


Abstract
18F-FDG PET/CT is of value in the diagnosis of prosthetic vascular graft infection, but potential pitfalls related to tracer uptake in noninfected implants have been described. The current study assesses the incidence and patterns of 18F-FDG uptake over time in noninfected grafts, in relationship to prosthetic material and location. Methods: A 12-y PET/CT database was retrospectively searched for cancer patients with prosthetic vascular grafts. Data retrieved from patient files included graft location, material, and time from surgery. Images were reviewed by 2 nuclear medicine physicians in consensus, with the presence and patterns (focal, diffuse homogeneous, inhomogeneous) of increased 18F-FDG uptake in grafts recorded. The mean standardized uptake value in grafts (SUV-G) and mediastinum (SUV-M) was measured. The ratio of SUV-G to SUV-M (SUV-G/SUV-M) was calculated for each graft. Results: One hundred seven prostheses were identified in 102 studies in 43 cancer patients. Sixty-seven prostheses were made of Dacron, 33 of Gore-Tex, and 7 were native veins. No increased 18F-FDG uptake was found in 9 grafts (native veins, 4; Gore-Tex, 3; Dacron, 2). There was diffuse homogeneous uptake in 68 and inhomogeneous uptake in 30 grafts. The homogeneous pattern was more prevalent in Gore-Tex whereas the inhomogeneous uptake was seen more in Dacron vascular grafts. None of the grafts demonstrated focal uptake. The SUV-G range was 0.4–6.3 (average, 1.9), and SUV-M range was 0.6–2.4 (average, 1.4). The intensity of uptake was significantly higher in Dacron (SUV-G = 2.35 and SUV-G/SUV-M = 1.72) than in Gore-Tex (SUV-G = 1.09, SUV-G/SUV-M = 0.91) and native vein grafts (SUV-G = 1.07, SUV-G/SUV-M = 0.75) (P < 0.005). Native vein grafts showed a significant decrease in 18F-FDG uptake over time whereas synthetic grafts showed no change in intensity for a follow-up of up to 16 y. Conclusion: Diffuse 18F-FDG uptake was found in 92% of noninfected vascular prostheses, more in Dacron grafts than with other materials. The intensity of 18F-FDG uptake of synthetic grafts did not change over time. With knowledge of the presence, patterns, and persistence of 18F-FDG uptake in noninfected vascular prostheses, misinterpretation of PET/CT studies in patients referred for suspected prosthetic infection and in those assessed for diseases unrelated to their graft status can be avoided.
Vascular grafts replace or bypass occluded or diseased blood vessels to preserve regional oxygen supply. Autologous vascular grafts are made of a patient’s vessel, commonly the long saphenous vein. Synthetic grafts are made of either Dacron or polytetrafluroethylene (commercially known as Gore-Tex). Dacron is used mainly in large vessels, such as with aortic and aortoiliac surgery, whereas polytetrafluroethylene is used for medium-sized vessels. such as the femoral, popliteal, and tibial arteries. The use of prosthetic vascular grafts during reconstructive surgery is common, with approximately 2 million people undergoing the procedure each year in the United States. Infection of the prosthetic vascular graft is a rare but severe complication (1–4). Death rates after vascular prosthetic graft infection range from 15% to 75%, amputation in up to 70% of cases, and reinfection in approximately 18% of patients (5–10). The risk of complications increases with delayed treatment, which occurs often as a result of failure to diagnose, mainly in cases with a subtle, nonspecific clinical presentation.
18F-FDG PET is widely used for the assessment of cancer. Given the high metabolic activity of inflammatory cells, 18F-FDG is also a useful marker for various active infectious and inflammatory processes (11–13), including reports of a high sensitivity in the diagnosis of vascular prosthetic infections (14,15). Hybrid 18F-FDG PET/CT has established the role of 18F-FDG imaging for the assessment of suspected vascular graft infection, providing accurate anatomic localization of the site of infection with subsequent improved specificity (16–20).
However, increased 18F-FDG activity may occur also in the absence of an acute infectious process. In the immediate postoperative period, inflammatory changes around the graft represent a component of the healing process. 18F-FDG is also taken up by scar tissue and native vessels. Synthetic grafts often induce a foreign-body chronic low-grade inflammatory reaction, which can also exhibit increased 18F-FDG activity, thus representing potential causes for false-positive results and erroneous interpretation of 18F-FDG PET/CT studies (21–23). At present, there is only limited information regarding the incidence and patterns of 18F-FDG uptake in noninfected vascular grafts, mainly in relationship to type and location of the implants. A low positive predictive value due to faulty interpretation of increased 18F-FDG uptake in an aseptic prosthetic graft as infected may have a negative effect on planning of further patient management. Also, failure to diagnose graft infection because of the misinterpretation of abnormal 18F-FDG uptake as physiologic can have severe clinical consequences. This retrospective study in a large patient population aimed at providing detailed knowledge regarding the incidence, distribution patterns, and dynamics of 18F-FDG uptake in noninfected prosthetic vascular grafts.
MATERIALS AND METHODS
Patient Population
A 12-y 18F-FDG PET/CT database was retrospectively searched for cancer patients with a history of vascular grafts. Patients in whom vascular graft infection was suspected or confirmed at any point before or after the study were excluded from further evaluation. After identification of the specific patient population, the following data were retrieved from their medical records: the reason for referral to PET/CT; date of vascular surgery; number, location, and material (Dacron, Gore-Tex, and native vein grafts) of grafts in each patient; and time elapsed from surgery to PET/CT study. In patients with multiple studies, only tests performed at a time interval of at least 6 mo were included in the present study population. The Institutional Review Board approved this retrospective study, and the requirement to obtain informed consent was waived.
PET/CT Acquisition and Processing
Patients were instructed to fast, except for glucose-free oral hydration, for 4–6 h before the injection of 370–555 MBq (10–15 mCi) of 18F-FDG. Diabetic patients were instructed to keep their regular glucose-controlling-drugs schedule. Blood glucose levels were measured before injection. None of the patients was withdrawn from the study because of high blood glucose levels, and no additional glucose control drugs were used. PET and non–contrast-enhanced CT were acquired consecutively 90 min after the injection of 18F-FDG, using a PET/CT system (Discovery LS or Discovery 690; GE Healthcare).
Interpretation and Analysis of PET/CT Images
All studies were reviewed retrospectively with knowledge of the patient’s clinical history and results of previous imaging studies. A team of 2 nuclear medicine physicians interpreted the PET/CT images in consensus. The presence or absence of 18F-FDG activity in each vascular graft was recorded. In implants showing 18F-FDG avidity, subsequent visual assessment included defining the pattern of uptake for each graft as focal, diffuse homogeneous, inhomogeneous, or absent. Mean standardized uptake value (SUVmean) was measured in each graft (SUV-G) using a 1-cm circular region of interest. To overcome a potential error that may arise in areas with inhomogeneous 18F-FDG uptake, an average value was calculated from SUVmean measurements over 5 regions of interest drawn at 5 different levels along the graft in each inhomogeneous graft.
The measurement of SUVmean rather than maximum SUV was performed because it represents more correctly the overall metabolic activity in the whole graft. In addition, the mediastinal SUVmean (SUV-M), an index of 18F-FDG uptake in the blood pool, was measured in each patient using a same-size region of interest in the proximal ascending aorta. For the purpose of standardization of 18F-FDG intensity, the graft–to–mediastinum SUV ratio (SUV-G/SUV-M) was calculated for each graft. Average SUVmean and the SUV-G/SUV-M ratio were compared between different subgroups of patients defined by graft material and locations using the Mann–Whitney nonparametric test, with a P value of less than 0.05 considered as statistically significant. The correlation between intensity of 18F-FDG uptake expressed as SUV-G/SUV-M and the time elapsed from surgery was determined using linear regression analysis. 18F-FDG uptake patterns in different graft types were recorded and compared using the χ2 test, with a P value of less than 0.05 considered statistically significant.
RESULTS
The PET/CT database search identified 102 studies in 43 patients who met the inclusion criteria and were further analyzed. The patient population included 31 men and 12 women aged 56–82 y (average, 63 y). Seventeen patients had a single study, and 26 had between 2 and 8 studies. The clinical indication for performing the PET/CT studies included staging (n = 34), monitoring response to treatment (n = 28), suspected recurrence (n = 14), and routine follow-up (n = 21) of cancer as well as the assessment of lung nodules in 5 cases. One hundred seven vascular grafts were indentified, including aorto-bifemoral (n = 54), femoro-popliteal (n = 18), aortic (n = 13), femoro-femoral cross over (n = 13), and mono-aorto-femoral (9) implants. The graft material was Dacron in 67 implants, Gore-Tex in 33, and native veins in 7. Sixty-nine grafts were localized in the abdominopelvic region and 38 in the groin and lower limbs. Time between vascular surgery and the PET/CT study ranged between 5 mo and 16 y (average, 10 y). Nine grafts (8%), including 5 femoro-popliteal, 2 aorto-bifemoral, and 2 mono-aorto-femoral grafts, demonstrated no 18F-FDG uptake, including 4 native veins, 3 Gore-Tex, and 2 Dacron grafts implanted 9 mo to 10 y before the PET/CT study. 18F-FDG avidity was found in 98 grafts. Diffuse homogeneous 18F-FDG uptake was found in 67 grafts (68%), including 36 Dacron, 28 Gore-Tex, and 3 in native vein grafts. Inhomogeneous uptake was observed in 31 grafts (32%), including 29 Dacron and 2 Gore-Tex prostheses and in none of the native vein grafts (Table 1; Figs. 1 and 2). The homogeneous pattern was significantly more prevalent in Gore-Tex while inhomogeneous 18F-FDG uptake was significantly more frequent in Dacron vascular grafts (P < 0.01). None of the 18F-FDG–avid grafts demonstrated focal uptake.
18F-FDG Uptake Patterns and SUVmean Measurements in 107 Vascular Grafts

A 65-y-old man with leiomyosarcoma, 3 y after insertion of femoro-femoral Gore-Tex graft. Coronal CT (A), PET (B), and PET/CT (B) slices demonstrate diffuse homogeneous 18F-FDG uptake along graft (arrows), with SUVmean of 1.1.

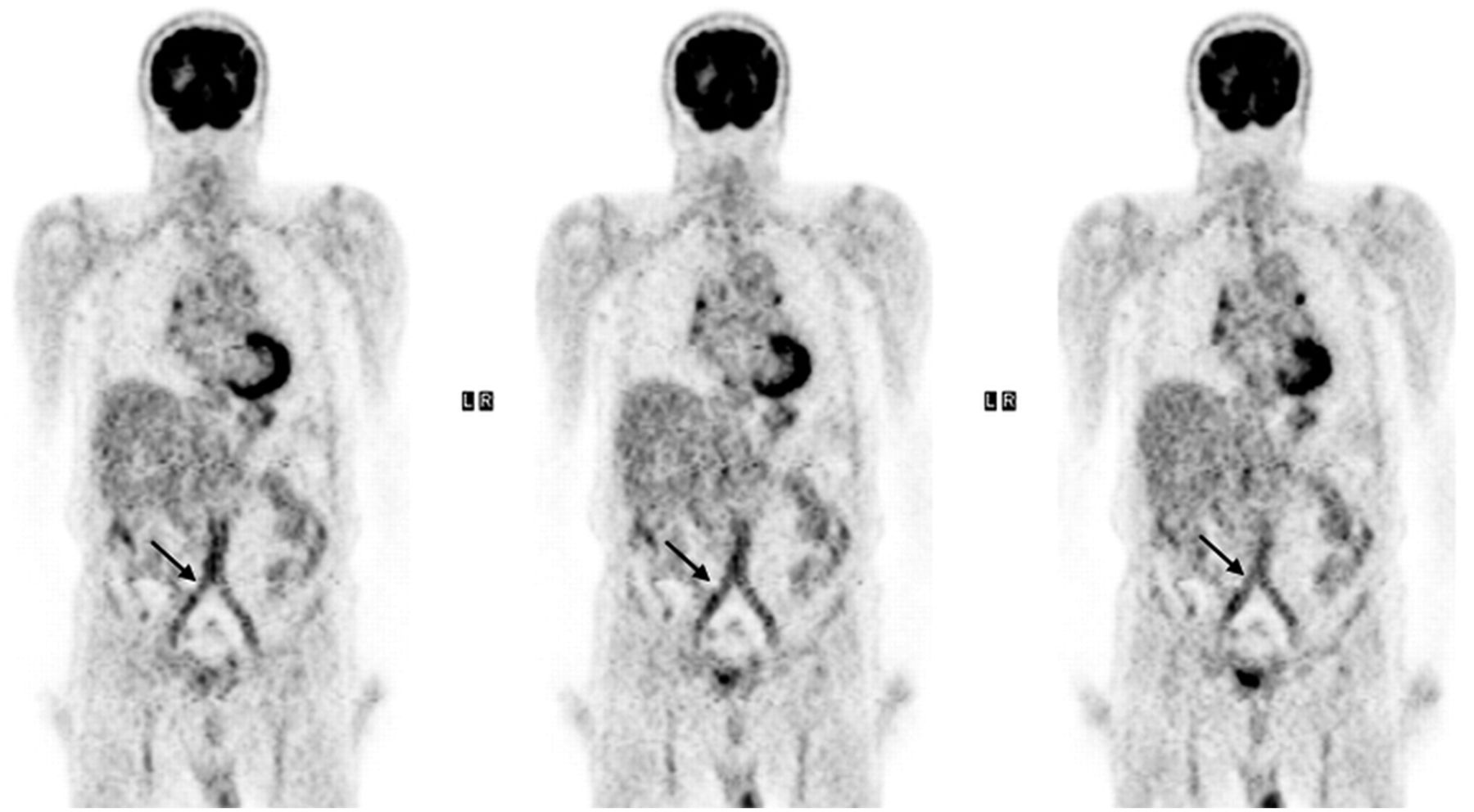
An 82-y-old man with newly diagnosed laryngeal cancer, 16 y after implant of aorto-bifemoral Dacron graft. Coronal PET slices demonstrate inhomogeneous 18F-FDG uptake along whole graft, with SUVmean of 2.5 (arrows).
SUVmean-G ranged between 0.4 and 6.3 (average, 1.9). SUVmean-M ranged between 0.6 and 2.4 (average, 1.4). The average SUV-G and SUV-G/SUV-M were significantly higher in Dacron (2.35 and 1.72, respectively) than in Gore-Tex (1.09 and 0.91, respectively) and native vein grafts (1.07 and 0.75, respectively) (P < 0.005) (Table 1). The average SUV-G and SUV-G/SUV-M were significantly higher in vascular grafts inserted in the abdominopelvic region (2.35 and 1.72, respectively) than in those localized in the groin and lower limbs (1.07 and 0.86, respectively) (P < 0.005). There was an inverse correlation between SUV-G/SUV-M and the time duration from surgery in native veins grafts (R2 = 0.73) (Fig. 3A). Synthetic grafts (both Dacron and Gore-Tex) showed no change in 18F-FDG uptake (expressed as SUV-G/SUV-M) over time after surgery (Figs. 3B and 3C). In a subgroup of 13 patients with synthetic grafts (10 Dacron and 3 Gore-Tex), repeated PET/CT studies were performed at a time interval of 1–5 y between studies. There was no statistically significant difference in average SUV-G/SUV-M between the first and the repeated study, 1.6 and 1.4, respectively (P = 0.3).
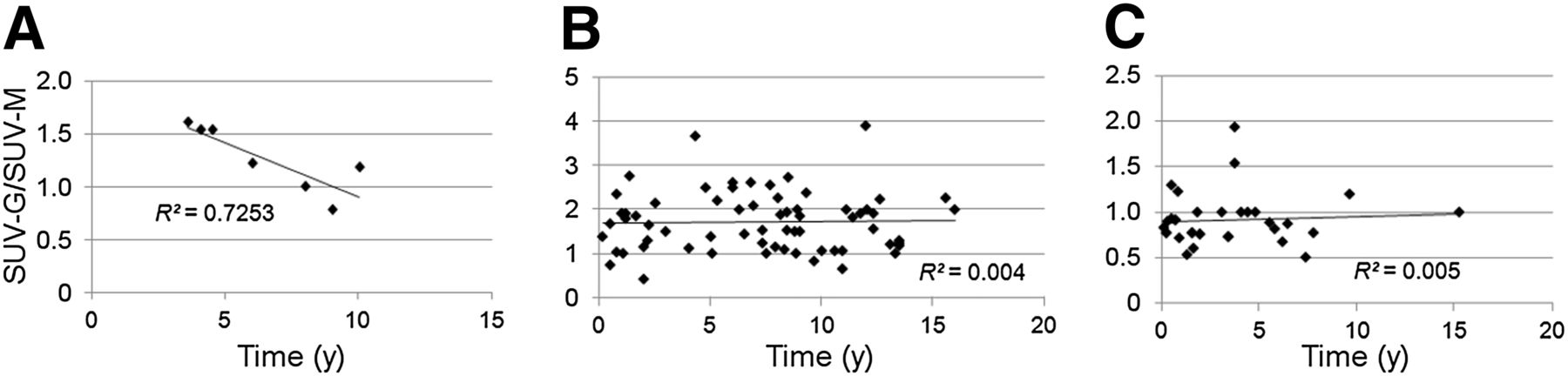
Relationship between SUV-G/SUV-M in each graft to time duration from prosthesis insertion surgery in 7 native vein grafts (A), in 67 Dacron grafts (B), and in 33 Gore-Tex grafts (C).
DISCUSSION
This retrospective study assesses the incidence and patterns of 18F-FDG uptake in noninfected vascular grafts and further analyzes the relationship between 18F-FDG avidity and specific prosthetic materials, graft location, and time elapsed from surgery. 18F-FDG uptake was found in most (92%) of the noninfected vascular prostheses. A previous preliminary report in a small group of 14 patients has demonstrated a frequency of 88% in 18F-FDG avidity of vascular graft prostheses (24). In the present study, Dacron grafts had a significantly higher metabolic activity expressed both as SUVmean-G and SUV-G/SUV-M than Gore-Tex and native vein grafts. Similar significant differences in the degree of 18F-FDG uptake were also found between prosthetic grafts inserted in the torso as compared with those localized in the groin and lower limbs. These differences can be most probably attributed to the association between graft material and location because most of the abdominopelvic grafts were made of Dacron whereas those in the lower limbs graft were either Gore-Tex or native veins. Although native vein grafts showed a significant reduction in 18F-FDG uptake with time, no change was observed for 18F-FDG–avid synthetic grafts over a period of up to 16 y after surgery. To the best of our knowledge, this is the first study to describe differences in 18F-FDG uptake levels in relationship to types of vascular graft material, location, and time from surgery. Approximately two thirds of the 92% of the 18F-FDG–avid noninfected prosthetic grafts showed diffuse homogeneous uptake, with the remaining one third showing inhomogeneous uptake (Figs. 1 and 2). The homogeneous pattern was significantly more prevalent in Gore-Tex whereas inhomogeneous 18F-FDG uptake was found to be significantly more frequent in Dacron vascular grafts. Diffuse 18F-FDG uptake in noninfected grafts is the result of a local sterile inflammatory process around the prosthesis due to a foreign body–related reaction. During this process, a relatively small number of inflammatory cells—such as macrophages, fibroblasts, and foreign body giant cells, known to take up small amounts of 18F-FDG—localized in the region of the graft (21,22,25). Notably, none of the noninfected grafts showed focal 18F-FDG uptake. In a previous study by our group investigating the role of 18F-FDG PET/CT in the diagnosis of vascular graft infection, focal 18F-FDG uptake had a sensitivity of 93%, specificity of 91%, positive predictive value of 88%, and negative predictive value of 96%, in sharp contrast with 10 of 54 noninfected grafts that demonstrated mild linear 18F-FDG uptake (26). Similarly, in a study by Spacek et al., intense focal uptake was specific in 92.7% of prostheses, with a positive predictive value of 93.5% for predicting graft infection. These authors also found that approximately one fifth of grafts showed inhomogeneous uptake, divided among two thirds of infected and one third of noninfected implants, thus concluding that this pattern of 18F-FDG avidity is a poor diagnostic marker (27). The results of the current study support the concept that although focal uptake is a strong indicator of graft infection, mild diffuse 18F-FDG activity is a by-product of either the surgical process or a reaction to the presence of prosthetic material and should be interpreted as such on 18F-FDG PET/CT studies.
Present data show that 18F-FDG uptake in native implanted vessels declines over time because of a decrease in the inflammatory activity with healing. A study including a small group of 16 patients with noninfected synthetic aortic grafts also reported the presence of 18F-FDG uptake in most vascular prostheses in the immediate postoperative period (25). In contrast, in the current study 18F-FDG uptake did not change over time in synthetic grafts, indicative of a prolonged foreign body inflammation. Although prolonged 18F-FDG avidity around synthetic grafts has been described (25,26,28), the present study demonstrates that this finding may be sustained for as long as 16 y with no significant change in the level of tracer uptake over time. The observation found in the whole study group that 18F-FDG uptake persists over time in prosthetic grafts is further supported by findings in the subgroup of patients with synthetic grafts who underwent repeated 18F-FDG PET/CT studies 1–5 y apart, with no significant change in the metabolic activity in the graft between repeated studies. It is therefore imperative that the pattern of 18F-FDG uptake should be carefully considered not just in the immediate postoperative period but also if imaging is performed at a much later date, to eliminate false-positive findings. A relative limitation in the present study is the use of data from repeated studies in the same patient. Because only tests performed at time intervals of at least 6 mo were included, it is assumed that these measurements appropriately reflect the metabolic behavior of all grafts as a group. Current results indicate that diffuse 18F-FDG uptake in synthetic grafts, even for years after the prosthesis was inserted, should be interpreted as noninfected. However, the same pattern seen in native vein grafts should raise the suspicion for infection. In addition, it is important to assess the degree of homogeneity of 18F-FDG uptake along the graft. Although an inhomogeneous uptake pattern is frequent in noninfected Dacron grafts, it is uncommon in noninfected Gore-Tex prostheses and, if present, should be interpreted with caution. Knowledge of the expected 18F-FDG uptake pattern in different noninfected graft types is expected to improve the diagnostic accuracy of 18F-FDG PET studies performed for the assessment of suspected vascular graft infection by decreasing the false-positive rate. Further studies are needed to test this hypothesis.
CONCLUSION
Diffuse 18F-FDG uptake was found in 92% of noninfected vascular prostheses, higher in Dacron grafts than with other materials. The intensity of 18F-FDG uptake in synthetic grafts did not change over time. Knowledge of the presence, patterns, and persistence of 18F-FDG uptake in noninfected vascular prostheses will aid in avoiding the misinterpretation of PET/CT studies in patients assessed for diseases unrelated to their graft status and in those referred for suspected prosthetic infection.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 10, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 25, 2013.
- Accepted for publication September 30, 2013.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Infection Imaging: Focus on New Tracers?
- The Value of 18F-FDG PET/CT in Diagnosis and During Follow-up in 273 Patients with Chronic Q Fever
- Metabolic Imaging of Infection
- FDG Uptake by Prosthetic Arterial Grafts in Large Vessel Vasculitis Is Not Specific for Active Disease
- 18F-Fluorodeoxyglucose Imaging of Inflammation: Ready to Represent a Standard in Diagnosing Endocarditis?
- Characterization of 18F-Fluorodeoxyglucose Uptake Pattern in Noninfected Prosthetic Heart Valves
- 18F-FDG PET/CT for Therapy Control in Vascular Graft Infections: A First Feasibility Study