


Abstract
There is recent in vitro and in vivo evidence that somatostatin receptor subtype 2 (sst2) antagonists are better tools to target neuroendocrine tumors (NETs) than sst2 agonists. Indeed, antagonists bind to a greater number of sst2 sites than agonists. Whether sst2 antagonists could be used successfully to target non-NETs, expressing low sst2 density, is unknown. Here, we compare quantitatively 125I-JR11 sst2 antagonist binding in vitro with that of the sst2 agonist 125I-Tyr3-octreotide in large varieties of non-NET and NET. Methods: In vitro receptor autoradiography was performed with 125I-JR11 and 125I-Tyr3-octreotide in cancers from prostate, breast, colon, kidney, thyroid, and lymphoid tissues as well as NETs as reference. Results: In general, 125I-JR11 binds to many more sst2 sites than 125I-Tyr3-octreotide. In 13 breast cancers, 8 had a low binding (mean density, 844 ± 168 dpm/mg of tissue) with the agonist whereas 12 had a high binding (mean density, 4,447 ± 1,128 dpm/mg of tissue) with the antagonist. All 12 renal cell cancers showed a low binding of sst2 with the agonist (mean density, 348 ± 49 dpm/mg of tissue) whereas all cases had a high sst2 binding with the antagonist (mean density, 3,777 ± 582 dpm/mg of tissue). One of 5 medullary thyroid cancers was positive with the agonist, whereas 5 of 5 were positive with the antagonist. In 15 non-Hodgkin lymphomas, many more sst2 sites were labeled with the antagonist than with the agonist. In 14 prostate cancers, none had sst2 binding with the agonist and only 4 had a weak binding with the antagonist. None of 17 colon cancers showed sst2 sites with the agonist, and only 3 cases were weakly positive with the antagonist. In the various tumor types, adjacent sst2-expressing tissues such as vessels, lymphocytes, nerves, mucosa, or stroma were more strongly labeled with the antagonist than with the agonist. The reference NET cases, incubated with a smaller amount of tracer, were also found to have many more sst2 sites measured with the antagonist. Conclusion: All renal cell cancers and most breast cancers, non-Hodgkin lymphomas, and medullary thyroid cancers represent novel indications for the in vivo radiopeptide targeting of sst2 by sst2 antagonists, comparable to NET radiotargeting with sst2 agonists.
- somatostatin sst2 receptors
- sst2 antagonist
- cancer radiopeptide targeting
- breast cancer
- renal cell cancer
Somatostatin receptors (sst) are highly overexpressed in gastroenteropancreatic and extra-gastrointestinal neuroendocrine tumors (NETs). This represents the molecular basis for sst-targeted diagnostic and therapeutic procedures in NET patients with somatostatin analogs (1–3). One main clinical application makes use of the inhibitory effects of somatostatin on NET cells, particularly on hormone secretion: long-acting somatostatin analogs, such as octreotide or lanreotide, potently inhibit tumoral hormone secretion and improve related symptoms. The second targeting approach is based on the administration of radioactive somatostatin analogs for diagnostic or therapeutic purposes. Indeed, 111In-octreotide scintigraphy (OctreoScan; Mallinckrodt) and other sst subtype 2 (sst2)–targeted imaging with, for example, 68Ga-DOTATATE, are gold standard methods for NET detection. Moreover, sst radionuclide therapy of NET with 90Y- or 177Lu-labeled somatostatin analogs is highly effective and increasingly applied (4,5). Recently, results of the first prospective, randomized, controlled phase III study using radiolabeled somatostatin analogs for peptide receptor radiotherapy were presented. Lutathera (177Lu-DOTATATE) significantly improved progression-free survival in comparison with cold octreotide therapy in advanced midgut NET (6).
Although it could be shown in vitro that sst2 antagonists do not trigger receptor internalization (7), we could show in animal models that radiolabeled sst2 or sst3 antagonists are not only as good in targeting in vivo the respective receptor, but also even considerably better than the respective agonists (8). The findings that antagonists for G-protein–coupled receptors (GPCRs) recognize more binding sites than agonists are not new and have been discussed in the literature by several groups (9,10). There are only hypotheses in regard to the origin of this difference. The difference is explained by distinct receptor states, those coupling to the G-proteins and uncoupled forms. Antagonists bind to all receptor states whereas agonists bind only to the G-protein–coupled forms that are assumed to represent only a small proportion of the total receptor population (9). In cancer, GPCRs are frequently overexpressed and the superiority of antagonists was shown for the gastrin-releasing peptide receptor (11), sst2 and sst3 (8), and the glucose-dependent insulinotropic polypeptide receptor (12).
A first pilot study in humans using a first-generation sst2 antagonist confirmed the animal studies (13). The antagonists were better than agonists for NET imaging (13). A parallel in vitro study on tissue sections fully confirmed that the 177Lu-DOTA-bass antagonist labeled more sst2 binding sites than the 177Lu-DOTATATE agonist (14). This was observed in NETs but, interestingly, also in a few non-NETs with a low number of sst2 (14). Presently, second-generation sst2 antagonists, such as JR11, are in clinical development, with promising results for diagnosis and targeted radionuclide therapy (15).
In the present study, we aimed at evaluating the in vitro binding properties of the second-generation antagonist JR11, labeled with 125I, and compared it with 125I-Tyr3-octreotide, the standard agonist radioligand (16,17). 125I labeling is the optimal choice for in vitro receptor autoradiography quantification (17,18). Indeed, 125I radioligands have been used for decades for receptor autoradiography measurements, and quantification of the data using radioactive reference standards has been routinely performed (18–20). The present study therefore allows a direct comparison of quantification data with previously published studies using 125I radioligands (18–20). This is at difference with the previous 177Lu-DOTA-bass study (14) in which the data using 177Lu-labeled ligands could not be directly compared with data with 125I-labeled ligands. In the present study, a large number of tumors, including such tumors with high-density sst2 (gastroenteropancreatic NET, pheochromocytomas) and those known to express little or no sst2 (renal cell cancer, breast cancer, prostate cancer, non-Hodgkin lymphoma [NHL], medullary thyroid cancer, colon cancer), were tested with both ligands. Nontumoral tissues, adjacent to the tumors, were also evaluated.
MATERIALS AND METHODS
In a first part, we designed cold iodinated JR-11 (iodo-JR11) (structure: DOTA-Cpa-d-Cys-Aph(L-HOro)-d-Aph(Cbm)-Lys-Thr-Cys d-3-iodo-Tyr-NH2) and measured its binding affinity to sst2. Iodo-JR11 was then tested in a displacement experiment using sst2-transfected cells in an in vitro autoradiography setting with 125I-Tyr3-octreotide as radioligand, as reported previously (21). IC50 (half maximal inhibitory concentration) values were 1.89 ± 1.1 nM (n = 3) for iodo-JR11 and 2.83 ± 1.6 nM (n = 3) for the reference peptide SS-28. The compound iodo-JR11 has therefore high-affinity binding to sst2 and is suitable as radioligand for the planned cancer experiments.
In a second part, we used 125I JR-11 (74,000 GBq [2,000 Ci]/mmol; Anawa) as radioligand to evaluate the presence of sst2 in human breast cancers, renal cell cancers, NHL, medullary thyroid cancers, prostate cancers, colon cancers, pheochromocytomas, paragangliomas, bronchial and ileal NET, and small cell lung cancers. Comparison was done with the agonist tracer 125I-Tyr3-octreotide (74,000 GBq [2,000 Ci]/mmol; Anawa), known to have an IC50 similar to the antagonist (21). Quantification was performed as previously reported (21). Specific binding was calculated as total binding minus nonspecific binding for each tumor case. Nonspecific binding was assessed in each case in an adjacent section incubated with 125I JR-11 or 125I-Tyr3-octreotide in the presence of 100 nM of the unlabeled antagonist or agonist, respectively. The study conformed to the ethical guidelines of the Medical Faculty of the University of Berne. The institutional review board approved this retrospective study and the requirement to obtain informed consent was waived.
RESULTS
One group of tumors, shown previously with sst2 agonist tracers to have low (<1,000 dpm/mg tissue) levels or a lack of sst2, consisting of 13 samples of breast carcinomas, 12 samples of renal cell cancers, 15 samples of NHL, 5 samples of medullary thyroid cancers, 14 samples of prostate cancers, and 17 samples of colon cancers was used in receptor autoradiography experiments as reported previously (22–29). Successive sections were incubated in a buffer solution containing the standard amount of 30,000 cpm/100 μL of 125I-Tyr3-octreotide or 30,000 cpm/100 μL of 125I-JR-11. Quantification was performed as previously reported (21). Tables 1 and 2 and Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org) show all the results.
Comparison of 125I-JR11 Antagonist Binding with 125I-Tyr3-Octreotide Agonist Binding in Breast Cancer and RCCs Using 30,000 cpm/100 μL of Radioligand
Comparison of 125I-JR11 Antagonist Binding with 125I-Tyr3-Octreotide Agonist Binding in Medullary Thyroid Cancers and NHLs Using 30,000 cpm/100 μL of Radioligand
A second group of tumors, shown previously with sst2 agonist tracers to have a high level of sst2, consisting of 5 pheochromocytomas, 2 paragangliomas, 4 ileal NET, 1 bronchial NET, and 4 small cell lung cancers, was also used in receptor autoradiography experiments; however, instead of 30,000 cpm/100 μL of tracer, only 10,000 cpm/100 μL of 125I-Tyr3-octreotide or 125I-JR11 were given. All these cases had been tested previously with 30,000 cpm/100 μL of 125I-Tyr3-octreotide and were shown to express a high density (>2,000 dpm/mg of tissue) of receptors in all cases. The rationale for the strategy to use 10,000 cpm/100 μL of radioligand was that we assumed, based on Cescato et al. (14), that the antagonist tracer binds to more sites than the agonist and that therefore it is mandatory to use a lesser amount of tracer to prevent overexposure of the films in the antagonist part of the experiment. The results are summarized in Table 3.
Comparison of 125I-JR11 Antagonist with 125I-Tyr3-Octreotide Agonist in Selected Tumors with High Density of sst2 Using 10,000 cpm/100 μL of Radioligand
Breast Cancers
Table 1 shows that 8 of 13 breast cancer samples express sst using 125I-Tyr3-octreotide, in most of the cases in low density. The mean density of the receptor-positive cases is 844 ± 168 dpm/mg of tissue (mean ± SEM). These data are comparable with previously reported results (22). With 125I-JR11, however, sst can be detected in as many as 12 of 13 breast cancers, often in high density. The mean density of the receptor-positive cases is 4,447 ± 1,128 dpm/mg of tissue. Figure 1 illustrates the results. Interestingly, although the antagonist labels more sites, the heterogeneity of labeling seen with the agonist is not abolished with the antagonist (Table 1), indicating that breast cancers are multiclonal tumors with areas with and without sst. Moreover, the tumoral and peritumoral vessels in the breast cancer samples are sometimes (4/9 cases) weakly labeled with 125I-Tyr3-octreotide. However, with 125I-JR11, all 9 cases with identified vessels show a moderate to high labeling of these vessels. Therefore, these results are strongly indicative for a markedly higher binding of 125I-JR11 versus 125I-Tyr3-octreotide.
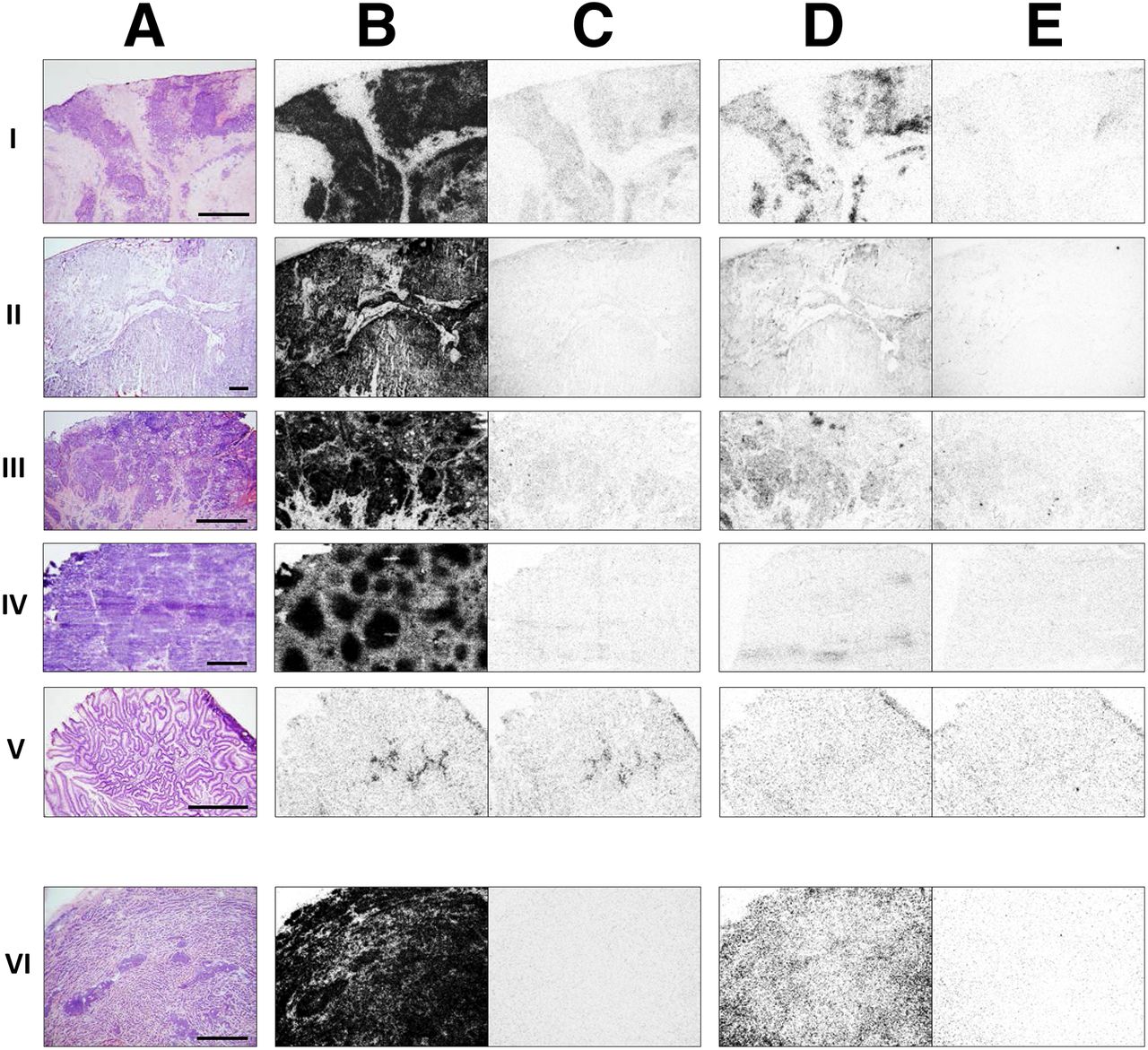
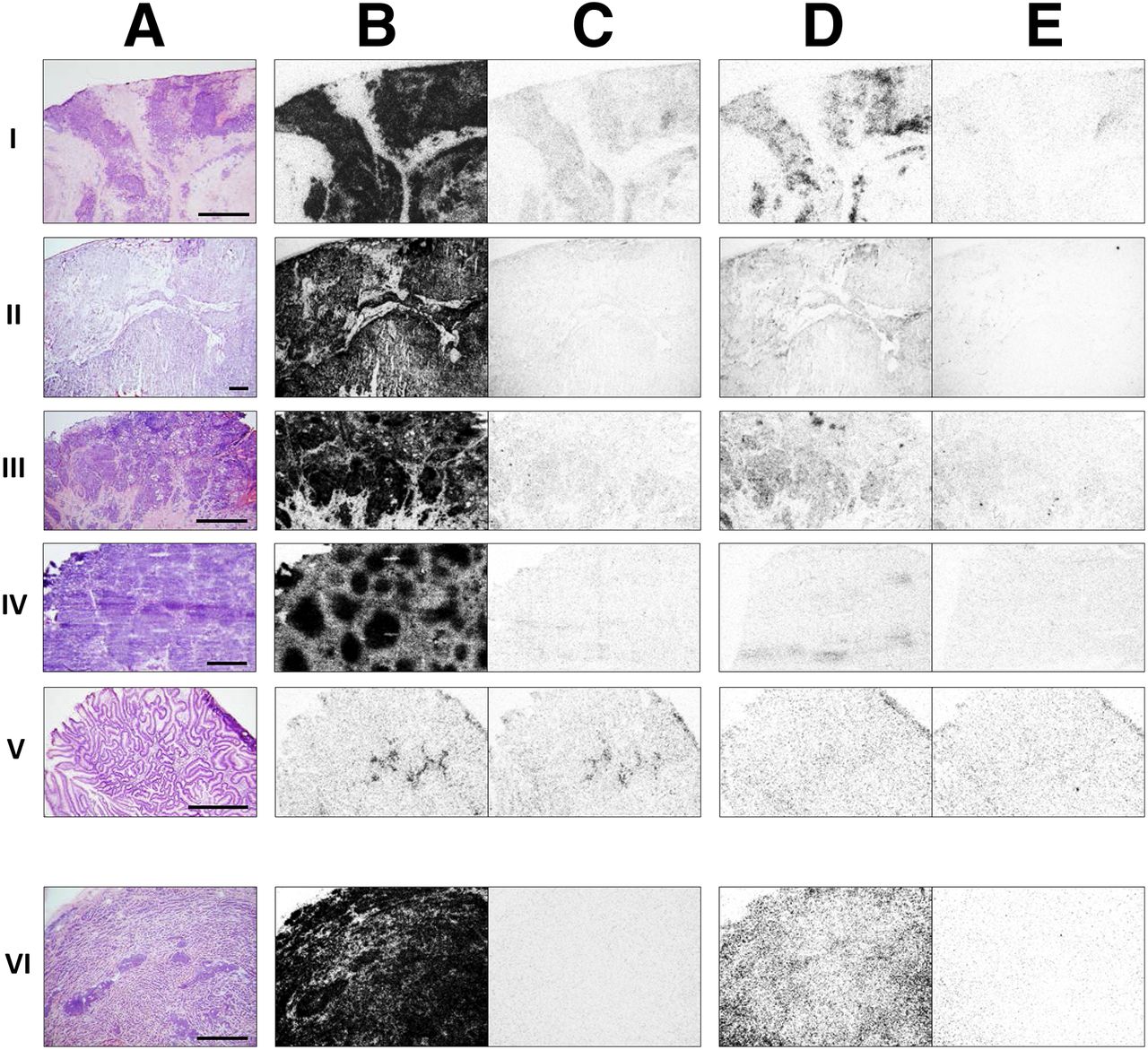
Comparative receptor autoradiography in various cancer types (A, hematoxylin and eosin staining) with 125I-JR11 (B and C) and 125I-Tyr3-octreotide (D and E). B and D are respective total binding, C and E are respective nonspecific binding. Bars = 1 mm. (I) Breast cancer. (II) RCC. (III) Medullary thyroid cancer. (IV) NHL. (V) Colon cancer. In cancers I–V, sections were incubated with 30,000 cpm/100 μL of antagonist or agonist. Cancers I–IV show much higher density of sst2 with antagonist. Colon cancer (V) is negative. (VI) Ileal NET, incubated with 10,000 cpm/100 μL of antagonist or agonist.
Renal Cell Cancers
Table 1 also shows in a series of 12 renal cell cancers a low level of sst with the agonist in all cases; however, a high density of sst can be identified in all cases with the antagonist. One example is shown in Figure 1. Mean density value with the agonist is 348 ± 49 dpm/mg of tissue (mean ± SEM) and 3,777 ± 582 dpm/mg of tissue with the antagonist, representing a more than 10 times difference. The density values with the antagonist resemble the levels seen in NETs in standard studies with the agonist (18–20). As seen previously in breast cancers, a much higher number of binding sites is detected in peritumoral vessels with the antagonist than with the agonist.
Medullary Thyroid Cancers
Table 2 reveals that 4 of 5 medullary thyroid cancers were not labeled with the agonist but that all showed moderate to high labeling with the antagonist. Figure 1 shows a representative example.
NHL
Similarly, Table 2 shows that in the 15 NHLs, the antagonist tracer bound to many more sst2 than the agonist. Whereas the values for the agonist were low or negative, the values measured with the antagonist could be compared with what was seen in NET with the agonist in standard studies (18–20). Figure 1 shows a representative example. Here again, tumoral vessels are strongly positive with the antagonist.
Prostate Cancers
Supplemental Table 1 shows that the agonist 125I-Tyr3-octreotide does not detect any sst2 in the 14 prostate cancer samples, confirming previously published results (23), whereas the antagonist 125I-JR11 detects 5 positive cases, 4 of them having only a low sst2 density. Therefore, the antagonist had a higher sensitivity to detect sst2 in prostate cancer than the agonist. The higher sensitivity was also observed in the normal adjacent prostate tissues, such as stroma, vessels, or nerves: indeed, whereas these tissues were occasionally labeled with 125I-Tyr3-octreotide, as reported previously as well (23), they were labeled to a much higher level in the experiments with 125I-JR11. Figure 2 summarizes these results.
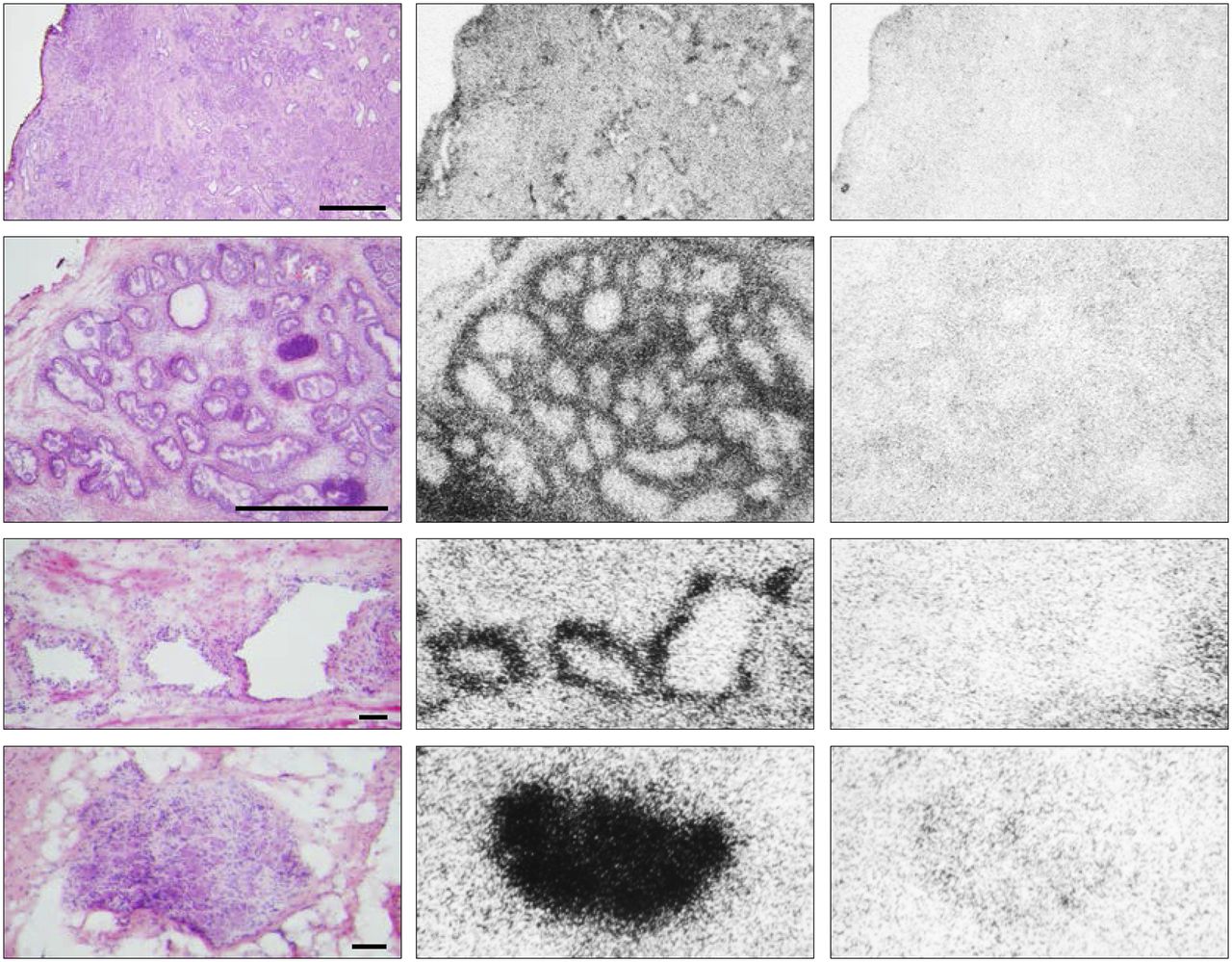
Receptor autoradiography with 125I-JR11 showing sst in a prostate cancer sample. (Left) Hematoxylin and eosin staining. (Middle) Total binding of JR11. (Right) Nonspecific binding. (First row) Weakly receptor-positive prostate cancer. Bar = 1 mm. (Second row) Receptor-positive stroma. Bar = 1 mm. (Third row) Receptor-positive vessels. Bar = 0.1 mm. (Fourth row) Receptor-positive nerve. Bar = 0.1 mm.
Colon Cancers
Supplemental Table 1 also shows that colon cancers in general do not express significant quantities of sst2, either with the agonist or with the antagonist tracer (Fig. 1), except for 3 cases with borderline levels of receptors as measured with the antagonist radioligand; this density is probably not clinically relevant for tumor targeting. However, in approximately half of the agonist experiments, tumoral vessels, lymphatic follicles, and mucosa are labeled as known from previous studies (30); in the antagonist experiments, not only are the vessels, lymphatic follicles, and mucosa labeled in all tested samples, but also the amount of labeling in these compartments is much higher than with the agonist.
NETs
In the series of tumors (Table 3) representing classic indications for sst targeting in vivo, based on the high number of sst, namely pheochromocytomas, paragangliomas, ileal, and bronchial NETs and small cell lung cancers, we have compared agonist and antagonist tracers using a lower amount of tracer of 10,000 cpm/100 μL to prevent overexposure of the films using the antagonist tracer. Despite the lower radioactivity application, the antagonist tracer bound with high levels whereas the agonist tracer bound in general with low levels, as seen in Figure 1. The difference in binding between antagonist and agonist varied between 2.5- and 40-fold.
DISCUSSION
The comparison of the binding of the sst2 agonist 125I-Tyr3-octreotide with the sst2 antagonist 125I-JR11 showed impressively that the antagonist labeled many more sst2 binding sites than the agonist, in tumor cells as well as in adjacent sst2-expressing tissues. The breast cancer data confirm and expand on the receptor quantification aspect of a previous paper (14) showing that a 177Lu-labeled sst2 antagonist labeled more sites than a 177Lu-labeled sst2 agonist. On the basis of the high number of 125I-JR11 binding sites (>2,000 dpm/mg of tissue) in more than half of the tested cases, we conclude in the present study that breast cancers should be added to the list of tumor types that may be successfully targeted in vivo with sst2 antagonist tracers. A similar conclusion can be drawn for renal cell carcinoma (RCC); the antagonist shows a more than 10 times mean increase in sst2 binding than with the agonist. Here, 10 of 12 cases showed an sst2 density higher than 2,000 dpm/mg of tissue. Such values predict a positive sst2 imaging in vivo in patients (18). Therefore, RCCs may be considered a serious indication for radiopeptide targeting with sst2 antagonists. In medullary thyroid cancer and NHL, the antagonist tracer labeled many more sites than the agonist, with 2 of 5 medullary thyroid cancers and 8 of 15 NHLs having an sst2 density over 2,000 dpm/mg of tissue, respectively. The marked differences between agonist and antagonist binding may be explained by G-protein coupling with the receptor, as discussed above. GPCRs were present in at least 2 affinity states for the radioligands, a small proportion in a GPCR conformation can be labeled by agonists, and a large proportion in a G-protein–independent (uncoupled) receptor conformation can be labeled by antagonists (9).
Importantly, in the past, there have been in vivo patient studies using sst2 agonists that documented the possible feasibility of sst2 targeting under certain conditions in several non-NETs or tumors expressing only occasionally sst2 (25–29). Such in vivo studies in patients included targeting of breast cancers (22,31), RCCs (32,33), NHL (34), prostate cancers (24), and medullary thyroid cancers (35). However, as opposed to NETs, there has never been a systematic follow-up and extension of these studies, because it was clear that the predominantly low number of sst2 detected by the agonist radioligands would prevent a routine application of sst2 ligands in these indications.
Other types of cancer tested in the present study do not appear to have a significant number of agonist or antagonist binding sites. Indeed, the prostate cancers are unlikely to be an adequate target for JR11, not only because the tumor cells rarely express sst, but also because adjacent tissues, in particular stroma, vessels, and nerves, regularly express sst that may mimic a tumoral sst2 expression. Similarly, colon cancers seem not to be appropriate tumor types for sst2 radiotargeting, either with sst2 agonists or with antagonists.
For comparison, the tumors with an established high density of sst2, namely the NETs in Table 3, show in all cases a massive overexpression of sst2 with the antagonist, despite the fact that in the present experimental setting the tumor sections were incubated with only one third of the standard radioligand dose. These data confirm what is seen in vivo in patients with gastroenteropancreatic NETs using the sst2 antagonist JR11, as reported by Wild et al. (15). Moreover, not only gastrointestinal NETs but also pheochromocytomas, paragangliomas, and lung NETs may be ideally targeted with sst2 antagonists.
CONCLUSION
Whereas the present in vitro data convincingly show that sst2 antagonists of the second generation such as JR11 are successful and superior to agonists in NETs, the data also strongly suggest that new indications for sst2 targeting with these antagonists should be seriously considered, namely renal cell cancers, breast carcinomas, medullary thyroid cancer, and NHL. These in vitro data provide the molecular basis to initiate a clinical trial in these indications.
DISCLOSURE
Octreopharm Sciences GmbH, Berlin, Germany, provided financial support of a part of the study. Jean Claude Reubi is a consultant to Ipsen and is inventor of several licensed patents. Helmut Mäcke and Jean Rivier are inventors of licensed patents. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Judit Erchegyi and Charleen Miller for providing technical assistance and Jean Laissue for reviewing selected tumor cases.
Footnotes
Published online Aug. 25, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 10, 2016.
- Accepted for publication August 3, 2016.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effect of Tumor Perfusion and Receptor Density on Tumor Control Probability in 177Lu-DOTATATE Therapy: An In Silico Analysis for Standard and Optimized Treatment
- P2X7 PET Radioligand 18F-PTTP for Differentiation of Lung Tumor from Inflammation
- New Developments in Peptide Receptor Radionuclide Therapy
- Advantages and Limits of Targeted Radionuclide Therapy with Somatostatin Antagonists
- Somatostatin Antagonists for Radioligand Therapy of Nonendocrine Tumors
- Reply: Advantages and Limits of Targeted Radionuclide Therapy with Somatostatin Antagonists
- Molecular Imaging of Human Embryonic Stem Cells Stably Expressing Human PET Reporter Genes After Zinc Finger Nuclease-Mediated Genome Editing
- SSTR-Mediated Imaging in Breast Cancer: Is There a Role for Radiolabeled Somatostatin Receptor Antagonists?
- Somatostatin Receptor Antagonists for Imaging and Therapy
- Approaches to Multireceptor Targeting: Hybrid Radioligands, Radioligand Cocktails, and Sequential Radioligand Applications
- Biodistribution, Pharmacokinetics, and Dosimetry of 177Lu-, 90Y-, and 111In-Labeled Somatostatin Receptor Antagonist OPS201 in Comparison to the Agonist 177Lu-DOTATATE: The Mass Effect
- Proof of Therapeutic Efficacy of a 177Lu-Labeled Neurotensin Receptor 1 Antagonist in a Colon Carcinoma Xenograft Model
- Citius, Altius, Fortius: An Olympian Dream for Theranostics