


Abstract
We tested the hypothesis that educational level influences regional cerebral blood flow (rCBF) in Alzheimer’s disease (AD) patients. Methods: The severity of AD was measured with the Cognitive Ability Screening Instrument (age and education adjusted). rCBF was assessed using 99mTc-hexamethylpropyleneamine oxime brain SPECT; differences in rCBF between groups with different educational levels were determined using statistical parametric mapping (SPM). Results: In matched low-education (≤6 y; n = 29) and high-education (>6 y; n = 29) groups, SPM revealed 2 statistically significant clusters of voxels with higher rCBF in the high-education group: one in the left lateral inferior, middle, and superior temporal gyrus; another in the left medial temporal area to the left inferior frontal gyrus. Conclusion: We provide biologic evidence that education may lead to relatively higher rCBF in specific areas in AD patients, which may explain the effects of education on clinical manifestations of AD.
Alzheimer’s disease (AD) is a rapidly growing major public health problem in our aging society. Many studies from different cultural settings have shown a higher prevalence of dementia in poorly educated individuals (1). Because of its profound social, biologic, and medical implications, whether education could provide “neuroprotection” to retard the clinical manifestations of AD has become an important and fascinating topic (2). On the other hand, diagnosis of AD by functional brain imaging might be also influenced by education because of its possible effects on regional cerebral blood flow (rCBF) (3). Therefore, we used 99mTc-hexamethylpropyleneamine oxime (99mTc-HMPAO) SPECT to measure the basal rCBF to study the brain functional difference between AD patients with high- and low- educational levels.
MATERIALS AND METHODS
Setting and Clinical Diagnosis
The study was conducted in the special behavioral neurology referral clinic of a 1,000-bed national university medical center. The clinic evaluates and treats patients with AD, Parkinson’s disease, and various higher cortical dysfunctions after brain damage. One of us made a diagnosis of AD according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) (4). All patients had brain CT or MRI, with scan interpretations of either a normal or an aging brain. We recorded the number of formal years of education of the patients, reported by the patients themselves and confirmed by their families. Those with ≤6 y of education were classified as the low-education (LE) group, and those with >6 y were classified as the high-education (HE) group.
Neuropsychologic Test
The Cognitive Ability Screening Instrument (CASI) (5) was administered to all patients by a well-trained psychologist. The CASI is a cross-culturally validated neuropsychologic test that consists of 9 items: long-term memory, short-term memory, attention, concentration or mental manipulation, orientation, visual construction, abstraction and judgment, list-generation fluency, and language. The norms for the CASI were obtained from a large-scale population stratified to 3 educational levels (<6, 6–8, and ≥9 y of education), and 3 age levels (<69, 70–79, and >80 y) (6). For comparison purposes, CASI performance scores were converted to z scores—that is, (original score -mean)/SD, where the mean and SD were obtained from the listed norms. This transformation removes variation attributable to the level of education and age on cognitive changes. As a screening tool for dementia, the sensitivity and specificity of the CASI were slightly higher than those of the Mini-Mental State Examination (MMSE) (7). CASI scores and pathologic findings of AD are strongly associated (8); therefore, it is reasonable to use CASI to determine AD severity.
SPECT and Image Reconstruction
All patients received 99mTc-HMPAO brain SPECT after giving informed consent. Each patient was injected intravenously with 740 MBq of 99mTc-HMPAO (Ceretec; Amersham) in a quiet room about 10 min after placement of an intravenous line. Imaging was initiated about 20 min later. Patients were examined in supine position; a head holder was used to avoid motion artifacts. We used a SPECT system with a 3-head rotating γ-camera (Multispect3; Siemens) equipped with ultrahigh-resolution fanbeam collimators, which yields an image resolution of approximately 8.5-mm full width at half maximum (FWHM). The SPECT data were acquired over a circular 360° rotation, 120 steps, 30 s per step, in a 128 × 128 × 16 matrix. Reconstruction was performed by filtered backprojection using a Butterworth filter (cutoff frequency, 0.4 Nyquist; power factor, 7) with an attenuation correction. The transverse slices then were reoriented parallel to the canthomeatal line.
Statistical Image Analysis
Using statistical parametric mapping (SPM99; Wellcome Department of Cognitive Neurology, Institute of Neurology, University College London, London, U.K.) (9), we compared the SPECT images of the 2 groups of AD patients. Each image was first spatially normalized into a Talairach and Tournoux–based (10) standard SPECT template provided in SPM99. Smoothing of the images was then performed with a 14-mm FWHM gaussian filter. Proportional scaling was used for the global cerebral blood flow, and the gray matter threshold was set at 0.8. Statistical comparisons between the 2 groups were performed on a voxel-by-voxel basis using t statistics to constitute an SPM of the t-statistic SPM{t}. The data were subsequently transformed to the unit of normal distribution SPM{Z} map. In considering the hypothesis of educational effects on neocortical association cortex, the voxel height threshold was set at P = 0.01 and an extent size threshold was set at P = 0.05, without correction for multiple comparison.
RESULTS
Table 1 summarizes the demographic and clinical characteristics of the groups. Although the HE group had higher original CASI scores than did the LE group, no difference existed after the adjustment for age and education (i.e., z score of CASI). (The subjects were selected to equate the mean z score of CASI.) SPM comparisons of 99mTc-HMPAO brain SPECT of the 2 matched groups identified 2 clusters of voxels with relatively higher rCBF in the HE patients than in the LE patients (Table 2). One cluster was in the left lateral inferior, middle, and superior temporal gyri (Brodmann areas [BA], 20, 21, and 22) and the other was in the left medial temporal area (hippocampus, parahippocampal gyrus; BA 28) to the left inferior frontal gyrus. A glass brain SPM map is shown in Figure 1. No significant rCBF reductions were evident in the HE subjects when compared with the LE subjects.
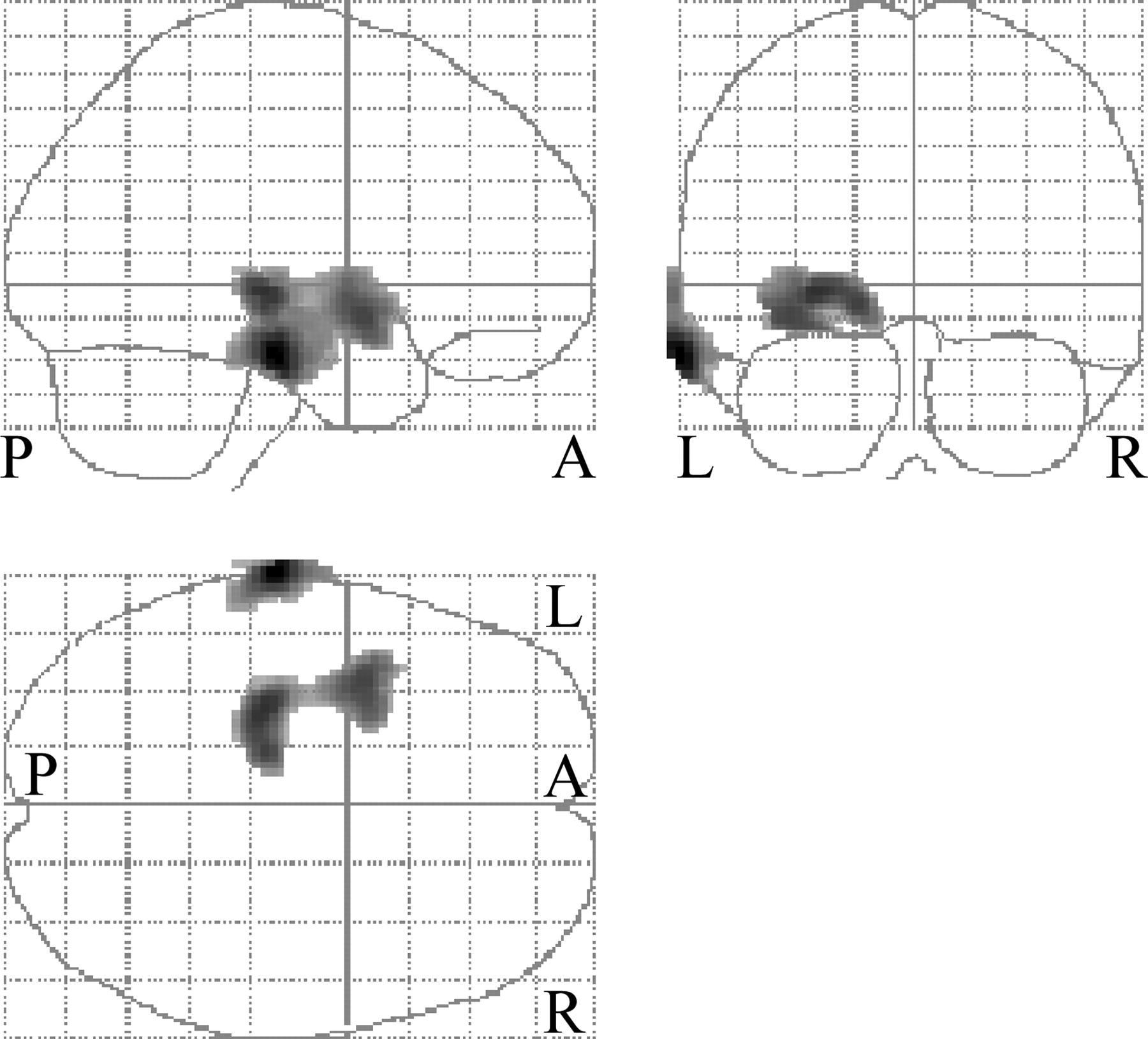
Three orthogonal projects of the statistical parametric map from SPM analysis for comparisons between LE and HE groups of AD patients. Two clusters with significantly relatively higher rCBF in HE group can be seen. Darker shading denotes a greater rCBF difference. P = posterior; A = anterior.
Demographic and Clinical Characteristics of 2 Groups with Different Levels of Education
Brain Regions with Significantly Reduced Perfusion in AD Patients with LE Level vs. HE Level
DISCUSSION
Our study showed that for the 2 matched groups of AD patients, the HE patients had relatively higher basal rCBF in some specific areas than did the LE patients. These findings suggest that education may influence rCBF in AD patients and provide a clue to understanding the effect of education on the incidence of AD. A brain reserve or neuroprotection hypothesis has been proposed (3) to explain the inverse association between educational level and the onset age and incidence of dementia. The hypothesis states that education can provide a reserve that must be depleted to a certain threshold before dementia clinically manifests. This reserve protects against the emergence of the clinical features of AD and produces a consequent reduction in the prevalence of AD. There is strong evidence that the biologic basis of cognitive deficit in AD is a loss of synapses (11), and education might provide a brain reserve by increasing the synaptic density in the association neocortex (12). Moreover, animal studies have shown that the weight of the adult brain and the number of its neuronal processes are related to environmental stimulation in early life (13). Because the tight relationship between neuronal functioning and local brain perfusion is intact in AD, rCBF may reflect synaptic activity after the local loss of neurons (14). Our findings suggest that, although education is unlikely to influence the progression of AD pathology of neural degeneration, education and related activities and stimulations may increase the synaptic density in a patient’s brain—as demonstrated in higher rCBF on neuroimaging—thereby deferring the emergence of the clinical features of AD.
The topography of the 2 clusters showing higher rCBF in the HE group is interesting. One is in the left lateral inferior, middle, and superior temporal gyri (BA 20, 21, and 22); the other is in the left medial temporal area (hippocampus, parahippocampal gyrus; BA 28) to the left inferior frontal gyrus. Functional imaging studies have shown that semantic memory, which refers to facts and general knowledge, is associated primarily with the left lateral temporal areas, left inferior frontal cortex, and left medial temporal area (15–17). Of these 3 areas, the left lateral temporal area is especially closely related to clinical manifestation in semantic memory in patients with dementia (18). In addition, medial temporal lobes—the hippocampus in particular—are highly related to episodic and autobiographic memory, with left lateral for verbal materials and bilateral for nonverbal materials (19). Finally, the left inferior frontal gyrus, left middle temporal gyrus (BA 21 and 22), a region of the left lateral inferior temporal gyrus, superior temporal gyrus (BA 22) are involved in human reasoning (20).
More education makes more environmental stimuli relevant, and this enhanced environment and brain relationship is based on increased cortical activation and cortical synapses (21) in some specific areas, as suggested in this study. This increased synaptic activation, as reflected in higher rCBF, is the basis of better perception, memorization, and reasoning ability that results in the cognitive reserve effect and increased resilience to the advancing AD pathology.
Our results, however, are contrary to the findings of Stern et al. (3). By using the 133Xe inhalation technique to quantify rCBF, they found an inverse relation between education and cerebral perfusion in AD patients. Their patients were matched for dementia severity by the MMSE, which was adjusted for age, but not for education. In the present study, the severity of AD was assessed by the CASI adjusted for both age and education. We believe that the adjustment for education, in addition to that for age, is necessary for the mental tests because subjects with higher education may in fact be worse in AD severity (neural degeneration) given equal cognitive performance compared with those with lower education (22). If no adjustment was made for education, the highly educated patients might have revealed more perfusion deficits in areas such as the parietotemporal cortex, as shown by Stern et al. (3). We believe that when cerebral perfusion images are interpreted, the educational level of the patients must be taken into consideration.
CONCLUSION
We showed that AD patients with a HE level had relatively higher rCBF in some specific areas than those with a LE level. These findings suggest that education may increase the cortical synaptic density and explain the association between education and the incidence of AD. This result indicates the necessity of considering the educational level when interpreting functional brain images.
Acknowledgments
This study was partially supported by grant NSC 91-2623-7-006-001-NU from the National Science Council, Taiwan.
Footnotes
Received Mar. 16, 2004; revision accepted May 27, 2004.
For correspondence contact: Ming-Chyi Pai, MD, PhD, Division of Behavioral Neurology, Department of Neurology, Medical College, National Cheng Kung University, 138 Sheng Li Rd., Tainan 704, Taiwan.
E-mail: pair{at}mail.ncku.edu.tw





{kind=link}