


Abstract
Imaging plays a critical role in the management of pheochromocytomas and paragangliomas and often guides treatment. The discovery of susceptibility genes associated with these tumors has led to better understanding of clinical and imaging phenotypes. Functional imaging is of prime importance because of its sensitivity and specificity in subtypes of pheochromocytoma and paraganglioma. Several radiopharmaceuticals have been developed to target specific receptors and metabolic processes seen in pheochromocytomas and paragangliomas, including 131I/123I-metaiodobenzylguanidine, 6-18F-fluoro-l-3,4-dihydroxyphenylalanine, 18F-FDG, and 68Ga-DOTA-somatostatin analogs. Two of these have consequently been adapted for therapy. This educational review focuses on the current imaging approaches used in pheochromocytomas and paragangliomas, which vary among clinical and genotypic presentations.
The World Health Organization defines paragangliomas as neuroendocrine tumors that originate in neural crest tissue (1). Most commonly, they arise in the adrenals and are called pheochromocytomas, whereas those outside the adrenals are called extraadrenal paragangliomas. Most parasympathetic paragangliomas arise in the head and neck (head and neck paraganglioma, or HNPGL), whereas most of sympathetic origin arise below the diaphragm. Most pheochromocytomas and paragangliomas are apparently benign, whereas 2%–26% develop metastases (2). Histopathology cannot differentiate between benign and malignant disease; therefore, the World Health Organization uses the term metastatic rather than malignant. Metastatic disease is defined by tumor presence in sites (e.g., lymph nodes and bones) where chromaffin cells or paraganglia are not normally present (2).
Classically, pheochromocytoma presents with hypertension, headaches, palpitations, pallor, sweating, and anxiety, whereas paraganglioma frequently presents with pain or mass effect (3). Biochemical phenotype (secretion patterns: norepinephrine, epinephrine, and dopamine and their metabolites) is reflective of genotype (4). Pheochromocytomas and paragangliomas may be biochemically silent in over 10% of cases (2), and a fraction present as incidentalomas (3).
GENETICS
Pheochromocytomas and paragangliomas are the group of tumors most frequently associated with genetic mutation. Driver mutations, fusion genes, or copy number alterations are identified in 95% of patients, with more than 20 germline or somatic gene mutations identified (5). Mutations in SDH (A/B/C/D/AF2), collectively SDHx, are most frequently encountered. Mutational status has implications for clinical, biochemical, and imaging phenotype. For example, VHL, RET, NF1, MAX, TMEM12, and HRAS mutations most often present with pheochromocytomas, whereas SDHx, FH, PHD1/2, and EPAS1/HIF2A mutations most often present with paraganglioma. Sporadic pheochromocytomas and paragangliomas often have somatic mutations in NF1, VHL, RET, and MAX (5). Three pheochromocytoma/paraganglioma clusters have been described: cluster 1, a pseudohypoxia cluster affecting hypoxia-signaling pathway (SDHx, FH, VHL/EPAS1); cluster 2, a tyrosine kinase signaling cluster (RET, NF1, TMEM127, MAX, HRAS); and cluster 3, a Wnt signaling cluster (CSDE1, MAML3) (5). Genetic testing is now recommended for all patients with pheochromocytoma or paraganglioma.
IMAGING MODALITIES
The role of imaging in pheochromocytoma and paraganglioma includes confirming the diagnosis when biochemical results are positive or borderline; defining the location, extent, and optimal approach to surgery; evaluating for multifocal or metastatic disease (staging); evaluating response to treatment (restaging); performing surveillance screening for the presence or recurrence of disease; and selecting suitable patients for theranostic applications (90Y/177Lu-DOTA-somatostatin analog [SSA] or 131I-metaiodobenzylguanidine [MIBG] therapy). Imaging modalities include anatomic imaging—principally CT and MRI—and functional imaging that relies on physiologic processes or receptor targeting. This continuing education review focuses on imaging modalities that are currently approved or are widely available for pheochromocytoma and paraganglioma.
131I/123I-MIBG
Radiolabeled MIBG (131I/123I-MIBG, iobenguane) binds to norepinephrine transporters, which are internalized and shuttled into secretory granules via vesicular monoamine transporters (6).
Patient Preparation, Administration, Pharmacokinetics, Biodistribution, and Dosimetry
Procedure guidelines for imaging pheochromocytoma or paraganglioma with 123I/131I-MIBG have been published (7). Before injection, it must be established that the patient has not taken pharmaceuticals that interfere with MIBG (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). Because free 123I/131I may be released, thyroid protection is performed, most commonly using a saturated solution of potassium iodide 2–24 h before injection of MIBG and continued for several days thereafter.
123I-MIBG is preferable for imaging (8), whereas 131I-MIBG is reserved for dosimetry before therapy or documenting posttherapy biodistribution. Administered activity and dosimetry are presented in Supplemental Table 1. After administration of MIBG, blood clearance occurs quickly, with whole-body excretion of more than 80% in 2–5 d, predominantly through the kidneys (9). Normal biodistribution includes uptake in the liver, lungs, heart, spleen, and salivary glands (Fig. 1). The adrenals are often visualized, and in the absence of CT abnormalities, uptake at or below the level in the liver is considered physiologic.
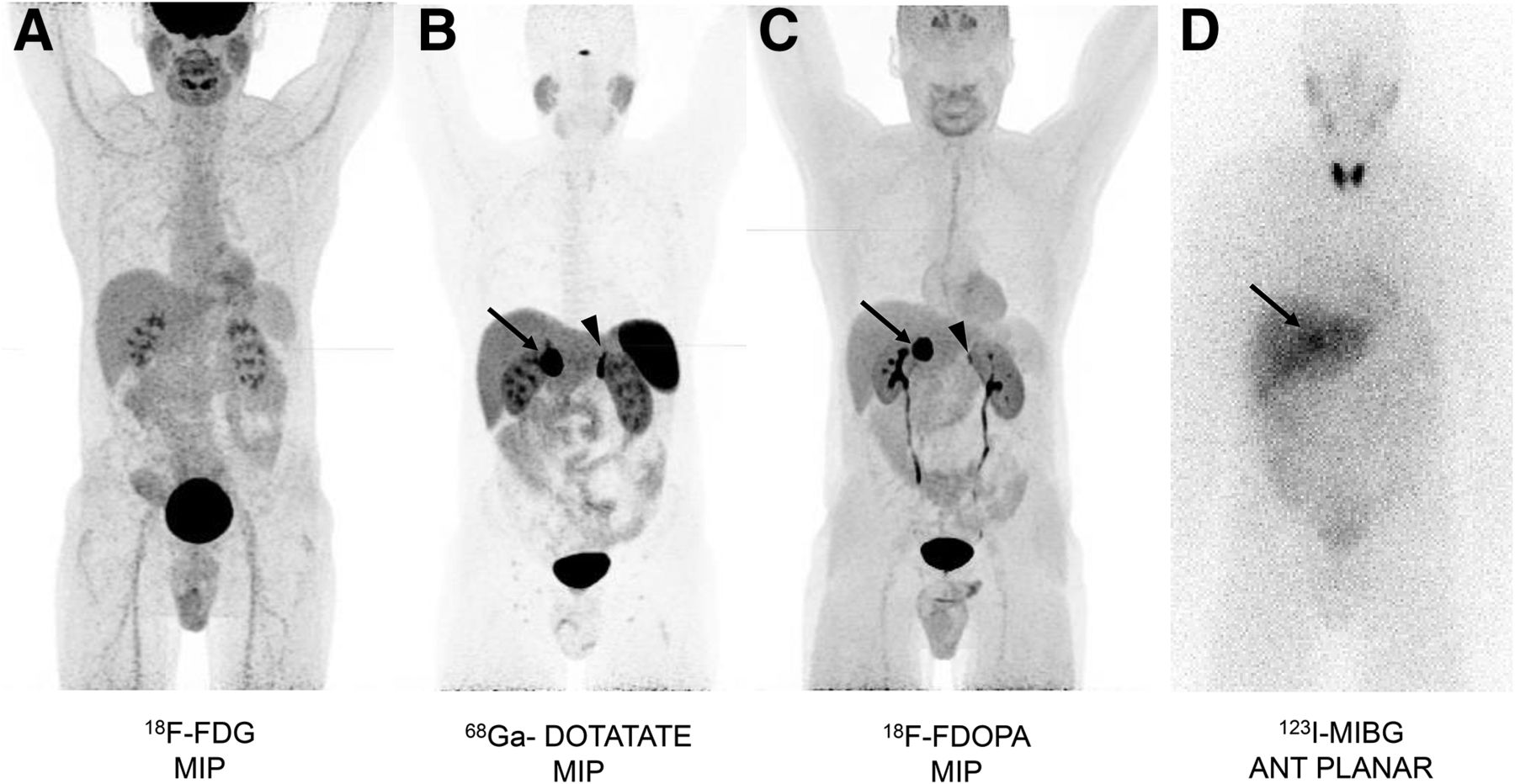
A 54-y-old man with benign sporadic right adrenal pheochromocytoma (arrows). (A) Maximum-intensity-projection (MIP) 18F-FDG PET scan (SUVmax, 3.7) showing physiologic brain uptake; urinary excretion; and mild activity in blood pool, cardiac wall, salivary glands, and gastrointestinal tract. (B) MIP 68Ga-DOTATATE PET scan (SUVmax, 75.5) showing prominent uptake in spleen, kidneys, liver, and pituitary; low-level uptake in salivary glands and thyroid; and prominent normal left adrenal (arrowhead). (C) MIP 18F-FDOPA PET scan (SUVmax, 23) showing uptake in basal ganglia; low-level uptake in esophagus and cardiac wall; normal left adrenal (arrowhead) and gastrointestinal tract; and excretion through kidneys and bladder. (D) Anterior 123I-MIBG planar scan at 24 h showing uptake in pheochromocytoma (arrow) (greater than liver level) and in thyroid, despite blockade; mild uptake in pheochromocytoma (arrow) in liver, salivary glands, and cardiac wall; and faint excretion into bladder and gastrointestinal tract.
Clinical Results
A metaanalysis found an123I-MIBG sensitivity of 96% in patients with nonmetastatic pheochromocytoma or paraganglioma and 79% in patients with metastatic pheochromocytoma or paraganglioma (10). Recent studies that include more cases of paraganglioma found an overall lower sensitivity in MIBG detection, especially in hereditary pheochromocytoma or paraganglioma (Tables 1 and 2). The per-lesion sensitivity in metastatic pheochromocytoma or paraganglioma is frequently less than 60% (11–16), although several studies show a higher per-patient sensitivity of 80%–92% (17–20). These differences may be related to different patient populations or methodologic differences. Typically, 123I-MIBG sensitivity is higher for detecting pheochromocytoma than for detecting paraganglioma, at 88% and 67%, respectively (21). Others report sensitivity of 76%–92% for pheochromocytoma and 35%–70% for paraganglioma (3,11,17,22,23). MIBG sensitivity in patients with SDHx is low (14,24). With newer radiopharmaceuticals, the once pivotal role of radiolabeled MIBG in pheochromocytoma/paraganglioma imaging has diminished to screening for 131I-MIBG therapy.
Sensitivity of Detection of Benign Pheochromocytoma and Paraganglioma (n ≥ 20 Patients or Prospective Studies)
Sensitivity of Detection of Metastatic Pheochromocytoma and Paraganglioma (n ≥ 20 Patients or Prospective Studies)
18F-FDOPA
6-18F-fluoro-l-3,4-dihydroxyphenylalanine (18F-FDOPA, IASOdopa; IASON GmbH) is a radiolabeled amino acid developed as a marker of dopamine synthesis for Parkinson disease or neuroendocrine tumors and approved by the European Medicines Agency and the U.S. Food and Drug Administration but limited in availability in the United States. 18F-FDOPA is transported into target cells via the large neutral amino acid transporter-1, after which it is decarboxylated to 18F-fluorodopamine, which is sequestered into secretory vesicles via vesicular monoamine transporters or degraded by other enzymes.
Patient Preparation, Administration, Pharmacokinetics, Biodistribution, and Dosimetry
Procedure guidelines for 18F-FDOPA have been published (25,26). No medications have been reported to interfere with imaging. Carbidopa, a peripheral decarboxylation blocking agent, improves uptake in pheochromocytoma and paraganglioma (27), although its use has not been incorporated by all groups (28).
The administered activity and dosimetry are presented in Supplemental Table 1. Pharmacokinetics and biodistribution studies of 18F-FDOPA (29) show rapid blood clearance, with most tumor uptake occurring within 30 min of administration (27). Physiologic uptake occurs in the basal ganglia, liver, and pancreas (Fig. 1). Mild uptake is seen in the bowel and esophagus. The low uptake of 18F-FDOPA in the normal adrenal (mean SUVmax, 1.9) is advantageous compared with the prominent uptake of 123I-MIBG (30).
Clinical Results
The utility of 18F-FDOPA in pheochromocytoma/paraganglioma imaging is presented in Tables 1 and 2. A metaanalysis of pheochromocytoma and paraganglioma demonstrated pooled 18F-FDOPA PET/CT sensitivities and specificities of 91% and 79%, respectively, on a per-patient basis and 95% and 95%, respectively, on a per-lesion basis (31). Table 1 shows 18F-FDOPA to have a high sensitivity (85%–100%) that outperforms MIBG in benign pheochromocytoma. The sensitivity of 18F-FDOPA for benign pheochromocytoma (94%) is better than that for benign sympathetic paraganglioma (70%) (32). The sensitivity for detecting metastatic pheochromocytoma can be more than 90% (23,33,34) in non-SDHx metastatic pheochromocytoma, although other reports show sensitivity of 81% in benign disease and 45% in malignant disease, for which many lesions may be missed (Fig. 2) (11).

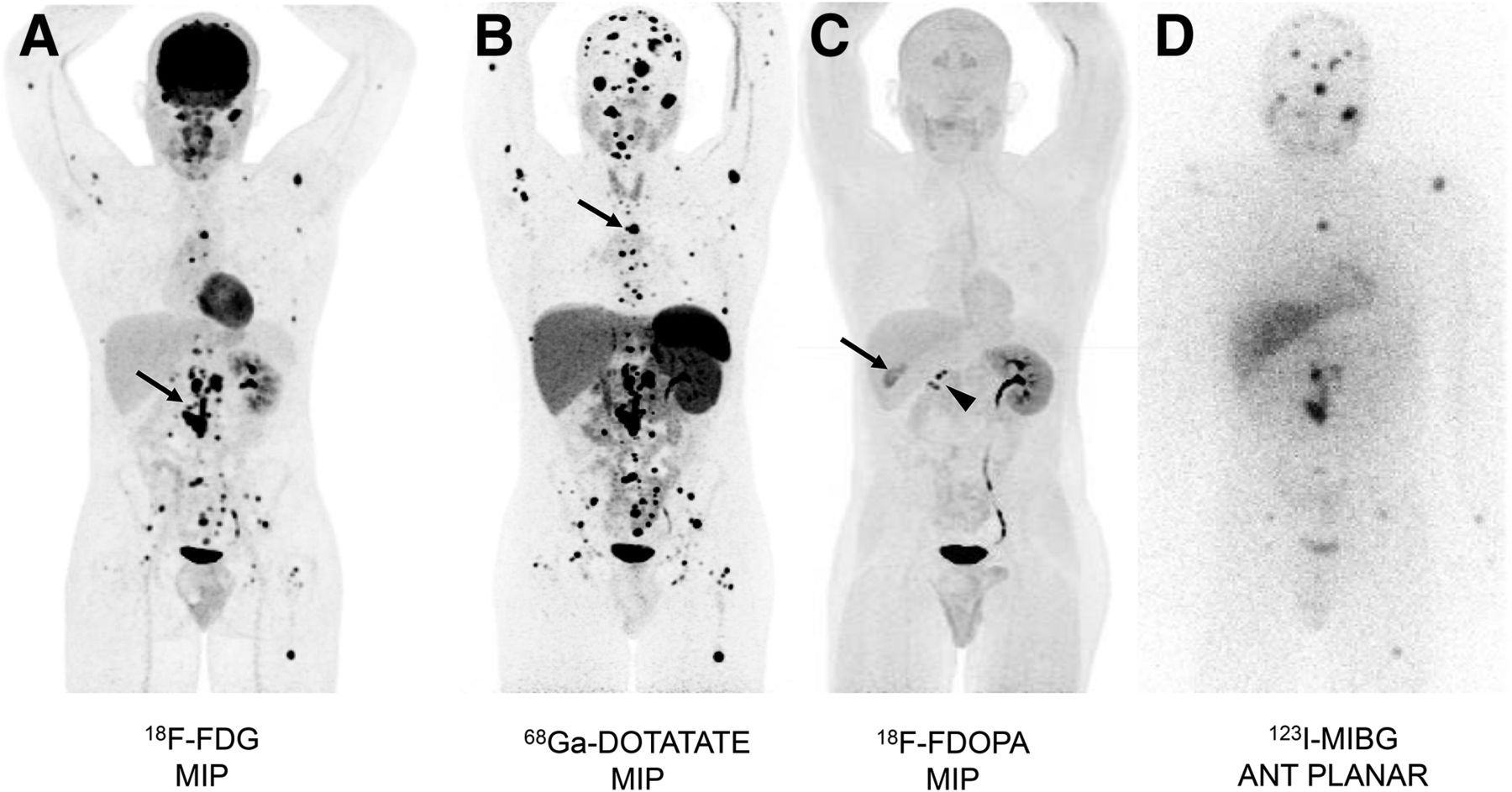
A 20-y-old man with SDHB-associated metastatic paraganglioma. (A) Maximum-intensity-projection (MIP) 18F-FDG PET scan showing excellent uptake in bones and retroperitoneal metastases (SUVmax, 54) (arrow), with fewer lesions than on 68Ga-DOTATATE PET. (B) MIP 68Ga-DOTATATE PET scan showing highest contrast and number of lesions of any of the imaging modalities (SUVmax, 94) in bone metastasis (arrow). (C) MIP 18F-FDOPA PET scan showing negative findings, with some physiologic uptake in gallbladder (arrow) and urinary excretion in right atrophic kidney (arrowhead). (D) Anterior 123I-MIBG planar scan showing uptake in limited number of known metastases.
In summary, 18F-FDOPA has high sensitivity for detecting benign pheochromocytoma or paraganglioma and metastatic pheochromocytoma (sporadic or associated with non-SDHx mutations), but the sensitivity is lower for metastatic paraganglioma. Procedure guidelines recommend the use of 18F-FDOPA in the workup for nonmetastatic pheochromocytoma and paraganglioma (35). Recent work with 68Ga-DOTA-SSA shows that in HNPGL, in metastatic sporadic pheochromocytoma or paraganglioma, and in metastatic SDHx-related pheochromocytoma or paraganglioma, the sensitivity of 68Ga-DOTA-SSA imaging surpasses that of 18F-FDOPA and other reagents.
18F-FDG
18F-FDG is a surrogate marker of glucose metabolism. Entry into tumor is mediated by glucose transporters, typically transporter-1, after which hexokinase-2 phosphorylates it and it becomes a trapped marker.
Patient Preparation, Administration, Pharmacokinetics, Biodistribution, and Dosimetry
Procedure guidelines for 18F-FDG apply to patients with pheochromocytoma or paraganglioma (25,36). Patient preparation, administered activity, and dosimetry results are shown in Supplemental Table 1. The normal distribution includes uptake in the brain, urinary tract, liver, and spleen, as well as variable cardiac and bowel uptake (Fig. 1). Normal adrenals have less uptake than liver (mean SUVmax, 1.6) (14).
Clinical Results
The utility of 18F-FDG in pheochromocytoma/paraganglioma imaging is presented in Tables 1 and 2. A metaanalysis found 18F-FDG to have a sensitivity of 85% and a specificity of 55% for metastatic pheochromocytoma and paraganglioma (37). One study identified new lesions that impacted management beyond the use of conventional imaging modalities in 15% of cases (38).
18F-FDG uptake in pheochromocytoma and paraganglioma varies: in cluster 1 tumors, there is a mean SUVmax of 13.0 ± 6.5 due to activation of hypoxia-signaling pathways, compared with 3.9 ± 3.1 for cluster 2 tumors and 9.0 ± 7.2 for mutation-negative tumors (20). The sensitivity of 18F-FDG was only 40% in patients with multiple endocrine neoplasia type 2–associated pheochromocytoma (cluster 2) (14).
For benign pheochromocytoma and paraganglioma tumors, 18F-FDG has variable sensitivity that is often lower than or similar to the sensitivity of MIBG (Fig. 1). In an early study, the sensitivity of 18F-FDG in tumor detection was 58%, compared with 83% for MIBG (18). In separate reports including nonmetastatic pheochromocytoma and paraganglioma, 18F-FDG had a sensitivity of between 76.8% and 88.0% (11,14).
18F-FDG frequently outperforms MIBG in detecting metastatic disease (33,39), with up to 90% of MIBG-negative lesions positive on 18F-FDG (Fig. 2) (15). In metastatic pheochromocytoma and paraganglioma, the sensitivity of 18F-FDG ranges from 51% to 100% and is usually more than 80% (11,14,15,24,39,40). This wide variability is likely due to the varying characteristics of the patient population being studied and the presence or absence of specific genetic mutations, as well as differences in the gold standard considered (Table 2). In a prospective study, Timmers et al. (24) were the first to report the superiority of 18F-FDG in imaging patients with SDHB mutation, where per-region sensitivity for metastatic disease was 97%, compared with 65% for 123I-MIBG, 50% for 111In-pentetreotide, and 83% for bone scans. Subsequent studies have confirmed the high sensitivity of 18F-FDG in SDHx patients, ranging from 79.4% to 100% (11,13,20,41–44). For this reason, 18F-FDG was the preferred modality for metastatic disease, particularly SDHx, for which it had a sensitivity of 83%–92%, compared with 62% for non-SDHx tumors (11,42). Yet as discussed below, this recommendation preceded the evaluation of 68Ga-DOTA-SSA.
68GA-DOTA-SSA
Somatostatin, a 14-amino-acid peptide hormone, binds to somatostatin receptors (SSTRs 1, 2, 3, 4, and 5). In vitro, pheochromocytoma and paraganglioma tumors express predominantly SSTR 2 and SSTR 3 (45,46).
Although 111In-pentetreotide was the first SSA approved for imaging NETs, it has been supplanted by DOTA-SSA, which has a stronger chelate and is labeled with 68Ga, a positron emitter with a 68-min half-life. 68Ga-DOTA-SSAs include DOTATOC (SSTRs 2 and 5), DOTANOC (SSTRs 2, 3, and 5), and DOTATATE (SSTR 2) (47). 68Ga-DOTATATE (Netspot; Advanced Accelerator Applications) is approved by the Food and Drug Administration and by the European Medicines Agency. This review will focus on 68Ga-DOTA-SSA, with emphasis on 68Ga-DOTATATE since it is the most widely used in pheochromocytoma/paraganglioma imaging, recognizing that 68Ga-DOTATOC is also effective and that 64Cu-DOTATATE (Detectnet; Curium) is probably a suitable alternative, although there are no published reports on pheochromocytoma or paraganglioma (Supplemental Table 1). Existing guidelines that recommend 18F-FDG imaging may be outdated by current practice, given clinical understanding of the superiority of 68Ga-DOTA-SSA.
Patient Preparation, Administration, Pharmacokinetics, Biodistribution, and Dosimetry
Procedure guidelines for 68Ga-DOTA-SSA have been published (25,26). The recommendations to discontinue SSAs are likely unnecessary (Supplemental Table 1). Administered activity, special considerations, and dosimetry are presented in Supplemental Table 1. The biodistribution of 68Ga-DOTATATE/TOC has been reported (48). Clearance from the blood is rapid. Renal clearance predominates. Prominent uptake occurs in the spleen, kidney, adrenal glands, pituitary gland, and liver (Fig. 1), with minor differences between analogs (48). Most tumor uptake occurs by 30 min after injection. Low uptake is seen in the salivary glands and thyroid. 68Ga-DOTATATE SUVmax is higher in normal adrenals (range, 16.4–20.3) than in benign adenomas (range, 6.3–11.8) (49). In contrast, paraganglioma have a mean SUVmax of 94.2 (range, 33.15–155.2).
Clinical Results
The utility of 68Ga-DOTA-SSA in pheochromocytoma/paraganglioma imaging is presented in Tables 1 and 2. 68Ga-DOTA-SSA studies have shown excellent lesion-based sensitivity in detecting pheochromocytoma and paraganglioma, often more than 92% (16,40,50). Recent publications suggest that 68Ga-DOTA-SSA provides a high detection rate across a wide range of mutations (34,44,51,52). A metaanalysis comparing the sensitivity of 18F-FDG and 68Ga-DOTA-SSA found that the sensitivity of 68Ga-DOTA-SSA (95%) was superior to that of 18F-FDG (85%). Even when germline mutations were considered, the per-lesion sensitivity of 68Ga-DOTA-SSA was 97%, compared with 79% for 18F-FDG (37). An additional metaanalysis demonstrated that the sensitivity of 68Ga-DOTA-SSA (93%) is superior to that of 18F-FDOPA (80%), 18F-FDG (74%), and 123I/131I-MIBG (38%) (53).
In a prospective trial of 22 patients with sporadic metastatic pheochromocytoma or paraganglioma, 68Ga-DOTATATE detected 98% of metastases, outperforming 18F-FDG (49.2%), 18F-FDOPA (74.8%), and CT/MRI (81.6%) (34). In patients with SDHx mutations, the per-lesion sensitivity of 68Ga-DOTATATE is higher than that of 18F-FDG (Fig. 2) or CT/MRI (13,43,44). Overall, 68Ga-DOTATATE should be considered the tracer of choice for evaluating metastatic pheochromocytoma, metastatic paraganglioma, SDHx mutations, and HNPGL. An exception is pheochromocytoma or paraganglioma associated with polycythemia, MAX mutations, or apparently sporadic pheochromocytoma, for which 18F-FDOPA may be preferable. Limited studies have evaluated the use of SSAs in benign pheochromocytoma. In a study of 32 patients, 111In-pentetreotide had a sensitivity of 25% (54), whereas that of 68Ga-DOTA-SSA was expected to be higher and 18F-DOPA was still the preferred agent.
CT AND MRI
CT and MRI (Supplemental Fig. 1) play an important role in diagnosis, staging, and therapy response assessment in patients with pheochromocytoma or paraganglioma. These modalities are used presurgically to determine the site of disease and the relationship to other structures. Current guidelines suggest CT rather than MRI for initial localization in biochemically positive patients (35). MRI is preferable for pediatric patients and for screening because of its lack of ionizing radiation.
A small percentage of pheochromocytoma cases present as adrenal incidentalomas, whereas approximately 75% of incidentalomas are adenomas (55). CT and MRI are used to differentiate between adenoma and other adrenal lesions, including pheochromocytoma (Supplemental Fig. 1). On unenhanced CT, 99.6% of pheochromocytomas have more than 10 Hounsfield units (HU) (56). Whereas most adenomas have 10 HU or less, the less common lipid-poor adenomas also have more than 10 HU. Contrast-enhanced CT is used to determine absolute and relative percentage contrast washout between the portal-venous and delayed phases; values of at least 60% and at least 40%, for absolute and relative washout, respectively, are typical of lipid-poor adenomas but unfortunately overlap those of pheochromocytoma (57). Venous-phase enhancement of at least 85 HU was seen in 88% of pheochromocytomas but in only 16% of adenomas. Because pheochromocytomas can be large, they may present with central necrosis that does not enhance with contrast (ring sign) on CT or MRI. Regardless of washout, growing adrenal lesions and those larger than 4–5 cm usually require further workup, such as resection or biopsy.
MRI also recognizes adenomas by their lipid content using chemical shift sequences, and the discovery of a high lipid content is generally diagnostic of adenoma. Lipid-poor adenoma findings may overlap with the findings of pheochromocytoma on MRI and MRI washout (58). A high signal intensity on T2-weighted images, particularly those with fat suppression, has been described as characteristic of pheochromocytoma and paraganglioma (Supplemental Fig. 1), and although highly sensitive, this finding lacks specificity.
Patients with metastatic disease undergo whole-body CT or MRI for staging and presurgical evaluation of pheochromocytoma and paraganglioma and for assessment of disease progression and treatment response. Nonetheless, in cases of metastatic disease, functional imaging often has higher sensitivity for tumor detection, given the high incidence of bone metastases and small soft-tissue lesions that may be difficult to visualize with CT or MRI.
HNPGL
HNPGL most commonly arises in the carotid body and jugulotympanic regions, but concurrent tumors below the neck may be present. Germline mutations, most commonly SDHD and SDHB, are responsible for 25%–50% of HNPGL (59).
First-line imaging of HNPGL for staging, determining locoregional extent, and planning treatment generally involves anatomic imaging such as MRI, MR angiography, CT, and CT angiography (60). On CT imaging (Fig. 3), HNPGLs are hypervascular, with intense early arterial-phase enhancement that is also present on contrast-enhanced MRI, often with a salt-and-pepper appearance. MRI and MR angiography are usually performed to determine the extent of involvement, support disease management, evaluate risk, and estimate prognosis. MRI can involve a series of time-consuming sequences. A prospective trial of HNPGL associated with SDHx limited the sequences to a short contrast-enhanced MRI protocol consisting of a 3-dimensional time-of-flight MR angiographic sequence and an axial-plane fast spin-echo T1-weighted sequence with fat saturation. These sequences had sensitivity and specificity of 88.7% and 93.7%, respectively, for identifying HNPGL (61).
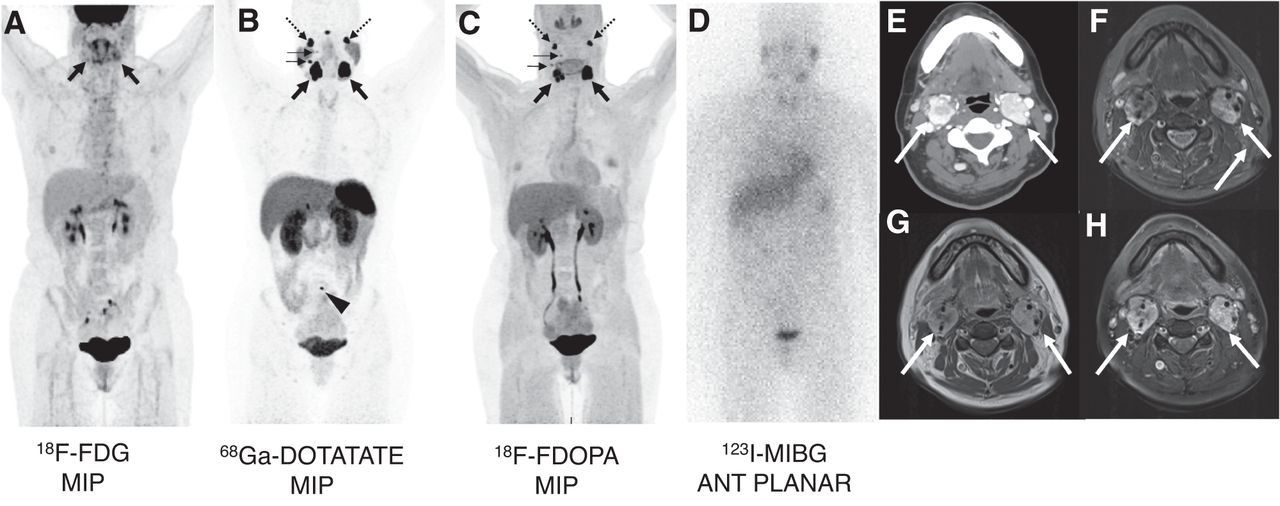
A 46-y-old woman with SDHD-associated HNPGL and metastases in lymph nodes and bones. (A) Maximum-intensity-projection (MIP) 18F-FDG PET scan showing carotid-body uptake (arrows) that is minor on right and slightly more prominent on left (SUVmax, 4.4 and 10.3, respectively) but not definitively identifying any other lesions. (B and C) MIP 68Ga-DOTATATE (B) and 18F-FDOPA (C) PET scans. Right and left carotid body tumors (horizontal solid arrows) are best identified in these (SUVmax, 134.6 and 199.1, respectively, for 68Ga-DOTATATE and 28.1 and 46.4, respectively, for 18F-FDOPA). Also seen are bilateral uptake in glomus jugulare paraganglioma (dashed arrows), as well as lymph node metastases (horizontal solid arrows). Highest contrast is noted in 68Ga-DOTATATE scan, which also identified L5 bone metastasis (arrowhead), not identified in any other functional modality. (D) Anterior 123I-MIBG planar scan with negative findings and showing normal salivary glands. (E) Axial contrast-enhanced CT scan showing enhancing right carotid body (2.1 cm) and left carotid body paraganglioma (2.7 cm) (arrows). (F–H) Axial short-τ inversion recovery MRI scan (F), contrast-enhanced T1-weighted MRI scan (G), and fat-suppressed contrast-enhanced T1-weighted MRI scan (H) demonstrating bilateral heterogeneous uptake (arrows). Lymph node metastases seen on 68Ga-DOTATATE and 18F-FDOPA were retrospectively identified on CT as subcentimeter lesions (not shown); however, on MRI they were difficult to discern from normal lymph nodes in region. Glomus jugulare paragangliomas seen bilaterally on 68Ga-DOTATATE and 18F-FDOPA were not seen on CT or MRI.
68Ga-DOTA-SSA, 18F-FDOPA, and to a lesser extent 18F-FDG imaging have high sensitivity for HNPGL (Fig. 3), whereas the sensitivity of 123I/131I-MIBG is poor (10%–42%) (Fig. 3; Table 3). The sensitivity of 68Ga-DOTATATE was 100% for HNPGL, with identification of additional lesions not visualized with other modalities (52). The sensitivity of 18F-FDOPA was also high (97%), although 18F-FDOPA detected only 60%, 18F-FDG only 70%, and CT or MRI only 77% of lesions outside the head and neck, whereas 68Ga-DOTATATE detected 100%. (52)
Sensitivity of Detection for HNPGL
18F-FDOPA has a high sensitivity (86.7%–100%) for HNPGL (23,31,32,50,62,63)—a sensitivity that surpasses that of MRI (Table 3) (50,62,63). Furthermore, interpretations of 18F-FDOPA were more reproducible than those of MR angiography and were often more informative than the MRI reading by directing attention to lesions that otherwise might have been missed (50,63). 18F-FDOPA has been considered a first-line imaging modality for HNPGL, although recent results for 68Ga-DOTA-SSA are superior (25,35).
The sensitivity of 18F-FDG in HNPGL ranges from 71% to 90.5% (52,62,64) but was not as high as that of 68Ga-DOTA-SSA or 18F-FDOPA. One group reported a 71% per-lesion sensitivity for 18F-FDG in a separate HNPGL patient group in which 18F-FDOPA had a sensitivity of 97% (52).
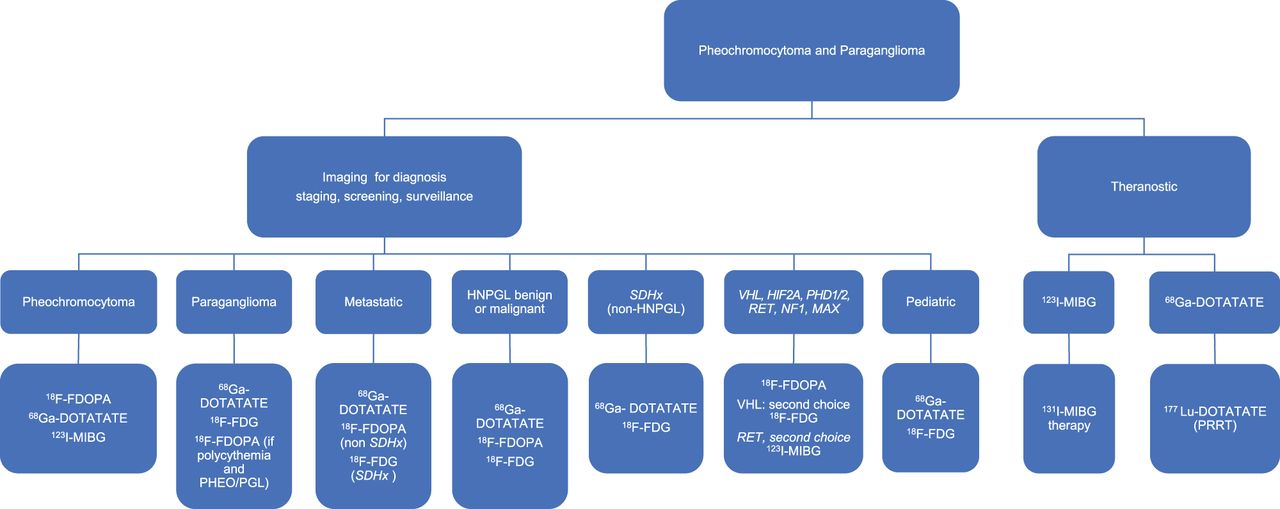
In summary, in patients with HNPGL or at high risk of developing HNPGL, functional imaging has high sensitivity and should be used in conjunction with MRI, with the latter required for surgical and treatment planning. In almost every situation, 68Ga-DOTA-SSA is considered the agent of choice, 18F-FDOPA the second choice, and 18F-FDG the third choice (Fig. 4).

Suggested imaging algorithm for various scenarios. If mutation status is unknown and only pheochromocytoma is present, 18F-FDOPA is first choice, followed by 68Ga-DOTATATE. For benign HNPGLs, 68Ga-DOTATATE is first choice, followed by 18F-FDOPA and then 18F-FDG. For metastatic disease outside head and neck, 68Ga-DOTATATE is first choice, followed by 18F-FDG if SDHx and 18F-FDOPA if non-SDHx. If mutation status is unknown in pediatric patient, 68Ga-DOTATATE is first choice, although this recommendation is based on data from small number of patients. In pediatric SDHx-related pheochromocytoma or paraganglioma, 68Ga-DOTATATE was inferior to 18F-FDG for abdominal lesions; thus, the recommendation is that 68Ga-DOTATATE be supplemented with contrast-enhanced CT/MRI or that 68Ga-DOTATATE PET/MRI be performed with intravenous contrast medium. PHEO/PGL = pheochromocytoma or paraganglioma; PRRT = peptide receptor radionuclide therapy.
PEDIATRIC PHEOCHROMOCYTOMA AND PARAGANGLIOMA
Ten to twenty percent of pheochromocytoma and paraganglioma cases occur in children (65), and most are hereditary (66). Pheochromocytoma is present bilaterally in 19% of cases, and 4%–65% present with or develop metastases (67,68). Babic et al. (68) reported the sensitivity in pediatric pheochromocytoma of CT (100%), MRI (93%), 18F-FDG (86%), MIBG (91%), 18F-FDOPA (100%), and 68Ga-DOTATATE (100%). Jha et al. (44) found that in 9 cases of pediatric SDHx pheochromocytoma or paraganglioma, the per-patient sensitivity was 100% for 18F-FDG and 68Ga-DOTATATE but the per-lesion sensitivity was lower (79.4% vs. 93.5%, respectively). Furthermore, 68Ga-DOTATATE was more sensitive than CT or MRI (73.8%). However, for abdominal lesions, the sensitivity of 68Ga-DOTATATE was 67%, whereas that of both 18F-FDG and CT or MRI was 80%. Thus, 68Ga-DOTATATE PET/CT is recommended as the functional imaging modality in pediatric SDHx with the exception of abdominal lesions, for which contrast-enhanced 68Ga-DOTATATE PET/CT or PET/MRI is suggested, although this exception warrants corroboration in larger numbers of patients.
IMAGING OF SPECIFIC MUTATIONS
Imaging phenotypes differ among germline mutations, although for some, data are very limited. Supplemental Table 2 provides some of the studies that described sensitivity results, as well as some of the relevant features regarding the presentation of the pheochromocytoma and paraganglioma cases associated with these mutations (RET, VHL, NF1, SDHx, EPAS1, and MAX). The best imaging data are for SDHx-related pheochromocytoma and paraganglioma, for which 68Ga-DOTATATE is the radiopharmaceutical of choice. 18F-FDG also has high sensitivity in these patients, although for HNPGL, 18F-FDOPA is the second choice (Supplemental Table 2). In patients with VHL, RET, and NF1 mutations, 18F-FDOPA is the most sensitive agent for tumor detection, but with limited comparisons with 68Ga-DOTATATE and 18F-FDG available. A study by Sharma et al. suggests high sensitivity for 68Ga-DOTANOC in patients with RET mutation (Supplemental Table 2) (16). Pheochromocytomas and paragangliomas associated with HIF2A (also known as EPAS1) and EGLN1 present with polycythemia, and those pheochromocytomas associated with MAX are better imaged with 18F-FDOPA, whereas imaging with 18F-FDG or 68Ga-DOTA-SSA had low sensitivity (Supplemental Table 2).
CONCLUSION
Pheochromocytoma and paraganglioma are complex molecularly driven diseases, with an increasing number of driver mutations identified. Because pheochromocytoma and paraganglioma are rare, studies are limited, typically small, and frequently retrospective. The identified pheochromocytoma and paraganglioma genotypes demonstrate imaging phenotypes that, although not perfectly predictive, offer guidance on the best functional imaging approaches. Frequently, PET/CT with 68Ga-DOTA-SSA has the highest diagnostic accuracy across imaging modalities. 123I-MIBG, 18F-FDOPA, and 18F-FDG can also be useful, especially in certain clinical presentations, in specific mutations, or for evaluating therapeutic options. Other tracers that target norepinephrine transporters are not routinely available and are thus beyond the scope of this review. This review has considered numerous studies using radiopharmaceuticals approved by the Food and Drug Administration or the European Medicines Agency. On the basis of this literature, we propose the imaging algorithm presented in Figure 4.
Footnotes
Learning Objectives: On successful completion of this activity, participants should be able to (1) identify the difference between pheochromocytoma and paraganglioma; (2) identify radiopharmaceutical agents available for imaging pheochromocytomas and extraadrenal paragangliomas; and (3) recognize the importance of genotype in selection of the imaging radiopharmaceutical for patients with pheochromocytoma or paraganglioma.
Financial Disclosure: This research was funded in part by NCI Cancer Center support grant P30CA008748 and the Eunice Kennedy Shriver National Institute of Child Health and Human Development, NIH. Dr. Pryma reports research and consulting funding from Siemens and 511 Pharma, as well as consulting funding from Bayer. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through August 2024.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 2, 2020.
- Accepted for publication February 16, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.