


Abstract
One problem of vascular angiogenesis therapy is the lack of reliable methods for evaluating blood flow in the microcirculation. We aimed to assess whether 99mTc-macroaggregated albumin perfusion scintigraphy (99mTc-MAA) predicts quantitated blood flow after therapeutic angiogenesis in patients with peripheral artery disease. Methods: Forty-six patients with peripheral artery disease were treated with bone marrow mononuclear cell implantation (BMCI). Before and 4 wk after BMCI, blood flow was evaluated via transcutaneous oxygen tension (TcPO2), ankle-brachial index, intravenous 99mTc-tetrofosmin perfusion scintigraphy (99mTc-TF), and intraaortic 99mTc-MAA. Results: Four weeks after BMCI, TcPO2 improved significantly (20.4 ± 14.4 to 36.0 ± 20.0 mm Hg, P < 0.01), but ankle-brachial index did not (0.65 ± 0.30 to 0.76 ± 0.24, P = 0.07). Improvement in 99mTc-TF count (0.60 ± 0.23 to 0.77 ± 0.29 count ratio/pixel, P < 0.01) and 99mTc-MAA count (5.21 ± 3.56 to 10.33 ± 7.18 count ratio/pixel, P = 0.02) was observed in the foot region but not the lower limb region, using both methods. When these data were normalized by subtracting the pixel count of the untreated side, the improvements in 99mTc-TF count (−0.04 ± 0.26 to 0.08 ± 0.32 count ratio/pixel, P = 0.04) and 99mTc-MAA count (1.49 ± 3.64 to 5.59 ± 4.84 count ratio/pixel, P = 0.03) in the foot remained significant. 99mTc-MAA indicated that the newly developed arteries were approximately 25 μm in diameter. Conclusion: BMCI induced angiogenesis in the foot, which was detected using 99mTc-TF and 99mTc-MAA. 99mTc-MAA is a useful method to quantitate blood flow, estimate vascular size, and evaluate flow distribution after therapeutic angiogenesis.
- angiogenesis
- bone marrow mononuclear cells
- peripheral artery disease
- radionuclide imaging
- sensitivity and specificity
Peripheral artery disease, which is mainly due to atherosclerosis, has a poor prognosis (1) and is increasingly becoming a worldwide problem (2). Recently, the therapeutic focus has shifted to regenerative techniques that induce angiogenesis. Human bone marrow is a diverse reservoir for several progenitor cell populations, including endothelial progenitor cells (EPCs) (3). The use of progenitor cells (stem cells) for cell-based regenerative therapy is promising because of the high proliferative capacity and multilineage differentiation potential of the progenitor cells and also because of their contribution to angiogenesis or arteriogenesis (4) through the recruitment of EPCs (5) and their functionality and secretion of growth factors (6) and cytokines (7–9) that promote cell survival. Thus, many approaches to therapeutic angiogenesis have been investigated (10–13). We have investigated therapeutic angiogenesis using bone marrow mononuclear cell implantation (BMCI) and have accumulated clinical evidence for different populations (12,14,15). To resolve the issue of the lack of a reliable technique for blood flow analysis at the microcirculation level, one of the aims of this study was to establish a method for analysis of angiogenesis by quantitative radionuclide determination to evaluate blood flow in terms of the target-to-background ratio (TBR), which references the brain count as a control, as we previously reported (12,14,15). A secondary aim was to confirm the location of improved blood flow using the radioisotope examination. Previous reports have evaluated the localization of perfusion using 99mTc-macroaggregated albumin (99mTc-MAA) (16–18). However, the results are difficult to interpret. A third aim of this study was to estimate the sizes of new arteries that are smaller than visible arteries (<200 μm). In this context, we hypothesized that radionuclide assessment after BMCI would be advantageous. 99mTc-MAA has been used almost universally as the perfusion agent for lung scintigraphy. After intravascular injection of 99mTc-MAA, radioisotope particles are lodged in the capillaries and precapillary arterioles of the target vessels in proportion to perfusion (19), and this is less affected by inflammation. 99mTc-MAA perfusion scintigraphy is a suitable method to confirm the presence of angiogenesis-related microvascular blood flow. In this investigation, we performed a quantitative analysis of perfusion, determined blood flow distribution, and estimated vessel size after BMCI using 99mTc-MAA perfusion scintigraphy as well as estimated the diagnostic accuracy.
MATERIALS AND METHODS
Study Design and Participants
We enrolled 46 consecutive patients (mean age ± SD, 59.8 ± 13.7 y; 63% men) with arteriosclerosis obliterans or thromboangiitis obliterans from September 2011 to December 2012 who had rest pain or ischemic ulcer (Fontaine class 3 to 4, Rutherford class III-4 to III-6) for more than 3 mo under standard treatment but were not eligible for bypass surgery or endovascular catheter treatment. Exclusion criteria were active infection confirmed by blood examination or the presence of osteomyelitis; no evidence of angiologic stenosis; vascular surgery within the previous 30 d; active malignancy as determined by endoscopy, tumor marker, or fecal occult blood testing or history of cancer treatment within the past 5 y; untreated proliferative diabetic retinopathy; current smoker; addiction to alcohol or any other drug; evidence of viral infection (HBV, HCV, HIV); complications of any serious disease affecting the patient’s general condition, such as organic brain disease or heart, lung, kidney, or liver failure; and inability to participate in radionuclide imaging studies before and after the BMCI. This study was performed at the Nippon Medical School Hospital and was approved by the Institutional Review Board (ethical committee of Nippon Medical School), and all patients provided written informed consent. The protocol was registered with the University Hospital Medical Information Network-Clinical Trial Registry (UMIN-CTR), which is accepted by the International Committee of Medical Journal Editors (no. UMIN000006166).
BMCI
Bone marrow mononuclear cells were injected in the calf and foot muscles of the ischemic limbs as previously described in detail (14,15). Briefly, bone marrow (400–600 mL) was collected from the bilateral iliac bones under general anesthesia. The mononuclear cell fraction was sorted, and 60–100 mL of the cell suspension were processed by a cell separator (AS-TEC 204; Fresenius Kabi). As bone marrow aspirates were being processed, necrotic tissue was surgically debrided under sterile conditions. Thereafter, the cell suspension (1 mL/point) was injected intramuscularly. Cell injection was performed using guidance from a marked transparent overlay, which helped to ensure that cells were evenly injected, at 1 mL per site, into the entire ischemic area of the below-knee muscles. Finally, skin grafting was performed to cover the ulcers unless there was spontaneous epithelialization of the wound margin.
Flow cytometry was performed with the bone marrow cells for quality analysis of the mononuclear cell count, including EPCs, as described previously (20). Briefly, EPCs were analyzed for the expression of CD34, CD45, CD133, and vascular endothelial growth factor receptor-2 (VEGFR-2) using 4-color flow cytometry (FACSCalibur; BD Biosciences). Samples were incubated with anti-CD34 FITC (Beckman Coulter Inc.), anti-CD45-PerCP (BD Biosciences), anti-CD133/2 (293C3)-APC (Miltenyi Biotec GmbH), and phycoerythrin-conjugated anti–VEGFR-2 (R&D Systems, Inc.) for 40 min at 4°C, followed by erythrolysis via the addition of a lysing reagent, and then washed once with 0.2% phosphate-buffered saline with bovine serum albumin. CD34+ cells were analyzed using sequential gating strategies. A CD45 versus side scatter dot plot was set to include all CD45+ events, and CD45+ events were set to include all nucleated white blood cells and to exclude red blood cells, nucleated red blood cells, platelets, and other cellular debris, which do not express CD45. CD45+ cells were gated on a forward-scatter versus side-scatter dot plot to confirm the mononuclear cell fraction. Mononuclear cells formed a cluster with low side-scatter and low to intermediate forward-scatter. CD34+ and CD45dim cells in the mononuclear cell fraction were gated on a forward-scatter versus side-scatter dot plot to obtain a cluster of true CD45dim CD34+ cells. True CD45dim and CD34+ events were displayed on a CD133 versus VEGFR-2 dot plot, and then the resulting population was examined for the dual expression of VEGFR-2 and CD133. CD45dim/CD34+/CD133+/VEGFR-2+ cells were enumerated in the upper right quadrant of the plot. At least 2,000,000 events were measured in the CD45+ gate. Data were analyzed using CELLQuest (BD Biosciences). The EPC values were defined as the percentage of CD34+, CD45dim, CD133+, and VEGFR-2+ cells per CD34+CD45dim cell fraction.
Clinical Assessment
The visual analog pain scale (mm) and maximum walking distance were evaluated. The visual analog pain scale scored maximal pain as 100 and minimal pain as 0. The maximum walking distance was determined using a standard treadmill test. Specialized personnel supervised the exercise tests. All patients were asked to walk on a treadmill at a speed of 3.1 km/h for a maximum of 5 min. No inclining-plane protocol was used. Patients were encouraged to finish the whole test, but it was stopped when the patient was unable to walk further. The time and walking distance until the occurrence of leg pain and the total walking time and distance were recorded.
Several parameters were evaluated to quantify recovery of local blood flow. The ankle-brachial index (ABI) (Omron Healthcare Co. Ltd.) was measured using standard methods and calculated as the ratio of ankle to brachial pressure. Tissue oxygen content was measured as transcutaneous oxygen tension (TcPO2) with a TCM 400 monitor (Radiometer, Inc.). The transducer was placed on the dorsum of the ischemic limb and warmed to 43.5°C to increase skin permeability to oxygen molecules at the measurement site. Consistent TcPO2 data were collected for approximately 20 min with the patient resting supine and breathing room air.
99mTc-TF radionuclide imaging was performed on 46 patients using a previously reported method (14,15). 99mTc-TF (740 MBq; total volume, 1.25 mL) was injected intravenously. The 99mTc-TF data were used to enable comparison and examination of 99mTc-MAA scintigraphy. 99mTc-MAA imaging analysis was performed for 11 patients who successfully underwent angiography. All other patients who did not undergo angiography were excluded from the 99mTc-MAA study. 99mTc-MAA scintigraphy was performed as follows: a pig-tail catheter was placed in the descending aorta below the renal artery and just above the iliac bifurcation, and 296 MBq of commercial 99mTc-MAA (Nihon Medi-Physics Co., Ltd.) were injected into the artery in an antegrade fashion. The 99mTc-MAA consisted of 1.7 mg of human serum macroaggregated albumin (24 × 104 particles; total volume, 19.8 mL) in which 95% of the 99mTc was bound to the MAA.
Data were acquired in a 256 × 1,024 matrix on the 140-keV photopeak of 99mTc. Approximately 12 min after injection of the radiotracer, whole-body scintigraphy was performed with the patient prone in both anterior and posterior projections with a dual-head large-field-of-view γ-camera (ADAC Vertex; Philips). Each head of the γ-camera was equipped with a low-energy, high-resolution collimator. The scan speed was 120 mm/min, and the image acquisition time was approximately 15 min. The data were averaged for quantitative analysis. To analyze the data acquired from 99mTc-TF and 99mTc-MAA scintigraphy, regions of interest of equal surface area were drawn around the appropriate muscle group (calf muscles and foot) in the anterior and posterior projections. After the radionuclide count within the regions of interest was determined, intracranial (brain) uptake was calculated as the background. The TBR was defined as the average counts per pixel in each muscle/the average counts per pixel in the brain. Examinations were performed before and at 4 wk after therapy. To avoid bias, the actual change in blood flow was analyzed by subtracting the pixel count of the untreated limb from that of the treated limb. Granulometric analysis of 99mTc-MAA microparticles was performed by a laser diffraction particle size analyzer (Sald-7000; Shimadzu Scientific Instruments), and the diameter was visually confirmed under a microscope after staining with a 1% 4,5,6,7-tetrachloro-2′,4′,5′,7′-tetraiodofluorescein solution. Samples from 3 lots were analyzed to determine these measurements and averaged. Granulometric analysis was performed by FujiFilm RI Pharma Co., Ltd. All data were collected retrospectively.
Patients were monitored for major adverse cardiovascular events until 4 wk after BMCI. Major adverse cardiovascular events were defined as all-cause mortality, nonfatal myocardial infarction (including silent myocardial infarction), stroke, acute coronary syndrome, and endovascular or surgical intervention on the coronary or leg arteries. In addition, patients were followed for 1 y to monitor for amputation-free limb survival and major adverse events.
Statistical Analysis
Exact 2-sided 95% confidence intervals (CIs) were evaluated using a binominal distribution. The association between BMCI and the untreated side was examined using 2-way repeated-measures ANOVA. Within-treatment analyses of changes were performed using a Wilcoxon rank-sum test. Cohen’s κ coefficient analysis was used to test for better-than-chance agreement between 2 observers (radiologists). For intraobserver comparisons, at least 2 examinations from each patient were assessed by each observer, and the observers were masked to the patient’s clinical condition.
Considering the high rate of limb amputations in the nontreatment group, untreated limbs in treated patients were used as controls. The sensitivity and specificity of radioisotope detection were calculated with TcPO2 threshold against limb amputation as the standard and used to determine likelihood ratios. For a positive change in the TBR, the likelihood ratio was calculated as sensitivity/1 – specificity; for a negative change in the TBR, the likelihood ratio equaled 1 – sensitivity/specificity. A 95% CI was calculated for every measure. The amputation-free limb survival rate and the occurrence of major adverse events within the 1-y follow-up period were assessed using a χ2 analysis. A P value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS statistics software (version 20; IBM Corp.).
RESULTS
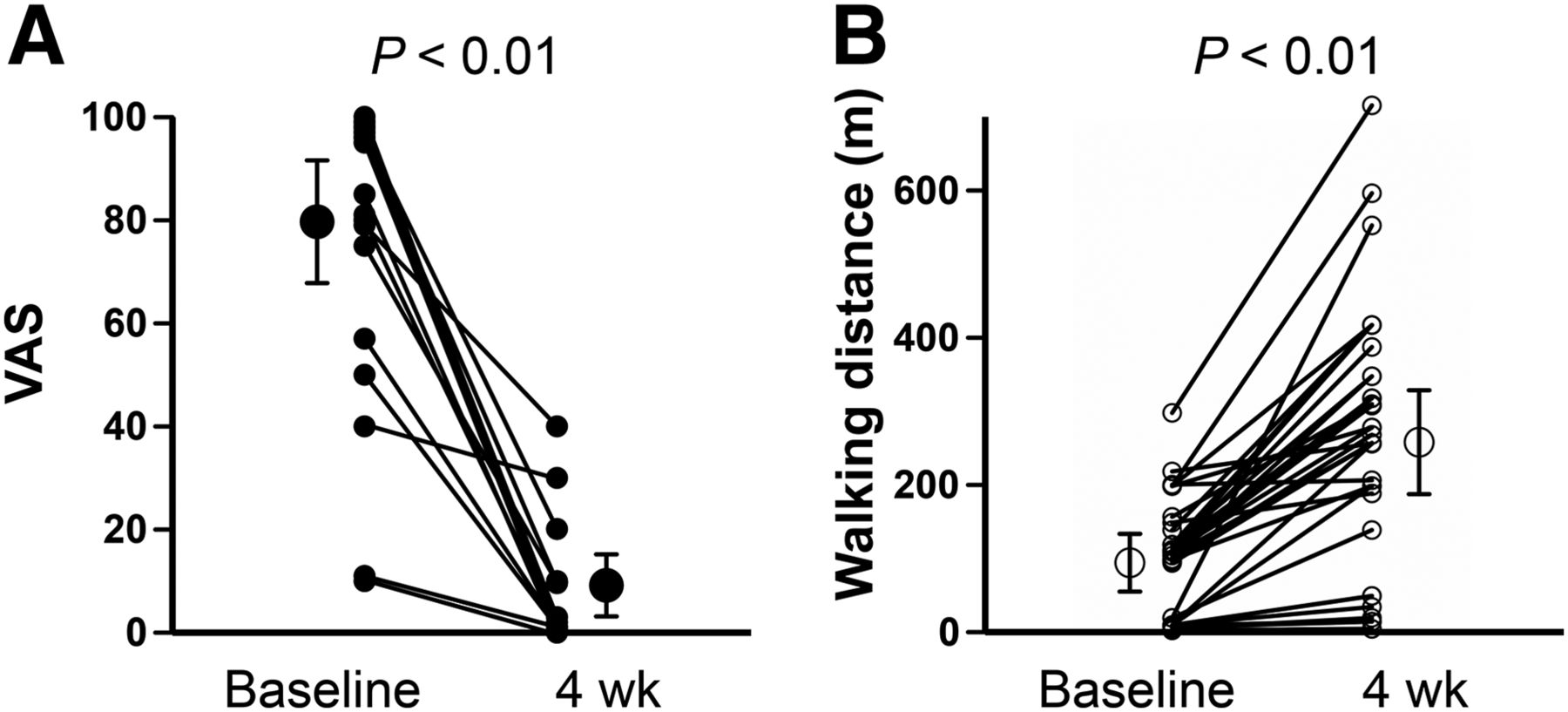
The baseline characteristics of the study participants are shown in Table 1. Improvements were seen in the indicators of clinical effectiveness. The visual analog pain scale decreased significantly, from 79.7 ± 23.8 at baseline to 9.2 ± 12.0 at 4 wk after BMCI (P < 0.01), and maximum walking distance increased significantly, from 94.3 ± 78.5 to 258.0 ± 141.1 m (P < 0.01) (Fig. 1). Skin perfusion increased significantly 4 wk after BMCI, as indicated by a change in TcPO2 from 20.4 ± 14.4 at baseline to 36.0 ± 19.8 mm Hg at 4 wk (P < 0.01), whereas the ABI did not change significantly (0.65 ± 0.30 to 0.76 ± 0.24, P = 0.07) (Fig. 2). ABI in the nontreated leg indicated no significant changes (0.86 ± 0.28 to 0.89 ± 0.27, P = 0.65).
Patient Characteristics

Visual analog scale (VAS) and maximum walking distance. Graphs show significant improvement in VAS score (A) and maximum walking distance (B) at 4 wk after therapy.

TcPO2 and ABI. TcPO2 (A) was significantly improved 4 wk after therapy. However, there was no significant change in ABI (B).
In the assessment of angiogenesis by radionuclide imaging (representative images are shown in Fig. 3), significant increase in the 99mTc-TF score was seen in the foot region in both the treated limb (0.60 ± 0.23 to 0.77 ± 0.29 count ratio/pixel, P < 0.01, Fig. 4A) and the untreated limb (0.64 ± 0.20 to 0.70 ± 0.24 count ratio/pixel, P = 0.04, Fig. 4A). The scores were changed significantly in the lower leg region at 4 wk after BMCI (treated limb, 1.03 ± 0.27 to 1.18 ± 0.38, P < 0.01; untreated limb, 1.01 ± 0.28 to 1.16 ± 0.34, P < 0.01, Fig. 4B). On the other hand, the 99mTc-MAA score was improved significantly in the foot region of the treated limb at 4 wk after treatment (5.21 ± 3.56 to 10.33 ± 7.18 count ratio/pixel, P = 0.02, Fig. 4C), compared with the untreated side (3.82 ± 1.63 to 6.05 ± 6.07, P = 0.33, Fig. 4C), but not in the lower leg region (treated limb, 5.28 ± 3.63 to 11.79 ± 10.22, P = 0.09; untreated limb, 6.17 ± 4.40 to 10.85 ± 8.90, P = 0.09, Fig. 4D). The interaction between the BMCI-treated side and the untreated side were compared (Fig. 4). There were significant interactions in the TBR in the foot region for both 99mTc-TF (P = 0.01, 2-way repeated-measures ANOVA between the 2 regions, Fig. 4A) and 99mTc-MAA (P = 0.01, 2-way repeated-measures ANOVA between the 2 regions, Fig. 4C). However, no interaction was observed in the lower leg region for 99mTc-TF (P = 0.94, 2-way repeated-measures ANOVA between the 2 limbs, Fig. 4B) or 99mTc-MAA (P = 0.31, 2-way repeated-measures ANOVA between the 2 regions, Fig. 4D). The net gain in blood flow (Fig. 5) was calculated by subtracting the pixel count of the untreated limb from that of the treated limb and is expressed as a normalized score. The normalized 99mTc-TF score in the foot region improved significantly after BMCI (−0.04 ± 0.26 to 0.08 ± 0.32, P = 0.04, Fig. 5A), but no improvement was observed in the lower leg region (0.01 ± 0.20 to 0.01 ± 0.26, P = 0.97, Fig. 5B). In addition, the normalized 99mTc-MAA score in the foot region improved significantly (1.49 ± 3.64 to 5.59 ± 4.84, P = 0.04, Fig. 5C), but no significant changes were observed in the lower leg region (−0.17 ± 4.36 to 1.55 ± 5.14, P = 0.45, Fig. 5D). There was no difference in TBR associated with disease type.
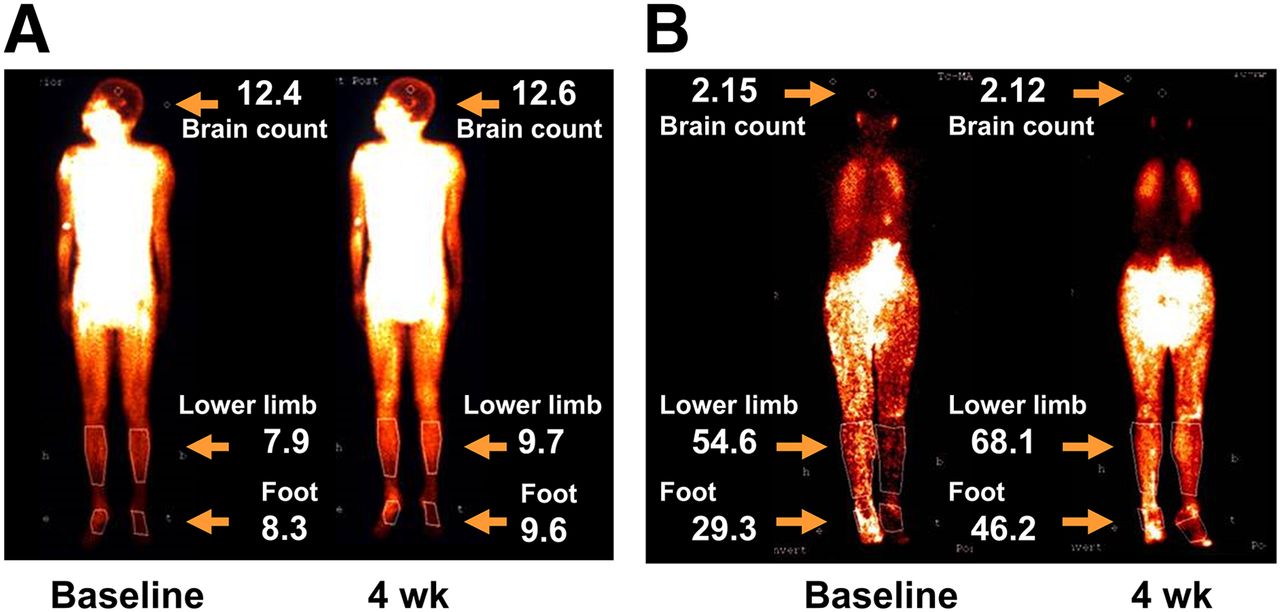
Representative radioisotope images of angiogenesis using 99mTc-TF and 99mTc-MAA perfusion scintigraphy. (A) Representative 99mTc-TF study from patient who underwent BMCI in ischemic left leg. (B) Representative 99mTc-MAA study in patient who underwent BMCI in ischemic right leg.
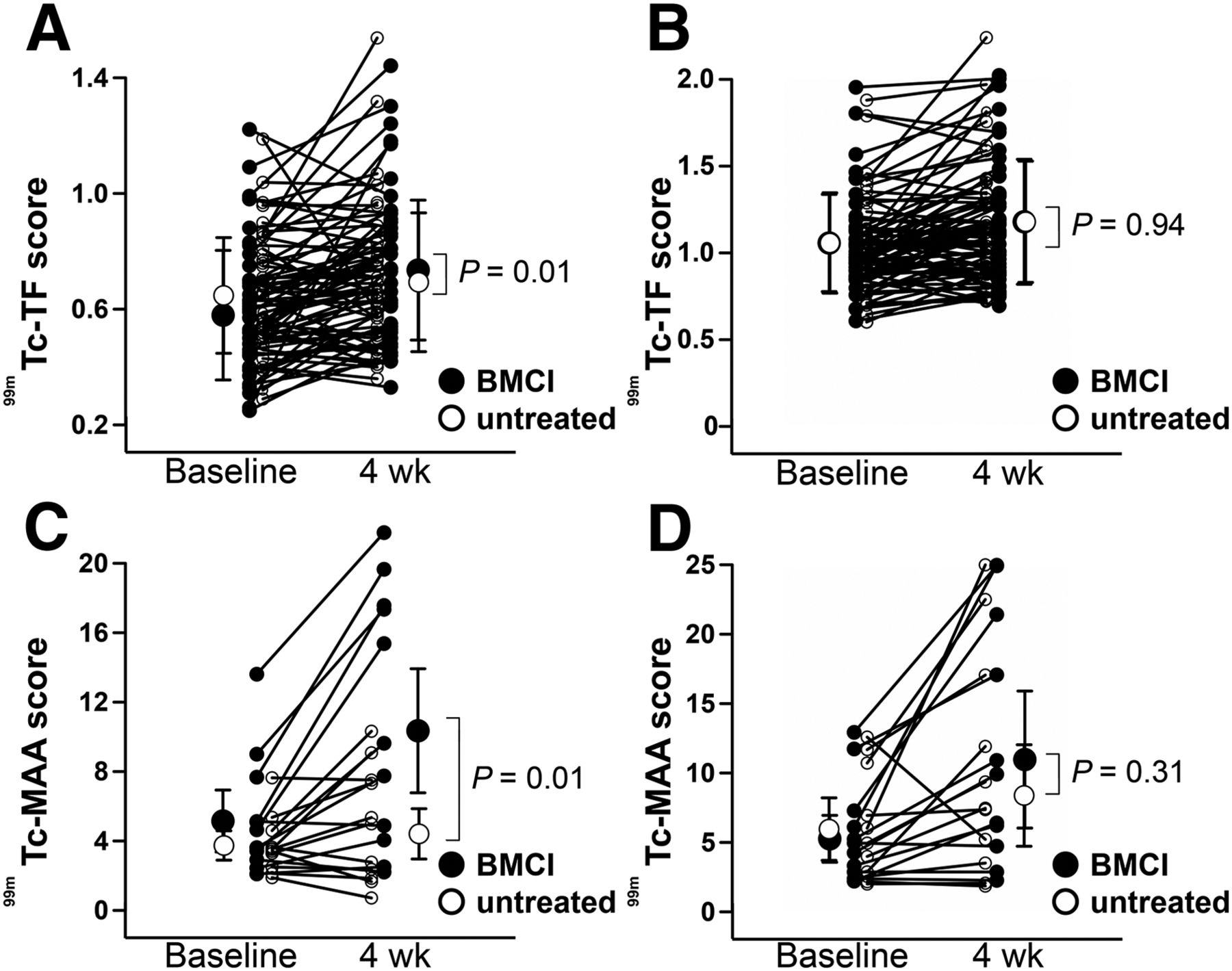
Quantitative radionuclide scores from treated and untreated limbs. A and C indicate foot region, and B and D indicate lower leg region. (A and B) 99mTc-TF perfusion scintigraphy score before and at 4 wk after BMCI. There was significant improvement in foot region of BMCI-treated leg, compared with untreated limb (A), but not in lower leg region (B). (C and D) 99mTc-MAA perfusion scintigraphy scores before and at 4 wk after BMCI. There was significant improvement in foot region of BMCI-treated leg, compared with untreated limb (C), but not in lower leg region (D).

Normalized radionuclide scores from treated and untreated limbs. A and C show results from foot region, and B and D show lower leg region. (A and B) 99mTc-TF perfusion scintigraphy scores before and 4 wk after BMCI. There was significant improvement at 4 wk after BMCI in foot region, compared with untreated limb (A), but not in lower leg region (B). (C and D) 99mTc-MAA perfusion scintigraphy scores before and at 4 wk after BMCI. There was significant improvement in the foot region after BMCI, compared with untreated limb (C), but not in lower leg region (D).
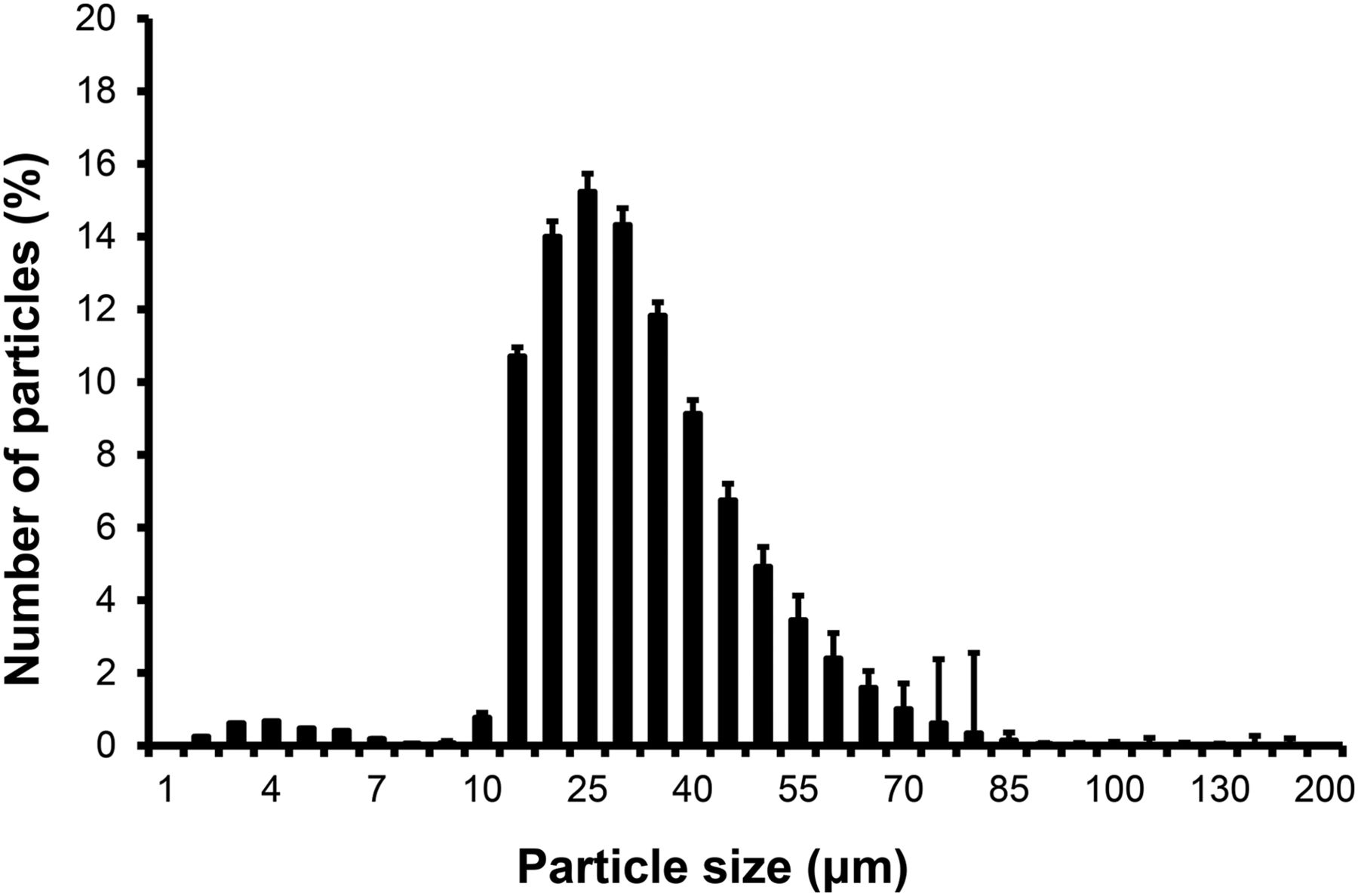
Regarding the reliability of the TBR assessment, the linear-weighted κ values indicated a moderate interobserver agreement of 0.710 and intraobserver agreement of 0.667 for 99mTc-TF, determined after rounding the numeric data to 1 decimal place. Amputation thresholds of TcPO2 and improvement in TBR were assessed at the 4-wk evaluation (χ2 test; P = 0.64 for 99mTc-TF and P = 0.024 for 99mTc-MAA). The sensitivity, specificity, positive predictive value, negative predictive value, and predictive accuracy for 99mTc-TF and 99mTc-MAA are shown in Table 2. The granulometric distribution of 99mTc-MAA displayed a mean particle size of 25.83 μm, and 92.7% of particles were within 10–60 μm (Fig. 6).
Diagnostic Accuracy and Areas Under Receiver-Operator Characteristic Curve

Particle size distribution patterns of 99mTc-MAA microspheres.
No adverse events occurred during the 4-wk follow-up period. All patients had healed ulcers, and all were able to use the affected foot at discharge. There were 3 major limb amputations and 1 death during the 1-y follow-up period (mean follow-up, 319 d; 95% CI, 291–347). The overall limb salvage rate was 93.5% (mean follow-up, 317 d; 95% CI, 287–348), and the major adverse cardiovascular event-free rate was 93.5% (mean follow-up, 309 d; 95% CI, 274–344). The cutoff value of Δ 99mTc-TF was 0.11 (determined by receiver-operator characteristic curve), and Kaplan–Meier analysis (P = 0.005 by log-rank test) against leg amputation showed significant differences (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). The cutoff for 99mTc-MAA was not included because no leg amputation was observed in this group.
DISCUSSION
In this study, we identified a reliable means of quantitative analysis of therapeutic angiogenesis after BMCI. To reduce the effect of confounding variables that relate to bilateral limb condition, such as improvements in walking distance and nutritional status (Fig. 1), normalized values were calculated by subtracting the untreated limb count (as an internal control) to confirm the clinical effects of BMCI, and the results showed statistically significant improvement in the foot region on both 99mTc-TF and 99mTc-MAA scintigraphy (Fig. 5). We also examined regional recovery after BMCI using specific regions of interest in the lower leg and foot region and successfully showed the regional differences. Furthermore, the scores of both 99mTc-TF (reference diameter of average triclinic crystal structure size, 1.25 nm) (21) and 99mTc-MAA (reference diameter of average microsphere size, 25 μm) showed improvement at 4 wk after BMCI, providing direct evidence that mature arterial growth was promoted in the ischemic foot area in the 4 wk after BMCI. Blood flow analysis by skin perfusion pressure and TcPO2 have also been useful parameters in several therapeutic angiogenesis protocols (12,14,15,22,23). 99mTc-TF scintigraphy is a useful examination for detection of early phase angiogenesis, as we have reported previously (14,15). However, the specificity is lower than that of 99mTc-MAA, which likely implies that a local inflammatory reaction, such as osteomyelitis or phlebitis (14,15), results in a large SD, even in the foot region, when compared with 99mTc-MAA (Figs. 4A and 5A). Concerning the feasibility of the examination, 99mTc-TF is useful because it can be performed at the outpatient screening, whereas 99mTc-MAA requires intraaortic injection. However, 99mTc-MAA can be performed at the time of diagnostic digital subtraction angiography.
Several limitations of this study deserve mention. Some of the ABI data were indicators of severity of disease. Most of the patients had calcified arteries that made it difficult to obtain correct pressure measurements or to detect ischemia localized only in the foot region. Also, other parameters, such as the skin perfusion pressure or toe pressure, could not be measured because of the location of the ulcers. Nonetheless, tissue ischemia was confirmed by several different modalities, consistent with our previous observations (15). The sample size of patients receiving 99mTc-MAA scintigraphy was small, and data for patients with both arteriosclerosis obliterans and thromboangiitis obliterans were included in the data analysis. Thus, it will be important to confirm these results with a large-scale investigation in a uniformly affected population.
CONCLUSION
Radionuclide determination of quantitative score, flow distribution, and vascular size with 99mTc-MAA appears to be a useful method to evaluate functional blood flow recovery after BMCI. Thus, it may be a reliable approach to confirm therapeutic angiogenesis in the clinical setting. Furthermore, the radionuclide approach is applicable for other angiogenesis protocols such as those using growth factors, genes, or pluripotent stem cells.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by JSPS KAKENHI (Grants-in-Aid for Scientific Research, nos. 20590844 and 24591075) and a Mitsukoshi Health and Welfare Foundation grant. Naoki Seki is an employee of FUJIFILM RI Pharma Co., Ltd. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Harumi Ohtsubo for technical assistance.
Footnotes
Published online Nov. 5, 2015.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 22, 2015.
- Accepted for publication October 19, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}