


Abstract
We evaluated the diagnostic value and accuracy of prostate-specific membrane antigen (PSMA) PET for the intraprostatic delineation of prostate cancer before prostatectomy. Methods: We identified 6 patients with biopsy-proven high-risk prostate cancer who were referred for 68Ga-PSMA PET/CT before radical prostatectomy to rule out metastasis. After prostatectomy, a histologic map of the prostate was reconstructed. The histologic extent and Gleason score of each segment of the prostate were compared with 68Ga-PSMA PET images resliced to the histologic axis. Sensitivity, specificity, positive and negative predictive value, and positive and negative likelihood ratios were calculated. The SUV of each segment was measured, and median values were compared. Results: Of the 132 segments, 112 were eligible for analysis. The correlation of histologic results with 68Ga-PSMA PET images showed a specificity and sensitivity of 92%. The positive and negative likelihood ratio and the positive and negative predictive value for detection of prostate cancer on 68Ga-PSMA PET were 11.5, 0.09, 96%, and 85%, respectively. The median SUVmax of true-positive prostate segments was significantly higher than that of true-negative segments (11.0 ± 7.8 vs. 2.7 ± 0.9, P < 0.001), and a cutoff of 4 revealed a sensitivity and specificity of 86.5% and an accuracy of 87.5%. Conclusion: These preliminary results show that the intraprostatic localization and extent of prostate cancer may be estimated by 68Ga-PSMA PET. This imaging method may be helpful for identifying target lesions before prostate biopsy and may support decision making before focal or radical therapy.
Prostate cancer is the most common cancer in men. Within the United States, an estimated 26% of cancer cases in 2015 were expected to be prostate cancer (1). Prostate-specific antigen–based screening leads to a significant proportion of overdiagnosis (2) and, consequently, overtreatment (3). Overtreatment is partly caused by an unknown true tumor extent before prostate biopsy and by the planning of a definitive therapy.
Prostate-specific membrane antigen (PSMA) is a transmembrane protein (4) expressed in prostate epithelial cells. Its expression is increased in prostate cancer cells and becomes higher as the cancer progresses (5,6). PSMA is also expressed in some normal tissues (e.g., small intestine, renal tubules, and salivary glands) (7), but in prostate cancer the expression levels are 100- to 1,000-fold higher (8). Some recently developed 68Ga-labeled PSMA ligands have been shown to have high specificity and sensitivity for the detection of recurrent prostate cancer and metastatic disease (9).
PSMA-based imaging may have the potential to exactly characterize the extent of intraprostatic disease and may therefore be a useful tool to identify and define malignant lesions before prostate biopsy and, finally, to help tailor an optimal, definitive therapy for each patient. Therefore, the aim of this proof-of-concept study was to analyze the performance of 68Ga-labeled 68Ga-PSMA PET/CT for prediction of the true extent of cancer within the prostate and seminal vesicles.
MATERIALS AND METHODS
Patient Population
Between May 2014 and August 2015, we identified 6 patients (mean age ± SD, 65 ± 8.2 y; range, 56–73 y) with biopsy-proven prostate cancer who had undergone 68Ga-PSMA PET/CT 3–32 d before radical prostatectomy (RPE) because of a high risk of extraprostatic manifestation of prostate cancer. Transrectal ultrasound–guided prostate biopsy with 6–14 cores had been performed for all patients. Local and external reference pathology institutions performed histologic analysis and Gleason scoring. 68Ga-PSMA PET/CT was performed to rule out metastasis. The indication for 68Ga-PSMA imaging was appointed by an interdisciplinary tumor board. All patients signed an informed consent form before undergoing PET/CT.
In 2 patients, metastasis was found (a single bone metastasis in one patient and nodal involvement in the other patient). There is increasing evidence that even in patients with lymph node involvement or a few bone lesions, RPE may delay progression, delay castration-resistant cancer, and even prolong survival (10,11). These available data were thoroughly clarified for the 2 patients with metastasis, and they were then offered the possibility of RPE. Both patients consented to it. The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived.
Patient Preparation and 68Ga-PSMA PET/CT
Whole-body PET/CT was performed 65.1 ± 7.0 min after injection of 161 ± 19.8 MBq (range, 131–193 MBq) of 68Ga-PSMA-HBED-CC (HBED-CC is N,N′-bis[2-hydroxy-5(carboxyethyl)benzyl]ethylenediamine-N,N′-diacetic acid) (12). The patients were asked to void immediately before undergoing scanning. The scans were obtained using a high-resolution hybrid PET/CT system (Biograph mCT, with a 128-slice CT component; Siemens Medical Solutions). Low-dose CT of the entire area covered by PET (from skull to mid-thigh) was performed for attenuation correction. After completion of the CT scan, PET data were acquired for 3 min per bed position. PET images were reconstructed using the standard manufacturer-supplied software (PET resolution of 3 mm).
Image Analysis
Two board-certified radiologists and nuclear medicine physicians clinically analyzed the images before RPE. SUVmax was measured within each prostate segment after reangulation of the images to match the histologic slices of the prostate, which were from base to apex and axial to the course of the urethra. A board-certified urologist, nuclear medicine physician, and pathologist compared the 68Ga-PSMA images with the postoperative histologic maps to determine whether the imaging findings for each prostate segment were true-positive, true-negative, false-positive, or false-negative.
Pathologic Evaluation
RPE was performed on all 6 patients. The prostate specimens were processed and evaluated according to the local standard operating procedures of the Institute of Pathology (13). After macroscopic examination, the prostate and seminal vesicles were fixed in 10% neutral buffered 4% formalin solution (∼4% formaldehyde). The gland was prepared for histology by a modified version of the technique introduced by the Association of Clinical Pathologists (14). After removal of the apex and base of the prostate, the gland was cut transversally into 5-mm-thick slices. Finally, the slices were separated into right and left halves and front and back sections. The complete slices of the specimen were embedded in paraffin blocks, which were then cut into 4-μm slices, stained with hematoxylin and eosin, and microscopically examined. The Gleason score (15) and the stage were determined according to the Union International Contre le Cancer and TNM systems (16).
Topographic Analysis
The extent of cancer within the specimen was mapped according to the method Bettendorf et al. (13) and Eminaga et al. (17). The map consists of 22 segments, including 2 segments for the seminal vesicles. The digitized data were the basis for calculation of percentage tumor volume. The Gleason score of each segment was individually documented. An example map is shown in Figure 1.

Reangulated slices from patient 1 show concordance between 68Ga-PSMA distribution and histologic maps. “10” represents 10-mm positive surgical margin.
Statistical Analysis
SPSS Statistics, version 23 (IBM), was used for analysis. Sensitivity, specificity, positive and negative predictive value, and positive and negative likelihood ratios were calculated for all available segments. A Kruskal–Wallis test was performed to compare the median SUVmax of true-positive and true-negative segments. We estimated the diagnostic performance of 68Ga-PSMA PET by calculating the area under the receiver-operating-characteristic curve. Two-sided P values of less than 0.05 were considered statistically significant.
RESULTS
Histologic results were available for 132 segments from 6 patients. For each patient, the analysis excluded 2 segments that could not be identified on PET/CT compared with the anatomy of the prostate. In 2 patients (patients 2 and 5), 4 segments adjacent to the bladder were excluded because of spillover of urine activity. Thus, a total of 112 segments were included in the statistical analysis.
Detailed clinical data and histopathologic results for the patients are summarized in Table 1.
Pre- and Postoperative Patient Characteristics
Comparison of Cancer Maps, Gleason Scores, and 68Ga-PSMA PET Results
Only 3 of 37 segments without histologic cancer on the maps were considered positive on the corresponding slices from 68Ga-PSMA PET, resulting in a specificity of 92% (Table 2). With the maps being defined as the gold standard, the sensitivity of 68Ga-PSMA PET for identifying areas with cancer was 92%. Of the 3 false-positive segments, one showed active prostatitis, one chronic prostatitis, and one high-grade prostatic intraepithelial neoplasia.
68Ga-PSMA vs. Histology Results for Segments Verified Histopathologically After RPE
The positive and negative likelihood ratios for 68Ga-PSMA PET in detecting prostate cancer were 11.5 and 0.09, respectively. The positive and negative predictive values were 96% and 85%, respectively, indicating a strong and exact correlation between 68Ga-PSMA positivity and the actual histologic presence of cancer. SUVmax was significantly higher for true-positive segments than for true-negative segments (median, 11.0 ± 7.8 vs. 2.7 ± 0.9; P < 0.001; Kruskal–Wallis test).
An analysis of the area under the receiver-operating-characteristic curve for SUVmax (Fig. 2) in correlation with the histologic results revealed an area under the curve of 0.93 (95% confidence interval, 0.89–0.99; P < 0.001). Using an SUVmax cutoff of 4.0, a sensitivity and specificity of 88% and 86.5% and an accuracy of 87.5% were achieved.

Area under receiver-operating-characteristic curve (AUC) for SUVmax according to histologic results. CI = confidence interval.
Comparison of Gleason scores and 68Ga-PSMA PET results (Fig. 3) showed a high detection rate for true-positive segments (80%), even in lower Gleason scores of 3 + 3 = 6.
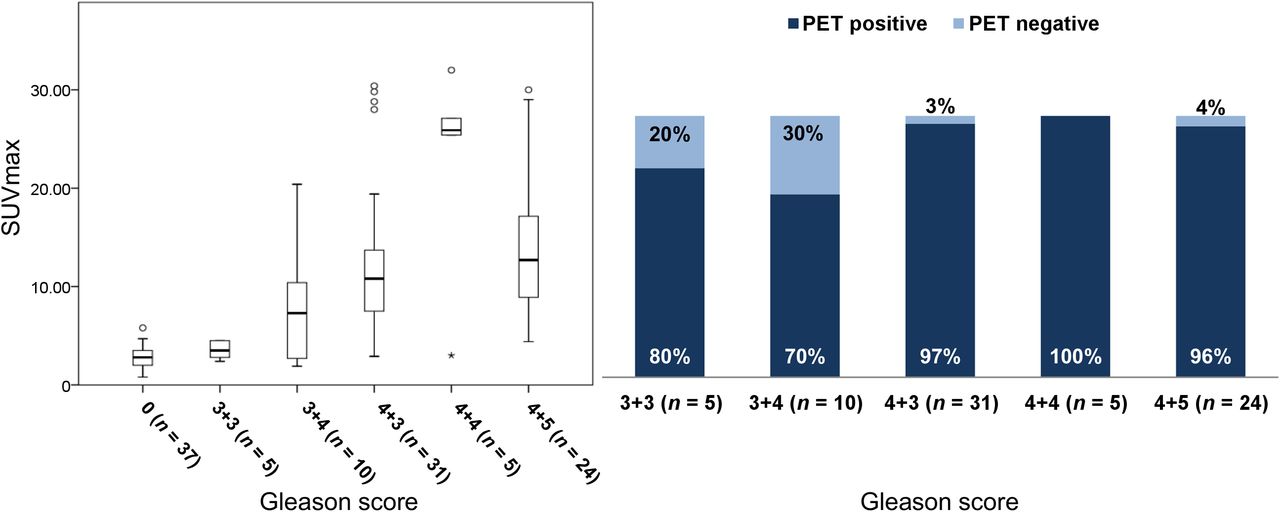
Graph on left plots SUVmax according to different locoregional Gleason scores. Graph on right depicts detection rates for segments true-positive on 68Ga-PSMA PET.
The box plot of SUVmax against Gleason score showed a tendency of SUVmax to increase, but because of the small number of patients no statistical analysis was performed (Fig. 3).
DISCUSSION
Preoperative information on the localization and extent of cancer within the prostate is limited, still lacks accuracy, and may result in inappropriate treatment (18). Multiparametric MRI is being increasingly used to display the local tumor burden within the prostate. However, despite its ability to detect lesions with a Gleason score of 7 or higher, especially in larger tumor foci, it has clinically significant limitations in smaller lesions and lesions with a Gleason score of less than 7. In a study in which multiparametric MRI was performed before RPE and correlated with the true tumor extent, Le et al. found that 80% of tumors were detected. However, tumors with a diameter smaller than 1 cm were missed by multiparametric MRI in most cases, even in some cases of high-grade lesions. Lesions with a Gleason score of 6 were missed in 80% of cases regardless of the diameter of the lesions (19).
In contrast, the specificity and sensitivity of 68Ga-PSMA PET in prostate cancer is reliable even when the Gleason score is 6 or less (9). The present preliminary analysis compared preoperative 68Ga-PSMA PET/CT imaging with postoperative cancer maps of the prostate. The results indicated high accuracy in predicting the pattern of cancer growth in the prostate by regional 68Ga-PSMA uptake.
To our knowledge, there have been only 2 publications reporting PSMA uptake in the prostate before RPE (20,21). Budäus et al. reported only about the use of 68Ga-PSMA to visualize cancer in the prostate gland (20). Using a 12-segment model, Rowe et al. showed a poor sensitivity of 10% and accuracy of 56% for detection of malignant prostate lesions in a stringent analysis of an 18F-labeled PSMA tracer (18F-DCFBC, or N-[N-[(S)-1,3-dicarboxypropyl]carbamoyl]-4-18F-fluorobenzyl-l-cysteine) that has a lower tumor-to-background contrast than 68Ga-PSMA-HBED-CC and seems to have a lower capability (21). In the same patient cohort and using the same stringent analysis, multiparametric MRI had a sensitivity of 35% and accuracy of 62%. In contrast, in applying 68Ga-PSMA PET imaging, we found a high sensitivity of 92% and accuracy of 92% in detecting malignant lesions using a 22-segment model. This discrepancy between our results and those of Rowe et al. might be explained not only by the superior tumor-to-background contrast of 68Ga-PSMA-HBED-CC but by the fact that reangulation of our images matched the histologic workup, in which the prostate was sliced axially to the urethra. A curved reangulation might match the histologic slices even better and should be evaluated in further studies.
Furthermore, in line with the results of Rowe et al. (21), our results indicated a significantly higher uptake in malignant lesions than in cancer-free segments (median SUVmax, 11.0 ± 7.8 vs. 2.7 ± 0.9; P < 0.001). However, their study found a lower SUVmax using an 18F-labeled PSMA tracer (median SUVmax, 3.5 vs. 2.2; P = 0.004).
In the present study, we thoroughly correlated histopathologic findings with 68Ga-PSMA PET findings and were able to confirm the results of a recent study by Afshar-Oromieh et al., who found that 68Ga-PSMA-HBED-CC is also reliable in the detection of prostate cancer that has a low Gleason score (≤7) (9).
Recent publications have demonstrated the increasing importance of using 68Ga-PSMA imaging to determine local recurrence or metastasis of prostate cancer (9,12,21). However, the decision to use 68Ga-PSMA imaging to rule out metastatic disease before prostatectomy must be made with caution and with an awareness of the patient’s disease history and of the potential for false-positive findings. For example, recent studies and case reports have shown high 68Ga-PSMA uptake in such conditions as schwannomas, celiac ganglia, and even differentiated thyroid cancer (22–24).
Our study was limited by deficiencies inherent in the retrospective approach and the small number of patients. In addition, to avoid spillover from urine activity, an indwelling catheter to empty the bladder before imaging could have been used. Despite these limitations, the present findings are a strong indication that the information provided by cross-sectional 68Ga-PSMA PET imaging may help clarify the localization and extent of cancer within the prostate both before biopsy and before definitive therapy. In particular, this novel technique has the potential to significantly improve decision making on the optimal, definitive therapy for individual patients. If our results are confirmed in larger collectives, 68Ga-PSMA PET imaging may help in decisions on whether to use focal treatment or radical treatment and—for RPE—on whether to use a nerve-sparing approach or a wide excision.
The data presented here are currently being validated. Optimization of the imaging protocols, such as through dynamic acquisition and dual-time-point imaging, seems to improve sensitivity further by further increasing the contrast of 68Ga-PSMA activity.
CONCLUSION
This preliminary proof-of-concept study showed that the localization and extent of cancer within the prostate can be estimated with high accuracy by 68Ga-PSMA PET technology. Therefore, this imaging method may be helpful for identifying target lesions before prostate biopsy and may support decision making on focal versus radical therapy. Larger studies with dedicated imaging protocols are needed to further evaluate the significance of these data, especially with use of hybrid imaging systems such as PET/MRI.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the PET radiochemistry group at the Department of Nuclear Medicine for highly reliable production of 68Ga-PSMA, as well as the PET/CT radiographers for excellent technical assistance.
Footnotes
Published online Jan. 14, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 4, 2015.
- Accepted for publication December 4, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence and Medium-Term Outcomes of Patients with Biopsy-Proven Intermediate- to High-Risk Prostate Adenocarcinoma with Low Intraprostatic Uptake on [68Ga]Ga-PSMA-11 PET/CT in the proPSMA Study
- Diagnostic Performance of [18F]AlF-Thretide PET/CT in Patients with Newly Diagnosed Prostate Cancer Using Histopathology as Reference Standard
- A Prostate-Specific Membrane Antigen PET-Based Approach for Improved Diagnosis of Prostate Cancer in Gleason Grade Group 1: A Multicenter Retrospective Study
- Analysing the tumor transcriptome of prostate cancer to predict efficacy of Lu-PSMA therapy
- Tumor Detection of 18F-PSMA-1007 in the Prostate Gland in Patients with Prostate Cancer Using Prostatectomy Specimens as Reference Method
- Head-to-Head Comparison of 68Ga-PSMA-11 with 18F-PSMA-1007 PET/CT in Staging Prostate Cancer Using Histopathology and Immunohistochemical Analysis as a Reference Standard
- qPSMA: Semiautomatic Software for Whole-Body Tumor Burden Assessment in Prostate Cancer Using 68Ga-PSMA11 PET/CT
- Detection Rate of 18F-Choline PET/CT and 68Ga-PSMA-HBED-CC PET/CT for Prostate Cancer Lymph Node Metastases with Direct Link from PET to Histopathology: Dependence on the Size of Tumor Deposits in Lymph Nodes
- Combination of 68Ga-PSMA PET/CT and Multiparametric MRI Improves the Detection of Clinically Significant Prostate Cancer: A Lesion-by-Lesion Analysis
- EBONI: A Tool for Automated Quantification of Bone Metastasis Load in PSMA PET/CT
- Immunohistochemical Validation of PSMA Expression Measured by 68Ga-PSMA PET/CT in Primary Prostate Cancer
- Intraindividual Comparison of 18F-PSMA-1007 PET/CT, Multiparametric MRI, and Radical Prostatectomy Specimens in Patients with Primary Prostate Cancer: A Retrospective, Proof-of-Concept Study
- PSMA Ligands for PET Imaging of Prostate Cancer
- Phase 2 Study of 99mTc-Trofolastat SPECT/CT to Identify and Localize Prostate Cancer in Intermediate- and High-Risk Patients Undergoing Radical Prostatectomy and Extended Pelvic LN Dissection
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy
- 68Ga-PSMA-11 PET as a Gatekeeper for the Treatment of Metastatic Prostate Cancer with 223Ra: Proof of Concept
- German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients
- What Medical, Urologic, and Radiation Oncologists Want from Molecular Imaging of Prostate Cancer
- Response and Tolerability of a Single Dose of 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer: A Multicenter Retrospective Analysis