


Abstract
This study was undertaken to identify the clinical value of incidentally detected lesions (IDLs) in the gastrointestinal tract (GIT) with 18F-FDG PET/CT. Methods: The reported database of 3,281 patients who underwent partial-body 18F-FDG PET/CT scans from April 2001 to September 2003 was reviewed. Patients with incidental 18F-FDG accumulations in the GIT that were associated with concomitant abnormal soft-tissue density or wall thickening on the native CT were evaluated. Incidental PET/CT findings were correlated with endoscopic and histopathologic results. Results: According to our selection criteria, 98 (3%) of the 3,281 patients had an IDL of the GIT on 18F-FDG PET/CT. Correlative endoscopic findings were available in 69 (70%) of 98 patients. Of these, 13 patients (19%) were harboring newly occurring cancers of the GIT in addition to preexisting aerodigestive tract tumors (n = 12) and malignant melanoma (n = 1). Twenty-nine (42%) patients were identified with precancerous lesions, such as advanced colonic adenomas (n = 27), Barrett’s esophagus (n = 1), and intestinal metaplasia of the gastric mucosa (n = 1). Inflammatory and other benign GIT lesions were detected in 12 (17%) and 6 (8%) patients, respectively. In 9 (13%) patients, PET/CT was false-positive, showing normal findings in subsequent endoscopic examinations. In 20 (28%) of 69 patients, PET/CT findings had a relevant impact on the clinical management. Twenty-nine (30%) of the 98 patients were not subject to a further endoscopic examination because of the extent and nature of the primary tumor (n = 17), loss to follow-up (n = 7), death shortly after PET (n = 3), and patient unwillingness (n = 2). Conclusion: Although IDLs of the GIT on 18F-FDG PET/CT scans are found only in about 3% of cases, they are associated with a substantial risk of an underlying cancerous or precancerous lesion. Early identification of these occult lesions may have a major impact on the patients’ management and outcome.
Use of the glucose analog 18F-FDG with PET has an increasing role in evaluating malignant and inflammatory disorders of the gastrointestinal tract (GIT) (1–4). The high lesion-to-background contrast and data acquisition from head to pelvic floor on PET represent critical advantages over CT and MRI, where the contrast between pathologic and normal structures is frequently inferior. Furthermore, these imaging methods are used primarily to evaluate a given region rather than extended areas of the body. Thus, additional findings outside the imaging field can be missed on CT and MRI. With the successful introduction of integrated PET/CT systems, the concomitantly acquired anatomic data offer an anatomic reference frame to 18F-FDG PET. This permits a direct correlation of the 18F-FDG-accumulating lesions with morphologic changes and helps to identify foci of physiologic 18F-FDG uptake (5,6). Incidental 18F-FDG accumulation may reflect additional pathology unrelated to the primary one for which the patient was originally referred for PET (7). It has been previously observed that both thyroid and colonic incidental 18F-FDG findings are associated with a considerable risk of an underlying neoplasia (8–10). Colonic adenomas with their well-known potential for malignant transformation and colorectal carcinoma may progress insidiously in an asymptomatic patient (11). Similarly, inflammatory bowel disorders in an early stage may present without clinical manifestations (12–14). This suggests that early identification of such occult lesions may have an impact on patient management and outcome. The purpose of this investigation was to evaluate incidental 18F-FDG accumulations in the GIT found in a patient population that was subject to PET/CT for other diagnostic purposes.
Additionally, we investigated whether these incidental 18F-FDG PET/CT findings had a relevant impact on the clinical management of these patients.
MATERIALS AND METHODS
Patients
From April 2001 to September 2003, the reported database of 3,281 patients who underwent partial-body 18F-FDG PET/CT scans was reviewed. Among this population, 2,836 (86%) patients were examined because of various oncologic diseases: lung cancer, 880 patients; gastrointestinal cancer, 542; lymphoma, 349; ear, nose, and throat cancer, 314; urogenital cancer, 229; breast cancer, 187; gynecologic cancer, 137; malignant melanoma, 130; and soft-tissue or bone cancers, 68. In 445 patients, 18F-FDG PET/CT was performed because of a suspicion of inflammatory or infectious disease.
Patients with incidental 18F-FDG accumulation in the GIT, which was associated with abnormal soft-tissue density or wall thickening on the concomitantly acquired CT, were included in the study. An 18F-FDG accumulation in the GIT was termed incidental only in patients who were referred for PET/CT with the diagnosis of a non-GIT disorder or in patients with a known GIT disease in whom 18F-FDG accumulation occurred in areas not consistent with the preexisting pathology.
One hundred five of 3,281 patients (64 men, 41 women; age range, 46–85 y; mean age, 62 y) showed incidental 18F-FDG PET/CT findings in the GIT. From these 105 eligible patients, 7 patients were excluded from further analysis because ensuing histologic examination revealed gastrointestinal metastases of preexisting gynecologic cancers (n = 5) and malignant melanoma (n = 2) Thus, 98 patients were included in our study.
PET/CT Protocol
Imaging was performed using an integrated PET/CT device (DISCOVERY LS; General Electric Medical Systems) combining the ability to acquire CT images and PET data of the same patient in 1 session. A General Electric Advance NXi PET scanner and a multislice helical CT scanner (LightSpeed Plus) were integrated in this dedicated system. The axes of both systems were mechanically aligned to coincide perfectly. Typically, 6 or 7 bed positions are obtained covering 867–1,011.5 mm of the body. This gave adequate coverage from head to pelvic floor in all patients examined. The arms of the patients were elevated above the abdomen to reduce beam-hardening artifacts at the level of the liver. As a standard procedure, all patients received oral x-ray contrast agent (1,000 mL of a 1.5% diluted barium sulfate suspension (Micropaque Scanner; Guerbet) 45 min before data acquisition. No bowel preparation regimen was applied for any patient in our series.
CT data were acquired first, with the following parameters: tube rotation time, 0.5 s per revolution; 140 kV; 80 mA; 22.5 mm per rotation; slice pitch, 6; and acquisition time, 22.5 s for a scan length of 867 mm. Subsequently, PET emission data were acquired in 2-dimensional mode. Emission counts were collected during 4 min per table position, and adjacent fields of view shared 1 overlapping slice. Matched CT and PET image were reconstructed with a field of view of 500 mm and a 4.25-mm slice thickness. An iterative reconstruction and CT-based attenuation correction were used for the PET images (15). For viewing the images, the PET and CT datasets were transferred to an independent, personal computer-based computer workstation by DICOM (Digital Imaging and Communications in Medicine) transfer. All viewing of coregistered images was performed with dedicated software (eNTEGRA; General Electric).
To increase image quality and to suppress myocardial glucose utilization, patients were asked to fast for at least 4 h before the PET/CT examination. At the outset, patients received an intravenous injection of 300–400 MBq of 18F-FDG and rested for 50 min for the uptake of 18F-FDG to occur. 18F-FDG was produced in house by using a 17.8-MeV cyclotron (PET Trace 2000; General Electric) and an automated FDG synthesis module (PET Tracer Synthesizer; General Electric Nuclear Interface). Before PET, patients were encouraged to void to minimize activity in the bladder due to renal excretion of 18F-FDG.
Evaluation of PET/CT Images
Pathologic 18F-FDG accumulation was identified either by tracer uptake that exceeded that of the normal hepatic parenchyma but was clearly inferior to that of the cerebral cortex (moderate uptake) or was comparable or more intense than that of the cerebral cortex (strong uptake). All PET/CT examinations were interpreted by at least 1 board-certified nuclear physician and 1 board-certified radiologist. Two board-certified nuclear physicians reevaluated the selected cases in consensus to ascertain the localization, the degree of 18F-FDG uptake, as well as the pattern (focal, segmental, or diffuse) of the incidental 18F-FDG accumulation in the GIT. Proximal large bowel lesions were defined as those located proximal to the sigmoid colon (16). In the present investigation, we decided to include only patients with incidental 18F-FDG accumulation that correlates with abnormal soft-tissue density or wall thickening on the native CT.
This approach was chosen since nonspecific, primarily nonfocal, 18F-FDG accumulation, which may occur incidentally in a considerable number of patients (17), has been shown to carry an unacceptable high rate of false-positive results or irrelevant pathologic value in most instances (e.g., low-grade colonic inflammation, hypertrophied lymphoid follicles of the ascending colon, and reflux esophagitis). Eligibility criteria for mural thickening included an 8-mm cutoff for the normal rectal wall thickness and 5 mm for the rest of the GIT according to Cai et al. (18).
Standard of Reference
The final diagnosis of incidental 18F-FDG PET/CT findings was made on the basis of correlative endoscopic examinations in 69 patients. In 60 of these patients, additional histology of the biopsied lesion was available. In 9 patients of the 69 patients with incidental 18F-FDG accumulations in the GIT, no biopsy was performed because of normal findings on endoscopy.
Statistical Analysis
We performed statistical data analysis using the Fisher exact test to summarize our findings. The primary aim of this statistical analysis was to determine whether there is a special 18F-FDG uptake pattern that may predict the existence of an underlying relevant pathologic finding. For that purpose, we decided to compare the outcome of focally increased 18F-FDG uptake (group I) with that of segmentally and diffusely increased 18F-FDG uptake patterns (group II). P < 0.05 was considered significant.
RESULTS
Of the 3,281 patients evaluated, 98 displayed incidentally detected lesions (IDLs) of the GIT, representing a prevalence of 3%. Correlative histopathologic or endoscopic examinations were available in 69 (70%) of 98 patients. Incidental 18F-FDG PET/CT findings in these 69 patients were distributed as follows: cancerous lesions, 13 patients; precancerous lesions, 29; inflammatory and miscellaneous lesions, 18; 9 patients displayed discordant findings with subsequent endoscopic examinations. In 29 (30%) patients, IDL was not verified because of advanced primary tumor stage (n = 17), loss to follow-up (n = 7), death shortly after PET/CT (n = 3), and patient unwillingness (n = 2). Interestingly, 90% of the cancerous and precancerous findings and 50% of the benign findings (inflammatory and miscellaneous lesions) were characterized by focally increased 18F-FDG uptake (P = 0.001) (Table 1).
Characterization of 18F-FDG Uptake Pattern of Incidentally Detected Lesions in GIT
Cancerous Lesions
Among the 69 patients with endoscopic evaluation, subsequent histopathologic examinations revealed that 13 (19%) patients were harboring synchronous (n = 10) and metachronous (n = 3) carcinomas of the GIT. These carcinomas were detected in the esophagus (n = 4), the proximal colon (n = 2; in the transverse colon in both patients), and the distal colon (n = 7; in the sigmoid colon in 4 patients and in the rectum in 3 patients). Synchronous carcinoma was defined as a tumor that occurred within 6 mo of the first primary carcinoma, whereas metachronous carcinoma was defined by its occurrence beyond this time period. The degree of 18F-FDG uptake in all of these lesions was comparable to that of the cerebral cortex (strong uptake). Focal 18F-FDG uptake was observed in 11 patients, whereas a segmental pattern was noted in 2 patients. All lesions showed a frank soft-tissue density or remarkable wall thickening on CT. These newly occurring secondary tumors were associated with or preceded by the existence of head and neck (n = 5), lung (n = 3), pancreatic (n = 2), stomach (n = 1), and colorectal (n = 1) cancers, all tumors of the aerodigestive tract. One patient had an esophageal cancer that was synchronous with a preexisting malignant melanoma. Altogether, 12 of 13 newly occurring cancerous lesions in the GIT occurred in patients with primary tumors of the aerodigestive tract.
Two patients with moderately differentiated adenocarcinoma of the rectosigmoid colon revealed histopathologic evidence of highly dysplastic tubullovillous adenomas within their resected tumor materials (Fig. 1). Based on our PET/CT findings, 8 of 13 (62%) patients with colorectal (n = 6) and esophageal (n = 2) cancers could be scheduled to undergo curative surgical resection. The remaining 5 patients obtained palliative chemotherapy (n = 4) and combined radiochemotherapy (n = 1) because of their advanced tumor burden.
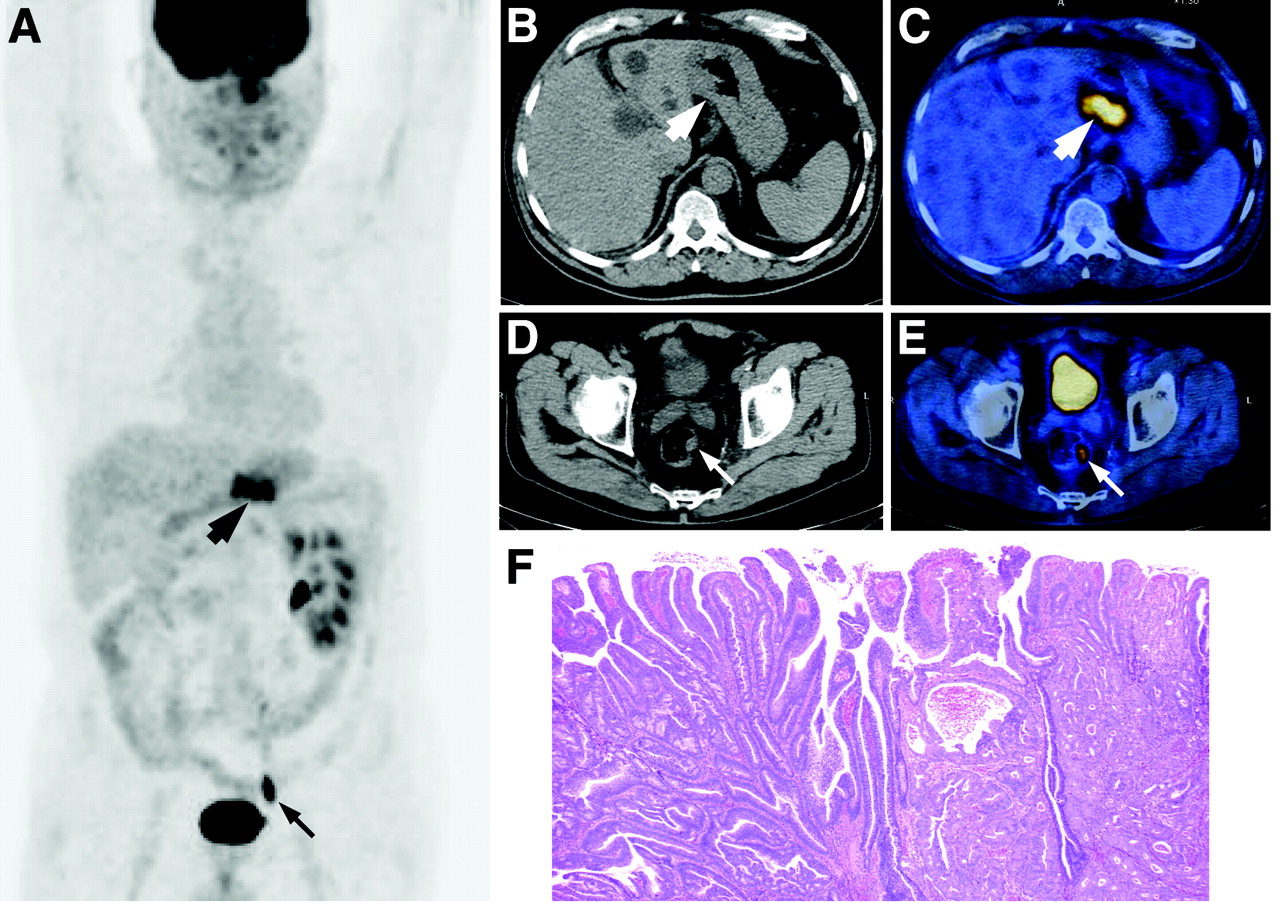
Maximum-intensity-projection PET (A), transaxial CT (B and D), and transaxial PET/CT (C and E) images from 68-y-old man with known gastric carcinoma and incidentally detected sigmoid carcinoma show pathologic 18F-FDG accumulation in stomach (thick arrows) and sigmoid colon (thin arrows) with correlative mural thickening. (F) Coronally sectioned specimen shows moderately differentiated adenocarcinoma (right half) in highly dysplastic tubulovillous adenoma (left half) (hematoxylin-eosin stain, ×20).
Precancerous Lesions
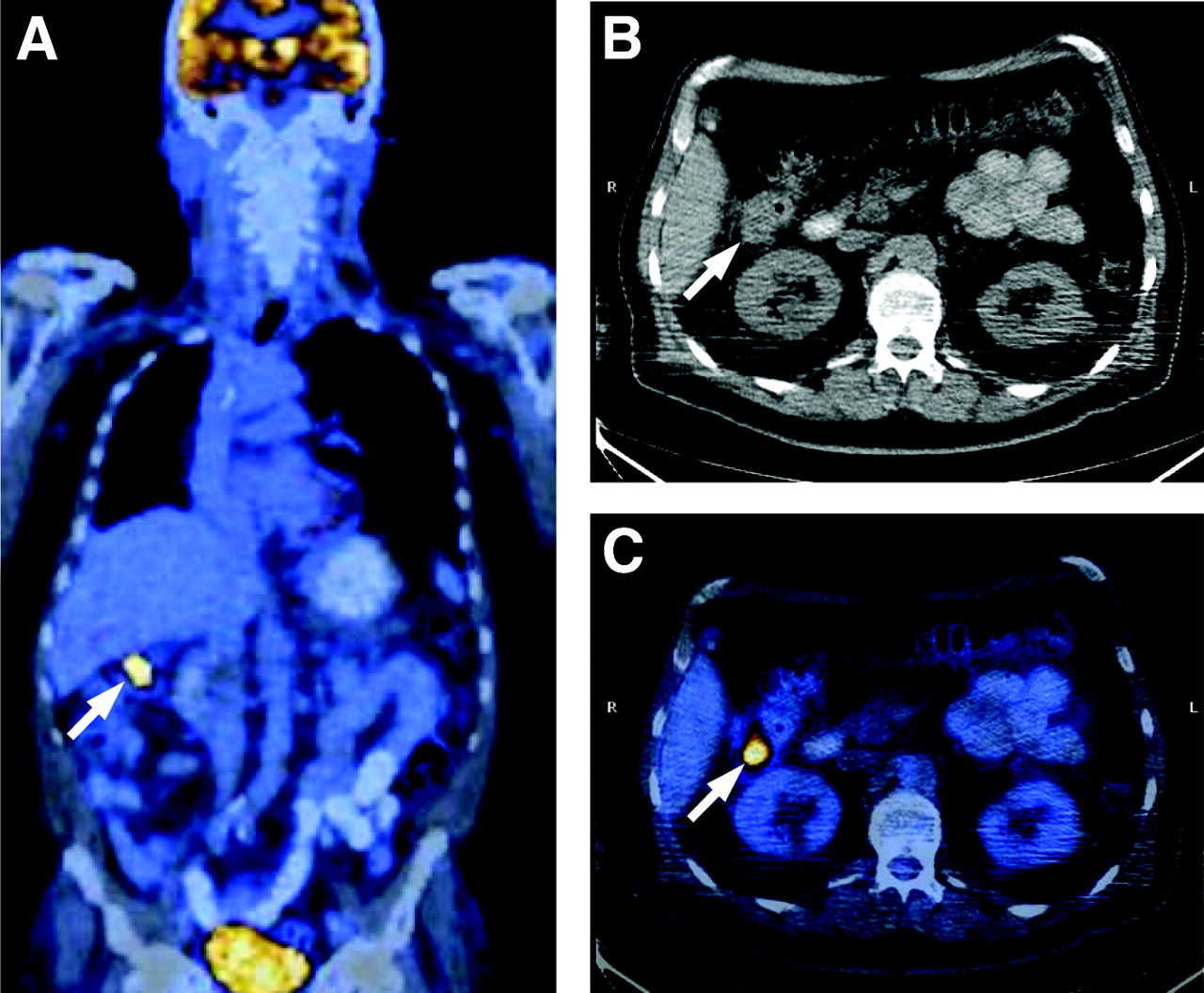
In 27 of 69 (39%) patients, ensuing endoscopic and histopathologic examinations confirmed the existence of colorectal adenomas (tubulovillous, n = 15; villous, n = 3; and tubular, n = 9) that correlated with incidental PET/CT findings in the ascending colon (n = 5), descending colon (n = 2), sigmoid colon (n = 15), and rectum (n = 5). These adenomas, which ranged in size from 1.2 to 4 cm, were characterized by focal moderate uptake (n = 6) and strong uptake (n = 21), respectively (Fig. 2). High-grade dysplasia was observed in 7 adenomas, whereas the other 20 were characterized by low-grade dysplasia.
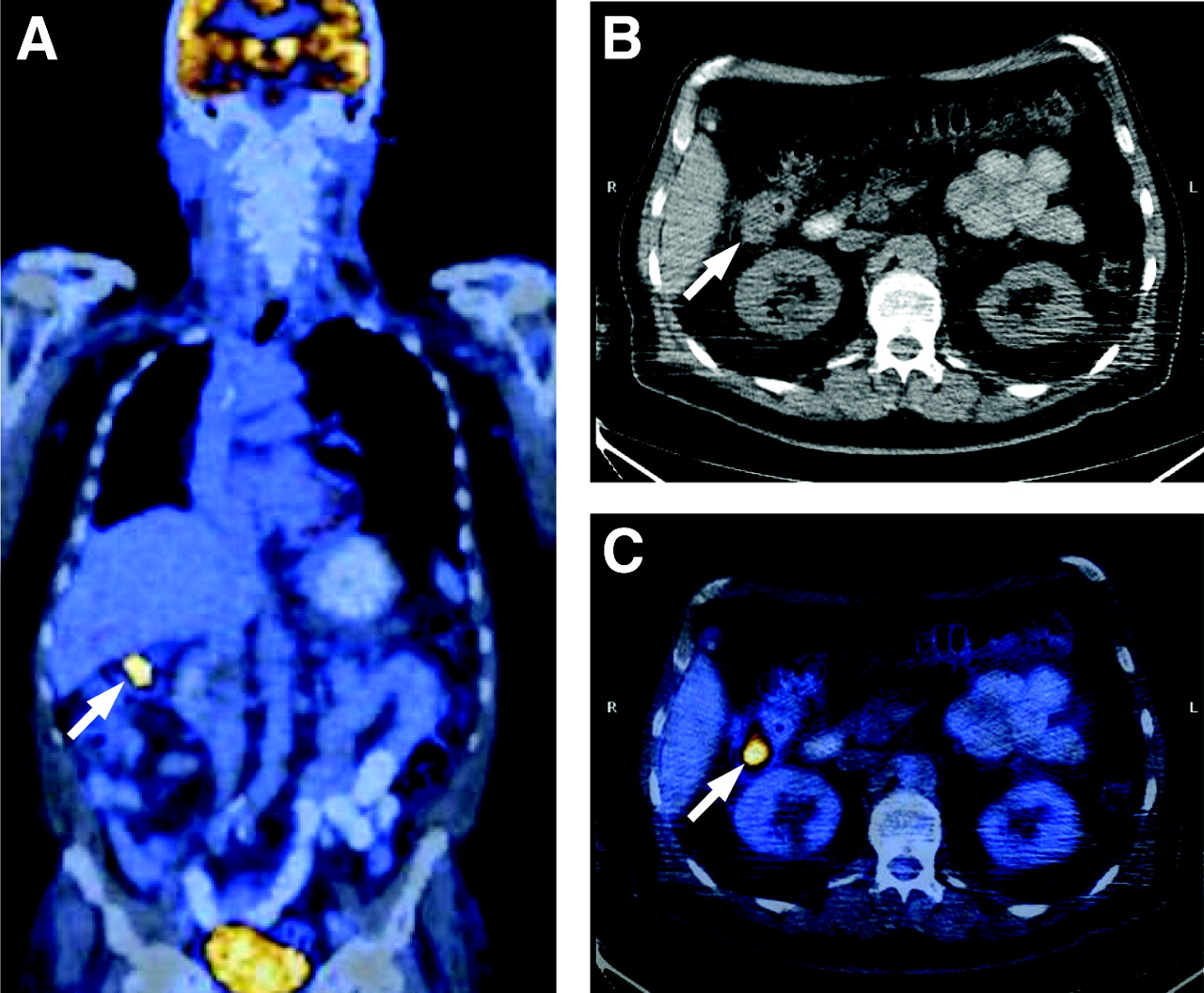
Coronal PET/CT (A), transaxial CT (B), and transaxial PET/CT (C) images from 69-y-old man show pathologic 18F-FDG accumulation with correlative soft-tissue density (arrows) in right colonic flexure. Endoscopic and histopathologic examinations revealed advanced colonic adenoma.
Seven adenomas were located in the proximal part of the colon and 20 were found distally (Table 2). According to the advanced adenoma concept (19), all 27 lesions met the criteria of a precancerous colorectal adenomatous polyp. Nineteen (70%) of these 27 precancerous adenomas occurred in patients who were initially identified with primary aerodigestive tract tumors. These primary tumors were distributed as follows: lung cancer (n = 10), head and neck cancer (n = 7), and colorectal cancer (n = 2).
Characterization of Incidentally Detected Advanced Adenomas Referring to Endoscopy and 18F-FDG PET/CT
In another 2 patients with segmental strong 18F-FDG uptake in the esophagus and the stomach, subsequent endoscopic and histopathologic examinations confirmed the existence of Barrett’s esophagus and intestinal metaplasia of the gastric mucosa, respectively (Fig. 3).
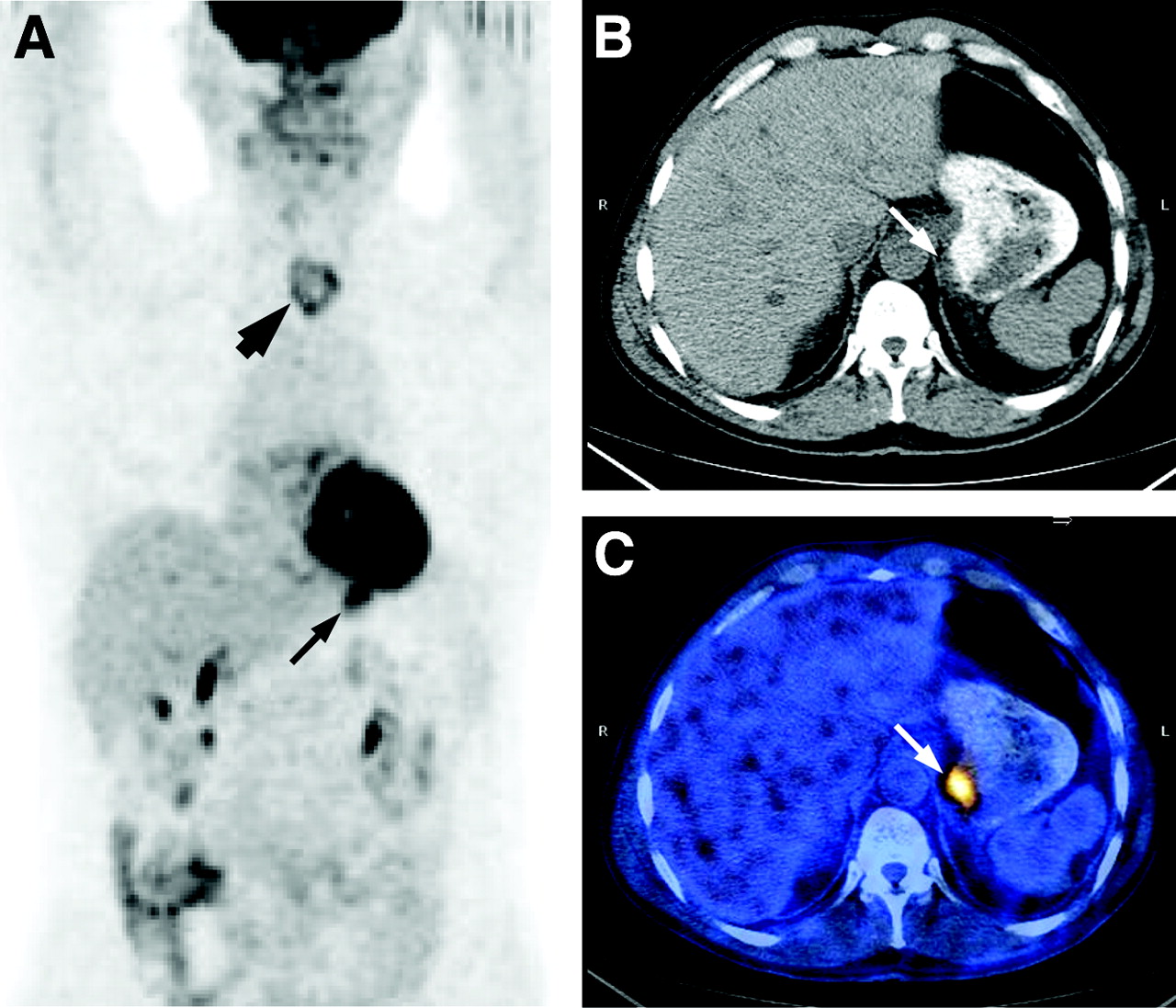
Coronal PET (A), transaxial CT (B), and transaxial PET/CT (C) images from 52-y-old woman with locoregional recurrence of epiglottic carcinoma (thick arrow) and pathologic 18F-FDG accumulation with correlative wall thickening of stomach (thin arrows) consistent with intestinal metaplasia of gastric mucosa.
Inflammatory Lesions
A total of 12 inflammatory lesions were detected according to histopathology findings. Four patients showed diffusely increased strong colonic 18F-FDG uptake. In 3 of them, the diagnosis of active colitis was made, which was necrotizing in 1 patient. In the fourth patient, who had a history of inflammatory bowel disease, correlative histopathologic findings confirmed reactivation of ulcerative colitis. Although acute exacerbation of inactive colitis can be expected at any time point during the disease course, in this patient, however, the colonic PET/CT finding was exceptionally considered as incidental since no specific clinical symptoms (e.g., mucous or bloody discharge, tenesmus, or characteristic abdominal pain) could be identified at the time of the PET/CT.
Three patients, with recent intake of ciprofloxacin, demonstrated segmentally increased strong 18F-FDG uptake. In 1 of these 3 patients, Clostridium difficile was cultivated in the stool probes; hence, the diagnosis of a pseudomembranous colitis was made (Fig. 4). In 2 patients, acute diverticulitis of the sigmoid colon with focally increased strong 18F-FDG uptake was diagnosed on PET/CT and colonoscopy findings. On the corresponding CT images, typical CT features in the form of wall thickening and inflammatory changes in the adjacent pericolic fat were present.
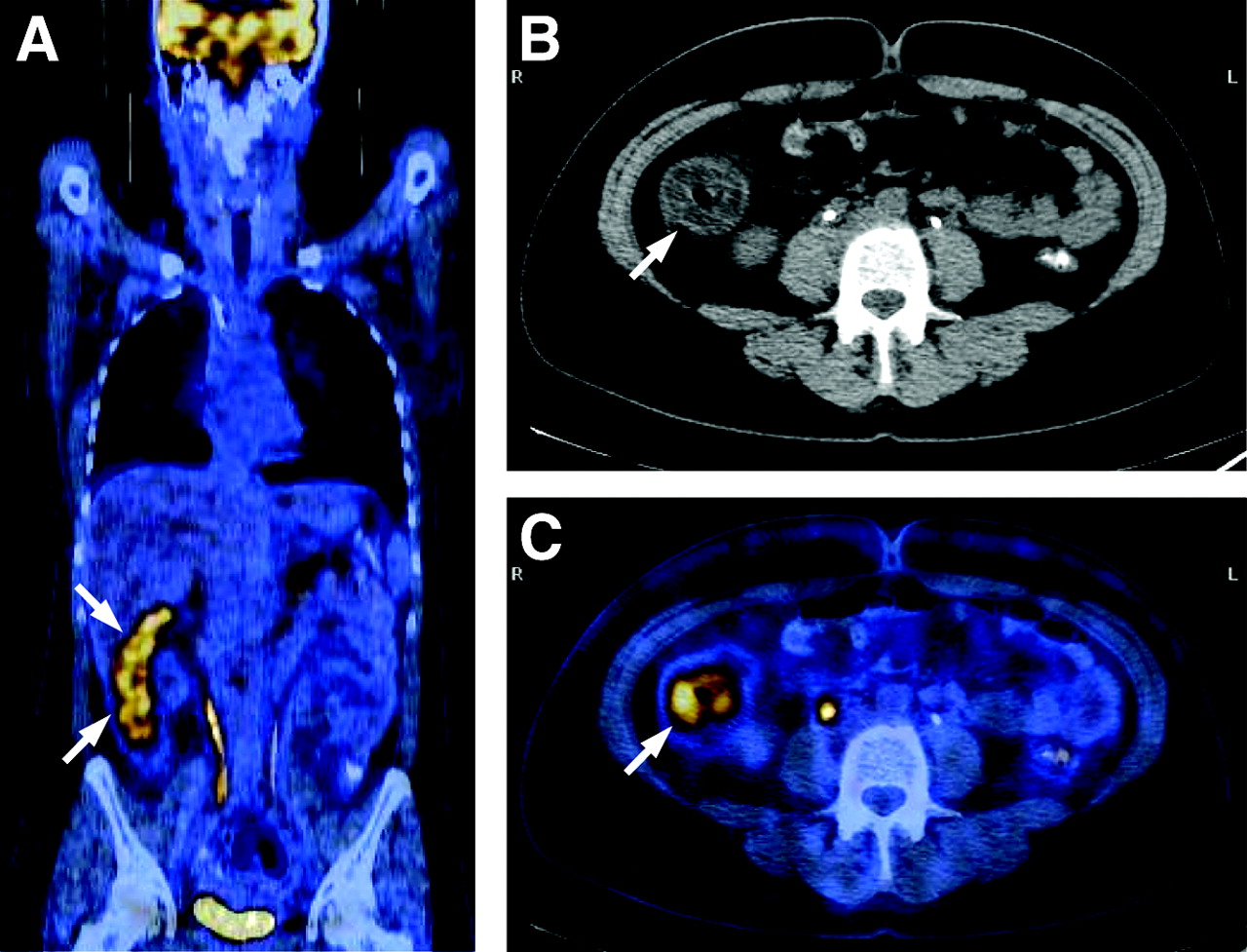
Coronal PET/CT (A), transaxial CT (B), and transaxial PET/CT (C) images from 42-y-old woman after recent intake of ciprofloxacin show segmental 18F-FDG accumulation in ascending colon with correlative circumscribed mural thickening (arrows). Pseudomembranous colitis was confirmed after cultivating Clostridium difficile in stool probes.
In the remaining 3 patients, endoscopy revealed an anal fissure, a hemorrhoidal lesion, and an anal ulcer with focally increased (n = 2) and segmentally increased (n = 1) strong 18F-FDG uptake. Ensuing histopathologic examination displayed remarkable inflammatory changes in these 3 lesions.
Miscellaneous Lesions
Six patients were identified with miscellaneous 18F-FDG PET/CT incidental findings of the GIT. The distribution of these lesions that showed focally increased 18F-FDG uptake was as follows: Two patients were harboring hemorrhoids with no signs of infection or inflammation. One had moderate and the other strong 18F-FDG uptake. In another 3 patients with strong (n = 2) and moderate (n = 1) 18F-FDG uptake, the diagnosis of a hyperplastic mucosal polyp was confirmed. These 3 polyps were located in the ascending colon, sigmoid colon, and the anal canal, respectively. The remaining patient revealed focally increased moderate 18F-FDG uptake in the esophagus. Endoscopic and histopathologic examinations identified glycogen acanthosis of the esophageal epithelium.
Discordant Findings
In 9 (13%) patients, pathologic 18F-FDG accumulation that correlated with abnormal soft-tissue density on the native CT did not correlate with any pathologic findings on endoscopy. In these patients, no biopsy was performed. Additionally, 7 small-sized, low-grade adenomas (range, 0.3–1.0 cm) were incidentally detected by colonoscopy in 5 patients in whom PET/CT and endoscopy already detected adenomas in another localization. Five of them displayed tubular and 2 displayed tubulovillous histology. These small adenomas did not show any 18F-FDG accumulation, even after reviewing the PET/CT data retrospectively.
Impact on Management
Besides the 27 patients with advanced colonic adenomas, who were certainly protected from potential malignant progression by virtue of PET/CT-guided polypectomy, the detection of incidental 18F-FDG PET/CT findings had a relevant impact on the clinical management of another 20 patients that were distributed as follows: The early detection of carcinoma in 13 patients lead to a curative resection in 8 of them (6 patients with occult colorectal and 2 patients with esophageal carcinomas). In 5 patients, the extent of the known primary carcinoma did not justify a resection of the newly diagnosed secondary carcinoma. These patients were treated by palliative chemotherapy (n = 4) and combined radiochemotherapy (n = 1). Furthermore, 2 patients with Barrett’s esophagus and intestinal metaplasia of the gastric mucosa were considered for close surveillance. In the group with inflammatory lesions, the detection of Clostridium difficile in 1 patient led to an appropriate antibiotic treatment.
The 2 patients with acute diverticulitis were also treated successfully with antibiotics. Four patients with colitis received either conservative therapy management with follow-up colonoscopy (n = 3) or an immunosuppressive therapy regimen (n = 1). The anal fissure, the anal ulcer, and the hemorrhoids were treated surgically. Thus, overall, the GIT findings resulted in changes in the clinical management in 20 (28%) of 69 patients.
DISCUSSION
The ability of 18F-FDG PET to detect a wide range of GIT tumors depends on the fact that most of these neoplasias have a strongly increased uptake of 18F-FDG (1,2). However, 18F-FDG is not tumor specific and may also accumulate in some inflammatory and benign disorders of the GIT (3,4). Gastrointestinal malignancies may exist synchronously or metachronously with other carcinomas that may or may not originate from the GIT (20,21). In the present study, 13 (19%) of 69 patients with incidental 18F-FDG accumulation in the GIT were proven to harbor cancerous lesions. Interestingly, 12 of these 13 occult GIT tumors were identified in patients previously diagnosed with primary cancer of the aerodigestive tract (53% of the studied patients in our series), whereas the remaining patient had a preexisting malignant melanoma. This may imply that the pathogenesis of these multiple aerodigestive neoplasias was chronologically related by virtue of a common provocative factor(s).
In patients with multiple primary tumors, early detection of the second primary tumor has been claimed to improve the overall outcome (20). Based on our PET/CT findings, 8 of 13 (62%) patients with GIT cancers were eligible for curative surgical resection, whereas the primary tumor stage in the remaining 5 patients was such that they were only eligible for palliative chemotherapy (n = 4) and combined radiochemotherapy (n = 1).
In accordance with the developmental sequence from adenoma to carcinoma (22), 2 patients with newly diagnosed rectosigmoid cancers had histopathologic features consistent with moderately differentiated adenocarcinoma in a highly dysplastic tubulovillous adenoma (Fig. 1). Continuous efforts have been devoted to identify special adenoma characteristics that may predict outcome. According to the recent literature, there is unanimous agreement that, adenomas with a size > 1.0 cm, with tubulovillous or villous histology, or with high-grade dysplasia, invariably carry a high likelihood of malignant transformation (19). Based on these criteria, the detection of 27 advanced adenomas would have been missed, or at least postponed, if colonoscopy and excisional biopsy were not triggered by the incidental 18F-FDG PET/CT findings in our series.
Of note, dysplastic changes were observed in all of these incidentally detected adenomas (high grade, n = 7; low grade, n = 20). Using immunohistochemistry, 2 recent studies have shown that the proliferative rate of colonic adenomas correlates positively with the degree of dysplasia in a stepwise fashion (23,24). Interestingly, no statistically significant difference was observed between the proliferation index of colorectal carcinoma and highly dysplastic adenomas (24). Given the fact that most 18F-FDG-avid tumors are highly proliferating (25,26), it is obvious why 18F-FDG PET was capable of detecting these advanced adenomas.
The occurrence of 19 (70%) of 27 advanced adenomas among patients with aerodigestive tract tumors strengthens our observation about the propensity of a second primary GIT tumor in subjects with a known head and neck, lung, and gastrointestinal cancer.
Twenty (74%) of the successfully detected advanced adenomas in our series (n = 27) originated from or were distal to the sigmoid colon, which is also concordant with the literature (27). Detecting the 2 other precancerous lesions (Barrett’s esophagus and intestinal metaplasia of the gastric mucosa) has also had obvious prognostic significance (Fig. 3), as these lesions are well known to be able to transform to differentiated adenocarcinoma if left without interference (28,29).
In patients with suspected cancer, infectious or inflammatory conditions are a major source of false-positive results on 18F-FDG PET. However, correlation of the PET data with those obtained by CT or MRI may allow more precise differentiation between malignant and benign lesions. In the present study, 12 (17%) of 69 patients had incidental inflammatory or infectious findings of the GIT. Of note, 4 patients were harboring pathologies prone to peritonitis: necrotizing colitis (n = 1), pseudomembranous colitis (n = 1), and diverticultitis (n = 2). Given the known morbidity and mortality that is associated with these entities, potential complications may have been averted due to their early identification by PET/CT.
Few studies have discussed the role of 18F-FDG PET in the diagnosis of enterocolitis as well as necrotizing and pseudomembranous colitis. Despite the small number of patients in these reports, it has been concluded that PET may be a useful noninvasive tool in identifying active bowel inflammation, even in the face of nondiagnostic structural imaging modalities and colonoscopy (3,4,30).
Three hyperplastic colonic polyps, 2 anorectal hemorrhoids, and 1 glycogenic acanthosis of the esophagus without signs of infection were incidentally detected in 6 patients on 18F-FDG PET/CT. 18F-FDG accumulation can be related to the proliferative activity in both hyperplastic polyps and esophageal glycogenic acanthosis (31,32). However, no obvious reason other than the existence of minimal thrombotic changes can explain 18F-FDG accumulation in the 2 patients with uncomplicated hemorrhoids (33).
When the focal 18F-FDG uptake pattern was compared with the segmental and diffuse pattern in the whole GIT, 90% of the cancerous and precancerous findings and 50% of the benign findings (inflammatory and miscellaneous lesions) were characterized by focally increased 18F-FDG uptake (P = 0.001). This may suggest that focally increased 18F-FDG uptake seems to be predictive of relevant pathologic findings on colonoscopy—primarily precancerous or cancerous lesions.
Discordant findings between 18F-FDG PET/CT and ensuing colonoscopy were observed in 9 (13%) patients. Based on our inclusion criteria, PET/CT suggested the existence of colonic pathology in these 9 patients. The origin of the increased 18F-FDG uptake could not be identified, but possible explanations are lesions below the mucosal surface inspected with the colonoscope or shedding of 18F-FDG-containing superficial mucosal cells into the stool. Additionally, 7 small colonic low-grade adenomas (0.3–1 cm) were not identified by PET/CT. Partial-volume effects that underestimate the 18F-FDG activity of small-sized lesions or activity smearing by bowel motion are the most likely explanations (34).
A limitation of this study is that 29 of 98 patients (30%) with incidental findings were not subject to further endoscopic examination. However, we were interested in evaluating the clinical significance of these incidental 18F-FDG PET/CT findings rather than to determine their prevalence in a typical population referred for PET. An additional limitation is that missing potentially non-18F-FDG-avid GIT lesions that might have had minor structural abnormalities on the native CT cannot be excluded since we did not apply either a standard bowel preparation regimen or intravenous contrast material as a part of standard protocol in the studied patient population.
CONCLUSION
Incidental 18F-FDG PET/CT findings in the GIT—though relatively infrequent in the range of 3%—have a remarkable risk of being a cancerous or precancerous process approaching 60% in the present series. Furthermore, 18F-FDG PET/CT is able to detect subclinical inflammatory bowel disorders. Thus, identifying such lesions on a PET/CT scan should prompt colonoscopic or other appropriate evaluation, as it leads to a management change in a considerable number of patients.
Acknowledgments
The authors gratefully acknowledge Thomas Berthold, Michael Belohlavy, and Conny Britt for technical help. This research was supported in part by the Federal Commission for Scholarships, Berne, Switzerland. Part of this work was presented at the Annual Meeting of the Swiss Society of Radiology, Interlaken, Switzerland, May 12–15, 2004; at the Digestive Disease Week, New Orleans, LA, May 15–20, 2004; and at the 51st Annual Meeting of the Society of Nuclear Medicine, Philadelphia, PA, June 19–23, 2004.
Footnotes
Received Apr. 28, 2004; revision accepted July 14, 2004.
For correspondence contact: Katrin D.M. Stumpe, MD, Nuclear Medicine, Department of Medical Radiology, University Hospital of Zurich, CH-8091 Zurich, Switzerland.
E-mail: katrin.stumpe{at}usz.ch
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Management of incidental esophageal uptake on FDG PET/CT
- Assessment of incidental and clinically unsuspected fluorodeoxyglucose-avid foci detected on oncological positron emission tomography/CT
- Incidental findings on positron emission tomography/CT scans performed in the investigation of lung cancer
- Uncommon Reason for High Fluorodeoxyglucose Positron Emission Tomography Uptake
- [18F]FDG PET/CT imaging of colorectal cancer: a pictorial review
- The role of positron emission tomography in the management of non-small cell lung cancer
- PET/CT assessment of clinically unsuspected, incidental FDG-avid lesions in oncological patients
- Noninvasive Assessment of Crohn's Disease Intestinal Lesions with 18F-FDG PET/CT
- Screening for Cancer with PET and PET/CT: Potential and Limitations
- Forced Diuresis Improves the Diagnostic Accuracy of 18F-FDG PET in Abdominopelvic Malignancies
- Role of Nuclear Medicine in the Management of Cutaneous Malignant Melanoma
- Etiology of Solitary Extrapulmonary Positron Emission Tomography and Computed Tomography Findings in Patients With Lung Cancer
- 18F-FDG Imaging: Pitfalls and Artifacts