


Abstract
Pheochromocytomas/paragangliomas overexpress somatostatin receptors, and recent studies have already shown excellent results in the localization of sympathetic succinate dehydrogenase complex, subunit B, mutation-related metastatic pheochromocytomas/paragangliomas using 68Ga-DOTATATE PET/CT. Therefore, the goal of our study was to assess the clinical utility of this functional imaging modality in parasympathetic head and neck paragangliomas (HNPGLs) compared with anatomic imaging with CT/MRI and other functional imaging modalities, including 18F-fluorohydroyphenylalanine (18F-FDOPA) PET/CT, currently the gold standard in the functional imaging of HNPGLs. Methods: 68Ga-DOTATATE PET/CT was prospectively performed in 20 patients with HNPGLs. All patients also underwent 18F-FDOPA PET/CT, 18F-FDG PET/CT, and CT/MRI, with 18 patients also undergoing 18F-fluorodopamine (18F-FDA) PET/CT. 18F-FDOPA PET/CT and CT/MRI served as the imaging comparators. Results: Thirty-eight lesions in 20 patients were detected, with 18F-FDOPA PET/CT identifying 37 of 38 and CT/MRI identifying 23 of 38 lesions (P < 0.01). All 38 and an additional 7 lesions (P = 0.016) were detected on 68Ga-DOTATATE PET/CT. Significantly fewer lesions were identified by 18F-FDG PET/CT (24/38, P < 0.01) and 18F-FDA PET/CT (10/34, P < 0.01). Conclusion: 68Ga-DOTATATE PET/CT identified more lesions than other imaging modalities. With the results of the present study, and the increasing availability and use of DOTA analogs in the therapy of neuroendocrine tumors, we expect that 68Ga-DOTATATE PET/CT will become the preferred functional imaging modality for HNPGLs in the near future.
Head and neck paragangliomas (HNPGLs) are neuroendocrine tumors (NETs) derived from the parasympathetic nervous system (1,2), representing approximately 0.6% of all head and neck tumors (3). These tumors mainly occur in the carotid body (CB) (60%), glomus vagale (GV) (13%), glomus jugulare (GJ) (23%), or glomus tympanicum (6%) regions (4). Depending on their localization and multiplicity, up to 38% or more of HNPGLs in patients with a negative family history are hereditary (5), mainly belonging to patients with succinate dehydrogenase complex, subunits B, C, or D (SDHB, SDHC, SDHD, collectively SDHx) mutations (5–7).
Although patients with hereditary HNPGLs are at a high risk for metastatic disease (particularly patients with SDHB mutations) or prone to developing multiple HNPGLs (especially those with SDHD mutations) (8), proper diagnosis of these tumors is often challenging because HNPGLs are typically biochemically silent and lack early symptoms (4).
Failure to accurately assess these tumors can lead to overlooked multiplicity and metastatic disease, resulting in an inappropriate follow-up, nondiagnosed heritability, and a delayed appropriate therapeutic plan with a high risk of noncurable disease.
18F-fluorohydroxyphenylalanine (18F-FDOPA) PET/CT, providing high sensitivity and specificity (2,9–11), is currently the functional imaging modality of choice in HNPGLs according to previous studies (2,9–11) and the current guidelines (12,13).
Because pheochromocytomas/paragangliomas (PPGLs) overexpress somatostatin receptors (SSTRs), especially SSTR2 (14), first studies were already able to show an excellent performance of 68Ga-DOTA-peptides in (genetically not further evaluated) HNPGLs (15,16). Similar diagnostic results were shown by our group in localizing sympathetic metastatic SDHB-related PPGLs outside the head and neck area (17), which otherwise are known to have a functional imaging signature and clinical behavior significantly different from parasympathetic HNPGLs (9,18).
Furthermore, DOTA-peptides are used for peptide receptor radionuclide therapy (PRRT), a potentially new treatment option in patients with HNPGLs, especially those around the foramen jugulare that are rarely suitable for surgical removal (19). This is important, because therapeutic approaches for surgically nonremovable tumors are limited and most of these patients are not eligible for 131I-metaiodobenzylguanidine (131I-MIBG) treatment because of their lack of 123/131I-MIBG uptake (9).
Therefore, our aim was to evaluate the diagnostic utility of 68Ga-DOTATATE PET/CT in SDHB or SDHD (SDHx)-related and other HNPGLs compared with 18F-FDOPA, 18F-FDG, and 18F-fluorodopamine (18F-FDA) PET/CT and CT/MRI, and to assess the potential eligibility of these patients for treatment with radiolabeled or cold somatostatin analogs.
MATERIALS AND METHODS
Patients
Between January 2014 and March 2015, 20 consecutive patients (11 men, 9 women) at a mean age of 48.4 ± 14.0 y were prospectively evaluated at the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health (NIH). All patients had presented with histologically confirmed PPGL at initial diagnosis. For ethical reasons, most lesions detected on imaging studies could not be histologically confirmed in the current study. Detailed information is provided in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
The study protocol was approved by the institutional review board of the Eunice Kennedy Shriver NICHD (protocol 00-CH-0093). All patients provided written informed consent for all clinical, genetic, biochemical, and imaging studies regarding PPGLs.
Seven patients had an SDHD mutation, 9 patients were positive for SDHB, 1 patient was positive for a hypoxia-inducible factor 2 α mutation, and 3 patients were apparently sporadic. Sixteen patients presented with additional primary PPGLs or metastatic disease (defined as PPGLs in sites in which chromaffin tissue is normally present) outside the head and neck region.
Imaging Techniques
CT scans of the neck were obtained using the following devices: Somatom Definition AS (Siemens Medical Solutions), Somatom Definition Flash (Siemens Medical Solutions), and Toshiba Aquilion ONE (Toshiba Medical Systems). Section thickness was 2 mm in the neck. All studies were performed with intravenous rapid infusion of 130 mL of nonionic water-soluble contrast agent (Isovue 300; Bracco Diagnostics), at 3–4 mL/s.
MR scans of the neck were obtained with 1.5- and 3-T scanners (Achieva 1.5 and 3 T [Philips] and Verio 1.5 T [Siemens Medical Solutions]). Image thickness was 5 mm for all neck studies. Pre- and postinjection images were obtained in the axial plane. All MR scans included axial T2 series with and without fat saturation, short tau inversion recovery series, and T1 pre- and postcontrast series after an intravenous injection of 0.2 mL/kg of body weight (Magnevist; Bayer Healthcare Pharmaceuticals).
All 20 patients underwent 68Ga-DOTATATE, 18F-FDOPA, and 18F-FDG PET/CT as well as CT or MRI, with 18 also undergoing 18F-FDA PET/CT. Fourteen patients received both a CT and an MRI of the neck whereas 3 patients received only a neck MRI and another 3 patients underwent only neck CT.
Whole-body PET/CT scans from the upper thighs to the skull were obtained 60 min after intravenous injection with mean doses of 192.4 ± 3.3 MBq of 68Ga-DOTATATE, 30 min after 465.1 ± 7.4 MBq of 18F-FDOPA, 60 min after 314.5 ± 81.4 MBq of 18F-FDG, and approximately 8 min after 38.9 ± 0.8 MBq of 18F-FDA. Sixty minutes before each 18F-FDOPA scan, a dose of 200 mg of carbidopa was administered orally. All PET/CT scans were obtained on a Biograph-mCT 128 PET/CT scanner (Siemens Medical Solutions). PET imaging was obtained in 3-dimensional mode. PET images were reconstructed on a 256 × 256 matrix using an iterative algorithm provided by the manufacturer, which also uses time of flight. Low-dose CT studies for attenuation correction and anatomic coregistration were performed without contrast.
Analysis of Data
68Ga-DOTATATE PET/CT studies were each interpreted independently by 2 nuclear medicine physicians, both of them with more than 10 y experience in PET and PET/CT imaging, masked to all imaging and clinical data except for the diagnosis, sex, and age of the patients. SUVmax was determined, and focal areas of abnormal uptake showing a higher SUVmax than surrounding tissue were considered as lesions. In all other imaging studies, physicians were masked to 68Ga-DOTATATE PET/CT scans and clinical data except for the diagnosis, sex, and age of the patients, as well as previous imaging studies. The CT and MR images were evaluated by a neuroradiologist with over 30 y of experience in HNPGL imaging. All imaging studies were performed within 3 mo of each other. All PET/CT studies were evaluated on workstations using MedView (MedImage); CT and MRI studies were evaluated on workstations using Vue PACS (Carestream).
Histologic proof of all head and neck lesions was not feasible. Therefore, all definite head and neck foci localized with 18F-FDOPA PET/CT or MRI (CT for the 3 patients in whom MRI could not be performed) were presumed to be true-positive lesions because these are the imaging modalities of choice for HNPGLs according to the current guidelines (12,13), with 18F-FDOPA known to have excellent sensitivity and specificity (2,9). Because differentiation between tympanic and GJ tumors is not always feasible, these lesions were summarized as jugulotympanic (JT) tumors. Abdomen, bones, liver, lungs, and mediastinum were evaluated for metastatic disease and considered positive regardless of the number of lesions.
Statistics
For statistical analysis, the McNemar test was used to compare sensitivities between 68Ga-DOTATATE PET/CT and the other imaging modalities. A 2-sided P value of less than 0.05 was considered significant.
RESULTS
Thirty-eight lesions were identified in total on 18F-FDOPA PET/CT and CT/MRI, with 37 of 38 lesions detected on 18F-FDOPA PET/CT and 23 of 38 lesions detected on CT/MRI. All 38 lesions were detected on 68Ga-DOTATATE PET/CT (mean SUVmax, 81.1 ± 83.6) as well as 7 additional head and neck lesions (P = 0.016) (mean SUVmax, 25.6 ± 27.7): 2 JT lesions, 1 GV lesion, 2 CB lesions (all related to SDHD mutations), and 2 lymph nodes (related to a SDHB mutation). Significantly fewer lesions were identified on 18F-FDG PET/CT (27/38, P < 0.01) and 18F-FDA PET/CT (10/34, P < 0.01). Except for the 7 lesions solely detected by 68Ga-DOTATATE PET/CT, 1 JT tumor (related to an SDHD mutation), measuring 1.6 cm on MRI and also positive on 18F-FDG and 68Ga-DOTATATE, was missed on 18F-FDOPA PET/CT. On CT/MRI, JT lesions and lymph nodes in particular were missed.
Detailed information about identified lesions and patient characteristics are provided in Table 1 and Supplemental Table 1.
Lesions Identified in Head and Neck on 68Ga-DOTATATE, 18F-FDOPA, 18F-FDG, and 18F-FDA PET/CT and CT/MRI, Compared with Lesions Identified by Imaging Comparator
On 68Ga-DOTATATE PET/CT, metastatic disease was identified in more patients and significantly more sites (P < 0.01) than in all other performed scans. Detailed information is provided in Supplemental Table 1 and Table 2.
Metastatic Disease Identified in Patients and Sites Outside Head and Neck on 68Ga-DOTATATE, 18F-FDOPA, 18F-FDG, and 18F-FDA PET/CT and CT/MRI
Figures 1–3 demonstrate patient examples, common sites of HNPGLs, and lesions solely detected by 68Ga-DOTATATE PET/CT.

Patient 5 with SDHD mutation–related HNPGLs. 68Ga-DOTATATE PET/CT (A) demonstrates lobulated finding in CB region on left side and additional lesion in GV region and in JT region on left side. JT findings are not visible on 18F-FDOPA PET/CT (B). 18F-FDG PET/CT (C) faintly demonstrates left CB and very faintly GV on left side. White arrow points to uptake in vocal cord. 18F-FDA PET/CT (D) is completely negative.

Patient 19 with SDHD mutation–related HNPGLs. 68Ga-DOTATATE PET/CT (A) demonstrates big mass in GV region on right side and additional lesion in CB region on right (white arrow). Finding in CB region is not visible on 18F-FDOPA PET/CT (B). On 18F-FDG PET/CT, only GV lesion is seen faintly (C). 18F-FDA PET/CT (D) is negative.
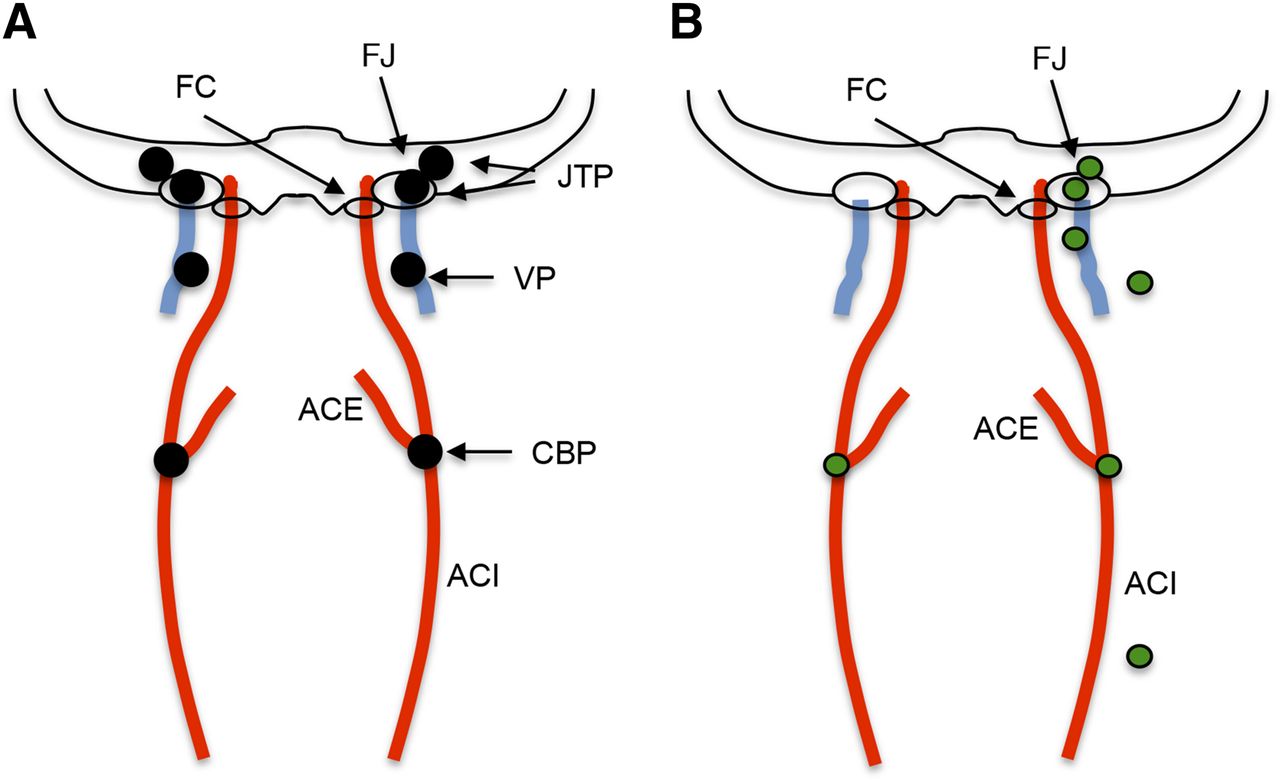
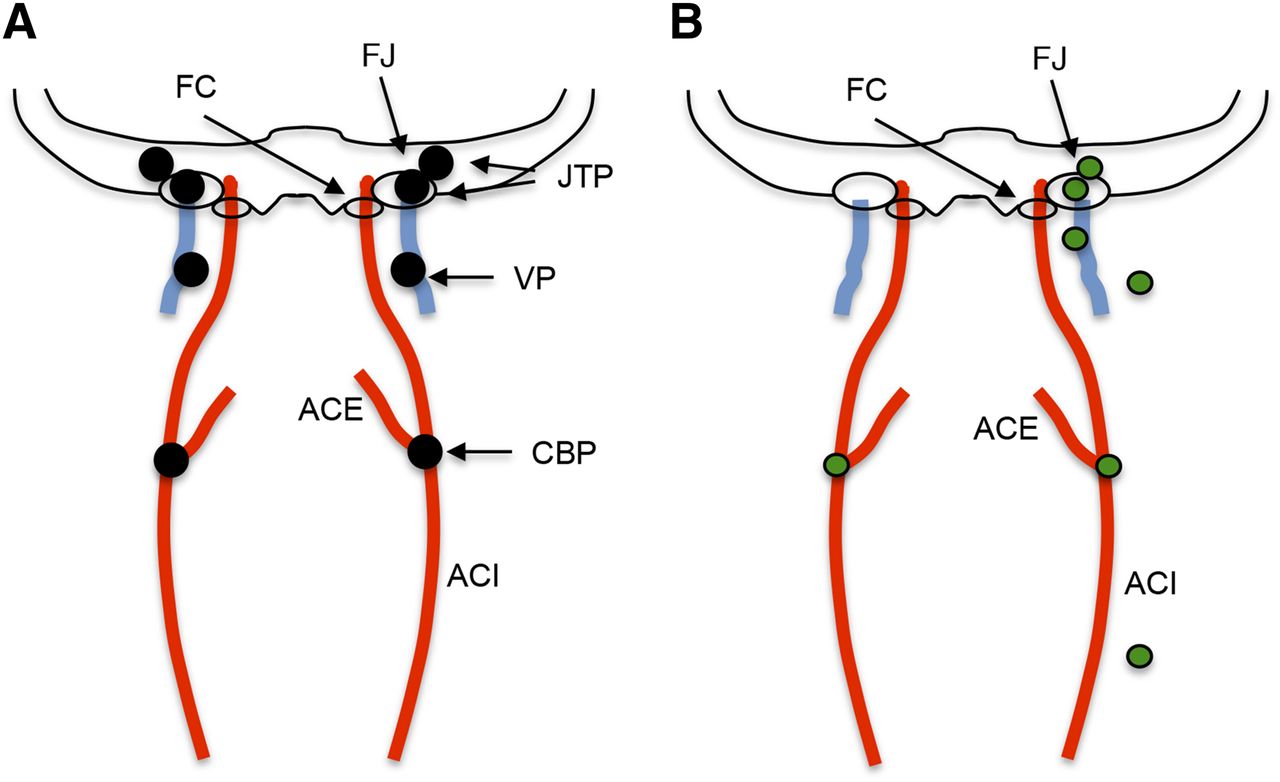
(A) Common sites of HNPGLs (black). (B) Localization of 7 lesions detected only on 68Ga-DOTATATE in our study (green). ACE = external carotid artery; ACI = internal carotid artery; CBP = carotid body paraganglioma; FC = carotid foramen; FJ = jugular foramen; JTP = JT paraganglioma; VP = vagale paraganglioma.
DISCUSSION
We present a comparison of 68Ga-DOTATATE PET/CT to 18F-FDOPA, 18F-FDG, and 18F-FDA PET/CT and to CT/MRI in a cohort of 20 patients with HNPGLs, 16 with underlying SDHx-related mutations, 1 with a hypoxia-inducible factor 2 α mutation, and 3 apparently sporadic.
On 68Ga-DOTATATE PET/CT, which highly selectively binds to SSTR2, significantly more lesions were detected than with the other imaging modalities used in this study, thus confirming the utility of 68Ga-DOTATATE in localizing HNPGLs and determining the possible eligibility of these patients for PRRT.
Functional imaging agents are able to target PPGLs through different mechanisms and have shown widely split performances based on tumor location and genetics.
18F-FDA specifically targets catecholamine synthesis, storage, and secretion pathways and enters the cell via the norepinephrine transporter (20). It has shown good imaging results in the localization of primary and metastatic sympathetic but not parasympathetic PGLs (21,22). In this study, only 10 of 34 lesions were detected on 18F-FDA PET/CT.
18F-FDG is a sensitive but nonspecific radiopharmaceutical using glucose transporters (23). Its accumulation is related to increased glucose metabolism as seen in many different types of tumors (23). SDHx-related HNPGLs and SDHx-related sympathetic PGLs have shown higher glucose uptake than sporadic and other hereditary PPGLs in previous studies (24,25), resulting in detection rates from 77% (9) to 90.5% (25). In our study, 27 of 38 lesions were detected, resulting in a lower detection rate of 71.1%, with 16 of our 20 patients being SDHx-positive. One reason for this may be that JT lesions might be missed because of their proximity to the brain, which shows high glucose uptake as well, or that not only the underlying genotype but also other not-yet-discovered mechanisms might influence the glucose uptake.
18F-FDOPA targets cells via the amino acid transporter system (26). It is the currently recommended functional imaging of choice in HNPGLs (12,13), proven to be sensitive and highly specific (2,9,10). This study confirms its strong diagnostic performance in localizing HNPGLs, identifying significantly more lesions than all other imaging modalities used except 68Ga-DOTATATE PET/CT (15). All lesions solely visualized on 68Ga-DOTATATE PET/CT were SDHx-positive, emphasizing a possible functional dedifferentiation of the large amino acid transporter in SDHx mutations.
PPGLs overexpress SSTR, mainly SSTR2 (14). SSTR imaging with 111In-DTPA-octreotide scintigraphy has already been shown to have strong diagnostic performance in parasympathetic HNPGLs (27). PPGL imaging with newly developed DOTA-analogs, binding to SSTR-expressing tumors much more effectively (28), has already been shown to have promising results (15,16,29–31). Recently, our group demonstrated the excellent diagnostic performance of 68Ga-DOTATATE PET/CT in localizing SDHB-related metastatic sympathetic PPGLs (17), which are otherwise known to show a substantially different imaging signature in specific and unspecific functional imaging modalities (9,18) when compared with HNPGLs, which are of parasympathetic origin.
In the current study, significantly more lesions of HNPGLs were identified on 68Ga-DOTATATE PET/CT than with all other imaging modalities combined, and no additional lesions were identified on any other imaging modality. Furthermore, 68Ga-DOTATATE PET/CT was able to detect metastatic disease outside the head and neck area in more patients and significantly more sites than all other imaging modalities and is therefore suggestive to have the largest impact on patient management. This finding is also in concordance with the increased expression of SSTR2A and SSTR3 found in PPGLs with an SDH deficiency (32), as most of our patients were positive for SDHx mutations.
Although false-positive findings cannot be fully excluded, we feel that the 7 lesions identified only by 68Ga-DOTATATE PET/CT most likely represent HNPGL manifestations for the following reasons: 5 of these lesions were found in typical locations for HNPGLs, all patients had confirmed HNPGLs, and all these lesions were seen in patients with SDHx mutation–related disease, who are at high risk for multiple primary or metastatic lesions. Furthermore, these lesions were characterized by relatively high SUVmax (25.6 ± 27.7).
Besides its diagnostic value, 68Ga-DOTATATE PET/CT is used to determine which patients may benefit from PRRT since surgery is not always feasible. PRRT is an established treatment option in gastroenteropancreatic NETs (33), and its successful use has already been reported in a limited number of patients with HNPGLs (19,34). Our data suggest that HNPGL patients who may benefit from PRRT could be detected with 68Ga-DOTATATE PET/CT. Prospective studies will have to prove the usefulness of PRRT and the value of 68Ga-DOTATATE PET/CT for the selection of these patients.
The results of the present study may also suggest that these patients can be treated with so-called cold SSTR analogs, including sandostatin LAR, lanreotide, or others. Although this has not yet been evaluated in HNPGLs, data from studies using lanreotide in gastroenteropancreatic NETs (35) and individual reports of octreotide treatment in patients with HNPGLs support this approach (36,37).
Anatomic imaging using CT/MRI is a main component of the diagnostic work-up of HNPGLs, with their greatest strength being the ability to estimate tumor delineation. However, functional imaging with 18F-FDOPA and 68Ga-DOTATATE PET/CT provides a higher sensitivity (9,10,16) and the advantage of whole-body imaging, which is especially important in the evaluation of patients with hereditary disease because of their increased risk for multiple tumors and metastases. In our study, lesions were missed by CT/MRI especially in the JT region. This might have been avoidable by performing 3-dimensional time-of-flight or 4-dimensional MR angiographic sequences, which seem to be more sensitive in detecting HNPGLs (2).
Although the patients in the present study underwent many PET/CT scans, the total radiation dose of the research scans 68Ga-DOTATATE, 18F-FDOPA, and 18F-FDA was slightly lower (∼24.2 mSv) than the total expected radiation dose of the still widely used 123I-MIBG and 111In-DTPA-octreotide SPECT/CT (∼26.1 mSv). Considering the potential of performing 68Ga-DOTATATE PET/CT with even lower activities than used in our study, and considering the opportunity to combine a 68Ga-DOTATATE PET/CT with a diagnostic contrast-enhanced CT in a single examination (1-stop), it might be possible to provide a desirable imaging work-up of these patients with a single imaging approach. This is supported by the fact that 68Ga-DOTATATE PET/CT may be superior to other currently used functional modalities in the detection of metastatic disease (currently known mainly for SDHx-related PPGLs) outside the head and neck region. This imaging work-up would result in a lower radiation exposure, decreasing costs, higher patient comfort, and improved therapeutic plans.
Limitations in our study consist of its small number of patients, with a significant portion having SDHB mutations (although SDHD mutations are more common in HNPGLs), a disproportionally low number of patients with apparently sporadic tumors, the lack of patients with underlying SDHC mutations, and a disproportionally high number of patients with metastatic disease. Furthermore, histologic proof was not feasible for most of lesions, explicitly including those that were only positive on 68Ga-DOTATATE PET/CT.
CONCLUSION
On 68Ga-DOTATATE PET/CT, more lesions were identified than on all other used imaging modalities, including the current gold-standard in functional imaging, 18F-FDOPA PET/CT. These results suggest a higher sensitivity and diagnostic value in the localization of SDHx-related and sporadic HNPGLs. Furthermore, the detection of metastatic disease outside the head and neck area was superior when using 68Ga-DOTATATE PET/CT than with other imaging modalities, suggesting the possible eligibility of primary HNPGLs as well as metastatic lesions for treatment with radiolabeled or cold somatostatin analogs. As the availability and use of DOTA-analogs in imaging and therapy of various NETs increases, we predict that 68Ga-DOTATATE PET/CT will become the preferred functional imaging modality for HNPGLs in the near future. However, the evaluation of the specificity of 68Ga-DOTATATE in these patients is subject to further large-scale studies with extended histologic confirmation of HNPGLs.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported, in part, by the Intramural Research Program of the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health and Human Development. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 12, 2015.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 18, 2015.
- Accepted for publication September 21, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Somatostatin Receptor-PET/CT/MRI of Head and Neck Neuroendocrine Tumors
- 68Ga-DOTATATE PET in Restaging and Response to Therapy in Neuroblastoma: A Case Series and a Mini Review
- 68Ga-DOTATATE PET in Restaging and Response to Therapy in Neuroblastoma: A Case Series and a Mini Review
- Imaging of Pheochromocytoma and Paraganglioma
- Performance of 68Ga-DOTA-Conjugated Somatostatin Receptor-Targeting Peptide PET in Detection of Pheochromocytoma and Paraganglioma: A Systematic Review and Metaanalysis
- False-positive findings on 6-[18F]fluor-L-3,4-dihydroxyphenylalanine PET (18F-FDOPA-PET) performed for imaging of neuroendocrine tumors
- Advances in adrenal tumors 2018
- Functional Imaging Signature of Patients Presenting with Polycythemia/Paraganglioma Syndromes
- Reply: 68Ga-DOTATATE PET/CT Versus MRI: Why the Comparison of 68Ga-DOTATATE PET/CT to an Appropriate MRI Protocol Is Essential
- 68Ga-DOTATATE PET/CT Versus MRI: Why the Comparison of 68Ga-DOTATATE PET/CT to an Appropriate MRI Protocol Is Essential
- Endocrine tumors associated with the vagus nerve