


Abstract
The purpose of this study was to evaluate outcome after 223Ra dichloride therapy (223Ra) and to determine whether skeletal tumor burden on whole-body 18F-fluoride PET/CT can be used as a predictive biomarker of survival in patients treated with 223Ra. Methods: Forty-two patients with hormone-refractory prostate cancer underwent 223Ra and a baseline fluoride PET/CT scan. Fluoride PET/CT parameters were generated, including maximum standardized uptake value (SUVmax) of the hottest lesion (hSUVmax), average SUV of disease (Mean10), and skeletal tumor burden indices of total fluoride skeletal metastatic lesion uptake (TLF10) and total volume of fluoride avid bone metastases (FTV10). Overall survival (OS) was the primary endpoint. Secondary endpoints were progression-free survival and skeletal-related event (SRE). Results: Skeletal tumor burden indices (TLF10 and FTV10) derived from fluoride PET/CT at baseline were highly correlated and significant independent predictors of OS (P = 0.0212; hazard ratio = 5.990; 95% confidence interval = 1.306–27.475). A TLF10 cutoff value of 8,000 discriminated survivors from nonsurvivors after 223Ra (with TLF10 values < 8,000, the median OS was not estimated, whereas with TLF10 > 8,000, the median OS was 6.67 mo). Visual analysis, Mean10, and hSUVmax were not predictors of OS or progression-free survival. Mean10 was found to be a significant univariate predictor of the odds of having an SRE (P = 0.0445; odds ratio = 1.30; 95% confidence interval = 1.006–1.681), with a Mean10 greater than 19 increasing the risk of SRE. Conclusion: Skeletal tumor burden on baseline fluoride PET/CT is a predictive biomarker of OS and the risk of an SRE in patients treated with 223Ra.
Several treatment modalities are used to control metastatic bone pain or prevent skeletal-related events (SREs) from prostate cancer, such as radiotherapy, bisphosphonates, denosumab, 153Sm-ethylene diamine tetramethylene phosphonate, 223Ra-dichloride therapy (223Ra), and other bone-seeking agents; however, only 223Ra has demonstrated improved survival (1–6).
In daily clinical practice, 18F-FDG PET/CT whole-body metabolic imaging is widely performed for staging, restaging, identifying responders, and predicting survival (7–10) and as a biomarker to assess tumor burden (11–14). One of the advantages of 18F-FDG PET/CT imaging is the ability to objectively quantify tumor metabolism, providing prognostic or predictive information (15–17).
Whole-body fluoride PET/CT bone imaging is ideal for staging and restaging prostate cancer patients because of greater sensitivity, specificity, and accuracy than conventional bone scintigraphy (18). Beyond lesion detection and staging, it is feasible to quantify skeletal tumor burden using fluoride PET/CT. Tumor burden determined by skeletal scintigraphy has been shown to differentiate responders from nonresponders with some therapies (19).
We hypothesized that skeletal tumor burden determined by fluoride PET/CT will be correlated with clinical outcomes in patients treated with 223Ra. By this determination, it may be possible to identify patients who will not respond to 223Ra, thus reducing morbidity and unnecessary costs.
The purposes of this study were to evaluate outcome after 223Ra and the potential of fluoride PET/CT to determine whole-body skeletal tumor burden as a prognostic biomarker of survival in patients treated with 223Ra.
MATERIALS AND METHODS
Study Design
This study was approved by the Institutional Review Board (PA14-0848). The Waivers of Informed Consent and Authorization were granted for the retrospective analysis. We reviewed castrate-resistant prostate cancer (CRPC) patients metastatic to bone treated with 223Ra who underwent baseline fluoride PET/CT scanning.
Patient Population
Three hundred eighty-nine doses were administered to 76 patients. Forty-two patients (Table 1) underwent baseline fluoride PET/CT imaging. Additionally, 38 of these 42 patients also underwent baseline bone scintigraphy and another 32 patients underwent bone scanning exclusively (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). Eleven patients (14.5%) had initial Hb levels below 10.0 g/dL and received blood transfusion before 223Ra.
Clinical Characteristics of Patients at Initial Presentation Before First 223Ra Dose
223Ra
223Ra-dichloride (Xofigo; Bayer) was administered per clinical standard of care to 76 patients. Patients received between 1 and 6 doses of 223Ra (50 kBq/kg or 1.4 μCi/kg) intravenously, at monthly intervals.
Fluoride PET/CT
Fluoride PET/CT scans were obtained after the intravenous injection of 158–370 MBq of 18F-sodium fluoride. Images were acquired on average 50–60 min after injection, from the vertex of the skull to the feet, on dedicated PET/CT scanners (Discovery STe, RX, VCT, 16- or 64-channel [GE Healthcare] or mCT Flow, 64-channel [Siemens Healthcare]). CT parameters included 3.75- or 2-mm axial reconstruction and 120 kV or Care kV tube voltage modulation (GE Healthcare or Siemens systems, respectively). PET was acquired in 3-dimensional mode using either 3–5 min/bed position or continuous bed motion (1 mm/s) according to the scanner platform. Images were reconstructed and displayed in the transverse, coronal, and sagittal planes using a MIM Vista workstation (MIM Vista).
Fluoride PET/CT Interpretation and Quantification
Baseline fluoride PET/CT images were analyzed by both visual and quantitative analyses by 2 board-certified nuclear medicine physicians. Visual analysis consisted of separating into 5 categories the number of bone metastatic lesions (1–6 lesions, 6–20, 20–50, above 50, and super scan).
Quantitative interpretation (using the MIM Vista workstation) was performed on all baseline fluoride PET/CT images to determine whole-body skeletal tumor burden (20). Briefly, the technique consists of drawing a rectangular semiautomatic volume of interest (VOI) in the whole-body image with caution to encompass all metastatic sites. After the whole-body VOI is drawn, the maximum standardized uptake value (SUVmax) threshold is set at 10, which excludes 99% of all normal bone uptake. Subsequently, the computer automatically generates individual VOIs surrounding only regions with an SUVmax of 10 or greater. Images are evaluated to manually exclude any sites of high uptake not related to bone metastases (such as the urinary activity in the renal collecting system, degenerative disease, and healing fractures). Afterward, volumetric parameters of skeletal fluoride uptake are automatically obtained from the statistics generated with the final volumetric extraction. The following parameters are obtained: highest SUVmax among all the metastases (hSUVmax), mean SUVmax of all metastases (Mean10), and skeletal tumor burden. The latter is determined by calculating the total fluoride skeletal metastatic uptake as a product of mean SUV × VOI10 (TLF10) and the total volume of fluoride bone metastases (FTV10). Figure 1 is an example of the calculation of the skeletal tumor burden.

Calculation of hSUVmax, skeletal tumor burden (TLF10 and FTV10), and Mean10 on fluoride PET/CT. (A) Fluoride PET/CT of CRPC patient being considered for 223Ra. (B) Semiautomatic VOI is drawn in whole-body image. (C) With established threshold SUVmax of 10 or greater, all background activity is subtracted, leaving metastases and some nonmetastatic VOIs with high uptake. (D) All nonmetastatic VOIs (e.g., bladder and degenerative processes) are subtracted. Statistics demonstrate hSUVmax of 138 (L1 vertebral metastasis), TLF10 of 10,965, and Mean10 of 31.63. After 6 mo, patient developed multiple vertebral compression fractures and died after 8 mo.
Once the images have been carefully analyzed, the process of calculating tumor burden is extremely fast because it is a semiautomatic measure, and the physician is not required to draw VOIs on all metastatic sites because, by establishing the threshold value for SUVmax of 10, the VOIs will automatically encircle the lesions and exclude all normal bone. If the amount of degenerative processes is minimal, the calculation of tumor burden takes less than 5 min.
Visual Interpretation of Other Imaging Modalities
Visual interpretation of 99mTc-methylene diphosphonate (99mTc-MDP) bone scintigraphy consisted of separating the number of bone metastases into the same 5 categories as with fluoride PET/CT (19). Nodal and visceral metastases were assessed visually on the images available (18F-FDG PET/CT, fluoride PET/CT, body CT scans, ultrasound, or MR imaging).
Statistical Analyses
The primary endpoint was overall survival (OS), established from initial 223Ra dose until date of death from any cause or last follow-up. Secondary aims were progression free-survival (PFS) and time-to-bone event (TTBE). PFS was established from initial 223Ra dose until date of objective tumor progression, death of any cause, or last follow-up. Objective tumor progression was defined as a new lesion or a lesion that increased in size (Response Evaluation Criteria In Solid Tumors) in bone, node, or viscera leading to a change in current therapy or initiation of another therapy. TTBE was defined from initial 223Ra dose until the date of a bone event (surgical intervention, spinal cord compression, pathologic fracture, bone pain, or rapid lesion progression requiring immediate intervention).
Frequencies and percentages were provided for categoric variables; mean (SD) and median (range) were provided for continuous variables. Kaplan–Meier survival curves demonstrated survival time distributions. Cox proportional hazards regression was used to analyze predictors of survival. Backward stepwise selection was performed for multivariable Cox models. Logistic regression modeled the odds of a bone event as a function of fluoride PET/CT variables. Spearman correlation assessed the amount of agreement between fluoride PET/CT variables. All statistical analyses were performed using SAS 9.3 for Windows (SAS Institute).
RESULTS
223Ra Doses in Relation to OS, PFS, and TTBE
223Ra doses were completed in 44 (57.9%) patients, 1 patient was still undergoing 223Ra, and 31 (40.8%) patients did not complete all 6 doses because of either progression, hematologic toxicity, declining Eastern Cooperative Oncology Group (ECOG) status by 2 points, or a bone event (Table 2). The mean number of doses performed was 5 (median, 6 doses). The median OS time was 11.93 mo (95% confidence interval [CI] = 8.12–censored). The median PFS was 3.68 mo (95% CI = 3.02–5.09), and the median TTBE could not be estimated (only 6 patients had bone events) (Tables 3 and 4).
Demographics and Clinical Characteristics of 42 Patients at Initial Presentation Before First 223Ra Dose
Correlation to OS
Correlation to PFS
There was a significant correlation between OS and the number of 223Ra doses administered, with improved survival in patients treated with a greater number of doses, especially in patients receiving all 6 doses. The number of 223Ra doses was an independent predictor of OS, was beneficial, and reduced the risk of death.
Likewise, the risk of progression was lower in patients receiving more 223Ra doses, and PFS was higher in patients who received all 6 doses. Additionally, more 223Ra doses was an independent predictor of PFS. There was no correlation between TTBE and the continuous number of 223Ra doses delivered to patients.
Visual Imaging Analysis in Relation to OS and PFS
Visual analyses were performed on 42 patients who underwent fluoride PET/CT and on 70 patients who underwent bone scintigraphy. Among these 70 patients, 32 underwent only bone scintigraphy and 38 underwent bone scintigraphy and fluoride PET/CT. There were no differences in the clinical characteristics among patients who underwent only bone scintigraphy versus patients who underwent both scans (Supplemental Table 2). OS strongly correlated with the presence of bone metastases on visual analysis only on fluoride PET/CT scans. On multivariate analysis, however, neither visual analysis of fluoride PET/CT scans nor the presence of nodal or visceral metastases were predictors of OS.
PFS had a strong correlation to visual analysis of both fluoride PET/CT and bone scintigraphy after 223Ra and to the presence of nodal or visceral metastases. For example, patients with more than 50 bone metastases had twice the risk of progression when compared with a patient with fewer than 20 bone metastases. The risk of progression increased 2.7 times for patients with nodal metastases and 2.1 times for the presence of visceral metastases. However, on a multivariate model, only the presence of nodal metastases at initial diagnosis was a significant predictor of PFS (P = 0.0080).
Quantitative Imaging Analysis in Relation to OS, PFS, and TTBE
Quantitative analyses were performed on baseline fluoride PET/CT in 42 patients. The parameters Mean10, hSUVmax, TLF10, and FTV10 were correlated to OS, PFS, and TTBE.
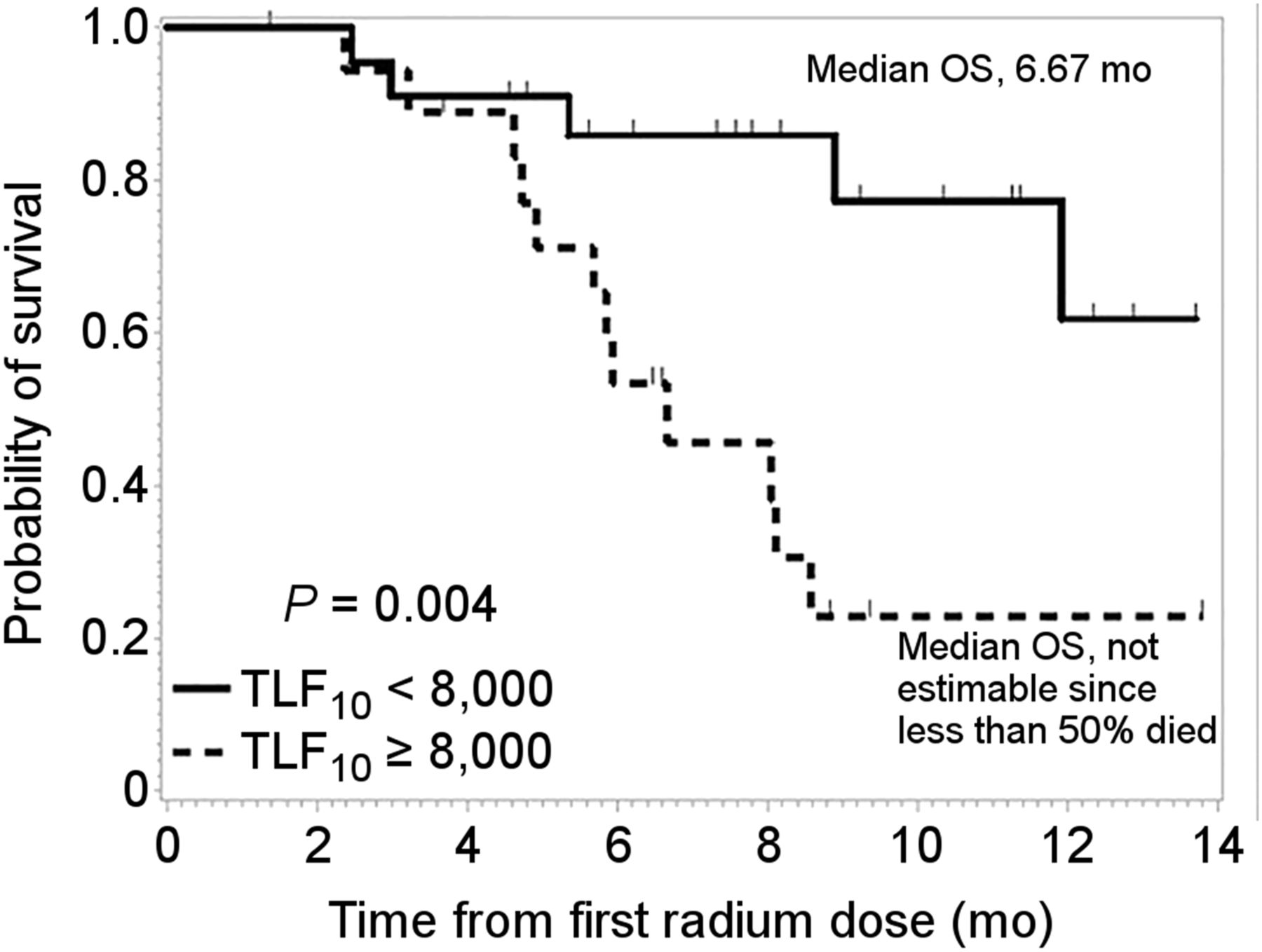
OS was strongly predicted by both TLF10 and FTV10. Because TLF10 and FTV10 were shown to be highly correlated (ρ = 0.95; P < 0.0001), all further analyses were performed solely with TLF10 values. TLF10 was shown to be significant independent predictor of OS. When establishing the TLF10 cutoff value at 8,000 (Fig. 2), it was possible to generate survival curves and identify which patients would most likely benefit from 223Ra. There were fewer than 50% of deaths with TLF10 less than 8,000; thus, the median OS was not estimated (95% CI = 8.90–not estimated). However, with a TLF10 greater than 8,000, the median OS was 6.67 mo (95% CI: 4.73–8.57). Mean10 and hSUVmax were not predictors of OS.

OS according to TLF10 on fluoride PET/CT.
PFS did not correlate with TLF10, FTV10, Mean10, or hSUVmax.
Mean10 was found to be a significant univariate predictor of the odds of having an SRE (P = 0.0445; odds ratio = 1.30; 95% CI = 1.006–1.681), with a Mean10 greater than 19 increasing the risk of SRE (sensitivity = 0.83; specificity = 0.67). It was not possible to predict TTBE or the odds of having a bone event by TLF10, FTV10, or hSUVmax. Figure 3 shows an example of fluoride PET/CT skeletal tumor burden determination and patient outcome.

Baseline fluoride PET/CT images of patient with castrate-resistant prostate cancer prior to 223Ra show widespread bone metastases (PSA = 36.0 ng/mL and ALP = 109 U/L). Skeletal tumor burden measurements were: TLF10 = 14,643 and Mean10 = 21.1. Patient developed compression fracture after 2 mo of 223Ra and died after 4 mo.
DISCUSSION
To our knowledge, this is the first study to demonstrate that volumetric semiautomatic quantification of whole-body skeletal tumor burden on fluoride PET/CT is an independent predictor of OS in CRPC patients treated with 223Ra. OS has been shown to improve after 223Ra in CRPC patients with bone metastases (1–3). We found that more 223Ra doses were an independent predictor of OS, reducing the risk of death by 60% for each continuous increase in dose. However, although 223Ra has been shown to improve survival, there is heterogeneity of response, with some patients showing limited or poor response.
As with any therapy, it is important to identify factors that may influence response. In the phase III study of 223Ra in CRPC, improvements in time to first SRE and OS occurred in the 223Ra arm (vs. placebo arm). Although time to total alkaline phosphatase (ALP) and prostate-specific antigen (PSA) progression and ALP response were significantly longer in the 223Ra arm, unfortunately these markers were not predictors of response or predictors of OS. In our study, fluoride PET/CT skeletal tumor burden correlated with OS, similar to prior studies using 18F-FDG PET/CT (21,22). Fluoride PET/CT skeletal tumor burden (TLF10) with a cutoff value of 8,000 discriminated survivors from nonsurvivors after 223Ra. The risk of death after 223Ra was increased by 76.5% for each unit increase in TLF10. Evaluation of target lesions with 18F-FDG PET/CT have demonstrated strong correlation to OS (17,23–25). We were not able to predict OS, PFS, or TTBE by evaluation of a target lesion (hSUVmax), because patients had widespread metastases, whereas target lesions usually were applicable for evaluation of the primary tumor.
Although previous reports have demonstrated the ability of predicting OS with bone scintigraphy, either visually or semiquantitatively, this can be a time-consuming process (19,26,27). Visual analysis of fluoride PET/CT and 99mTc-MDP bone scintigraphy demonstrated that only fluoride PET/CT scans were a significant univariate predictor of OS (visual analysis of 99mTc-MDP scans were not, although there was a tendency [P = 0.0871] in patients with multiple metastases). Possibly we did not reach statistical significance in bone scanning because of the small number of patients studied. On the other hand, fluoride PET/CT imaging has a high impact on management of CRPC patients when compared with body CT or MR imaging (28). In addition, 18F-fluoride uptake is 2-fold higher than 99mTc-MDP, leading to improved lesion detectability (29,30). Furthermore, although fluoride PET/CT has a higher cost, acquisition time is faster and spatial resolution higher, and images may be acquired earlier (31–33). All these factors lead to a better performance of fluoride PET/CT to detect bone lesions and to define equivocal bone metastases (18,34,35). For example, in our patient population, among the cases in which fluoride PET/CT detected above 20 bone metastases, bone scintigraphy detected less in 63% of the patients, although we cannot be certain if this difference of lesion detectability could affect patient management. However, because visual analysis of fluoride PET/CT was not an independent predictor of OS, the findings in our study support the idea that objective skeletal tumor burden quantification is an important parameter to independently predict OS.
Bone-related laboratory parameters in CRPC patients have also been described as predictors of survival (36). Worse survival has been associated with ALP greater than 146 U/L, pain score greater than 3, SREs, PSA greater than 10 ng/mL, hemoglobin less than 12.8 g/dL, visceral metastases, ECOG greater than 1, and older age. In our patient group, we did not evaluate these parameters because our cohort was composed of patients in whom most of these parameters already indicated advanced disease. Among the patients with a TLF10 greater than 8,000, PSA levels were high in 83% (mean = 211 ng/mL). Interestingly, though, 4 patients in our study had a PSA less than 10 ng/mL, with surprisingly high TLF10 (>8,000). One patient had a PSA of 2.3 ng/mL with a TLF10 of 22,969 whereas the other had a PSA of 7.5 ng/mL with a TLF10 of 25,841, both having deceased after 5 mo of beginning 223Ra. ALP may reflect more accurately than PSA levels the extent of bone disease (37); however, in our study, 9 patients with an ALP less than 146 U/L had a TLF10 greater than 8,000 and 6 of them were deceased after an average of 6.9 mo. In addition, as with other studies, visceral and nodal metastases were also univariate predictors of OS. Because the number of 223Ra doses in itself is a strong predictor of OS, the fact that skeletal tumor burden was an even a stronger predictor establishes fluoride PET/CT as an important imaging modality to guide treatment strategies, combined with laboratory results, which sometimes may be misleading.
Many of the patients progressed during 223Ra (median time to progression = 3.68 mo). We found that the risk of progression (including death) was reduced by 55.3% with more 223Ra doses, and patients who received all 6 doses had a 65% reduction of PFS. Although it seems logical that PFS would be longer in patients who received more 223Ra doses in comparison to those who did not receive doses because of death, this was not the case. Among the patients who progressed during 223Ra, only 20% died immediately after 223Ra, whereas the other 80% continued 223Ra (with the addition of chemotherapy) or discontinued 223Ra (and were switched to chemotherapy). Those patients who continued 223Ra benefitted from more doses as opposed to those who discontinued the treatment. We did not find a correlation between skeletal tumor burden and PFS. On the other hand, nodal or visceral metastases were strong univariate predictors of shorter PFS, which could be expected, because 223Ra does not target extraskeletal metastases. However, on a multivariate analysis, only the presence of nodal metastases at the first 223Ra treatment was an independent predictor of shorter PFS. Because chemotherapy and hormonal therapy has improved OS of prostate cancer patients with visceral metastases (38–41), our patients with visceral metastases were treated with combination 223Ra and chemotherapy (cyclophosphamide [6 patients], paclitaxel [3 patients], doxorubicin [1 patient], docetaxel [1 patient], and mitoxantrone [1 patient]) or secondary hormonal agents (abiraterone or enzalutamide). The concomitant use of chemotherapy with 223Ra may account for the fact that the presence of visceral metastases was not an independent predictor of PFS.
A 30% increase in the risk of a bone event occurred in patients with a higher Mean10. Bone events occurred only in 6 patients (spinal cord compression [1 patient], pathologic bone fracture [4 patients], and intractable bone pain [1 patient]). Therefore, knowledge up front that a Mean10 greater than 19 on a baseline fluoride PET/CT before 223Ra increases the risk of a bone-related event should heighten awareness of potential complication and may prompt close surveillance.
When our results were compared with the ALSYMPCA trial (1), we found that our median OS was lower (11.93 vs. 14.9 mo, respectively), which may be due to patient characteristics. We also found that the percentages of patients with super scans (27.6% vs. 9%), with ECOG status greater than 2 (32.9% vs. 13%), and with fewer than 6 bone metastases (5.3% vs. 16%) were lower. Combined, these indicate a higher skeletal tumor burden in our population, which likely accounts for the reduced OS in comparison to the ALSYMPCA trial. The greater proportion of patients in our group with high skeletal tumor burden was not based on a specific selection criteria, and many patients underwent 223Ra in a compassionate setting.
A high Gleason score normally accounts for patients having high skeletal tumor burden. It could be that the outcome we observed was related to most of our patients having a high Gleason score. Maybe, in patients with lower Gleason scores (6 and 7) the outcome might have been better and a study evaluating patients only with low Gleason score is necessary to confirm our findings. However, in our study, a low Gleason score was also related to a high tumor burden. All patients in our study were already castrate-resistant, with progression, and had already undergone multiple lines of chemotherapy before 223Ra. There was a similar percentage of deaths among patients with a Gleason score of 8–10 and Gleason 6 and 7 (45% vs. 40%, respectively). The comparable outcome is not surprising because patients with low Gleason scores tend to develop castrate-resistance after many years of initial diagnosis when compared with patients with higher Gleason score: the mean time to perform 223Ra from initial diagnosis of prostate cancer was 11 y for patients with a Gleason score of 6 or 7 and 7 y for patients with Gleason 8–10.
CONCLUSION
Fluoride PET/CT skeletal tumor burden is a powerful and novel predictive biomarker of OS and of the risk of a bone event in CRPC patients treated with 223Ra. Fluoride PET/CT skeletal tumor burden before 223Ra may be able to separate responders from nonresponders in a reproducible and objective manner and identify patients at most risk of SREs during or after 223Ra therapy.
It might be that fluoride PET/CT is a robust prognostic predictive imaging biomarker for other therapies in CRPC. Its use could extend beyond CRPC, as well, providing determination of skeletal tumor burden in patients with breast cancer and sarcomas. Further work is needed to assess whether fluoride PET/CT measures of skeletal tumor burden in these other settings impart similar predictive value with OS and other outcomes as with 223Ra.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work is supported by the James E. Anderson Distinguished Professorship Endowment and also in part by the Cancer Center Support grant (NCI grant P30CA016672) and the Fundação de Amparo à Pesquisa da Universidade de São Paulo (FAPESP 2014/03317-8). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 11, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 31, 2015.
- Accepted for publication May 23, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Whole-Skeleton SUVmean Measured on 18F-NaF PET/CT Studies as a Prognostic Indicator in Patients with Breast Cancer Metastatic to Bone
- The Prognostic Value of Quantitative Bone SPECT/CT Before 223Ra Treatment in Metastatic Castration-Resistant Prostate Cancer
- First Whole-Body Three-Dimensional Tomographic Imaging of Alpha Particle Emitting Radium-223
- Comparison of the Variability of SUV Normalized by Skeletal Volume with the Variability of SUV Normalized by Body Weight in 18F-Fluoride PET/CT
- Development of sodium fluoride PET response criteria for solid tumours (NAFCIST) in a clinical trial of radium-223 in osteosarcoma: from RECIST to PERCIST to NAFCIST
- Validation of the Semiautomatic Quantification of 18F-Fluoride PET/CT Whole-Body Skeletal Tumor Burden
- 223Ra Therapy of Advanced Metastatic Castration-Resistant Prostate Cancer: Quantitative Assessment of Skeletal Tumor Burden for Prognostication of Clinical Outcome and Hematologic Toxicity
- Hospice Admission and Survival After 18F-Fluoride PET Performed for Evaluation of Osseous Metastatic Disease in the National Oncologic PET Registry
- Exploring New Multimodal Quantitative Imaging Indices for the Assessment of Osseous Tumor Burden in Prostate Cancer Using 68Ga-PSMA PET/CT
- Association between neuroendocrine tumors biomarkers and primary tumor site and disease type based on total 68Ga-DOTATATE-Avid tumor volume measurements
- 68Ga-PSMA-11 PET as a Gatekeeper for the Treatment of Metastatic Prostate Cancer with 223Ra: Proof of Concept
- Radium-223: Insight and Perspectives in Bone-metastatic Castration-resistant Prostate Cancer
- Bone-Targeted Imaging and Radionuclide Therapy in Prostate Cancer
- Reply: Prediction vs. Prognostication and Guarantee-Time Bias: Steering Clear of the Pitfalls of Interpreting Observational Data
- Prediction vs. Prognostication and Guarantee-Time Bias: Steering Clear of the Pitfalls of Interpreting Observational Data
- 18F-Fluoride PET in the Assessment of Malignant Bone Disease