were at high risk for bowel obstruction due to existing mesenteric or peritoneal disease. Five patients experienced at least 1 episode of bowel obstruction within 3 mo of treatment. PRRT can lead to bowel obstruction in patients with mesenteric or peritoneal disease, likely by inducing inflammation. Corticosteroids can potentially play a role in treatment and prophylaxis.
IMPLICATIONS FOR PATIENT CARE: Treating physicians and patients should be aware of the potential complication of intestinal obstruction in high-risk patients, and corticosteroids should be considered as a treatment option in patients who experience bowel obstruction within a short time-frame after 177Lu-DOTATATE.
Footnotes
Published online May 22, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 5, 2020.
- Accepted for publication April 29, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Consensus Guideline for the Management of Peritoneal Metastases in Patients with Neuroendocrine Neoplasms
- Sequencing of Somatostatin-Receptor-Based Therapies in Neuroendocrine Tumor Patients
- Outcome on Mesenteric Mass Response of Small-Intestinal Neuroendocrine Tumors Treated by 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy: The MesenLuth Study, a National Study from the French Group of Endocrine Tumors and Endocan-RENATEN Network
- Reply: Bowel Obstruction as a Complication of Peptide Receptor Radionuclide Therapy
- Bowel Obstruction as a Complication of Peptide Receptor Radionuclide Therapy