


Abstract
131I whole-body scintigraphy (WBS) is a highly sensitive method for the detection of differentiated thyroid tumors and metastases. However, a lack of anatomic landmarks and the physiologic accumulation of the tracer complicate interpretation of the images. This prospective study was designed to evaluate the incremental value of 131I SPECT/CT over planar WBS in the management of patients with differentiated thyroid carcinoma (DTC). Methods: Planar imaging was performed on 66 consecutive DTC patients who were considered to have locally advanced or metastatic disease after total or nearly total thyroidectomy. SPECT/CT was added for patients whose planar findings were inconclusive. The planar images were interpreted by 2 experienced nuclear medicine physicians. Interpretation of the SPECT/CT images was a consensus opinion of one of the nuclear medicine physicians and an experienced radiologist. Fusion images were considered to improve image interpretation when they better localized sites of increased 131I uptake. The final diagnosis was verified by pathologic findings, other imaging modalities, and clinical follow-up. Both site-based and patient-based analyses were performed, and the impact of SPECT/CT results on therapeutic strategy was assessed. Results: A total of 232 foci were observed by 131I WBS, including 33.2% of foci localized in the thyroid bed, 62.1% due to malignant lesions, and 4.7% caused by nonthyroidal physiologic or benign uptake or a contaminant. Overall, 37 SPECT/CT studies were performed on 23 patients, whose planar images showed 81 inconclusive lesions. Precise localization and characterization of 131I-avid foci were achieved through 131I SPECT/CT in 69 (85.2%) and 67 (82.7%) of the 81 foci, respectively. Fusion images were considered to be of benefit in 17 (73.9%) of 23 patients. The therapeutic strategy was changed in 8 (47.1%) of 17 patients. Uncommon metastatic lesions were found in 9 (13.6%) of 66 patients with regard to SPECT/CT fusion images. Conclusion: Fusion of SPECT and CT images was of incremental value over WBS in increasing diagnostic accuracy, reducing pitfalls, and modifying therapeutic strategies in 73.9% of DTC patients. As SPECT/CT techniques emerge, 131I SPECT/CT may demonstrate higher value than WBS in the management of DTC.
Recently, combined functional information from nuclear medicine imaging and anatomic information from CT or MRI has been available. Numerous preliminary studies have demonstrated that image fusion is clinically useful through its ability to improve diagnostic accuracy and reporter confidence in many conditions, such as lymphoma (1), melanoma (2), infection (3), parathyroid tumor (4), endocrine neoplasm (5,6), breast cancer (7), and bone disease (8,9).
With regard to SPECT/CT, efforts were initially focused on brain studies using special devices, such as face masks or stereotactic head holders, to facilitate image fusion. Yamamoto et al. (10), using external markers to obtain fusion images, reported 131I SPECT/CT to be clinically useful in patients with differentiated thyroid carcinoma (DTC). By the late 1980s, image fusion had been achieved by a variety of software techniques using internal markers (11). During the last 20 y, these algorithms have become more robust and accurate, and current software algorithms permit accurate coregistration of anatomic and functional images (12). More recently, fused anatomic and functional images could be obtained with integrated SPECT/CT systems providing CT and SPECT images obtained in a single imaging session without moving the patient from the imaging table (13).
DTC is a malignant neoplasm with a good prognosis and low mortality rate, provided that proper therapy is given and systematically monitored. Although the use of PET with 18F-FDG has been suggested for the diagnosis of DTC, the indication is currently limited to patients with high levels of serum thyroglobulin but negative findings on iodine whole-body scintigraphy (WBS) (14). Because of high sensitivity and specificity, thyroglobulin measurement combined with 131I WBS currently remains indispensable for the management of patients with DTC (15). However, a lack of anatomic landmarks and the physiologic or other pathologic uptake of the tracer somewhat complicate interpretation of the images. This prospective study was designed to evaluate the incremental value of 131I SPECT/CT over planar WBS in the management of DTC patients after oral administration of a therapeutic dose of 131I. Uncommon findings via this fusion imaging modality are reported in detail.
MATERIALS AND METHODS
Patients
Sixty-six consecutive DTC patients (27 male, 39 female; age range, 12–78 y; mean age, 51.8 y; 52 with papillary carcinoma, 14 with follicular carcinoma) who were considered to have locally advanced or metastatic disease after total or nearly total thyroidectomy were enrolled in the study. Thyroxine withdrawal for at least 4 wk was required before blood samples were drawn and 131I administered. Serum thyroid-stimulating hormone, thyroglobulin, and thyroglobulin autoantibody levels were measured using a chemiluminescent immunoassay system (Immulite; Diagnostic Products Corp.). Planar imaging including WBS and spot views was performed routinely 5 d after an oral therapeutic dose of 131I (3.7–7.4 GBq). 131I SPECT/CT was added immediately after planar imaging for patients whose planar images showed inconclusive findings; that is, the localization of lesions accumulating 131I was unclear or a malignant origin could not be ruled out. Patients were asked to void and then lie supine with the arms down and immobilized to minimize movement during the acquisition and ensure optimal fusion of images. Approval for the protocol had been received from the ethics board before the beginning of the study. All subjects gave written informed consent to participate in the study.
Imaging Protocol
A hybrid SPECT/CT system (Millennium VG and Hawkeye; GE Healthcare) was used. It consists of a dual-head, variable-angle γ-camera equipped with high-energy parallel-hole collimators and an x-ray tube with a set of detectors mounted on the opposite site of the γ-camera gantry. Planar imaging for WBS was acquired at a speed of 10 cm/min and 5 min for each spot view. CT data were acquired over 360° during 14 s for each transaxial slice. Multiple transmission slices were obtained by moving the table by 1 slice step before acquisition of each subsequent slice. The full field of view consists of 40 slices. SPECT images were acquired in a 128 × 128 matrix, obtaining multiple views over 360° at a 30-s acquisition time per projection with an angular step of 6°. The field of view for SPECT/CT was determined by findings on planar images. Images were reconstructed using Butterworth filtered backprojection (cutoff, 0.5; order, 10). Transverse, sagittal, and coronal slices were generated.
Transmission data were reconstructed at a nuclear medicine workstation (eNTEGRA; GE Healthcare) to obtain cross-sectional attenuation images (256 × 256 matrix) in which each pixel represents the attenuation value of the corresponding tissue. The reconstructed CT data and nuclear medicine data were transmitted to a nuclear medicine database. The matching SPECT and CT data were subsequently fused on a computer workstation by a Digital Imaging and Communications in Medicine network.
Data Analysis
Initially, planar images were assessed by 2 experienced nuclear medicine physicians who were aware of the medical history and the results of the serum thyroid globulin, prior ultrasonographic, and radiologic investigations (CT or MRI). Scintigraphic results were considered to be positive when one or more areas of uptake greater than background activity were identified. A hot nose was considered normal, as was uptake in the thyroid remnant, symmetrically in the salivary glands, and in the gastrointestinal tract and urinary bladder. Diffuse uptake in the liver was also considered normal if functional thyroid tissue was present. Any other areas of radioiodine accumulation were considered abnormal.
The 131I SPECT/CT findings were compared with the findings of planar imaging obtained on a dedicated workstation (eNTEGRA). SPECT/CT was considered contributory if it accurately localized the anatomic site of a hot spot—in particular, when it discriminated between metastatic DTC lesions and physiologic or other pathologic distributions. The SPECT/CT images were interpreted by one of the nuclear physicians and an experienced radiologist, who reached an opinion by consensus.
The SPECT/CT findings were confirmed by pathologic findings; by the findings of other imaging modalities, such as high-resolution ultrasonography, diagnostic CT, and MRI; and by correlation with clinical follow-up of at least 12 mo. Both site-based and patient-based analyses were performed, and the impact of SPECT/CT results on therapeutic strategy was assessed.
RESULTS
In the 66 patients, 232 foci avid for 131I were observed on WBS. According to clinical and imaging follow-up, 77 (33.2%) of 232 foci were localized in the thyroid bed (i.e., thyroid remnant). In 144 (62.1%) of 232 foci, radioiodine accumulation was due to malignant lesions. Eleven (4.7%) of 232 foci were caused by nonthyroidal physiologic or benign uptake or a contaminant. The actual etiology of the 11 foci comprised thymus uptake in 1, ileocecal junction accumulation in 3, cholecystitis or cholecystolithiasis in 2, maxillary sinusitis in 1, and tracer contamination in 4.
Planar images showed conclusive findings in 43 (65.2%) of 66 patients. 131I SPECT/CT was then added immediately after planar imaging for the 23 (34.8%) of 66 patients whose planar images showed inconclusive imaging findings; that is, the localization of lesions accumulating 131I was unclear or a malignant origin could not be ruled out. Interpretation of the planar images indicated that equivocal uptake was seen in the cervical region in 15 patients, outside the neck in 14 patients, and both in and outside the neck in 6 patients. In these 23 patients, 81 equivocal foci were found by planar imaging, including 36 foci in the neck and 45 foci outside the neck, which included head/skull, chest, abdomen/pelvis, and extremities. Precise localization was determined by 131I SPECT/CT for 69 (85.2%) of 81 foci. Also, precise characterization was achieved for 67 (82.7%) of 81 foci, including 24 foci due to physiologic or benign uptake or contamination and 43 malignant lesions.
Overall, the number of 131I SPECT/CT studies performed on the 23 patients was 37, with an average number of 1.6 SPECT/CT studies per patient (37/23). Of these 37 SPECT/CT studies, 9 were performed on 9 patients with lesions only in the neck, 19 were performed on 8 patients with lesions only outside the neck, and 9 were performed on 6 patients with lesions both in the neck and outside the neck. Of these 9 SPECT/CT studies performed on 6 patients with lesions both in the neck and outside the neck, 3 studies on 3 patients evaluated lesions both in the neck and adjacent to the neck simultaneously and 6 studies on 3 patients evaluated lesions either in the neck (3 studies) or distant from the neck (3 studies). As a result, the numbers of SPECT/CT studies for lesions in the neck and for lesions outside the neck were 15 and 25, respectively. The average numbers of SPECT/CT studies per patient performed for further evaluation of inconclusive planar imaging findings were 1.0 (15/15) for lesions in the neck and 1.8 (25/14) for lesions outside the neck. In evaluations of foci in the neck and outside the neck, SPECT/CT was found to have an incremental value in 11 (73.3%) of 15 and 21 (84.0%) of 25 studies, respectively.
Table 1 summarizes the detailed data for 17 (73.9%) of 23 patients for whom additional conclusive information was provided by 131I SPECT/CT fusion imaging after planar imaging. In particular, all the lesions accumulating 131I were precisely localized and were given final diagnoses. Equivocal foci were characterized as metastases in 16 (94.1%) of the 17 patients and as physiologic activity in only 2 patients (patients 4 and 15) by 131I SPECT/CT. 131I SPECT/CT findings for the 17 patients were confirmed by pathologic examination in 8 patients, ultrasonography in 6 patients, MRI or CT in 10 patients, repeated scanning in only 1 patient, and correlation with clinical follow-up of up to 20.0 ± 10.9 mo (mean ± SD) in all 17 patients. Among these 17 patients, the therapeutic strategy was changed for 8 (47.1%), including a change to surgery in 6 patients (patients 1, 3, 4, 5, 7, and 8), to external-beam radiotherapy in 1 patient (patient 6), and to interventional therapy in 1 patient (patient 2).
Data for Patients with Additional Information Provided by 131I SPECT/CT
However, SPECT/CT findings remained equivocal and required further investigation in 3 (13.0%) of 23 patients; that is, 3 (8.1%) of 37 SPECT/CT findings were concordant with the planar imaging findings. Site-based analysis revealed that 5 (6.2%) of 81 lesions remained inconclusive in these 23 patients. Based on clinical and imaging follow-up, the final diagnoses were sphenoid bone metastasis in 1 patient, maxillary sinusitis in 1 patient, and inflammatory lung disease in 1 patient. In addition, 9 (11.1%) of 81 foci detected by WBS in 3 (13.0%) of 23 patients could not be visualized on 131I SPECT/CT. According to follow-up, the final diagnoses included physiologic uptake, contamination, and lung metastases.
Uncommon metastatic lesions were found in 9 (13.6%) of 66 patients on 131I SPECT/CT: 2 patients with metastatic lesions in subcutaneous soft tissues, 3 patients with metastatic lesions in the parapharyngeal space (Fig. 1), 2 patients with metastatic lesions in muscles, 1 patient with a metastatic lesion in a salivary gland, and 1 patient with a metastatic lesion in the appendicular skeleton.
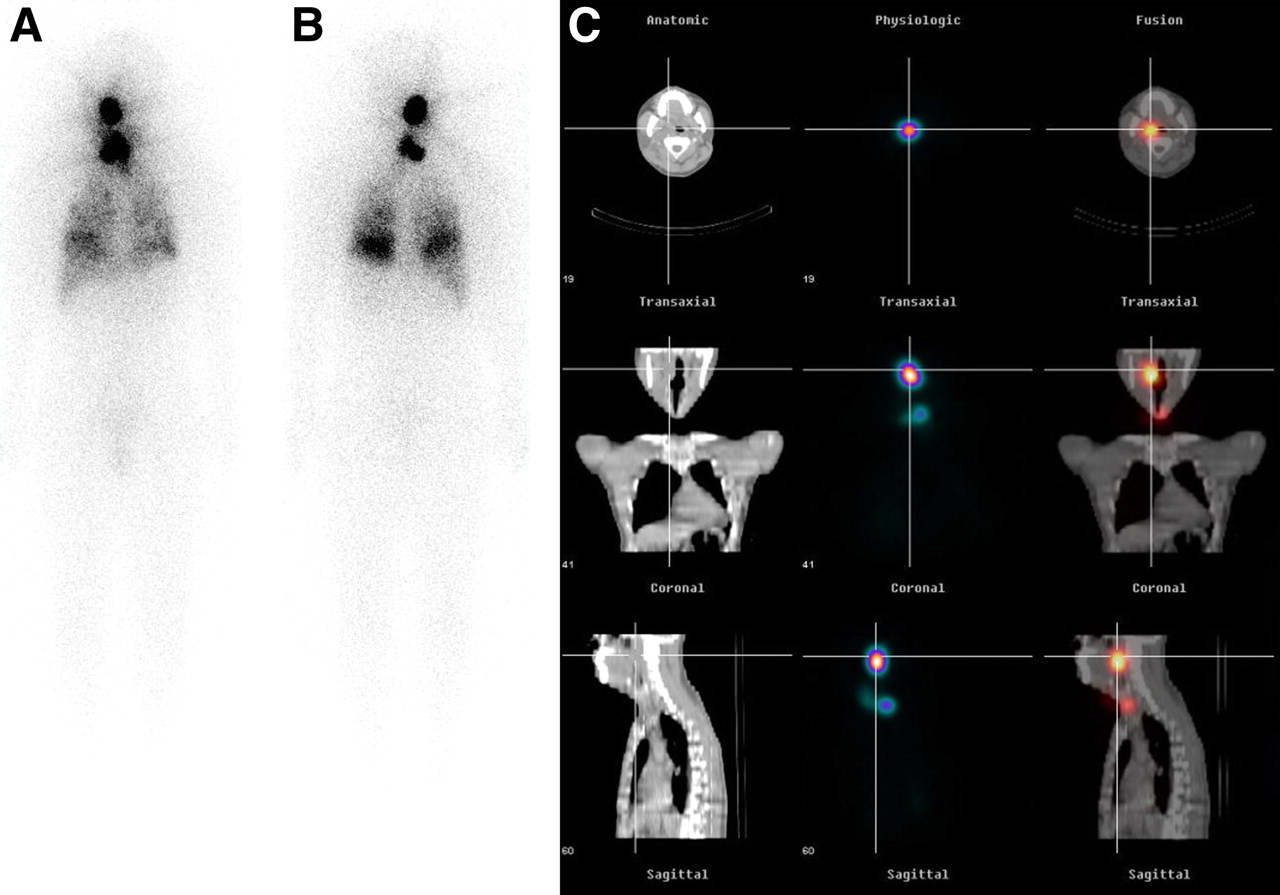
A 43-y-old woman (patient 6) who had undergone nearly total thyroidectomy for follicular thyroid carcinoma was referred for 131I therapy because of lung metastases. WBS showed 131I accumulation in head, neck, and lungs (A, anterior view; B, posterior view). 131I SPECT/CT fusion images (C: left, CT; middle, SPECT; right, 131I SPECT/CT) revealed prestyloid parapharyngeal space metastasis and thyroid remnant. In this patient, final diagnosis of metastasis from follicular thyroid carcinoma was based on findings of fine-needle aspiration biopsy. Because surgery was refused, adjuvant external-beam radiotherapy was performed to relieve dysphagia caused by progressively growing parapharyngeal metastasis, followed by radioiodine therapy.
DISCUSSION
Thyroid carcinoma accounts for roughly 1% of all new malignant diseases. Of these, at least 94% are DTC—either papillary thyroid carcinoma or follicular thyroid carcinoma, both of which keep some of the morphologic and functional characteristics of follicular epithelium. The primary treatment of DTC is total or nearly total thyroidectomy with or without lymph node dissection (16). In the present study, all patients who had undergone total or nearly total thyroidectomy were considered to have locally advanced or metastatic disease. This may explain the high prevalence (62.1%) of malignant foci and the fact that the main advantage of SPECT/CT was in localizing metastases but not in excluding disease from sites of physiologic uptake. On the other hand, the fact that uptake in thyroid remnants was considered physiologic and that disease could have been missed because of neglect to perform SPECT/CT after planar imaging could introduce a selection bias, excluding a certain number of patients who would have benefited from SPECT/CT assessment.
The sensitivity of radioiodine imaging depends on the given radioactivity. Therefore, low-activity diagnostic 131I WBS (74–185 MBq) has a lower detection rate than a high-activity posttherapy scan (3,700–7,400 MBq) (17). In our study, all patients had undergone thyroxine withdrawal of at least 4 wk and had received an oral therapeutic dose of 131I, which optimized the results of 131I WBS and SPECT/CT. The unique feature of these 2 imaging modalities is the ability to localize recurrent or metastatic disease and to exclude benign uptake, which is complementary to the examination of serum thyroglobulin level. However, our study demonstrated that SPECT/CT findings remained equivocal or could not visualize the foci in a few patients, and further investigations were still needed for precise localization and characterization of uptake in these patients. The main causes include the low amount of radioiodine accumulated by the lesion and the low resolution of the CT scan.
Common metastatic sites of DTC and their corresponding therapeutic methods have been discussed in detail, including lymph node metastasis to the neck and mediastinum (18,19), osseous metastasis, and pulmonary metastasis (20,21). However, fewer reports concentrating on DTC metastases to other organs can be found. In this study, we reported some relatively uncommon findings via fusion of SPECT and CT images, such as subcutaneous soft-tissue metastasis, soft-tissue metastasis in the parapharyngeal space, parotid gland metastasis, erector spinae metastasis, and femoral metastasis.
Hybrid SPECT/CT has many clinical applications; however, relatively few reports have been published on its application to the imaging of thyroid carcinoma. In 2004, Tharp et al. reported that SPECT/CT had an incremental diagnostic value, compared with planar imaging, in 57% of the 71 patients with thyroid carcinoma in a retrospective study (22). At the same time, Ruf et al. performed a prospective study and concluded that the addition of SPECT/CT improved the interpretation of inconclusive 131I findings on planar scans after ablative radiotherapy (23). In addition, the role of 131I SPECT/CT in DTC patients has been described in a few case reports, including detection of benign struma ovarii in a patient with invasive papillary thyroid cancer (24), renal metastases from follicular thyroid cancer (25), and retained radioiodine in the respiratory tract of a patient with papillary thyroid carcinoma (26). In our series, the hybrid imaging device provided a significant contribution in up to 73.9% of patients whose 131I WBS findings were inconclusive, thus having a substantial impact on the clinical management of DTC patients referred for radioiodine therapy. This ability is of particular importance because the therapeutic approaches to different metastatic DTC lesions are completely different (27). Compared with previous literature data on the same topic, patients enrolled in our prospective study were considered to have locally advanced or metastatic disease after thyroidectomy and given a therapeutic dose of radioiodine, which may have contributed to the much more encouraging results. On the other hand, our SPECT/CT studies were performed only on patients whose planar images showed inconclusive imaging findings. Theoretically, finding a few lesions on SPECT/CT but not on planar imaging may compromise the incremental value of the former. Image-based techniques were suboptimal because of possible movement by the patient between the 2 scans and the relative complexity of the preparation. In the present study, SPECT/CT hybrid systems allowed functional and morphologic images to be acquired in a single session, thus eliminating many possible pitfalls of the image-based fusion methods and the need for complex algorithms. As an alternative, all patients were asked to cooperate and were immobilized to minimize movement during the acquisition. Moreover, low-dose CT allows for attenuation correction, thereby improving SPECT image quality (28).
Our study also indicated that lesions can be identified by planar scanning in most patients with DTC and that 131I SPECT/CT after planar scanning should be considered in selected patients with inconclusive planar scan results. Although we describe the incremental value of SPECT/CT in the management of DTC, 131I WBS is still an initial and primary method for the detection of this disease. Because not all 66 patients underwent SPECT/CT, whether planar imaging was accurate enough in those who did not undergo SPECT/CT was determined by follow-up. On the other hand, because, in more than one third of foci detected by 131I WBS, radioiodine uptake was found not to be due to malignancies, other diagnostic tools including testing of the thyroglobulin level, ultrasonography, MRI, and even delayed scanning may be helpful in selecting appropriate patients for 131I SPECT/CT, especially patients with foci in the neck.
The clinical usefulness of fusion of 131I SPECT and CT images in patients with DTC has been demonstrated using an external marker (10). A hybrid SPECT/CT system, the first commercial SPECT/CT system (which was developed in 1999), was used in the present study (13). The x-ray portion operated at 140 kVp with a tube current of only 2.5 mA, resulting in a significantly lower patient dose than what would be delivered using a conventional CT scanner. This is especially advantageous to patients whose SPECT/CT findings allow the exclusion of metastatic lesions. In contrast to other image fusion techniques, SPECT/CT can be performed easily using the hybrid system, requiring almost no patient preparation or special logistics before imaging. However, the quality of the CT images was inferior to that of images obtained with state-of-the-art CT scanners. The integrated low-dose CT images provided by the Hawkeye system are of little diagnostic value, as they do not possess the image properties of diagnostic CT images. This is especially disadvantageous to surgical candidates who need a contrast-enhanced high-resolution diagnostic CT scan to evaluate the extent of disease and the relationship of lesions to vascular structures. As SPECT/CT techniques emerge, 131I SPECT/CT may demonstrate higher value than WBS in the management of DTC.
CONCLUSION
131I SPECT/CT after planar imaging represents a new imaging modality for DTC patients who have received an oral therapeutic dose of 131I. In this study, the fusion of SPECT and CT images was of incremental value over WBS in increasing diagnostic accuracy, reducing pitfalls, and modifying therapeutic strategies in 73.9% of DTC patients through precise localization and characterization of 131I-avid foci. As SPECT/CT techniques emerge, 131I SPECT/CT may demonstrate higher value than WBS in the management of DTC.
Acknowledgments
We thank Shiwei Sheng and Qiong Luo for collecting most of the clinical data; Changqing Jin, Hong Ji, Jianfang Yu, and Cide Ding for technical help; and Prof. Yingjian Zhang for helpful discussions. This work was sponsored by the National Natural Science Foundation of China (30700187), Shanghai Rising-Star Program (08QA14040), and the Public Health Bureau of Shanghai Municipality (2006Y34).
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication March 3, 2008.
- Accepted for publication August 14, 2008.





{kind=link}
Jump to section
Related Articles
Cited By...
- Unexplained Hyperthyroglobulinemia in Differentiated Thyroid Cancer Patients as an Indication for Radioiodine Adjuvant Therapy: A Prospective Multicenter Study
- Appropriate Use Criteria for Nuclear Medicine in the Evaluation and Treatment of Differentiated Thyroid Cancer
- Radioiodine Scintigraphy with SPECT/CT: An Important Diagnostic Tool for Thyroid Cancer Staging and Risk Stratification
- Post-operative neck ultrasound and risk stratification in differentiated thyroid cancer patients with initial lymph node involvement
- Recombinant Human TSH Versus Thyroid Hormone Withdrawal
- The SNMMI Practice Guideline for Therapy of Thyroid Disease with 131I 3.0
- Radioiodine Scintigraphy with SPECT/CT: An Important Diagnostic Tool for Thyroid Cancer Staging and Risk Stratification
- Rare metastases of differentiated thyroid carcinoma: pictorial review
- The Effect of Posttherapy 131I SPECT/CT on Risk Classification and Management of Patients with Differentiated Thyroid Cancer
- The Significance of 99mTc-MAA SPECT/CT Liver Perfusion Imaging in Treatment Planning for 90Y-Microsphere Selective Internal Radiation Treatment
- Single photon emission computed tomography (SPECT)/computed tomography using Iodine-123 in patients with differentiated thyroid cancer: additional value over whole body planar imaging and SPECT