


Abstract
The purpose of this study was to correlate 18F-sodium fluoride accumulation in the common carotid arteries of neurologically asymptomatic patients with cardiovascular risk factors and carotid calcified plaque burden. Methods: Two hundred sixty-nine oncologic patients were examined by 18F-sodium fluoride PET/CT. Tracer accumulation in the common carotid arteries was analyzed both qualitatively and semiquantitatively by measuring the blood-pool–corrected standardized uptake value (target-to-background ratio) and comparing it with cardiovascular risk factors and calcified plaque burden. Results: 18F-sodium fluoride uptake was observed at 141 sites in 94 (34.9%) patients. Radiotracer accumulation was colocalized with calcification in all atherosclerotic lesions. 18F-sodium fluoride uptake was significantly associated with age (P < 0.0001), male sex (P < 0.0001), hypertension (P < 0.002), and hypercholesterolemia (P < 0.05). The presence of calcified plaque correlated significantly with these risk factors but also with diabetes (P < 0.0001), history of smoking (P = 0.03), and prior cardiovascular events (P < 0.01). There was a highly significant correlation between the presence of 18F-sodium fluoride uptake and number of present cardiovascular risk factors (r = 0.30, P < 0.0001). Conclusion: Carotid 18F-sodium fluoride uptake is a surrogate measure of calcifying carotid plaque, correlates with cardiovascular risk factors, and is more frequent in patients with a high-risk profile for atherothrombotic events but demonstrates a weaker correlation with risk factors than does calcified plaque burden. This study provides a rationale to conduct further prospective studies to determine whether 18F-sodium fluoride uptake can predict vascular events, or if it may be used to monitor pharmacologic therapy.
The occurrence of cerebral infarction in patients with carotid atherosclerosis is closely associated with the degree of luminal stenosis (1,2). The role of invasive therapy such as carotid endarterectomy remains uncertain in a substantial number of patients, particularly in those who are asymptomatic and have only moderate stenosis (3,4). Therefore, other markers are needed to identify high-risk patients and guide timely intervention.
Pathophysiologic processes involved in development and progression of atherosclerotic plaque include inflammation, necrosis, apoptosis, and mineralization (5,6), each of which represents a possible target for imaging (7,8).
Numerous studies have demonstrated the reliability of 18F-FDG PET/CT in imaging plaque inflammation in large arteries (9–11). 18F-FDG uptake in atherosclerotic lesions correlates with the presence of cardiovascular risk factors and might identify patients at risk for future vascular events (9,12–14). Recently, several authors reported visualization of macrophage activity in atherosclerotic plaque using 18F-fluorocholine and 11C-choline PET/CT (15–17). Because most of these studies demonstrated infrequent colocalization of radiotracer uptake and calcification, the ability of these tracers to provide insights into functional properties of calcified atherosclerotic lesions appears to be limited.
Calcium mineral deposits are a common constituent of atherosclerotic plaque, are readily quantifiable radiographically, and serve as a surrogate marker for atherosclerosis. The feasibility of 18F-sodium fluoride PET/CT for imaging of atherosclerotic plaque has recently been demonstrated by our group (18). We postulated that 18F-sodium fluoride may provide molecular information about the activity of the calcification process and that plaques still accumulating 18F-sodium fluoride might represent progressive lesions. Tracer uptake associated with calcified plaque might predict an increased likelihood of adverse events (19).
The purpose of the present study was to further investigate the nature of 18F-sodium fluoride accumulation in atherosclerotic plaque in the common carotid arteries. To that end, we correlated carotid 18F-sodium fluoride uptake with atherogenic risk factors and carotid calcified plaque burden in a large cohort of neurologically asymptomatic patients.
MATERIALS AND METHODS
Study Patients
The study group consisted of 269 oncologic patients (166 women, 103 men; mean age ± SD, 66.1 ± 12.4 y; age range, 21.6–90.1 y) who had been referred to our department for an 18F-sodium fluoride PET/CT scan between December 2008 and April 2010 for exclusion of bone metastases. The patient inclusion criterion was the availability of digital image data for retrospective analysis. Exclusion criteria included the inability or unwillingness to provide informed consent for the retrospective analysis of the data, history of vasculitis or systemic inflammatory disease, vascular event in the preceding 12 wk, and chemotherapy in the preceding 8 wk.
Atherogenic risk factors including patient age; sex; body mass index (BMI); smoking habits; and presence of hypertension, hypercholesterolemia, and diabetes were documented. A history of prior vascular events defined as myocardial infarction or cerebrovascular insult was identified for all patients. Treatment with statins was recorded (10). Risk factors were considered categoric variables. Patients were considered at risk if they were 55 y or older for women or 45 y or older for men, adopting a cutoff for age from the Framingham heart study (20). Patients were assigned to groups according to the number of present cardiovascular risk factors: group 1, no or 1 risk factor; group 2, 2 or 3 risk factors; group 3, 4, or 5 risk factors; and group 4, more than 6 risk factors. The study protocol had been approved by the local Clinical Institutional Review Board and complied with the Declaration of Helsinki. All patients had given written informed consent for the retrospective evaluation of their data. Seventy-five of the 269 patients had been included in a previous study assessing the feasibility of 18F-sodium fluoride PET/CT for plaque imaging (18).
Image Acquisition and Reconstruction
All patients underwent 18F-sodium fluoride PET/CT on a hybrid system (Gemini GXL 10; Philips) combining a full-ring, 3-dimensional–only PET scanner equipped with gadolinium orthosilicate crystal detectors. Patients received an intravenous injection of 18F-sodium fluoride (350 ± 50 MBq). During the uptake period of 60 min, patients were hydrated orally with water. Imaging started with a nonenhanced, low-dose CT scan of the whole body (120 kV, 80 mA). Next, PET of the whole body was performed, with 90 s per bed position starting at the head. Overlap between consecutive bed positions was 50%. Transversal PET slices were reconstructed into a 144 × 144 matrix using the iterative 3-dimensional line-of-response reconstruction algorithm of the system software, with standard parameter settings. The low-dose CT scan extrapolated to 511 keV was used for PET attenuation correction. Voxel size was 4 × 4 × 4 mm. The spatial resolution in the reconstructed PET images was about 8 mm in full width at half maximum.
Image Analysis
All images were analyzed by 2 independent readers masked to all subjects’ clinical information both on the basis of lesions and on the basis of arterial segments.
18F-Sodium Fluoride Uptake.
PET images were visually evaluated for the presence of focal radiotracer accumulation in the vessel wall of the common carotid arteries. A lesion was excluded from further analysis if it was suspected of being an artifact caused by incorrect coregistration of PET and CT images or by activity spillover from extravascular structures. Arterial segments were classified as being PET-positive (PET+) if at least 1 location with radiotracer uptake was detected in the vessel wall. Semiquantitative analysis was performed by measuring the maximum standardized uptake value (SUVmax) by placing an individual region of interest (ROI) around the lesion on coregistered transaxial PET/CT images. That standardized uptake value was divided by an averaged blood-pool standardized uptake value derived from 3 circular ROIs placed in the mid lumen of the superior vena cava. This calculation yielded an arterial target-to-background ratio (TBR).
Arterial Calcification.
CT images were visually evaluated for the presence of sites of arterial calcification in the carotid arteries, defined as high-density mural areas (attenuation > 130 Hounsfield units). The number of distinct calcification sites was determined, and the largest calcified plaque in each carotid segment was further characterized by measuring its maximum thickness and by scoring it on a scale for grading circumferential extent (Table 1). An arterial segment was classified as being CT-positive (CT+) if at least 1 calcified lesion was detected in it.
Quantification of Arterial Wall Calcifications Using CT-Based Score
Statistical Analysis
Continuous variables are expressed as mean ± SD. Categoric variables are presented with absolute and relative frequencies. For between-group comparisons of continuous data, P values were calculated from unpaired t tests for parametric data and from Mann–Whitney U rank sum tests for nonparametric data. For categoric variables, P values were computed from contingency tables using Fisher's exact test. The nonparametric Spearman correlation coefficient (r) was used to correlate imaging findings. P values of less than 0.05 were considered statistically significant.
Reproducibility.
To evaluate intra- and interrater agreement, assessment of carotid calcification and radiotracer uptake was repeated 4 wk after the initial review by the same reader and by a second reviewer. Cohen's κ with 95% confidence interval (CI) was used to measure both intra- and interrater agreement (21).
RESULTS
Patient Population
18F-sodium fluoride measurements in the common carotid arteries were feasible in all patients. Five lesions were excluded from further analysis because they were suspected of being an artifact. Relevant characteristics of the included patients are reported in Table 2.
Subject Characteristics and Atherogenic Risk Factors of Study Population (n = 269)
Carotid 18F-Sodium Fluoride Accumulation and Calcification
18F-sodium fluoride uptake was observed at 141 sites in 94 (34.9%) of the 269 study patients (Table 3). Radiotracer accumulation was bilateral in 46 (48.9%) patients. Mean SUVmax was 1.9 ± 0.5, and values ranged from 0.8 to 4.2. Mean TBR was 2.2 ± 0.6, and values ranged from 1.0 to 4.5.
Calcification and 18F-Sodium Fluoride Uptake in Carotid Arteries
Calcified atherosclerotic plaques were observed at 381 sites in 115 (42.8%) of the 269 study patients (Table 3). There were on average 2.0 ± 1.2 distinct calcification sites in an affected patient. The mean calcification score of the largest lesion in carotid arterial segments with 18F-sodium fluoride uptake was 1.9 ± 1.0, and the mean thickness of these calcified lesions was 2.6 ± 1.1 mm (range, 0.5–6.4 mm).
Of the 538 studied segments in total, 140 (26.0%) were found to be PET+ and CT+ and 46 (8.6%) PET-negative (PET−) and CT+. Because 18F-sodium fluoride uptake and calcification were colocalized at all sites, no PET+/CT-negative (CT−) patients were observed in our study. Relevant clinical data of PET+/CT+ and PET−/CT+ patients are reported in Table 4.
Subject Characteristics and Atherogenic Risk Factors of Patients with Calcified Carotid Plaque (n = 115)
In 154 (57.2%) patients, no vascular wall lesion was found by either CT or PET (PET−/CT−). When compared with the PET+ study population, these patients were found to be significantly younger (62.2 ± 12.7 vs. 70.0 ± 9.2 y; P < 0.0001). Additional information about PET−/CT− patients is reported in Table 2. Examples of 18F-sodium fluoride uptake in calcified carotid plaque are shown in Figures 1 and 2.
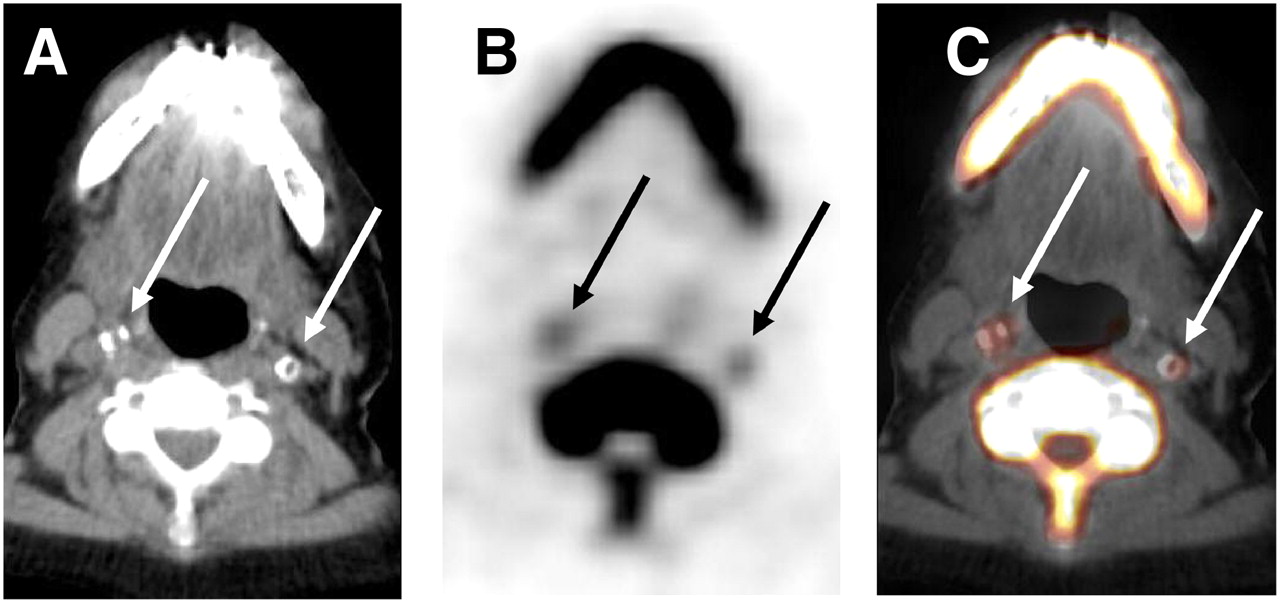
Transaxial 18F-sodium fluoride PET/CT images of common carotid arteries of 72-y-old woman: CT (A), PET (B), and fused PET/CT (C) images. 18F-sodium fluoride accumulation in carotid plaque is bilateral and colocalized with calcification. Arrows = calcified lesion.
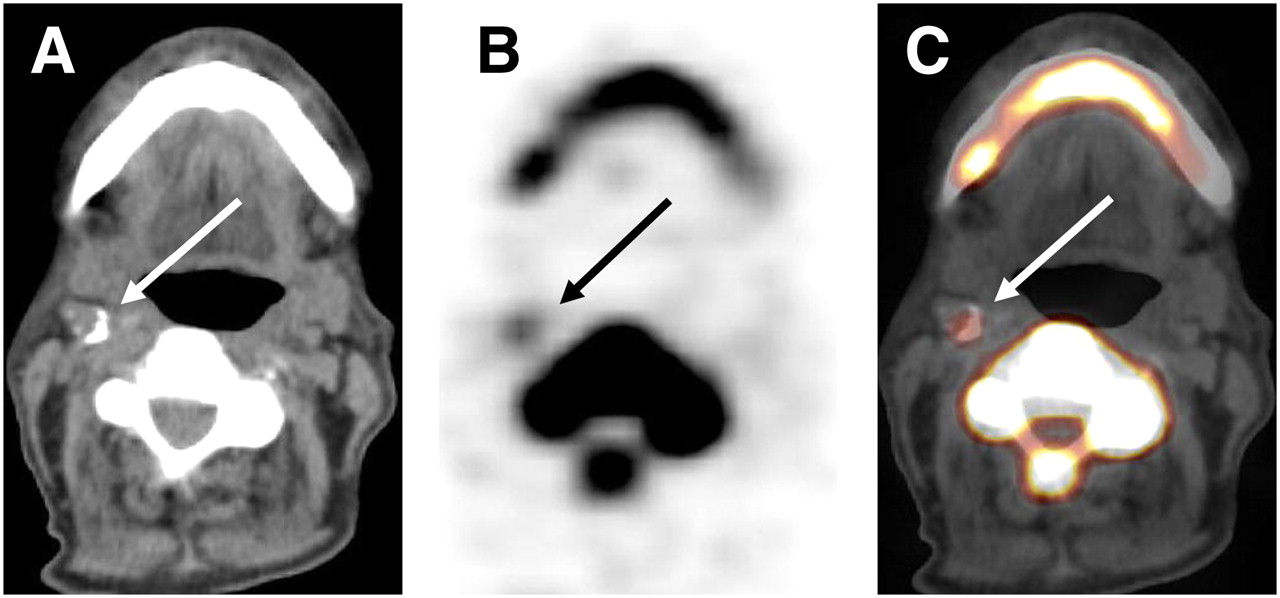
Transaxial 18F-sodium fluoride PET/CT images of common carotid arteries of 80-y-old man: CT (A), PET (B), and fused PET/CT (C) images. 18F-sodium fluoride uptake accumulation in atherosclerotic lesion coincides with calcification. Arrows = calcified lesion.
Relationship Between Carotid 18F-Sodium Fluoride Uptake, Calcified Plaque Burden, and Risk Factors
The presence of vascular 18F-sodium fluoride accumulation showed highly significant correlation with calcification within the atherosclerotic lesion (r = 0.85; P < 0.0001). There was also significant correlation between intensity of radiotracer uptake (SUVmax) and both calcification score (r = 0.33; P < 0.0001) and calcified lesion thickness (r = 0.23; P < 0.01). The presence of carotid radiotracer accumulation (Table 2) was significantly associated with age (P < 0.0001), male sex (P < 0.0001), hypertension (P < 0.002), and hypercholesterolemia (P < 0.05). No statistically significant association was found between 18F-sodium fluoride uptake and history of smoking (P = 0.12), diabetes (P = 0.11), obesity (P = 0.44), or prior cardiovascular events (P = 0.65). However, tracer accumulation correlated significantly with pack years (r = 0.14; P < 0.02) and inversely with BMI (r = −0.13; P < 0.04).
The presence of calcified carotid plaque was significantly associated with age (P < 0.0001), male sex (P < 0.0001), hypertension (P < 0.0001), hypercholesterolemia (P = 0.002), diabetes (P < 0.0001), history of smoking (P = 0.03), and prior cardiovascular events (P < 0.01). No statistically significant association was found between calcification and presence of obesity (P = 0.62). Both presence of calcified plaque and tracer uptake were significantly associated with current statin medication (P < 0.002 and 0.04, respectively), likely due to the high cardiovascular risk profile in these patients requiring medication. TBR for calcified lesions in patients with current statin medication (2.2 ± 0.4) did not significantly differ from TBR in patients without statins (2.2 ± 0.2).
When patients were assigned to groups according to the number of present cardiovascular risk factors, the prevalence of carotid 18F-sodium fluoride uptake increased as the number of cardiovascular risk factors increased (r = 0.30, P < 0.0001). Carotid tracer uptake was seen in 10.9% of patients in group 1 (n = 46), 33.6% in group 2 (n = 128), 48.1% in group 3 (n = 81), and 57.1% in group 4 (n = 14). There was no significant correlation between TBR and number of risk factors (r = −0.009, P = 0.93). The relationship between the number of cardiovascular risk factors and presence of 18F-sodium fluoride uptake is illustrated in Figure 3.

Relationship between cardiovascular risk factors and presence of 18F-sodium fluoride uptake in carotid arteries. Percentage of patients with radiotracer accumulation increases as number of risk factors increases (P < 0.0001).
When patients with calcified plaque in the carotid arteries (CT+) were subdivided into those with (PET+) or without arterial radiotracer uptake (PET−), absence of vascular 18F-sodium fluoride was associated with both diabetes (P < 0.02) and prior cardiovascular events (P = 0.01). Without reaching statistical significance, there was a trend toward higher prevalence of all risk factors except hypertension in those PET− patients (Table 4). In patients with carotid calcifications, statin medication was more frequent in the PET− subgroup (28.6%) than in the subjects with 18F-sodium fluoride accumulation (19.1%).
Therefore, we subdivided subjects with calcified plaque in the carotid arteries (CT+) into those with (n = 24) or without (n = 91) statin medication. The prevalence of carotid tracer uptake was lower in those patients with statin medication, without reaching statistical significance (75% vs. 83%, P = 0.38). Post hoc power analysis revealed that the experiment had a power of just 20% to detect a change of 10% in the prevalence of radiotracer uptake with a significance level of 0.05 (2-tailed). The prevalence of hypertension (87.5% vs. 49.5%, P < 0.001) and hypercholesterolemia (91.7% vs. 16.5%, P < 0.0001) was significantly higher in patients receiving statins. The prevalence of diabetes (33.3% vs. 17.6%, P = 0.1) and prior cardiovascular events (25% vs. 11%, P = 0.1) was higher in patients receiving statins, without being significant.
Reproducibility
The interrater Cohen's κ was 0.92 (95% CI, 0.87–0.97) for radiotracer uptake and 0.94 (95% CI, 0.90–0.98) for calcified plaque burden. The intrarater Cohen's κ was 0.94 (95% CI, 0.89–0.98) for tracer accumulation and 0.98 (95% CI, 0.96–1.0) for calcified plaque burden.
DISCUSSION
We present the first study, to our knowledge, that reports on the correlation of 18F-sodium fluoride uptake in calcifying carotid plaque with conventional cardiovascular risk factors in a large cohort of asymptomatic individuals who were investigated for noncardiovascular indications. We found a highly significant correlation between 18F-sodium fluoride uptake and the presence and extent of arterial wall calcification. Additionally, we found significant correlations between tracer uptake and cardiovascular risk factors. These findings indicate a potential role for 18F-sodium fluoride as a tool for the visualization of ongoing mineral deposition in atherosclerotic plaque in the carotid arteries and in other major arteries.
Comparison to Other PET Tracers and Cardiovascular Risk Factors
There is an emerging role for nuclear medicine techniques such as PET/CT in assessing atherosclerosis by analyzing the biologic composition and pathophysiologic processes in atherosclerotic lesions (9,13,16,22). Common PET tracers currently in use or under investigation for assessment of atherosclerosis exhibit some inherent limitations. 18F-FDG often shows significant myocardial uptake and intense tracer accumulation in the brain, making evaluation of clinically relevant atherosclerotic lesions in coronary or cerebral arteries somewhat difficult. Assessment of the right coronary artery using 11C-choline or choline derivatives is impaired because of high uptake of these tracers in the liver (16). Additionally, the clinical use of 11C-choline is limited by its short half-life. 18F-sodium fluoride is rapidly cleared from the circulation and demonstrates no relevant soft-tissue uptake. Consequently, we found a mean TBR of 2.2 ± 0.6 in the studied arterial walls—substantially higher than the intensity of arterial tracer uptake reported for 18F-FDG (12,13). Therefore, 18F-sodium fluoride demonstrates certain favorable characteristics for arterial plaque imaging, including the potential evaluation of coronary and cerebral vascular disease.
Several studies have correlated radiotracer uptake on PET/CT with the presence of cardiovascular risk factors (9,23). Saam et al. demonstrated significant correlations between TBR of the left anterior descending coronary artery and risk factors using 18F-FDG PET/CT (13). Rudd et al. evaluated 18F-FDG uptake within carotid plaques in patients with recently symptomatic carotid stenosis, with considerably less uptake being shown in contralateral asymptomatic arteries (14). Moreover, Rominger et al. found that 18F-FDG uptake in large arteries may be associated with subsequent vascular events (12). In our study, 18F-sodium fluoride uptake in the common carotid arteries was significantly associated with age, male sex, hypertension, hypercholesterolemia, and cumulative smoking exposure. Additionally, the prevalence of radiotracer uptake strongly increased with the number of present atherogenic risk factors. The fact that radiotracer uptake was not significantly associated with diabetes or a history of cardiovascular events might be explained by insufficient statistical power as revealed by post hoc power analysis. Furthermore, tracer accumulation correlated inversely with BMI, but significance was weak (P < 0.04). This might in part be explained by the fact that assessment of body mass is affected by cachexia in our oncologic patient cohort, possibly distorting these results.
Interestingly, in those patients with calcified carotid plaque, all cardiovascular risk factors except hypertension were more frequent in those subjects without arterial 18F-sodium fluoride accumulation (Table 4). Although one would expect 18F-sodium fluoride uptake to be more frequent in patients with a higher prevalence of risk factors based on the correlations described in this article, that finding might in part be explained by the fact that medication with statins was more common in the PET− group (28.6 vs. 19.1%). When the analysis of CT+ patients was adjusted for statin use, carotid 18F-fluoride uptake was less frequent in patients receiving statins, without reaching statistical significance, although the prevalence of risk factors was higher in those patients. Tahara et al. observed that the attenuation of plaque inflammation caused by statins can be monitored by 18F-FDG PET/CT (10). Another study demonstrated that statin therapy is associated with reduced rates of plaque progression among individuals with asymptomatic carotid atherosclerosis (24). Because statins exhibit a variety of cholesterol-independent, plaque-stabilizing effects involved in endothelial function, cell proliferation, inflammatory response, and lipid oxidation, they might ultimately affect 18F-sodium fluoride uptake (25). However, in the present study it could not be demonstrated that statin therapy significantly affected tracer uptake. These findings provide a rationale for further prospective studies to investigate whether 18F-sodium fluoride may be used to monitor response to pharmacologic interventions.
The highly significant correlation between radiotracer uptake and calcification in our study demonstrates that 18F-sodium fluoride provides additional information about pathophysiologic processes and biologic activity of calcified plaque. As is well known from previous studies using different tracers such as 18F-FDG or choline derivatives, focal vascular metabolic activity and vascular calcification rarely overlap (9,11,15,16). In contrast, in the present study we observed colocalization of carotid 18F-sodium fluoride uptake and calcification at all sites—a finding that is in line with observations in a previous investigation by our group analyzing 18F-sodium fluoride uptake in various arterial segments, which found coincidence of tracer accumulation and calcification in 88% of lesions (18).
In the present study, 18F-sodium fluoride PET/CT identified plaques with continuing calcification, which might represent stable, static stages of atherosclerotic disease. The intensity of radiotracer uptake correlated with the calcified lesion thickness and the grading score as determined by the circumferential extent of calcified plaque. Although one may hypothesize that continuing mineral deposition is associated with growing calcifications and plaque growth per se, further prospective investigations are needed to determine whether, by correctly identifying those atherosclerotic lesions with increasing luminal stenosis, 18F-sodium fluoride uptake can eventually be used to target therapeutic interventions.
Molecular Background
Vascular calcification may arise as a result of both active and passive mechanisms. Passive mineral deposition may occur in areas of advanced tissue degeneration or necrosis within the arterial wall, which are frequent in advanced atherosclerotic plaque (5,26). Calcium physiochemically precipitates when local ion concentrations exceed the salt solubility threshold (27). This mainly acellular extracellular process is associated with cell fragments from foam cells and cholesterol crystals, which can serve as a crystallization nidus (5,27). Moreover, there is accumulating evidence that arterial calcification is an active and regulated process analogous to bone formation (5). That model is supported by histologic findings of ectopically formed bone, the presence of osteoblast- and osteoclastlike cells, and the secretion of numerous bone-related peptides in calcified atherosclerotic lesions (26,28–31). Therefore, 18F-sodium fluoride depicts pathophysiologic processes different from those depicted by 18F-FDG or choline compounds, which are assumed to visualize macrophage-mediated inflammation as measured by glucose metabolism or cell proliferation, respectively (6,32). It would be highly desirable to obtain a direct comparison of the relative accumulation of 18F-FDG, 18F-sodium fluoride, and choline derivatives within atheroma to assess the relative contribution of these tracers for the functional evaluation of atherosclerosis.
Limitations
The following limitations of the present investigation should be mentioned. First, because this study was performed on oncologic patients, the results might not be perfectly generalizable to other patient populations. However, most patients were referred for 18F-sodium fluoride imaging as part of the primary staging and have therefore been untreated. Factors supposed to possibly affect physiologic processes in the vessel wall were carefully excluded. Second, in all patients whole-body 18F-sodium fluoride PET/CT was performed using a routine protocol for oncologic imaging. The optimal circulation time for atherosclerotic plaque imaging with 18F-sodium fluoride might differ from the 1 h postinjection time point used for bone imaging. Dynamic and delayed data acquisition has been investigated for inflammation imaging with 18F-FDG, and although an acquisition beginning 90 or 120 min after injection might be superior for the assessment of 18F-FDG uptake in atherosclerotic lesions, the results so far have been somewhat inconclusive (22,33). However, there are currently no data available concerning dynamic or delayed imaging of arterial plaque using 18F-sodium fluoride. Finally, partial-volume effects might cause underestimation of tracer accumulation. Although that limitation applies to all PET studies analyzing vascular tracer uptake, partial-volume correction algorithms might be applied in future studies to reduce the impact of this error.
CONCLUSION
Carotid 18F-sodium fluoride uptake is a surrogate measure of carotid mineral deposition, correlates with cardiovascular risk factors, and is more frequent in patients with a high-risk profile for atherothrombotic events but demonstrates a weaker correlation with risk factors than does calcified plaque burden. 18F-sodium fluoride uptake may quantify continuing mineral deposition in carotid plaque, suggesting a potential role of this tracer for imaging and characterization of atherosclerotic plaque in the carotid arteries.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication July 12, 2010.
- Accepted for publication December 8, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Exploring Vessel Wall Biology In Vivo by Ultrasensitive Total-Body PET
- Three-Hour Delayed Imaging Improves Assessment of Coronary 18F-Sodium Fluoride PET
- Imaging Cardiovascular Calcification
- Clinical Molecular Imaging of Chemokine Receptor CXCR4 Expression in Atherosclerotic Plaque Using 68Ga-Pentixafor PET: Correlation with Cardiovascular Risk Factors and Calcified Plaque Burden
- Coronary Artery Calcification: From Mechanism to Molecular Imaging
- Evaluation of 68Ga-Glutamate Carboxypeptidase II Ligand Positron Emission Tomography for Clinical Molecular Imaging of Atherosclerotic Plaque Neovascularization
- Impact of Personal Characteristics and Technical Factors on Quantification of Sodium 18F-Fluoride Uptake in Human Arteries: Prospective Evaluation of Healthy Subjects
- 18F-NaF Uptake by Atherosclerotic Plaque on PET/CT Imaging: Inverse Correlation Between Calcification Density and Mineral Metabolic Activity
- Molecular imaging of atherosclerosis: clinical state-of-the-art
- 18F-Sodium Fluoride Uptake Is a Marker of Active Calcification and Disease Progression in Patients With Aortic Stenosis
- The Advancing Clinical Impact of Molecular Imaging in CVD
- Coronary Arterial 18F-Sodium Fluoride Uptake: A Novel Marker of Plaque Biology
- Assessment of Valvular Calcification and Inflammation by Positron Emission Tomography in Patients With Aortic Stenosis