


Abstract
The anti–human epidermal growth factor receptor 2 (HER2/neu) antibody trastuzumab is administered to patients with HER2/neu-overexpressing breast cancer. Whole-body noninvasive HER2/neu scintigraphy could help to assess and quantify the HER2/neu expression of all lesions, including nonaccessible metastases. The aims of this study were to develop clinical-grade radiolabeled trastuzumab for clinical HER2/neu immunoPET scintigraphy, to improve diagnostic imaging, to guide antibody-based therapy, and to support early antibody development. The PET radiopharmaceutical 89Zr-trastuzumab was compared with the SPECT tracer 111In-trastuzumab, which we have tested in the clinic already. Methods: Trastuzumab was labeled with 89Zr and (for comparison) with 111In. The minimal dose of trastuzumab required for optimal small-animal PET imaging and biodistribution was determined with human HER2/neu-positive or -negative tumor xenograft–bearing mice. Results: Trastuzumab was efficiently radiolabeled with 89Zr at a high radiochemical purity and specific activity. The antigen-binding capacity was preserved, and the radiopharmaceutical proved to be stable for up to 7 d in solvent and human serum. Of the tested protein doses, the minimal dose of trastuzumab (100 μg) proved to be optimal for imaging. The comparative biodistribution study showed a higher level of 89Zr-trastuzumab in HER2/neu-positive tumors than in HER2/neu-negative tumors, especially at day 6 (33.4 ± 7.6 [mean ± SEM] vs. 7.1 ± 0.7 percentage injected dose per gram of tissue). There were good correlations between the small-animal PET images and the biodistribution data and between 89Zr-trastuzumab and 111In-trastuzumab uptake in tumors (R2 = 0.972). Conclusion: Clinical-grade 89Zr-trastuzumab showed high and HER2/neu-specific tumor uptake at a good resolution.
Human epidermal growth factor receptor 2 (HER2/neu) belongs to the ErbB tyrosine kinase receptor family, which consists of 4 receptors, HER1–HER4. Members of the HER family have growth-stimulating activity and play an important role in the regulation of cell growth, survival, and differentiation (1). HER2/neu is genetically encoded by the HER2/neu proto-oncogene (HER2/neu or c-erbB-2). HER2/neu overexpression or amplification occurs in a wide range of human cancers, including breast (incidence, 20%−30%), colon, lung, and ovarian cancers (2,3). HER2/neu overexpression and amplification are associated with oncogenic transformation and, for breast cancer, with a poorer prognosis and more aggressive behavior of the tumor in the clinical setting when no HER2/neu-directed therapy is used (4–8). HER2/neu is therefore a relevant target for therapy in breast cancer in the metastatic setting as well as in the adjuvant setting (9). The monoclonal antibody (mAb) trastuzumab and the dual-target (epidermal growth factor receptor 1 and HER2/neu tyrosine kinase) inhibitor lapatinib are currently used in clinical practice to target HER2/neu.
To determine HER2/neu overexpression or amplification in tumor biopsies, a wide variety of techniques have been used. Of these, immunohistochemistry and fluorescence in situ hybridization are currently the standard techniques (10,11).
Although the HER2/neu status provides important information about the molecular composition of the tumor, it is generally only determined at diagnosis of the primary tumor. The HER2/neu tumor status can show a time-dependent change after therapy and can be different across tumor lesions in a single patient (12). Repeat biopsies would be an interesting way to analyze the HER2/neu tumor status during the course of the disease because of the possible time-dependent change in status after therapy. However, doctors and patients are frequently reluctant to use invasive techniques, particularly for poorly accessible lesions (13). Whole-body noninvasive HER2/neu scintigraphy could be a strategy for determining the HER2/neu expression of all lesions, including nonaccessible distant metastases, in a single scan and overcoming this problem. In addition, immunoscintigraphy could help to improve diagnostic imaging and to guide antibody-based therapy.
This situation has led to the development of 111In-radiolabeled trastuzumab. Using SPECT, we have shown HER2/neu-specific uptake of this radiopharmaceutical in xenograft-bearing animals (14) and HER2/neu-positive metastatic breast cancer patients (15). 111In-diethylaminetriaminepentaacetic acid (DTPA)-trastuzumab scintigraphy revealed new tumor lesions in 13 of 15 patients and was therefore considered to be of potential value for clinical staging (15).
In an attempt to further optimize HER2/neu imaging, PET was used instead of conventional nuclear medicine techniques because of its higher spatial resolution, better signal-to-noise ratio, and straightforward data quantification.
In line with our previous studies, our goal was to develop a radiopharmaceutical suitable for clinical HER2/neu immunoPET scintigraphy. The new PET radiopharmaceutical had to be at least comparable to 111In-DTPA-trastuzumab in uptake, biodistribution, and imaging quality. Here we describe the development and in vitro and in vivo characterization of 89Zr-radiolabeled trastuzumab and a comparison of 89Zr-trastuzumab with 111In-trastuzumab.
MATERIALS AND METHODS
The trastuzumab conjugation and labeling procedures described here were performed under good manufacturing practice (GMP) conditions at our manufacturing licensed department of nuclear medicine and molecular imaging. Materials and solvents for the labeling procedure were sterile and endotoxin and metal free (except for the Vivaspin-2 filters [see next paragraph]). Protein concentration, endotoxin content, and sterility were measured. Both radiopharmaceuticals met European Pharmacopoeia and U.S. Pharmacopoeia requirements for sterile radiopharmaceuticals. All chemicals used for the study complied with European Pharmacopoeia or U.S. Pharmacopoeia specifications.
89Zr-Trastuzumab Production
In the first step, reconstituted trastuzumab (21 mg/mL; Roche) was purified with water for injection from excipients by ultrafiltration. Vivaspin-2 filters (30 kDa; Sartorius AG; 2 × 10 min at 2,684g) were used for all ultrafiltration purification steps. Purified trastuzumab was conjugated essentially as described by Verel et al. (16). In short, trastuzumab was diluted with 0.1 M Na2CO3 (pH 9.5; Bufa) and allowed to react with a 2-fold molar excess of a tetrafluorophenol-N-succinyldesferal-Fe (TFP-N-SucDf-Fe; VU University Medical Center) active ester. After 30 min, the pH was adjusted to 4.0 with sulfuric acid (Merck). The number of desferal ligands per antibody was assessed by size exclusion high-performance liquid chromatography (SE-HPLC) at 430 nm, and ethylenediaminetetraacetic acid (Merck) was added to remove Fe(III). The premodified antibody was purified by ultrafiltration with 0.9% sterile NaCl (B. Braun) and immediately used or stored at −80°C. Frozen N-SucDf-trastuzumab proved to be stable for at least 12 mo. In the second step, the conjugate was radiolabeled with clinical-grade 89Zr-oxalate (99.99% pure; BV Cyclotron, VU University Medical Center) in 1 M N-2-hydroxyethylpiperazine-N′-2-ethanesulfonic acid (HEPES, pH 6.8; Invitrogen) and purified by ultrafiltration with 0.9% NaCl:0.5% gentisic acid (Merck) to obtain a radiochemical purity of at least 95%. 89Zr-N-SucDf-trastuzumab is hereafter referred to as 89Zr-trastuzumab.
111In-Trastuzumab Production
Conjugation and radiolabeling were performed as described by Ruegg et al. (17). First, purified trastuzumab was conjugated in 0.1 M NaHCO3 (pH 8.4; Merck) with a 25-fold molar excess of the bifunctional chelate 2-(4-isothiocyanatobenzyl)-DTPA (p-SCN-Bn-DTPA; Macrocyclics). Unbound conjugate was removed by ultrafiltration with 0.15 M acetate buffer (pH 5.5, freshly prepared from ammonia and acetic acid, both obtained from Merck). The conjugated antibody was immediately used or stored at −80°C. Frozen p-SCN-Bn-DTPA-trastuzumab proved to be stable for at least 12 mo. Conjugated trastuzumab was radiolabeled with 111InCl3 (370 MBq/mL, >1.85 GBq/mg, 99.9% radionuclidic purity; Covidien) in 0.15 M acetate buffer (pH 5.5), and the number of DTPA ligands per trastuzumab molecule was established as described by Hnatowich et al. (18). To obtain a radiochemical purity of at least 95%, we purified 111In-p-SCN-Bn-DTPA-trastuzumab by ultrafiltration with 0.15 M acetate buffer. 111In-p-SCN-Bn-DTPA-trastuzumab is hereafter referred to as 111In-trastuzumab.
Quality Control of Premodified and Radiolabeled Trastuzumab
Radiochemical purity and stability were confirmed by SE-HPLC and by 30% trichloroacetic acid (TCA; Department of Hospital and Clinical Pharmacy, University Medical Center Groningen [UMCG]) precipitation for 89Zr-trastuzumab or thin-layer chromatography (TLC) for 111In-trastuzumab.
The Waters SE-HPLC system was equipped with a dual-wavelength absorbance detector, an in-line radioactivity detector, and a size exclusion column (Superdex 200 10/300 GL; GE Healthcare). Sodium phosphate buffer (0.025 M Na2HPO4·2H2O and NaH2PO4·H2O, both obtained from Sigma-Aldrich) was used as a mobile phase. The retention time for trastuzumab was approximately 17 min; 89Zr-N-SucDf, 111In-DTPA, and low-molecular-weight impurities eluted at 28 min (at a flow of 0.7 mL/min).
TCA precipitation was performed with phosphate-buffered saline, 0.5% human serum albumin (Sanquin), and 30% TCA. Radioactivity was determined with a calibrated well-type γ-counter (LKB 1282; Compugamma).
TLC was performed with silica-impregnated glass fiber sheets (TLC-SG, 2.5 × 10 cm; Pall Gelman Sciences), and 0.1 M citrate buffer (pH 6.0) was used for elution. Radioactivity was determined with an instant chromatography scanner (VCS-IOI; Veenstra Instruments) equipped with an NaI crystal.
Immunoreactive Fraction
Flow cytometry was performed with trastuzumab and a fluorescein isothiocyanate–labeled antihuman antibody (F5016; Sigma-Aldrich) to confirm HER2/neu expression as described earlier (19). The in vitro binding characteristics (immunoreactive fraction) of radiolabeled trastuzumab were determined in a cell-binding assay, essentially as described by Lindmo et al. (20), with SKOV3 (a naturally HER2/neu-overexpressing human ovarian cancer cell line) and GLC4 (a HER2/neu-negative human small cell lung cancer cell line). SKOV3 cells were cultured in Dulbecco's modified Eagle's medium with a high glucose concentration, and GLC4 cells were cultured in RPMI 1640 medium, both with 10% fetal calf serum. SKOV3 cells were harvested with trypsin; GLC4 cells grow in suspension.
For the antigen-binding experiment, cells were collected, and a fixed amount of radioactivity (10,000 cpm) was added to an increasing number of cells. After 1 h of incubation, the cell suspensions were centrifuged and repeatedly washed with phosphate-buffered saline containing 0.5% human serum albumin to determine the radioactivity uptake. The specific binding was calculated as the ratio of cell-bound radioactivity to the total amount of applied radioactivity and was corrected for nonspecific binding, as determined with a 500-fold excess of nonradioactive trastuzumab. All binding assays were performed in triplicate.
Stability Testing of Radiolabeled Compounds
The stability of the labeled compounds was evaluated at 4°C in solution (0.9% NaCl:0.5% gentisic acid or ammonium acetate [pH 5.5] for 89Zr-trastuzumab and 111In-trastuzumab, respectively) and in human serum at 37°C for 7 d. The radiochemical purity and the immunoreactive fraction were determined by SE-HPLC, TLC, or TCA precipitation and the assay described by Lindmo et al. (20).
In Vivo Biodistribution Studies
An animal study was conducted to assess the minimal dose of trastuzumab required for optimal imaging, to determine HER2/neu-specific tumor uptake, and to compare 89Zr-trastuzumab and 111In-trastuzumab biodistributions in mice bearing human ovarian carcinoma SKOV3 (HER2/neu-positive) or human small cell lung carcinoma GLC4 (HER2/neu-negative) xenografts. Male athymic mice (Hsd:Athymic Nude/nu) were obtained from Harlan. All animal studies were conducted in accordance with the Dutch Law on Animal Experimentation and were approved by the local ethics committee. At 4–6 wk of age (weight, 30 g), the mice were injected subcutaneously with 106 tumor cells (mixed with equal amounts of Matrigel [Becton Dickinson]). Approximately 2 wk after inoculation, animals were used for the in vivo studies (tumor diameters, 5–8 mm).
Protein Dose Escalation Study
Before a larger biodistribution study was carried out, a protein dose escalation study was performed to determine the minimal dose of trastuzumab required for optimal imaging. SKOV3 xenograft–bearing nude mice (5 per group) were injected intravenously in the penile vein with 5 MBq of 89Zr-trastuzumab, corresponding to a total amount of 100, 250, or 500 μg of trastuzumab per animal. At 1, 3, and 6 d after injection, animals were anesthetized with 2% isoflurane and underwent small-animal PET imaging (Focus 220 microPET scanner; Siemens) in the transaxial position for 30–60 min. A transmission scan with a 57Co point source was used for scatter and attenuation corrections. Images were reconstructed in the 2-dimensional ordered-subset expectation maximization mode with 4 iterations by use of microPET manager (Siemens). The voxel size of the images was 0.47 × 0.47 × 0.82 mm, and a gaussian filter of 1.2 mm was applied to the images after reconstruction.
In vivo quantification was performed with AMIDE Medical Image Data Examiner software (version 0.9.1; Stanford University) (21).
The accumulation of radioactivity in tumors and a representative subset of the tumor volume were determined by drawing an 80% isodensity contour volume of interest around the tumor on the small-animal PET images as previously described (22). The total injected dose was calculated by decay correction of the activity present in the animal at 24 h after injection, at which time the clearance of the injected antibodies was considered to be almost negligible, as described earlier (23). The data are presented as the percentage injected dose per gram (%ID/g) of tissue, with the assumption of a tissue density of 1 g/cm3.
After the scan on day 6, the animals were sacrificed and dissected to confirm the noninvasive small-animal PET data. The radioactivity in dissected tissues was counted in a well-type γ-counter. All data were corrected for physical decay and compared with known standards. Tissue radioactivity was expressed as %ID/g and as a ratio of tumor to normal tissue (T/NT ratio).
Comparative Biodistribution Study of 89Zr-Trastuzumab and 111In-Trastuzumab
Once the minimal required trastuzumab dose had been determined in the protein dose escalation study, a comparative biodistribution study was performed. The aims of this study were to validate HER2/neu-specific tumor uptake and to compare the tumor accumulation and organ biodistribution of 89Zr-trastuzumab with those of 111In-trastuzumab. Mice bearing SKOV3 (n = 5) or GLC4 (n = 4) xenografts were coinjected with 1:1 89Zr-trastuzumab and 111In-trastuzumab (100 μg of trastuzumab, 1 MBq each). The animals were sacrificed and dissected at days 1, 3, and 6, and the radioactivity in tissues was determined and expressed as %ID/g and as T/NT ratios.
Immunohistochemistry
Xenograft HER2/neu expression was confirmed by immunohistochemistry. Formalin-fixed, paraffin-embedded tumors were stained with antibodies against HER2/neu (HercepTest; DAKO). Immunohistochemical results were scored semiquantitatively in accordance with the guidelines developed by the American Society of Clinical Oncology and the College of American Pathologists for clinical testing. In short, a 4-tier system was used: 0 corresponded to no staining; 1+ corresponded to weak and incomplete staining; 2+ corresponded to weak to moderate complete staining; and 3+ corresponded to strong, complete circumferential, membranous staining (24). The slides were scored by a pathologist.
Statistical Analysis
Data are presented as mean ± SEM. Statistical analysis was performed with the nonparametric Mann–Whitney test (SPSS version 14.0; SPSS Inc.). P values of less than 0.05 were considered significant. The agreement between the quantified in vivo small-animal PET images and the ex vivo biodistribution data was estimated by Bland–Altman analysis (25).
RESULTS
Trastuzumab Conjugation, Radiolabeling, and Quality Control
Trastuzumab was premodified with either N-SucDf or p-SCN-Bn-DTPA. The number of chelating groups per antibody was estimated to be 1.3 for N-SucDf and 1.9 for p-SCN-Bn-DTPA. The radiolabeling efficiency for 89Zr-trastuzumab was 77.6% ± 3.9% (n = 3), and the radiochemical purity after ultrafiltration was 98.1% ± 1.1% (n = 3). The radiolabeling efficiency for 111In-trastuzumab was 89.3% ± 2.1% (n = 3), and the radiochemical purity was 97% ± 1% (n = 3). The obtained specific activities were 67.2 ± 2.4 MBq/mg (n = 3) for 89Zr-trastuzumab and 78.2 ± 3.1 MBq/mg (n = 3) for 111In-trastuzumab. SE-HPLC analysis (column recovery, >95%; data not shown) of both radiopharmaceuticals revealed no aggregates, fragments, or radioactive impurities. 89Zr-trastuzumab and 111In-trastuzumab proved to be sterile and endotoxin free.
Immunoreactive Fraction
Flow cytometry confirmed a high level of HER2/neu expression for SKOV3 (760 ± 59 events) and a low level of receptor expression for GLC4 (38 ± 1 events). The maintenance of the in vitro binding characteristics of 89Zr-trastuzumab and 111In-trastuzumab was determined with the cell-binding assay described by Lindmo et al. (20). The immunoreactive fraction of 89Zr-trastuzumab was 0.87 ± 0.06, and that of 111In-trastuzumab was 0.85 ± 0.11. Nonspecific cellular binding was less than 0.10 and was comparable to the binding of the radiopharmaceutical to GLC4.
Stability Testing of Radiolabeled Compounds
89Zr-trastuzumab appeared to be stable, with mean decreases in radiochemical purity of only 0.07% ± 0.03% in solvent at 4°C and 0.39% ± 0.02% in human serum at 37°C per day. The immunoreactive fraction was determined directly after labeling and decreased only marginally with storage in solvent at 4°C (from 0.87 to 0.85 ± 0.06) and in human serum at 37°C (from 0.87 to 0.78 ± 0.01) for up to 7 d.
111In-trastuzumab also appeared to be stable, with minimal decreases in protein-bound radioactivity of 0.09% ± 0.14% in solvent at 4°C and 0.39% ± 0.53% in human serum at 37°C per day. The immunoreactive fraction decreased only slightly with storage in solvent at 4°C (from 0.85 to 0.75 ± 0.04) and in human serum at 37°C (from 0.85 to 0.78 ± 0.08) after 7 d.
In Vivo Biodistribution Studies
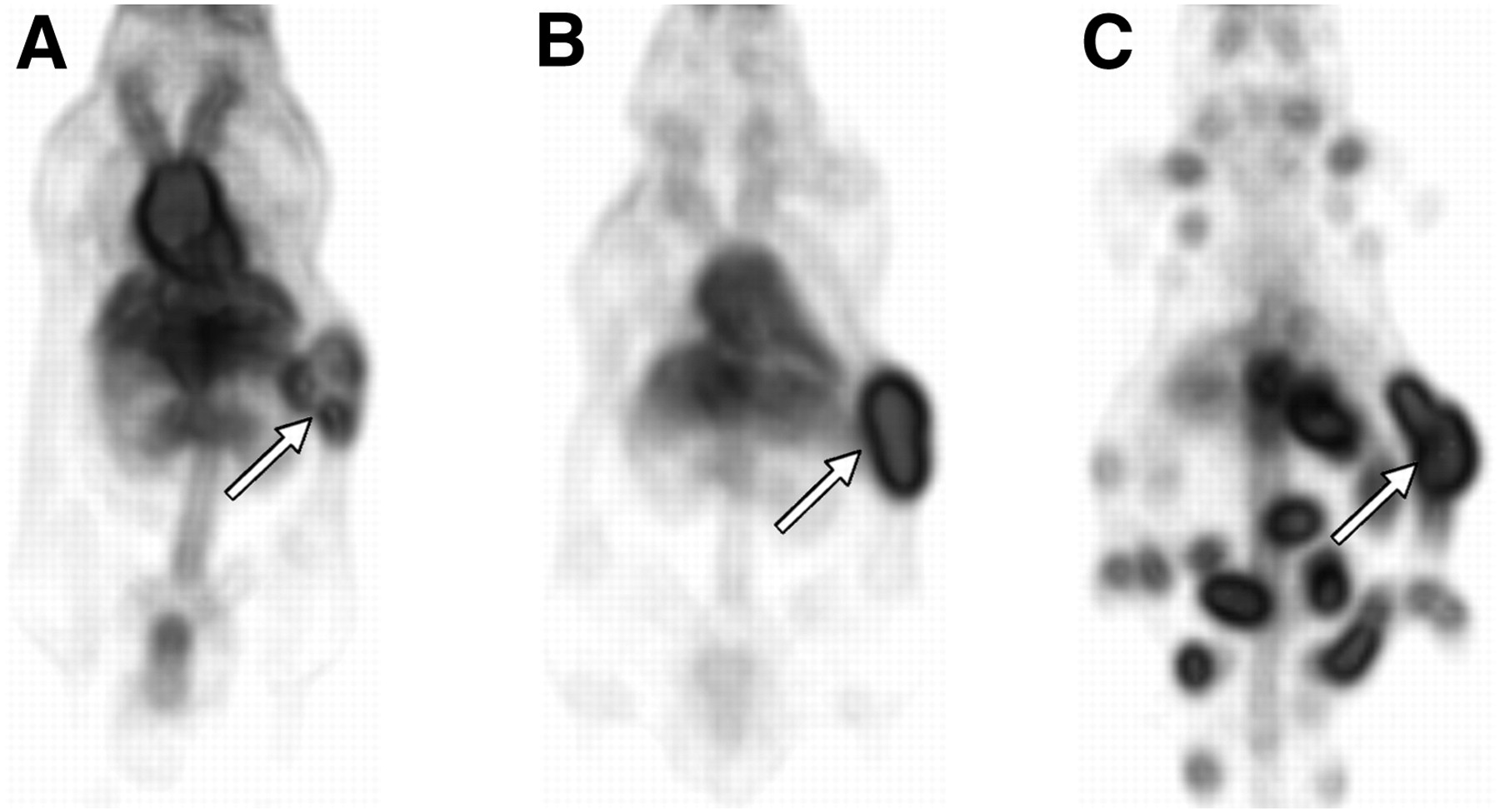
In the protein dose escalation study, small-animal PET imaging revealed excellent tumor uptake in all 15 mice. Tumor uptake could already be demonstrated as early as 6 h after 89Zr-trastuzumab injection, although blood-pool activity was dominant at this time point (Fig. 1A). From day 1 to day 6, tumor uptake significantly increased, whereas blood-pool activity decreased (Fig. 1B). Interestingly, HER2/neu-positive metastases, which could be detected easily (Fig. 1C), spontaneously developed in one mouse, even though some metastases were as small as the spatial resolution of the small-animal PET camera (as confirmed by dissection of the animal and pathology). Ex vivo biodistribution data from the protein dose escalation study revealed high tumor uptake (30–33 %ID/g) (Fig. 2) and excellent tumor-to-blood (T/B) and T/NT ratios 6 d after injection. The maximal T/B ratio for animals that received 100 μg of protein was 7.6. Only the liver and the spleen showed slightly higher radioactivity uptake than other organs with a large blood supply; the maximal uptake in the liver and the spleen was 9 %ID/g. The accumulation of radioactivity in the muscle and the brain was negligible (<1 %ID/g), resulting in high T/NT ratios.
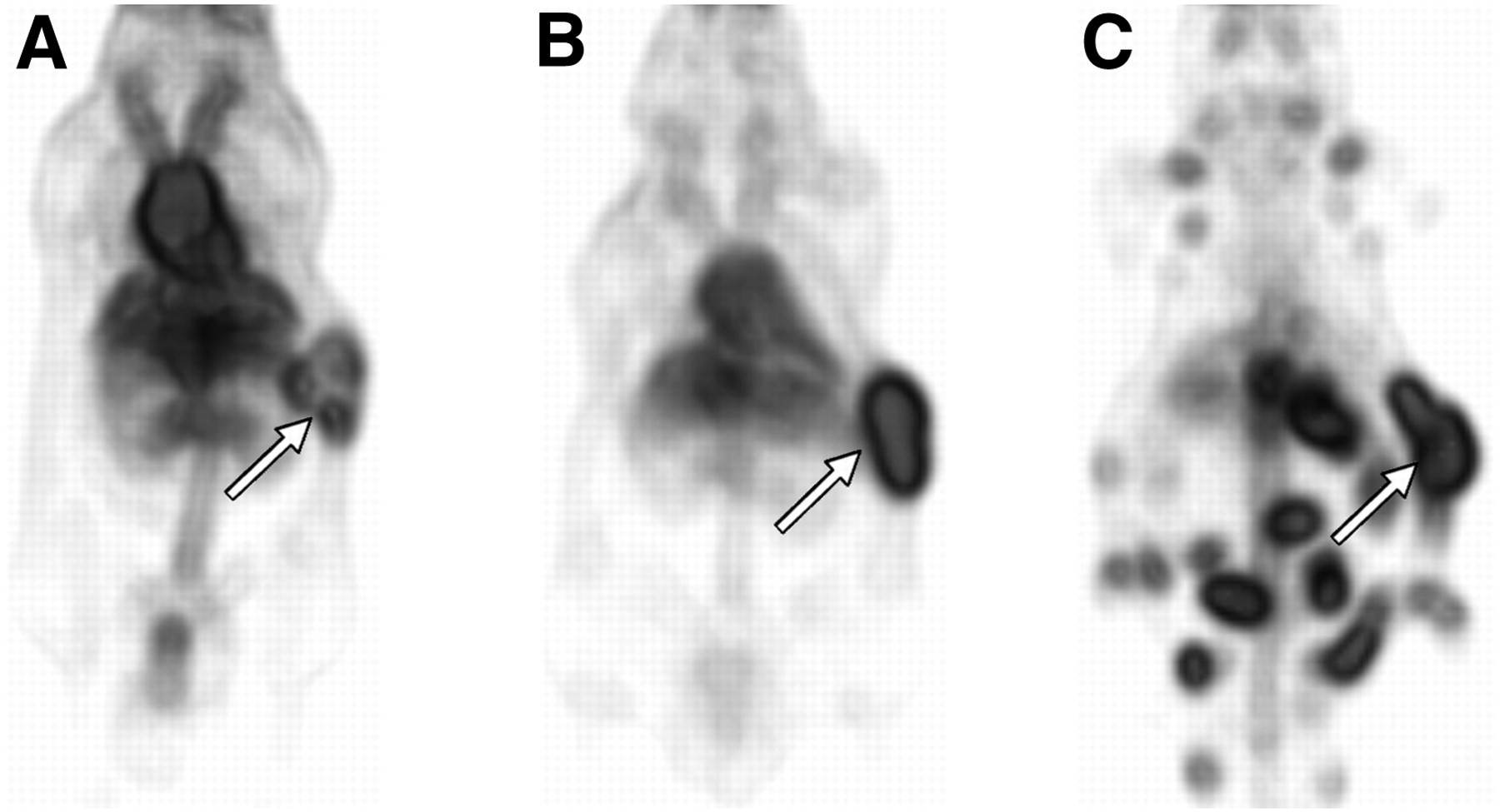
Examples of noninvasive small-animal PET images (dorsal presentation). 89Zr-trastuzumab (5 MBq per mouse) uptake in human SKOV-3 xenografts in 3 mice at 6 h (A), day 1 (B), and day 6 (C, metastasized tumor) after injection is shown. Primary tumors are indicated by arrows.

Ex vivo tissue uptake of 100 (black), 250 (light gray), or 500 (dark gray) μg of protein 6 d after intravenous injection of 5 MBq of 89Zr-trastuzumab. Data are presented as %ID/g of tissue (mean ± SEM for 5 mice per group). Significance is indicated (*P < 0.05; **P < 0.01).
As shown in Figure 2, there appeared to be a statistically significant difference in radioactivity uptake in the blood and several tissues with a large blood supply (including the heart, kidneys, pancreas, spleen, and muscle). Tumor uptake was not significantly different at the 3 trastuzumab doses (P = 0.75). The T/B ratios decreased with increasing doses of trastuzumab (7.3, 5.3, and 4.7, respectively) but did not differ significantly at the 3 applied doses (P ≥ 0.47). The tumor-to-liver (T/L) ratios varied slightly but not significantly at the 3 doses (being 3.3, 4.6, and 4.0, respectively; P ≥ 0.18).
Overall, of the tested protein doses, the minimal dose of 100 μg of trastuzumab per animal (approximately 4 mg/kg) was considered to be optimal for imaging because it resulted in excellent tumor uptake and the highest T/B ratios and was therefore used in the comparative biodistribution study of 111In-trastuzumab and 89Zr-trastuzumab.
No apoptosis was noted during microscopic evaluation of the tumor tissue at a protein dose of 100–500 μg.
According to the Bland–Altman analysis, all data were well within the limits of agreement and evenly distributed along the mean difference, indicating similarities between the in vivo quantified small-animal PET data and the ex vivo biodistribution data.
The comparative biodistribution study data for 89Zr-trastuzumab and 111In-trastuzumab in HER2/neu-positive SKOV3 tumor–bearing mice and HER2/neu-negative GLC4 tumor–bearing mice are shown in Figure 3. For clarity, only days 1 and 6 and the key organs are shown.
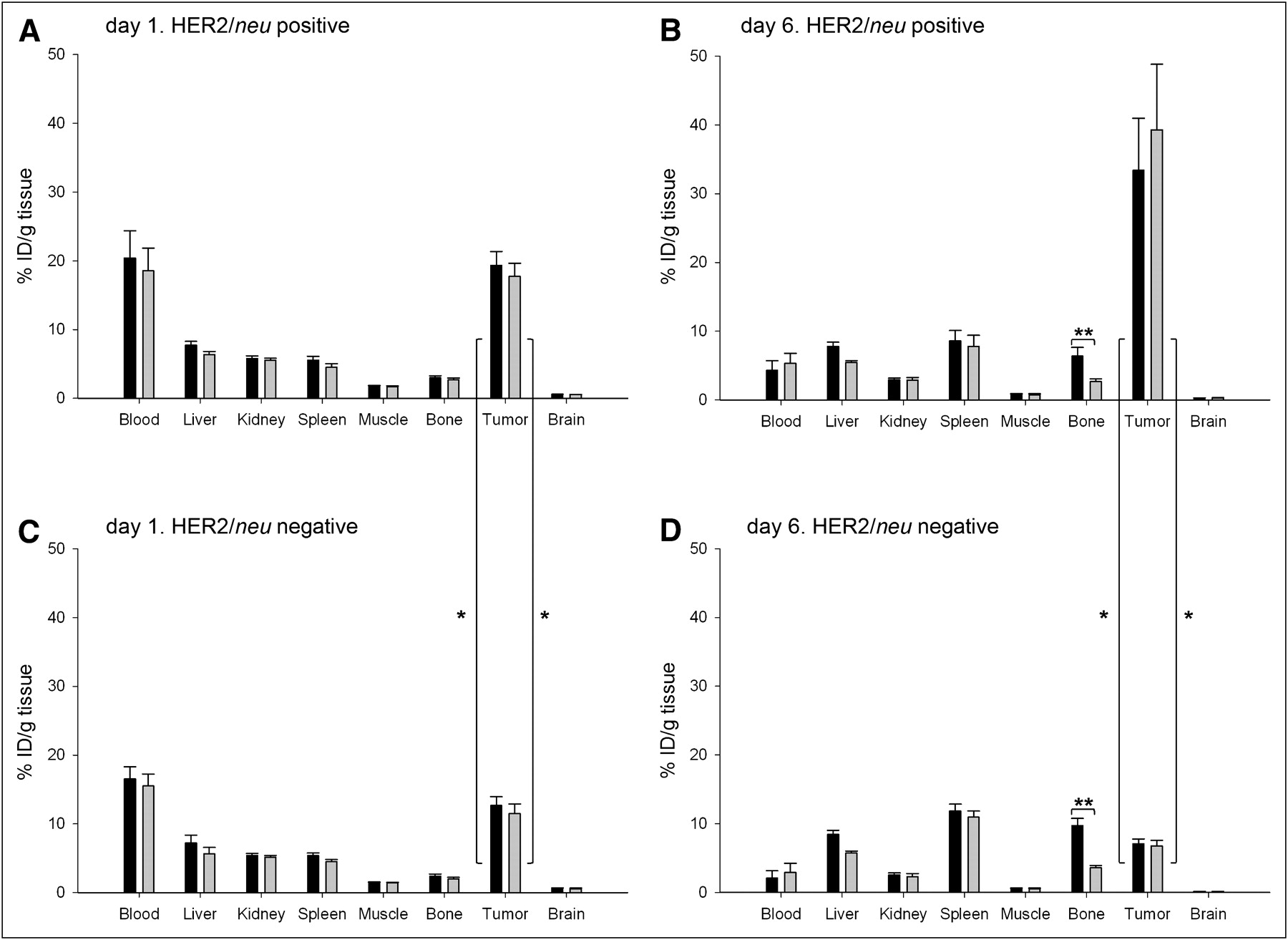
Ex vivo tissue uptake after intravenous coinjection of 89Zr-trastuzumab (black) and 111In-trastuzumab (gray) (100 μg of trastuzumab, 2 MBq in total) at day 1 (A and C) and day 6 (B and D). Data are presented as %ID/g of tissue (mean ± SEM for 5 HER2/neu-positive mice and for 4 HER2/neu-negative mice per group). Significance is indicated (*P < 0.05; **P < 0.01).
The biodistribution data revealed significantly higher uptake of radioactivity in the HER2/neu-positive tumor than in the HER2/neu-negative tumor. Uptake in the HER2/neu-positive tumor could already be demonstrated at day 1 and proved to be similar for 89Zr-trastuzumab and 111In-trastuzumab (19.3 ± 2.0 %ID/g for 89Zr-trastuzumab and 17.7 ± 1.9 %ID/g for 111In-trastuzumab; P = 0.47). The tumor uptake increased even further to day 6 (33.4 ± 7.6 %ID/g for 89Zr-trastuzumab and 39.3 ± 9.5 %ID/g for 111In-trastuzumab; P = 0.47). In contrast, the uptake of radioactivity in the HER2/neu-negative tumor was lower. At day 1, 89Zr-trastuzumab had accumulated to 15.7 ± 1.3 %ID/g in the HER2/neu-negative tumor, and 111In-trastuzumab had accumulated to 15.0 ± 1.4 %ID/g; there was no significant difference between 89Zr-trastuzumab tumor uptake and 111In-trastuzumab tumor uptake (P = 0.56). At day 6, the accumulation had decreased to 7.1 ± 0.7 %ID/g for 89Zr-trastuzumab and 6.8 ± 0.8 %ID/g for 111In-trastuzumab (P = 0.56).
At day 1, however, there was already a significant difference in tumor uptake in the HER2/neu-positive tumor and the HER2/neu-negative tumor (P = 0.027 for 89Zr-trastuzumab and P = 0.049 for 111In-trastuzumab). At day 6, the radiopharmaceutical uptake in the HER2/neu-negative tumor was significantly lower than that in the HER2/neu-positive tumor (P = 0.014 for both 89Zr-trastuzumab and 111In-trastuzumab).
Meanwhile, the percentage of radiolabeled trastuzumab circulating in the blood in mice with HER2/neu-positive tumors declined from 20.4 %ID/g for 89Zr-trastuzumab and 18.6 %ID/g for 111In-trastuzumab at day 1 to 4.3 and 5.3 %ID/g, respectively, at day 6. Because of the high tumor uptake and low tissue uptake, excellent T/B and T/NT ratios were achieved at day 6. Liver uptake was limited, and T/L ratios for both radiopharmaceuticals (5.2 for 89Zr-trastuzumab and 7.3 for 111In-trastuzumab) were high and comparable to the data from the protein dose escalation study.
The data obtained in the comparative biodistribution study of 89Zr-trastuzumab and 111In-trastuzumab confirmed the data from the noninvasive small-animal PET images and were similar to the data from the protein dose escalation study at day 6.
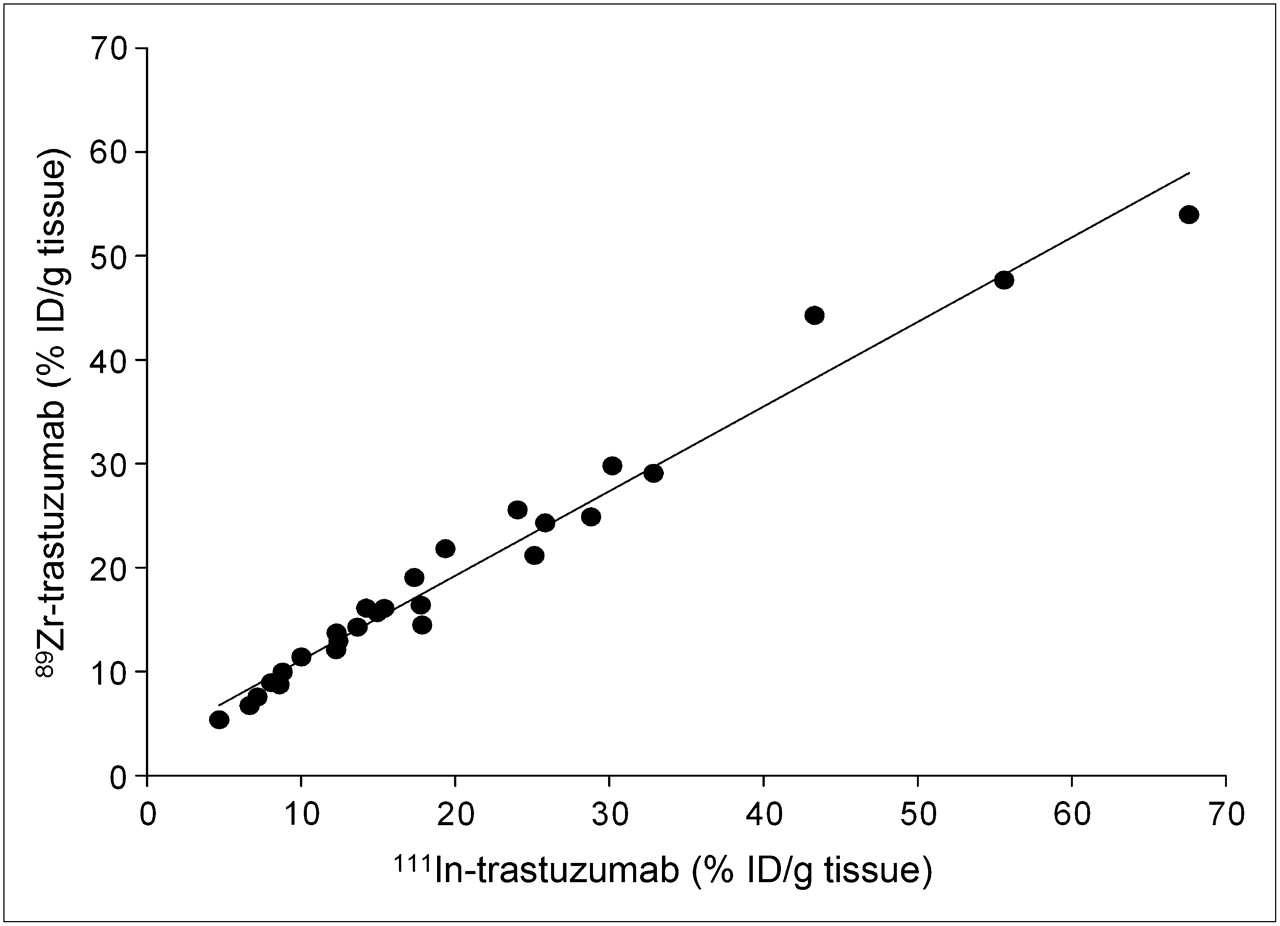
Overall, there was no significant difference in uptake. In contrast, there was a good correlation (R2 = 0.972) between 89Zr-trastuzumab uptake and 111In-trastuzumab uptake in tumors (Fig. 4).
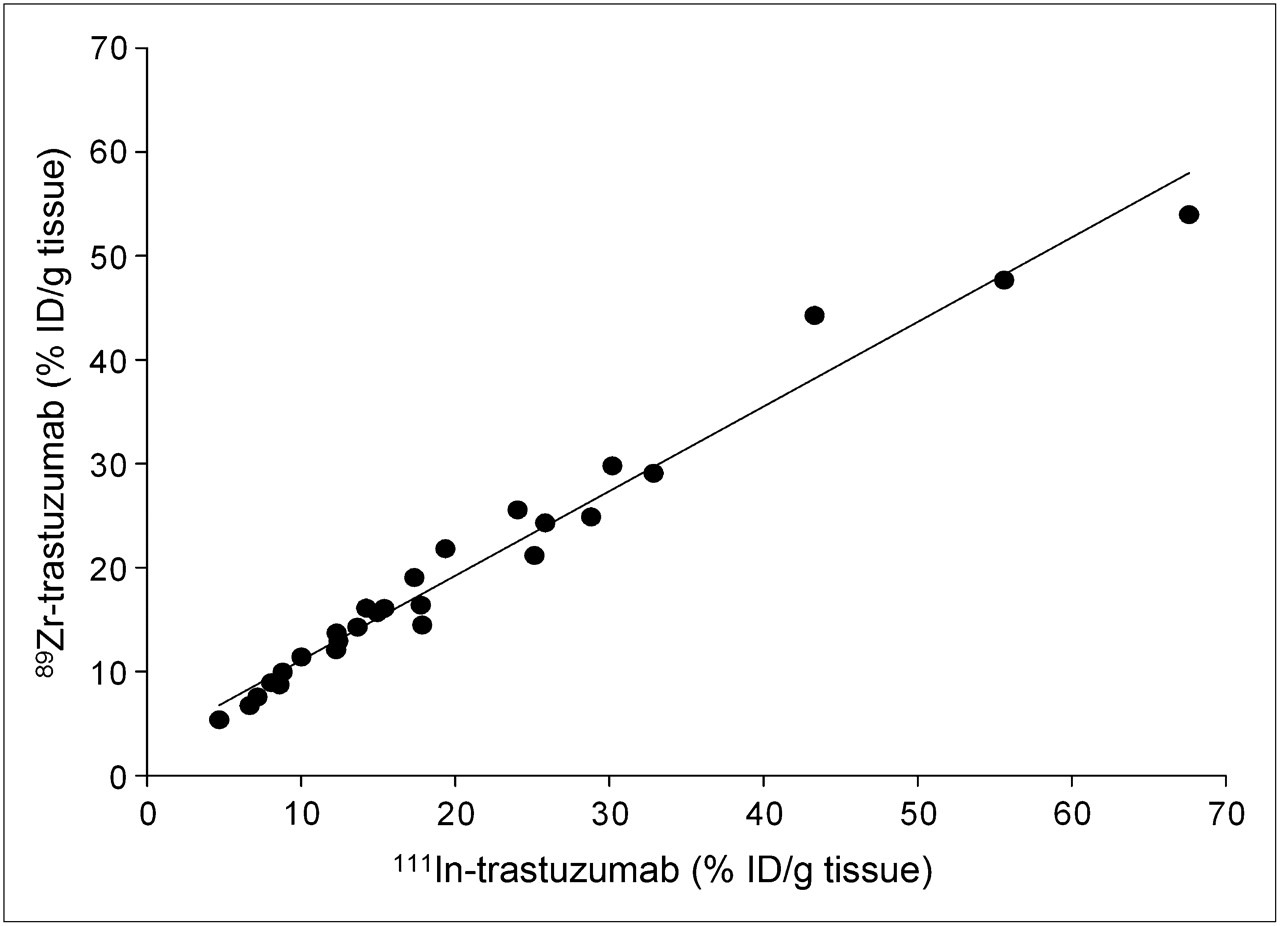
Overall correlation of ex vivo tumor uptake of 89Zr and 111In after intravenous coinjection of 89Zr-trastuzumab and 111In-trastuzumab (100 μg of trastuzumab, 2 MBq in total) at days 1, 3, and 6. Correlation coefficient (R2) was 0.972.
Immunohistochemistry
Immunohistochemistry confirmed a high (3+) level of HER2/neu expression for the HER2/neu-positive SKOV3 tumor and a low (0–1+) level of receptor expression for the HER2/neu-negative GLC4 tumor (data not shown).
DISCUSSION
The present study showed that 89Zr-trastuzumab could be radiolabeled efficiently, with preservation of the antigen-binding capacity, and was stable for up to 7 d. A high level of HER2/neu-driven tumor uptake of radiolabeled trastuzumab at excellent T/NT ratios was observed. 89Zr-trastuzumab showed a biodistribution similar to that of the control, 111In-trastuzumab, at a spatial resolution unapproachable by SPECT. Produced according to GMP requirements, this radiopharmaceutical is applicable for clinical use.
The tumor uptake of 89Zr-trastuzumab at 100 μg was similar to that at 500 μg, but the T/L ratio at 100 μg was lower than that at 500 μg. This result may have been attributable to faster blood clearance, as animal studies have shown the rapid clearance of human IgG in nude mice with low endogenous IgG titers (26)—a phenomenon restricted to the nude-mouse model. The species-specific IgG pharmacokinetics hamper the prediction of the trastuzumab dose required for optimal imaging in humans. Phenomena such as differences in IgG clearance and metabolism, shedding of HER2/neu, and tumor load will influence pharmacokinetics in humans and imaging characteristics. A dose escalation study in patients is therefore mandatory.
Compared with other radiopharmaceuticals developed for HER2/neu immunoPET, 124I-ICR12 demonstrated reasonable and specific uptake (12 %ID/g at 120 h) in athymic mice bearing human HER2/neu–overexpressing breast carcinoma xenografts (27). Tumor uptake of ICR12 was further increased, to 20 %ID/g, with residualizing isotopes (28,29). Similar to what we observed in the present study, tumor uptake of ICR12 was not influenced by the protein dose, but the T/B ratio decreased with an increasing amount of protein (30). With the murine predecessor of trastuzumab (4D5), maximal tumor uptake was 35% (31,32), comparable to what we found.
89Zr is a relatively new, yet promising, long-lived PET isotope. 89Zr was considered to be a suitable isotope because it has a sufficiently long physical half-life (3.3 d) to match the relatively slow pharmacokinetics of an intact antibody, is well suited to being combined with an internalizing antibody, and can be used clinically (33). Perk et al. (34) showed that 89Zr-radiolabeled anti–epidermal growth factor receptor antibody cetuximab could accurately predict 177Lu and 88Y (as a substitute for 90Y) biodistributions. 89Zr-cetuximab therefore has the potential to be used as a scouting procedure in preparation for radioimmunotherapy, for confirming tumor targeting, and for estimating radiation dose delivery to both tumor and normal tissues (34). Using 89Zr-radiolabeled bevacizumab (an anti–vascular endothelial growth factor mAb), our group reported specific, vascular endothelial growth factor–related tumor uptake at 7 d after injection in a preclinical study (23).
In the first clinical study with a 89Zr-radiolabeled mAb (89Zr-U36, a CD44v6 domain–binding chimeric IgG) immunoPET performed at least as well as CT or MRI for the detection of lymph node metastases in patients with squamous cell carcinoma of the head and neck (35). 89Zr-oxalate produced according to GMP has been commercially available since the end of 2008.
Clinical HER2/neu immunoscintigraphy has been performed with 99mTc-ICR12, 111In-trastuzumab, and 89Zr-trastuzumab. In the early 1990s, the rat antibody 99mTc-ICR12 was administered to 8 breast cancer patients. Tomographic images were obtained at 24 h. The study indicated that 99mTc-ICR12 could be used for the imaging of HER2/neu overexpression (29), but no further clinical results with this rodent antibody have been published. In a preliminary report, Behr et al. suggested that 111In-trastuzumab could predict the therapeutic efficacy of trastuzumab in 20 patients with HER2/neu-overexpressing metastatic breast cancer (36). In a study of HER2-positive metastatic breast cancer patients, our group reported that 111In-trastuzumab scintigraphy revealed new tumor lesions in 13 of 15 patients and was therefore suggested to be of value for the clinical staging of HER2/neu-positive metastatic breast cancer (15). Unfortunately, no clinical studies of HER2/neu targeting of smaller proteins have been published.
HER2/neu immunoscintigraphy has many potential clinical applications (33), including improved diagnosis, guidance for targeted therapy (37,38), and early drug development. Therefore, larger studies to prove whether this imaging technique can indeed affect clinical practice are of major interest (12).
Generally, large intact antibodies penetrate solid tumor tissue more slowly but constantly, ultimately resulting in a higher level of tumor accumulation, whereas small proteins (mAb fragments, minibodies, single-chain variable antibody fragments, diabodies, or affibodies) penetrate tumor tissue more swiftly but show less tumor uptake because of their rapid blood clearance (12). With 68Ga-trastuzumab F(ab′)2 fragments, relatively good tumor uptake was obtained (12 %ID/g), and the loss and recovery of HER2/neu induced by the HSP90 inhibitor 17-AAG was quantified (37). In a follow-up study, a reduction in 68Ga-F(ab′)2-trastuzumab tumor uptake predicted 17-AAG–induced tumor growth inhibition earlier than a reduction in 18F-FDG tumor uptake (38). Divalent single-chain variable antibody fragment (scFv) tumor accumulation is limited to 2–3 %ID/g (T/B ratio, 3–29); diabody and minibody tumor accumulation is approximately 6 %ID/g (T/B ratio, 3–13) (12). Affibody experiments have shown promising results. With affibodies, excellent tumor uptake has been demonstrated (4.4−23 %ID/g), especially when the size of the molecule is considered, and high T/B ratios (7–190) have been observed (12).
We have chosen to use the radiolabeled approved intact antibody trastuzumab instead of smaller proteins to determine HER2/neu expression. The choice of a radiopharmaceutical for HER2/neu imaging should depend on the question to be answered. If only receptor expression is relevant for diagnostic purposes, then imaging can be performed with small proteins, allowing patients to be diagnosed in a single day. If evaluation (and response prediction) of trastuzumab therapy are desired, then radiolabeled intact antibodies, which most likely mimic drug behavior more accurately, are preferable.
89Zr-trastuzumab seems to be a valuable addition to the arsenal of radiolabeled intact antibodies that can be used in patients. It has a higher spatial resolution and a better signal-to-noise ratio than 111In-trastuzumab, and data quantification is more straightforward. The preliminary results obtained with 89Zr-trastuzumab immunoPET in HER2-positive breast cancer patients indicated good radiopharmaceutical uptake by the tumor and excellent spatial resolution (39).
CONCLUSION
The present study showed that clinical-grade 89Zr-trastuzumab can be manufactured with high stability and maintenance of antigen binding. The first immunoPET radiopharmaceutical displayed excellent tumor accumulation, with high T/NT ratios and a biodistribution similar to that of 111In-trastuzumab (which was previously used successfully in a clinical study of metastatic breast cancer patients) at a significantly higher spatial resolution and with better T/NT ratios. These data validate this radiopharmaceutical for further clinical testing.
Acknowledgments
The authors thank Sander de Korte and Wouter Nagengast for assistance during the in vivo biodistribution study and Wim Sluiter for statistical advice. This study was supported by grant 2007-3739 from the Dutch Cancer Society.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 19, 2008.
- Accepted for publication March 4, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Whole-Body HER2 Heterogeneity Identified on HER2 PET in HER2-Negative, -Low, and -Positive Metastatic Breast Cancer
- Development of 89Zr-anti-CD103 PET imaging for non-invasive assessment of cancer reactive T cell infiltration
- 89Zr-pembrolizumab biodistribution is influenced by PD-1-mediated uptake in lymphoid organs
- Development and Evaluation of Interleukin-2-Derived Radiotracers for PET Imaging of T Cells in Mice
- Development of 64Cu-NOTA-Trastuzumab for HER2 Targeting: A Radiopharmaceutical with Improved Pharmacokinetics for Human Studies
- PET Imaging of Receptor Tyrosine Kinases in Cancer
- Preclinical and clinical applications of specific molecular imaging for HER2-positive breast cancer
- Preclinical Efficacy of an Antibody-Drug Conjugate Targeting Mesothelin Correlates with Quantitative 89Zr-ImmunoPET
- Nuclear Medicine in Cancer Theranostics: Beyond the Target
- Molecular Imaging and Quantitation of EphA2 Expression in Xenograft Models with 89Zr-DS-8895a
- Biodistribution and PET Imaging of Labeled Bispecific T Cell-Engaging Antibody Targeting EpCAM
- Microfluidic Preparation of a 89Zr-Labeled Trastuzumab Single-Patient Dose
- Molecular Imaging of Biomarkers in Breast Cancer
- Noninvasive Imaging of Tumor PD-L1 Expression Using Radiolabeled Anti-PD-L1 Antibodies
- 89Zr-Labeled Versus 124I-Labeled {alpha}HER2 Fab with Optimized Plasma Half-Life for High-Contrast Tumor Imaging In Vivo
- Immuno-PET and Immuno-SPECT of Rheumatoid Arthritis with Radiolabeled Anti-Fibroblast Activation Protein Antibody Correlates with Severity of Arthritis
- Role of Positron Emission Tomography for the Monitoring of Response to Therapy in Breast Cancer
- Update on Time-of-Flight PET Imaging
- Glypican-3-Targeting F(ab')2 for 89Zr PET of Hepatocellular Carcinoma
- 89Zr-trastuzumab and 89Zr-bevacizumab PET to Evaluate the Effect of the HSP90 Inhibitor NVP-AUY922 in Metastatic Breast Cancer Patients
- Glypican-3-Targeted 89Zr PET Imaging of Hepatocellular Carcinoma: Where Antibody Imaging Dares to Tread
- In Vivo Visualization of MET Tumor Expression and Anticalin Biodistribution with the MET-Specific Anticalin 89Zr-PRS-110 PET Tracer
- Early-onset Brain Metastases in a Breast Cancer Patient after Pathological Complete Response to Neoadjuvant Chemotherapy
- Synthesis, Preclinical Validation, Dosimetry, and Toxicity of 68Ga-NOTA-Anti-HER2 Nanobodies for iPET Imaging of HER2 Receptor Expression in Cancer
- Review on Production of 89Zr in a Medical Cyclotron for PET Radiopharmaceuticals
- Molecular Pathways: Next-Generation Immunotherapy--Inhibiting Programmed Death-Ligand 1 and Programmed Death-1
- Advances in Immuno-Positron Emission Tomography: Antibodies for Molecular Imaging in Oncology
- Molecular Imaging of Tumors with Radioactive Labeled Antibodies from Laboratory to the Clinic
- Imaging of Human Epidermal Growth Factor Receptor Type 2 Expression with 18F-Labeled Affibody Molecule ZHER2:2395 in a Mouse Model for Ovarian Cancer
- PET with the 89Zr-Labeled Transforming Growth Factor-{beta} Antibody Fresolimumab in Tumor Models
- Intraoperative Near-Infrared Fluorescence Tumor Imaging with Vascular Endothelial Growth Factor and Human Epidermal Growth Factor Receptor 2 Targeting Antibodies
- ImmunoSPECT and ImmunoPET of IGF-1R Expression with the Radiolabeled Antibody R1507 in a Triple-Negative Breast Cancer Model
- 89Zr-DFO-J591 for ImmunoPET of Prostate-Specific Membrane Antigen Expression In Vivo
- Targeting of HER2-Expressing Tumors Using 111In-ABY-025, a Second-Generation Affibody Molecule with a Fundamentally Reengineered Scaffold
- Cerenkov Luminescence Imaging of Medical Isotopes