


Abstract
For decades, several amino acid PET tracers have been used to optimize diagnostics in patients with brain tumors. In clinical routine, the most important clinical indications for amino acid PET in brain tumor patients are differentiation of neoplasm from nonneoplastic etiologies, delineation of tumor extent for further diagnostic and treatment planning (i.e., diagnostic biopsy, resection, or radiotherapy), differentiation of treatment-related changes such as pseudoprogression or radiation necrosis after radiation or chemoradiation from tumor progression at follow-up, and assessment of response to anticancer therapy, including prediction of patient outcome. This continuing education article addresses the diagnostic value of amino acid PET for patients with either glioblastoma or metastatic brain cancer.
Contrast-enhanced anatomic MRI is the diagnostic method of choice for patients with primary (gliomas) and secondary (brain metastases) brain cancer because of excellent soft-tissue contrast, high spatial resolution, and widespread availability (1,2). Anatomic MRI is also an essential component of almost all clinical trials on brain tumor patients, based on its ability to generate surrogate endpoints (e.g., MRI findings consistent with complete or partial response or progressive disease) that can be correlated with progression-free and overall survival. On the other hand, its specificity for tumor tissue is suboptimal, resulting in challenges in distinguishing cancer from nonneoplastic lesions at initial presentation; delineating tumor extent, especially in nonenhancing tumors; and differentiating treatment-related changes from tumor relapse (1,3–8). Irrespective of a continuously expanding number of advanced MRI sequences, other modalities—especially PET using multiple radiolabeled molecules—have been evaluated over the past few decades to overcome these limitations of anatomic MRI. In particular, the PET task force of the Response Assessment in Neuro-Oncology Working Group emphasized that the additional clinical value of amino acid PET for glioma patients, compared with anatomic MRI, is outstanding and justifies its widespread clinical use at all disease stages (9). In addition, the PET/Response Assessment in Neuro-Oncology Working Group has published recommendations for using amino acid PET in patients with brain metastases (10).
Although various new applications have been addressed recently using PET techniques (e.g., noninvasive grading in primary brain tumors characterized according to older classifications of the World Health Organization [WHO] (11), noninvasive prediction of molecular markers, diagnosis of malignant progression, and the prognostic value of PET in patients with newly diagnosed and untreated brain tumors), for neurooncologists and medical professionals involved in the care of patients with brain tumors, the following PET applications are of particular clinical interest: differentiation of neoplasms from nonneoplastic etiologies, delineation of tumor extent for further diagnostic and treatment management, differentiation of treatment-related changes such as pseudoprogression or radiation necrosis after radiation or chemoradiation from tumor relapse at follow-up, and prediction of response to anticancer therapy as evaluated by patient outcome. This continuing education article addresses the diagnostic value of amino acid PET for these clinically highly relevant indications in patients with either glioblastoma or metastatic brain cancer.
RADIOLABELED AMINO ACIDS
The most widely used amino acid tracers for PET to date are O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET), 11C-methyl-l-methionine (11C-MET), and 3,4-dihydroxy-6-18F-fluoro-l-phenylalanine (18F-FDOPA). Their uptake is facilitated by large neutral amino acid transporters of the L-type (LAT) in gliomas and brain metastases (i.e., subtypes LAT1 and LAT2), which are regularly overexpressed in both brain tumor types (1,12–15). Most early amino acid PET studies used 11C-MET, but the short half-life of 20 min imposes logistic challenges, necessitating an on-site cyclotron (16,17). The advent of 18F-labeled radiolabeled amino acids with a considerably longer half-life of 110 min allowed transport to other neurooncologic centers. For example, 18F-FET was developed almost 25 y ago, and its use has multiplied (16,18,19), resulting in 11C-MET replacement, especially in Europe (1). After being moved by LAT transporters into neoplastic tissue, 18F-FET is not metabolized (20), whereas 11C-MET shows incorporation into protein, participation in other metabolic pathways, or metabolic degradation (21).
18F-FDOPA is another 18F-labeled amino acid analog initially developed to evaluate dopamine synthesis in the basal ganglia and has also increasingly been used for imaging brain tumors (22). In the United States and Europe, 18F-FDOPA is approved for characterizing presynaptic dopaminergic activity in patients with Parkinsonian syndromes, and in Europe 18F-FDOPA has also been approved for imaging of brain tumors and various neuroendocrine tumors. Notably, physiologic uptake of 18F-FDOPA in the striatum may hamper its use in evaluating tumor extent (1,23). On the other hand, uptake in the striatum can also be used as a reference for qualitative (visual) analysis of tumor uptake.
Acquisition of dynamic amino acid PET data (predominantly using the tracer 18F-FET) allows characterization of the temporal pattern of tracer uptake by deriving a time–activity curve. Subsequently, qualitative and quantitative dynamic uptake parameters such as the configuration of time–activity curves, time to peak, and slope can be calculated for further data analysis to increase diagnostic performance, such as for diagnosis of treatment-related changes (24,25). Initial data suggest that the dynamic 18F-FDOPA PET acquisition is also of value for differentiating glioma progression from treatment-related changes (26).
Although first used for brain tumor imaging in 1999 (27), the synthetic amino acid analog anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (18F-fluciclovine) has gained clinical interest, particularly for imaging of primary and secondary brain tumors in recent years. Since this tracer was initially used primarily to diagnose prostate cancer recurrence (28), 18F-fluciclovine was approved in the United States and Europe for evaluating recurrent prostate cancer (29), but the tracer also received orphan drug status for glioma imaging in the Unites States. Transport of 18F-fluciclovine is mediated to some extent by LAT1 but predominantly by another neutral amino acid transporter, the neutral alanine, serine, cysteine transporter 2, which is not expressed at the luminal side of the blood–brain barrier (30). In general, significantly higher tumor-to-brain contrast is observed with 18F-fluciclovine than with the established amino acid tracers (31), primarily because of the low transport of 18F-fluciclovine through the intact blood–brain barrier. Like 11C-MET, 18F-FET, and 18F-FDOPA, it appears that 18F-fluciclovine accumulates also in nonenhancing gliomas and identifies infiltrating tumor areas that do not show contrast enhancement on MRI (32,33).
In general, all radiolabeled amino acids exhibit relatively low uptake in normal brain tissue, and brain tumors can easily be distinguished from the surrounding healthy-appearing brain tissue with high contrast. Of note, the use of 18F-FDG—the most widely applied PET tracer in oncology—in distinguishing tumor tissue from normal tissue is limited by the physiologically increased rate of glucose metabolism in the cerebral cortex. Therefore, in recent years, radiolabeled amino acids have become the preferred PET probes in neurooncology (1,9,10,34).
DIFFERENTIATION OF NEOPLASM FROM NONNEOPLASTIC ETIOLOGIES
In general, neoplastic lesions such as glioblastoma or brain metastases exhibit a considerably higher uptake of radiolabeled amino acids than do nonneoplastic lesions, a factor that may be considered for differential diagnosis. A metaanalysis including more than 450 patients from 13 18F-FET PET studies yielded a pooled sensitivity of 82% and specificity of 76% for diagnosing primary brain tumors (35). In that study, most patients had gliomas (n = 338; 84%) of various central nervous system (CNS) WHO grades. Eighteen patients had a nonglial brain tumor (5%). Across all tumor types, a mean tumor-to-brain ratio of 1.6 and a maximum tumor-to-brain ratio of 2.1 best separated primary neoplastic lesions from nonneoplastic lesions. A large single-center study including 393 patients observed comparable diagnostic performance (36). In that study, 68 patients were diagnosed with glioblastoma (17%). Of note, in that study, 18F-FET uptake was evaluated only visually by a single nuclear medicine physician, and the results should be considered with caution (37). Another study of 174 patients with newly diagnosed cerebral lesions suggestive of brain tumors reported a high specificity (92%) but a lower sensitivity (57%) for the differentiation of neoplastic lesions from nonneoplastic lesions using 18F-FET PET (38). On the other hand, a maximum tumor-to-brain ratio of more than 2.5 yielded a convincing positive predictive value of 98% for tumor tissue. For 11C-MET PET, a series of 196 consecutive patients revealed that differentiation between gliomas and nontumoral lesions using a simple threshold was correct in 79% (39). Similar findings were recently observed in 101 pretreatment patients (40).
Thus, amino acid PET adds valuable information for differential diagnostics of suggestive CNS lesions for glial brain tumors, but neuropathologic tissue evaluation remains mandatory in most patients to provide a final diagnosis. Nevertheless, it should be kept in mind that mild but increased amino acid tracer uptake may also occur—although it is much less common—in nonneoplastic lesions (e.g., acute or subacute brain ischemia, brain abscess, inflammatory lesions related to active multiple sclerosis, or status epilepticus) (41–46). In addition, 20%–30% of patients with gliomas of CNS WHO grade 2 with an isocitrate dehydrogenase (IDH) gene mutation exhibit no amino acid uptake (42,43,47,48).
A subgroup of patients who had brain lesions without 18F-FET uptake but with MRI findings suggestive of CNS WHO grade 2 gliomas (i.e., hyperintense T2/fluid-attenuated inversion recovery [FLAIR] signal without contrast enhancement) may even show photopenic defects on 18F-FET PET with uptake visually lower than the healthy background uptake but harbor gliomas of higher CNS WHO grades (49). This phenomenon has also been described for the radiolabeled amino acids 11C-MET and 18F-FDOPA (50).
In most patients with metastatic brain cancer, even small brain metastases (maximal diameter, <5 mm) can easily be delineated by contrast-enhanced anatomic MRI. In addition, the increased expression of amino acid transporters in brain metastases is a compelling target for amino acid PET (13). For example, in 30 patients with 45 newly diagnosed brain metastases from cancer of different origins, approximately 90% of the lesions had a 18F-FET uptake of 1.6 or more compared with the healthy-appearing contralateral hemisphere. In particular, in all lesions with a diameter larger than 1 cm, the 18F-FET uptake was pathologically increased (51). A similar dependence on lesion size was observed in patients with newly diagnosed brain metastases evaluated using 18F-fluciclovine PET (52). Nevertheless, the most commonly used imaging modality for brain metastasis detection remains thin-slice contrast-enhanced MRI, which has the highest sensitivity for this application.
In contrast to extracranial cancer, the value of 18F-FDG PET for brain metastasis detection appears to be limited. For example, a metaanalysis revealed 18F-FDG PET to have a cumulative sensitivity of only 21% for diagnosis of brain metastases secondary to lung cancer (53).
DELINEATION OF TUMOR EXTENT
Regarding delineation of tumor extent in glioma patients, anatomic MRI is particularly limited in its ability to identify nonenhancing glioma subregions (1). Radiolabeled amino acids for PET can pass the intact blood–brain barrier (54,55). Predominantly in nonenhancing gliomas, several studies have spatially compared amino acid tracer uptake with neuropathologic findings obtained by stereotactic biopsy and shown that radiolabeled amino acids identify glioma extent more reliably than standard MRI (56–62). Furthermore, in patients with an MRI-based suspicion of a CNS WHO grade 2 glioma (typically a T2-hyperintense lesion without contrast enhancement on MRI), amino acid PET parameters obtained from both static and dynamic acquisitions correlated neuropathologically with the most malignant tumor parts (56–62)—a finding that is of considerable interest for prognostic evaluation and the planning of diagnostic and therapeutic interventions (e.g., biopsy and target volume definition for radiotherapy).
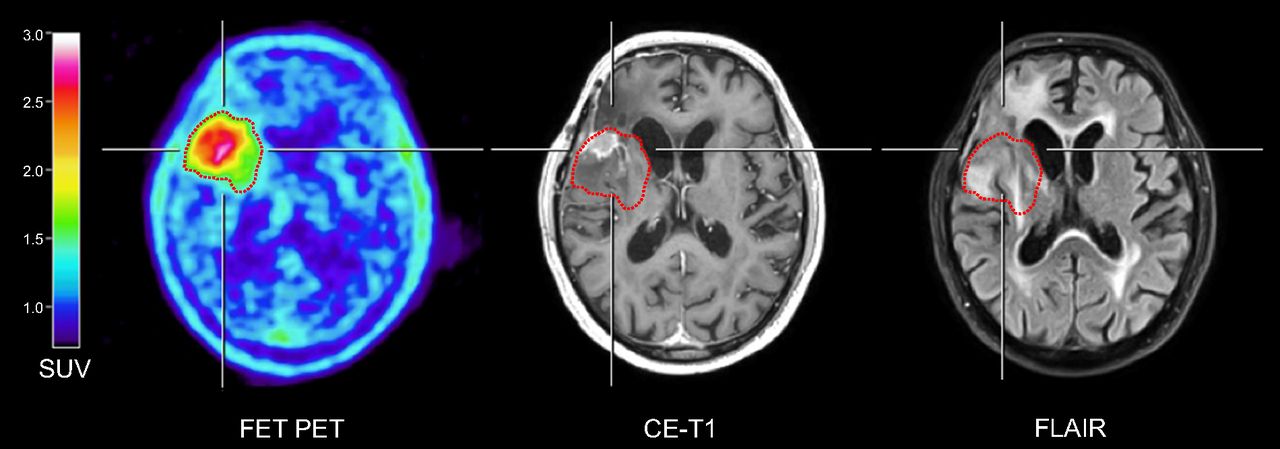
In terms of volumetric comparison of contrast enhancement with the tumor volume obtained by amino acid PET, previous studies of both newly diagnosed and recurrent IDH–wild-type glioblastomas suggested that there are significant differences in the size, overlap, and spatial correlation of tumor volumes (3,63,64), indicating that conventional contrast-enhanced MRI considerably underestimates the metabolically active tumor volume (Fig. 1). Consequently, efforts have been initiated to evaluate whether an amino acid PET–guided treatment may improve patient outcomes. Initial studies suggested that amino acid PET–based radiotherapy significantly affects patient survival (65,66).

18F-FET PET, contrast-enhanced MRI, and FLAIR MRI of 89-y-old patient with recurrent IDH–wild-type glioblastoma. Metabolically active tumor as identified by increased uptake of 18F-FET (threshold of 1.6 based on mean tumor-to-brain ratio) is outlined and projected onto MR images (red contour). Extent of metabolically active tumor on 18F-FET PET exceeds contrast-enhancing tumor portion and shows considerable spatial discrepancies from area of FLAIR hyperintensities. CE = contrast-enhanced.
In contrast to gliomas, the size and volume of brain metastases are usually well delineated on contrast-enhanced MRI because of fewer infiltrative growth characteristics on a submillimeter level (67). Thus, for biopsy or treatment planning, amino acid PET does not add valuable information on extent, as reported for patients with newly diagnosed gliomas (58,68).
DIFFERENTIATION OF TUMOR RELAPSE FROM TREATMENT-RELATED CHANGES
After treatment for brain tumors, differentiation of treatment-related changes from actual tumor relapse remains challenging (1,4,8,69,70) and is of paramount clinical relevance, with considerable impact on clinical management. For example, a recent retrospective study of 189 patients found that amino acid PET changed clinical management in 53% of patients with suspected recurrent disease (71). Erroneous interpretation of treatment-related changes as tumor progression may lead to unnecessary and premature termination of an effective treatment option, with a subsequent potentially negative impact on survival. Furthermore, the efficacy of the subsequent treatment (72) may be overestimated, generating misleading results in studies evaluating recurrent treatment options (73).
In clinical routine, this differentiation is the most frequent indication for amino acid PET and is requested in almost 50% of glioma patients (74). In patients with predominantly IDH–wild-type glioblastoma, high diagnostic accuracy has repeatedly been shown for amino acid PET using 18F-FET and 18F-FDOPA in differentiating between tumor progression and treatment-related changes that occur early (i.e., pseudoprogression after chemoradiation plus temozolomide within the first 3 mo) or late (e.g., radiation necrosis, onset usually > 6 mo after radiotherapy completion) (24,69,75–82). In these studies, differentiation was correct 80%–90% of the time. For 11C-MET PET, diagnostic performance appears to be slightly lower, with an accuracy of approximately 75% (83,84), most probably related to a higher affinity of 11C-MET for inflammatory lesions (85). A recent prospective study evaluated 18F-fluciclovine PET for diagnosing pseudoprogression and provided 90% sensitivity and 83% specificity for this clinically relevant indication (86). Importantly, PET findings were validated neuropathologically in that study in all patients (n = 30).
In patients with brain metastases, radiosurgery has become an indispensable and frequently used local treatment option (10,87). Depending on the irradiated lesion volume and radiation dose, an increased radiation necrosis rate has been reported in patients with brain metastases treated by radiosurgery (88). For differentiation of local radiation injury such as radiation necrosis from brain metastasis relapse after radiosurgery, PET using 18F-FDOPA and 11C-MET has consistently demonstrated high sensitivity and specificity of approximately 80% (Fig. 2) (83,89–92). Similarly, 18F-FET PET parameters derived from static and dynamic acquisitions showed high sensitivity and specificity of 80%–90% for distinguishing radiation-induced changes after radiosurgery from recurrent brain metastases (25,93,94). A recent metaanalysis including 13 11C-MET, 18F-FET, or 18F-FDOPA PET studies with almost 400 patients highlighted the added clinical value of amino acid PET for differentiating treatment-related changes from brain metastasis relapse (95). In that study, pooled sensitivity and specificity were 82% and 84%, respectively.

A 68-y-old woman with brain metastasis secondary to renal cell carcinoma who underwent anatomic MRI and 18F-FDOPA PET. Twelve months after resection with postoperative radiosurgery, MRI suggested local tumor recurrence. In contrast, 18F-FDOPA PET showed no increased metabolic activity (mean tumor-to-brain ratio, 1.0) indicating treatment-related changes such as radiation injury. Diagnosis was confirmed by subsequent neuroimaging 3 mo later, including amino acid PET and anatomic MRI, demonstrating unchanged imaging findings and stable clinical course without any therapeutic intervention. CE = contrast-enhanced.
In most of these studies, radiation-induced changes were distinguished from brain metastasis relapse solely on the basis of a single amino acid PET scan. A recent study evaluated serial amino acid PET scans and suggested that stable 18F-FDOPA uptake over a long-term follow-up (median, 18 mo) identified radiation-induced changes with a relatively high accuracy of 94% (96). 18F-FDOPA uptake did not change significantly in radionecrotic lesions but did increase significantly over time in patients with brain metastasis relapse.
Checkpoint inhibitor immunotherapy as a systemic treatment option has considerable efficacy in patients with brain metastases, showing intracranial objective response rates of almost 60% (97,98). On the other hand, reactive changes on MRI may also occur after these systemic treatment options and can also be challenging to distinguish from brain metastasis relapse. For example, pseudoprogression related to inflammation triggered by immune system reactions may occur in patients with brain metastases treated with immune checkpoint inhibitors using antibodies against cytotoxic T-lymphocyte–associated antigen 4 (e.g., ipilimumab), programmed death protein 1 (e.g., pembrolizumab and nivolumab), or programmed cell death ligand 1 (e.g., atezolizumab). A pilot study highlighted the potential of amino acid PET using 18F-FET to identify pseudoprogression in patients with melanoma brain metastases treated with blockade of cytotoxic T-lymphocyte–associated antigen 4 (99). A subsequent study confirmed the potential of amino acid PET in patients undergoing immune checkpoint inhibition; pseudoprogression was detected in a higher number of patients with brain metastasis secondary to lung cancer or melanoma (100).
ASSESSMENT OF TREATMENT RESPONSE
In glioma patients, changes in the extent of contrast enhancement on MRI are typically used as an indicator of complete or partial response or tumor progression (72,101). In addition, in patients treated with antiangiogenic agents for glioblastoma recurrence, an increase in signal hyperintensity on T2 or FLAIR MRI sequences was frequently used to diagnose nonenhancing tumor progression (72). Nevertheless, these signal changes are unspecific and may be related to perifocal edema, radiation injury, demyelination, inflammation, or ischemia, hampering the distinction from nonenhancing tumor (4,8,70). Alternative diagnostic methods such as amino acid PET have been evaluated to improve treatment response assessment. In glioblastoma patients, alkylating chemotherapy and antiangiogenic therapy are frequently applied systemic treatment options.
For 11C-MET PET, a reliable response assessment to temozolomide and nitrosourea-based chemotherapy has been demonstrated primarily in glioblastoma patients at recurrence (102–105). Notably, metabolic responders on 11C-MET PET had a significantly improved outcome compared with metabolic nonresponders (102). Subsequently, 18F-FET PET has been used to evaluate the effects of temozolomide in patients with CNS WHO grade 2 gliomas (106). In metabolic responders, 18F-FET PET tumor volume reductions after treatment initiation were observed considerably earlier than volume reductions on FLAIR MRI. These findings were confirmed by subsequent 18F-FET PET studies with more patients (107,108).
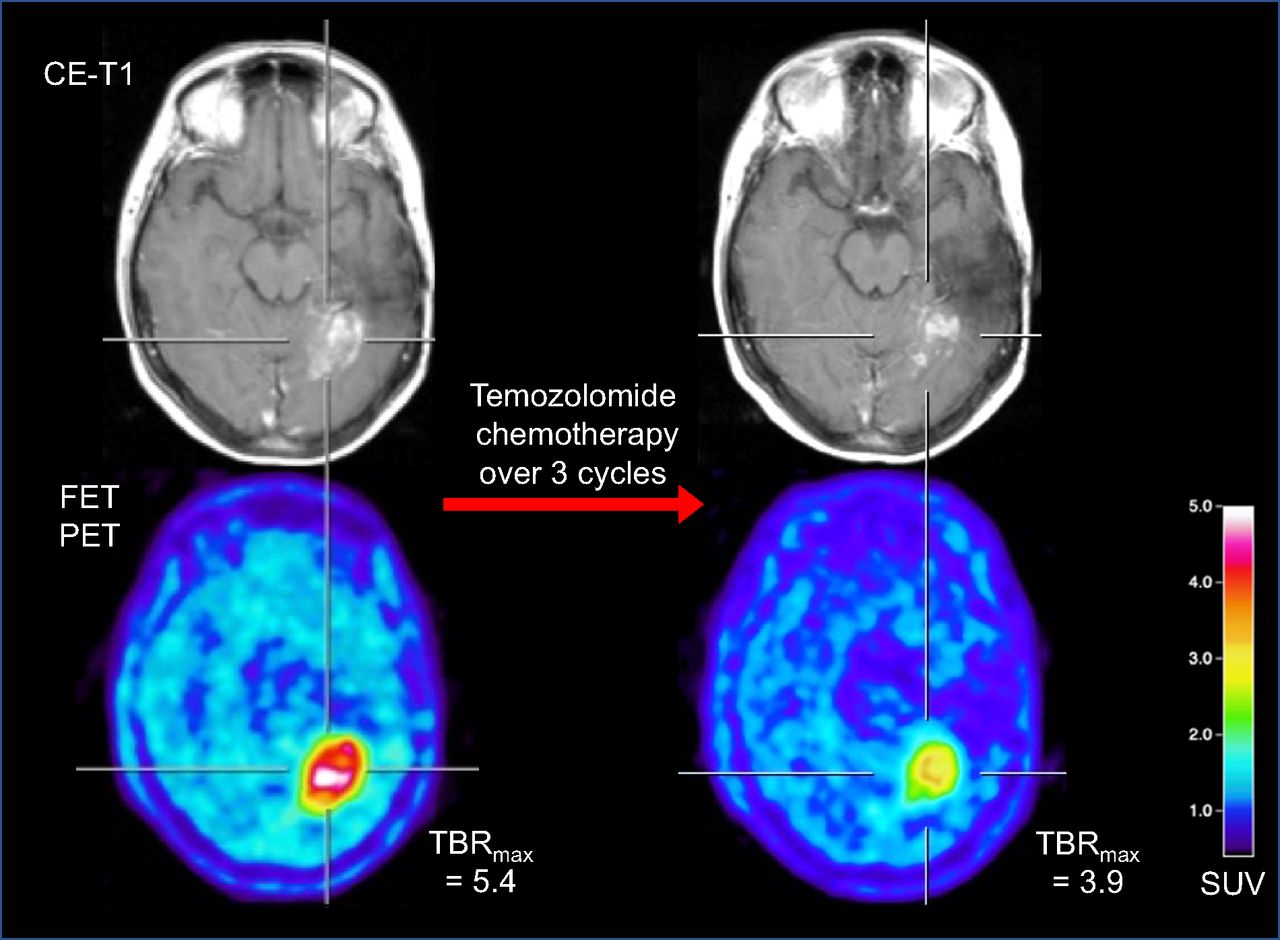
In patients with newly diagnosed IDH–wild-type glioblastoma, prospective studies assessed the predictive value of early 18F-FET uptake changes 6–8 wk after postoperative chemoradiation with concomitant temozolomide relative to the baseline scan (109,110). 18F-FET PET responders with a decrease in metabolic activity as assessed by tumor-to-brain ratios had significantly longer survival than patients with stable or increasing tracer uptake after chemoradiation. Similar findings were reported in newly diagnosed glioblastoma patients early after initiating adjuvant temozolomide chemotherapy, that is, after 2 cycles (111). An example for response assessment of temozolomide chemotherapy used in a patient with a progressive glioblastoma is shown in Figure 3.
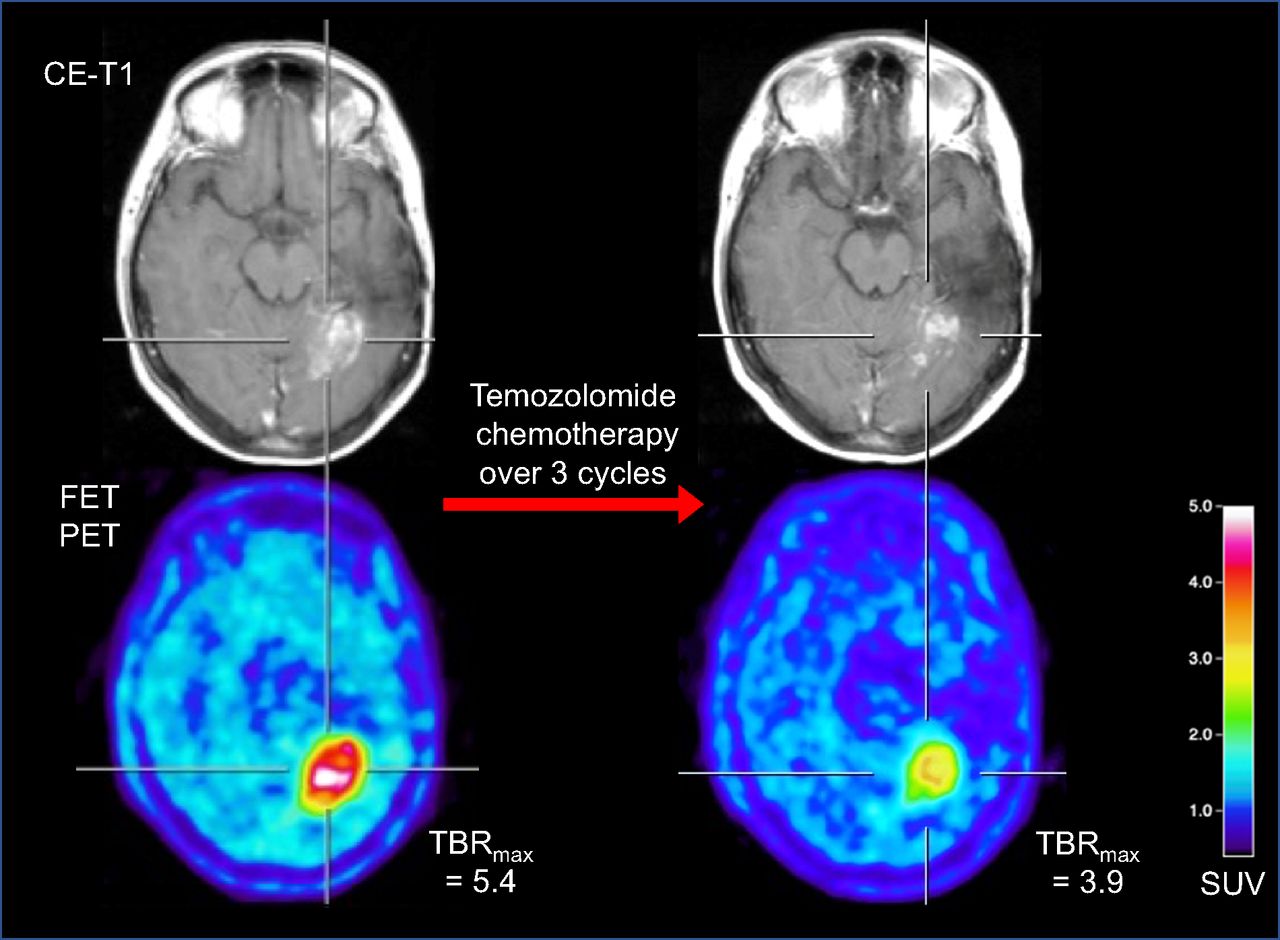
A 45-y-old woman with IDH–wild-type glioblastoma who underwent partial resection and radiotherapy with temozolomide plus lomustine chemotherapy as first-line treatment. Twenty-two months later, contrast-enhanced MRI and 18F-FET PET were consistent with tumor progression (left). For treatment, temozolomide chemotherapy was initiated. After 3 cycles, clear decrease in maximum tumor-to-brain ratios (−28%) was observed, whereas MRI showed only slight decrease in contrast enhancement (right). Metabolic response was associated with progression-free survival of 6 mo after temozolomide initiation. CE = contrast-enhanced; TBRmax = maximum tumor-to-brain ratio.
According to current guidelines (112), lomustine-based chemotherapy is recommended for patients with CNS WHO grade 3 or 4 gliomas at recurrence, especially in Europe, where bevacizumab is not approved in most countries. A recent study evaluated the new occurrence of lesions on follow-up 18F-FET PET scans showing pathologically increased metabolic activity remote from the tumor at baseline in mostly glioblastoma patients undergoing lomustine-based chemotherapy (113). In that study, the occurrence of these distant and metabolically active hot spots on 18F-FET PET proved to be the strongest predictor for nonresponse.
Furthermore, amino acid PET has been particularly evaluated in the recurrence setting to assess response to antiangiogenic therapy such as bevacizumab (114). In addition, 18F-FDOPA and 18F-FET PET have been found useful for identifying pseudoresponse (115–119). Moreover, 18F-FDOPA and 18F-FET Pet also seem helpful in predicting a favorable outcome in bevacizumab responders (118–120). A prospective study suggested that 18F-FET PET is useful for identifying metabolic responders to bevacizumab combined with lomustine in newly diagnosed IDH–wild-type glioblastoma patients early after treatment initiation (121). In that study, MRI changes according to the criteria of the Response Assessment in Neuro-Oncology Working Group (72) were not predictive of a favorable outcome, whereas 18F-FET PET parameters significantly predicted an overall survival of more than 9 mo.
Another anticancer therapy option with considerable efficacy in glioblastoma patients at recurrence is the multikinase inhibitor regorafenib, which is characterized by pronounced antiangiogenic activity (122). On the other hand, similar to glioma patients treated with standard chemoradiation using alkylating agents, equivocal MRI findings were also reported in glioma patients undergoing regorafenib treatment at recurrence (123–125). It has been suggested that amino acid PET using 18F-FET or 18F-FDOPA may help identify both treatment-related changes such as pseudoresponse or pseudoprogression and response to regorafenib (123–125).
The advent of immunotherapy using immune checkpoint inhibitors and targeted therapy has dramatically improved the treatment of extracranial cancer, especially in patients with skin, lung, or breast cancer. Moreover, recent trials have shown that patients with brain metastases may also benefit from these agents, especially when dual checkpoint blockade is applied (97,98). Similar to the response assessment in glioma patients, initial studies suggest that serial amino acid PET can potentially add valuable information to anatomic MRI for the assessment of immunotherapy effects. For example, a more recent study in 40 patients with more than 100 lung cancer or melanoma brain metastases treated with radiosurgery, checkpoint inhibitors, or combinations thereof evaluated whether 18F-FET PET may provide important diagnostic information on both response assessment and diagnosis of pseudoprogression (100). In that study, metabolic responders had significantly longer progression-free survival.
In addition to immune checkpoint blockade, targeted therapy using small molecules has demonstrated activity against brain metastases (126–128). The presence of predictive genetic alterations such as mutation of epidermal growth factor receptor, translocation of anaplastic lymphoma kinase or c-ROS oncogene 1, overexpression of human epidermal growth factor receptor 2, or mutation of BRAF V600E is considered an essential prerequisite for a response to targeted therapy options (129). Monitoring of metabolic activity reduction in patients with brain metastasis secondary to non–small cell lung cancer or melanoma treated with targeted therapies such as inhibitors of BRAF kinase or epidermal growth factor receptor as a sign of response appeared feasible using 18F-FET PET, whereas findings on anatomic MRI remained unchanged (10,130).
SUMMARY AND OUTLOOK
The current literature provides strong evidence that amino acid PET is of considerable clinical value for the most critical diagnostic indications in neurooncology. PET using amino acid tracers offers a variety of insights for the assessment of brain tumors, with the potential to overcome the limitations of anatomic MRI. The diagnostic improvement probably facilitates meaningful decision making and justifies more widespread use of this diagnostic tool (9,131). Furthermore, the necessary PET infrastructure is widely available, and the production of radiolabeled amino acids is well established, with costs comparable to other tracers routinely used in clinical practice. Moreover, additional costs for amino acid PET can potentially be saved by the incurred costs of less reliable diagnostic imaging techniques (132–136).
Clinicians will find amino acid PET to be an especially robust and attractive approach for many indications, with the advantage of easy scan reading. Importantly, most studies using amino acid PET provide comparable results across different scanners, as is also a consequence of international and interdisciplinary efforts by major nuclear medicine and neurooncology societies regarding standardization of amino acid PET acquisition and evaluation in brain tumor imaging in adults and children (137,138).
Adding novel advanced MRI techniques (e.g., ultra-high-field 2-hydroxyglutarate spectroscopic MRI and chemical exchange saturation transfer imaging) to amino acid PET has the potential to provide a more profound evaluation of biologic characteristics in patients with glioblastoma or metastatic brain disease. The complementary information derived from these imaging techniques suggests differential biologic information warranting further evaluation (139).
A methodologic innovation that may significantly alleviate research in brain tumor patients is the increasing availability of hybrid PET/MRI scanners, which enable time-saving simultaneous acquisition of several PET and advanced MR parameters under the same physiologic or pathophysiologic conditions. In addition, hybrid PET/MRI provides practical advantages and is convenient for patients such as children and individuals with a poor clinical condition. On the other hand, initial research suggests that for frequently requested indications for amino acid PET in clinical routine, such as differentiating treatment-related changes from tumor relapse, there is no significant difference in diagnostic performance between simultaneous and sequential acquisitions of PET and MRI (140).
Footnotes
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) advantages and limitations of anatomic MRI for brain tumor diagnostics; (2) the added clinical value of amino acid PET in glioblastoma patients or in patients with brain metastases for differential diagnosis, delineation of tumor extent, diagnosis of treatment-related changes, and assessment of treatment response; and (3) the differences in the information obtained by anatomical MRI and amino acid PET.
Financial Disclosure: Drs. Galldiks and Lohmann received honoraria for lectures from Blue Earth Diagnostics, and Dr. Galldiks received honoraria for advisory board participation from Telix Pharmaceuticals. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through May 2026.
Published online Apr. 13, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.
- 6.
- 7.
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.
- 58.↵
- 59.
- 60.
- 61.
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.
- 91.
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.
- 104.
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.
- 117.
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.
- 125.↵
- 126.↵
- 127.
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.
- 134.
- 135.
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- Received for publication January 16, 2023.
- Revision received March 10, 2023.





{kind=link}
{kind=link}
{kind=link}