


Abstract
The aim of this study was to evaluate the clinical value of PET/CT with 18F-FDG for therapy control in patients with prosthetic vascular graft infections (PVGIs). Methods: In this single-center, observational, prospective cohort study, 25 patients with a median age of 66 y (range, 48–81 y) who had a proven PVGI were included. Follow-up 18F-FDG PET/CT was performed at a median of 170 d (range, 89–249 d) after baseline examination. Two independent and masked interpreters measured maximum standardized uptake values to quantify metabolic activity and analyzed whole-body datasets for a secondary diagnosis (i.e., infectious foci not near the graft). The metabolic activity of the graft was correlated with clinical information and 2 laboratory markers (C-reactive protein and white blood cell count). Results: 18F-FDG PET/CT had an impact on management in all patients. In 19 of 25 patients (76%), antibiotic treatment was continued because of the results of follow-up 18F-FDG PET/CT. Antibiotic treatment was stopped or changed in 8% and 16% of patients, respectively. In 8 patients (32%), additional incidental findings were detected on follow-up 18F-FDG PET/CT and had a further impact on patient management. Only in a subgroup of patients with PVGI and no other sites of infection was a significant correlation found between the difference in C-reactive protein at the time of baseline and follow-up 18F-FDG PET/CT and the difference in maximum standardized uptake value (n = 11; R2 = 0.67; P = 0.002). Conclusion: 18F-FDG PET/CT represents a useful tool in therapy monitoring of PVGI and has an impact on patient management.
Morbidity and mortality in prosthetic vascular graft infections (PVGIs) are as high as 20%–40% (1,2). Outcome data on different treatment modalities are scarce and partly controversial (2–4). Routinely performed treatments for PVGI comprise a combination of surgical intervention with systemic antibiotic medication, since the latter without surgery is associated with an increased mortality rate (1). There are no valid guidelines on either the diagnosis and management or the treatment of PVGI. A reliable monitoring tool for therapy control in PVGI is desirable.
18F-FDG PET/CT is a well-established imaging modality for therapy control in many malignant diseases (5–9) and has been suggested to be useful in patients with infectious disease (10). Initial reports demonstrated a high diagnostic accuracy for 18F-FDG PET/CT in detecting PVGI (73%–94%) (11–15), with a recent article showing an excellent positive predictive value, especially in patients who did not receive antibiotics before undergoing PET (16). The known high negative predictive value of the method might allow the endpoint of treatment to be determined when a known infectious site becomes metabolically inactive on follow-up 18F-FDG PET/CT. Treatment for a minimum of 3–6 mo is suggested for PVGI (4), and early prediction of response may identify patients with graft infection who will benefit from shorter treatment and, hence, may allow for more individualized approaches. Furthermore, 18F-FDG PET/CT may also identify nonresponders in need of different therapy approaches. There are only limited data on imaging-guided therapy control in patients with chronic infections, and there are no data with regard to PVGI (17). The aim of this feasibility study was to evaluate the use of 18F-FDG PET/CT for therapy control in patients with PVGI.
MATERIALS AND METHODS
Study Design, Patient Population, and Data Collection
The Vascular Graft Cohort Study (VASGRA) is an open, observational cohort with continued enrollment of patients aged 18 y or older receiving any type of vascular graft at the University Hospital of Zurich, Switzerland. The institutional review board approved this study, and all subjects give written informed consent. Surgical, demographic, clinical, and treatment information is prospectively collected every 6 mo.
We used the criteria proposed by FitzGerald et al. (18), by which PVGI is diagnosed on the basis of positive bacterial cultures of intraoperative specimens or blood samples, as well as clinical, laboratory, or radiologic signs of infection such as perigraft air, fluid persisting for more than 8 wk postoperatively, or abscess formation. Information on PVGI is ascertained and adjudicated by a team of infectious disease specialists and vascular surgeons. Patients receive empiric and, later, antimicrobial therapy. Operable patients presenting with an infection involving the vascular graft (Szilagyi grade III (19)) are treated according to an in-house standardized algorithm in a graft-preserving manner (20). Surgical debridement of infected tissue is combined with negative-pressure wound therapy. Tissue obtained during surgical debridement is processed for histopathologic and microbiologic examination. A positive microbiologic culture of the deep tissue around the vascular graft (obtained by open biopsy) or a positive microbiologic culture of an explanted vascular graft represents our gold standard for diagnosis of graft infection. Patients with proven PVGI are clinically monitored; at follow-up visits, C-reactive protein (CRP) and white blood cell count (WBC) are obtained.
Since May 2013, patients have undergone 18F-FDG PET/CT for diagnosis of PVGI before surgical reintervention (baseline 18F-FDG PET/CT) and 3–6 mo later while receiving antimicrobial therapy (follow-up 18F-FDG PET/CT).
PET/CT Data Acquisition
18F-FDG PET/CT was successfully performed twice, with diagnostic image quality, in all 25 patients. These 25 patients were a subset of VASGRA patients with PVGI. Per the protocol, imaging took place at least 60 d after the last vascular operation or wound closure, at a median of 439 d (range, 70–5,381 d) and 171 d (range, 75–5,491 d) for baseline and follow-up imaging, respectively. The same imaging protocol was used for both. The patients had been fasting for at least 4 h before 18F-FDG administration and had received no insulin injections for 4 h. Body weight, height, and blood glucose level were measured before injection of 18F-FDG. The acceptable blood glucose levels for imaging were less than 8 mmol/L in nondiabetic patients (n = 21) and less than 12 mmol/L in diabetic patients (n = 4) (mean ± SD, 6.2 ± 1.2 mmol/L at baseline and 6.3 ± 1.7 mmol/L at follow-up). After intravenous injection of body weight–adjusted 18F-FDG (337 ± 58 MBq at baseline and 336 ± 56 MBq at follow-up), the patients rested for 60 min. Scanning was performed on an integrated PET/CT system (DiscoveryTM VCT; GE Healthcare).
Data were acquired while the patient was supine with arms overhead. Low-dose CT for attenuation correction was performed from the mid thigh to the vertex of the skull with the following parameters: tube voltage, 140 kVp; tube current–time product, 10–80 mAs/slice; pitch, 1.4; collimation, 64 × 0.625 mm; rotation time, 0.5 ms; and field of view, 50 cm. Directly after the CT data acquisition, PET data were acquired using the 3-dimensional mode with a fixed scan duration of 2 min per bed position and a field of view of 157 mm. Emission data were corrected for randoms, dead time, scatter, and attenuation. CT data for attenuation correction and anatomic referencing were reconstructed with a slice thickness of 3.75 mm and an increment of 3.0 mm using a filtered back-reconstruction algorithm. Attenuation-corrected axial PET images were reconstructed using a standard iterative ordered-subset expectation maximization 3-dimensional algorithm (256 × 256 matrix, Fourier rebinning, 8 iterations, and 16 subsets).
Image Analysis
All 18F-FDG PET/CT images were independently analyzed by 2 experienced nuclear medicine physicians on an Advantage Windows Workstation, version 4.4 (GE Healthcare). Whole-body datasets were analyzed for a secondary diagnosis, that is, infectious foci not near a graft or other relevant or potentially malignant findings. To measure the metabolic activity of the tracer in all grafts on baseline and follow-up 18F-FDG PET/CT, we calculated maximum standardized uptake value (SUVmax) using built-in software by placing a volume of interest at the site of highest uptake in the wall of the graft. The SUVmax measurements followed the guidelines of the European Association of Nuclear Medicine and the Society of Nuclear Medicine and Molecular Imaging for use of 18F-FDG PET/CT in inflammation and infection (21). Correct volume-of-interest placement in the strongest focus of 18F-FDG activity was confirmed on axial, coronal, and sagittal reformatted images to avoid partial-volume effects or signal spillover from neighboring organs such as the kidney. When measurements were not identical (n = 2), both interpreters made additional measurements in consensus. Because 18F-FDG uptake patterns are important for the diagnosis of PVGI (16,22), we used a previously published 5-point visual grading score (16) to better describe the PVGI (Table 1). In follow-up PET/CT scans, nonresponse was defined as an equal or increasing SUVmax in the PVGI, partial response as a decrease in SUVmax of more than 20%, and complete response as disappearance of the focal uptake pattern and a decrease in SUVmax below the level of the mediastinal blood pool. Finally, we defined additional metabolically active foci as being any other sites of infection or inflammation on baseline or follow-up 18F-FDG PET/CT, as such foci may impair the clinical presentation or laboratory testing of patients with PVGI.
Patient and 18F-FDG PET/CT Characteristics at Diagnosis and at Follow-up
Statistical Analyses
We used the Wilcoxon matched-pairs signed-rank test to compare baseline and follow-up values. A P value of less than 0.05 was considered statistically significant. Linear regression was performed to compare the difference in, and the relative change in, CRP and SUVmax between baseline and follow-up imaging. In additional analyses, the difference and relative change in WBC relative to SUVmax were compared between baseline and follow-up imaging. We differentiated between patients with a graft infection only and patients with a graft infection plus additional metabolically active foci on follow-up imaging. We performed univariable logistic regression analyses to identify potential predictors of clinical response (absence of clinical signs of infection, negative microbiologic cultures, and declining or normal inflammatory markers). Statistical analyses were performed with Stata (version 13; StataCorp).
RESULTS
The index surgical interventions included total arch or descending aorta replacements (n = 6), aortobiiliac grafts (n = 7), femorofemoral crossover bypass (n = 2), and iliofemoral or femorotibial bypass (n = 2). Seven patients underwent endovascular placement of a stent-graft in the iliac artery (n = 3) or endovascular aortic repair (abdominal aorta, n = 4; thoracic aorta, n = 3). Twenty-five patients (2 women, 23 men) with a median age of 66 y (range, 48–81 y) had a microbiologically proven PVGI at the time of baseline 18F-FDG PET/CT. Patient and 18F-FDG PET/CT characteristics at diagnosis and at follow-up are shown in Table 1. Follow-up 18F-FDG PET/CT was performed at a median of 170 d (range, 89–249 y) after baseline examination.
Metabolic Activity
Graft Infection
The 18F-FDG uptake pattern was focal in all PVGIs at baseline (16) and remained focal on most follow-up scans. Median SUVmax at the site of highest uptake decreased between baseline (SUVmax, 6.7; range, 4.0–17.8) and follow-up (SUVmax, 4.9; range, 3.0–10.5; P = 0.002) (Fig. 1). The metabolic activity of PVGI increased in 4 patients (16%) (Fig. 2) and decreased in 21 patients (84%). None of the 25 patients showed a complete response to therapy on follow-up 18F-FDG PET/CT (the lowest measured SUVmax at follow-up was 3.0).
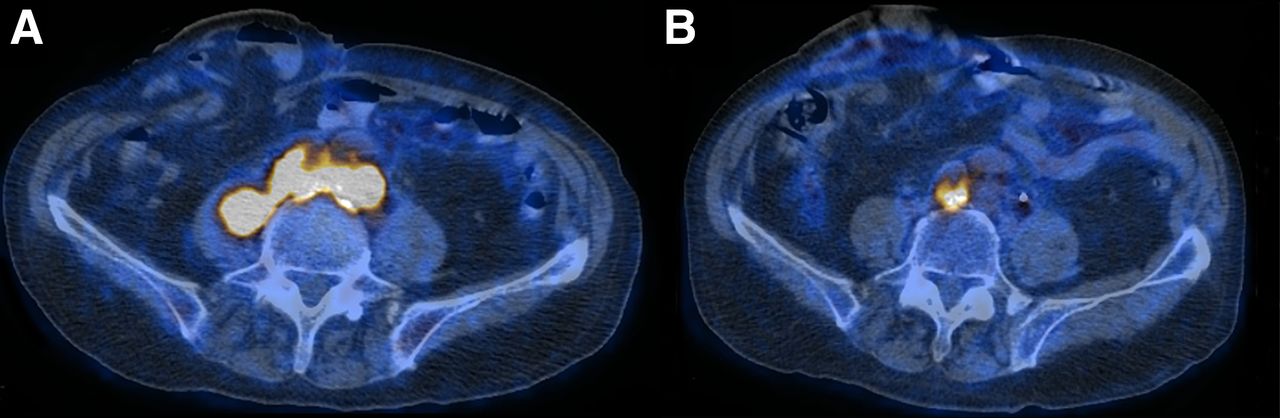
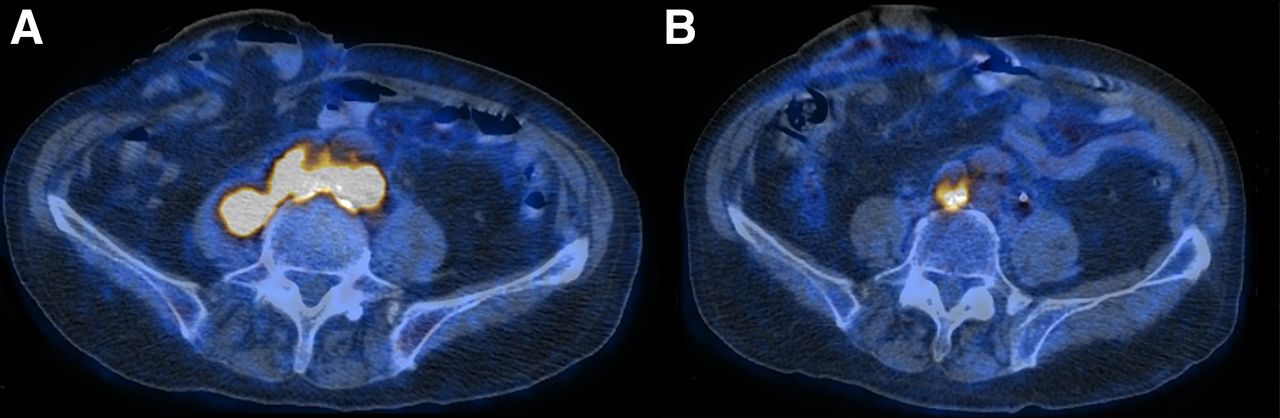
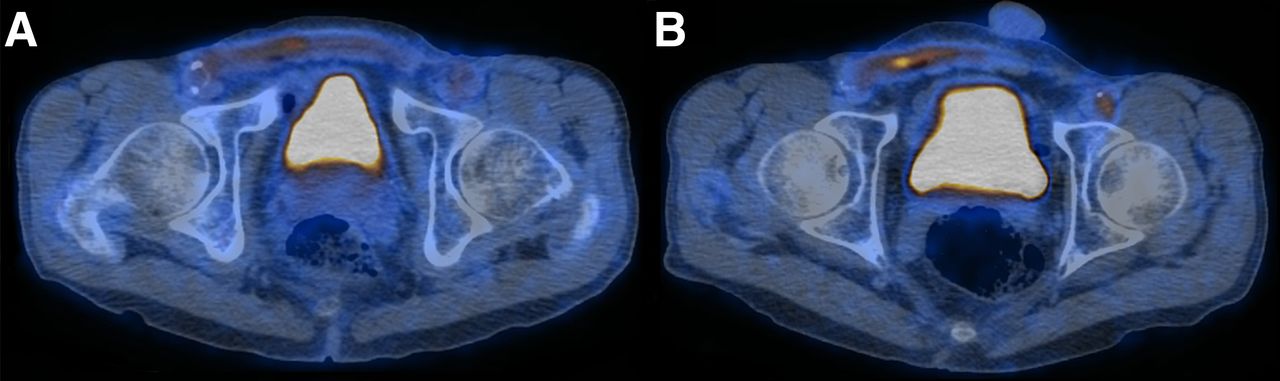
An 81-y-old man with bifurcated graft infection (polytetrafluoroethylene graft). (A) Baseline 18F-FDG PET/CT in September 2013 shows strong 18F-FDG avidity. (B) Follow-up 18F-FDG PET/CT in January 2014 demonstrates partial response to therapy after surgery and antimicrobial therapy. SUVmax decreased from 16.2 to 9.2, CRP decreased from 85 to 15 mg/L, and WBC decreased from 9.2 to 5.3 g/L.
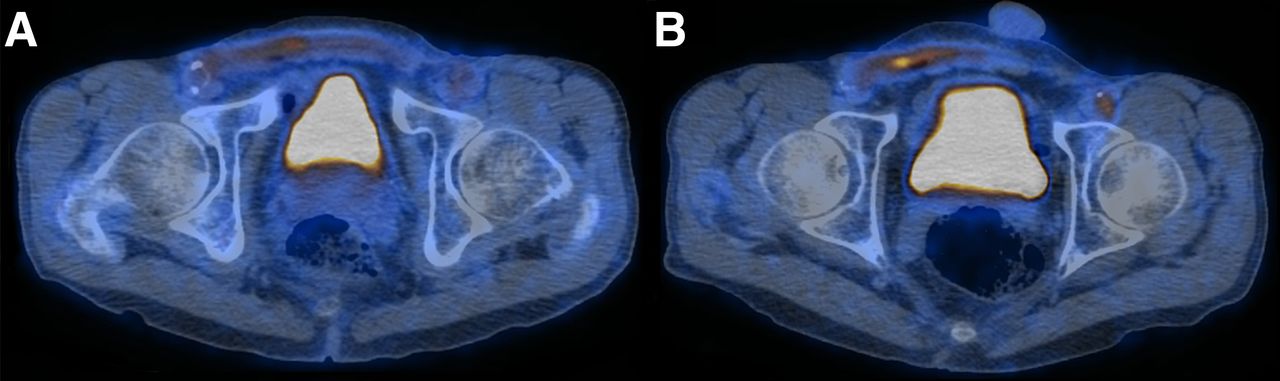
74-y-old man with infection of femorofemoral crossover bypass (polyethylene terephthalate graft). (A) Baseline 18F-FDG PET/CT in November 2013 displays 18F-FDG–avid graft infection. (B) Follow-up 18F-FDG PET/CT in April 2014 shows progression of 18F-FDG activity (SUVmax increased from 4.0 to 5.2). CRP increased from 6 to 10 mg/L, and WBC decreased from 9.9 to 9.1 g/L.
Detection of Other Foci with 18F-FDG PET/CT
Fourteen patients had additional metabolically active foci at either one or both time points (baseline and follow-up) (Fig. 3). At baseline, 10 patients had 11 infectious foci: sternum (n = 5), gastritis (n = 1), spondylodiskitis (n = 1), septic arthritis (n = 1), colitis (n = 2), and septic embolisms of left thigh (n = 1) (Table 1). At follow-up, 12 patients had 14 metabolically active foci: rheumatoid arthritis (n = 1), sternum (n = 6), gastritis (n = 1), spondylodiskitis (n = 1), arthritis (n = 1), pneumonia (n = 1), subcutaneous abscess (n = 1), and soft-tissue inflammation (n = 2). Only PET/CT findings deemed clinically relevant were proven by further clinical work-up; Table 1 states whether other foci were only suspected by PET/CT or also proven clinically.
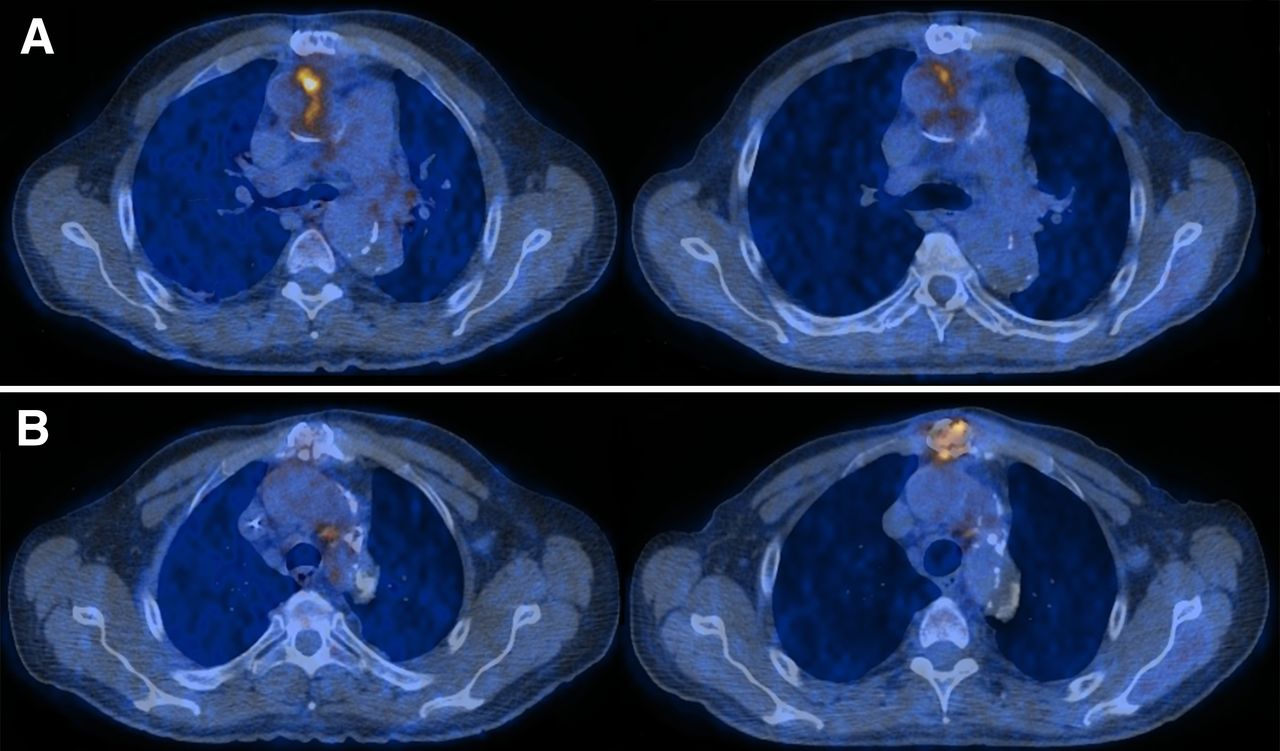
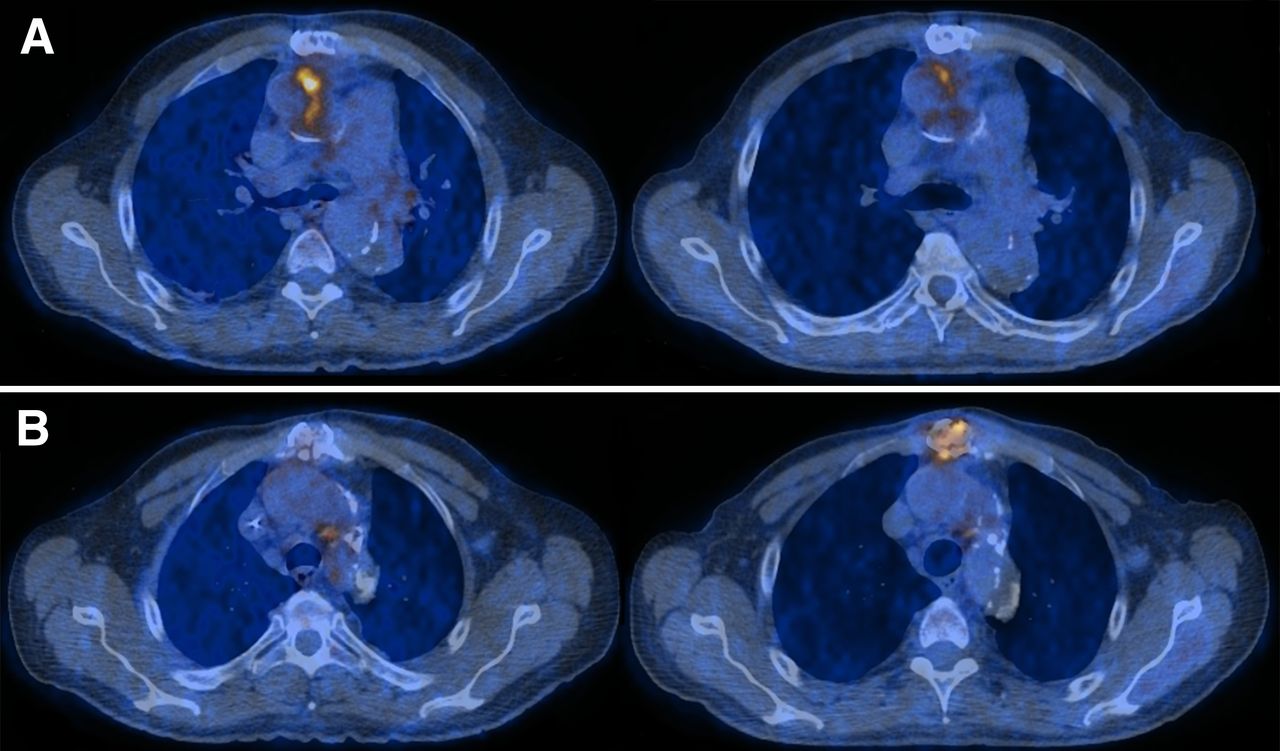
A 60-y-old man with PVGI after aortic root and total arch replacement (pyrolytic carbon valve; double-velour graft and collagen-coated polyester graft). (A) Baseline 18F-FDG PET/CT in September 2012 displays 18F-FDG–avid infection of graft (SUVmax, 7.6) and only mild 18F-FDG activity in sternum (SUVmax, 4.0). (B) Follow-up 18F-FDG PET/CT in June 2013 shows partial therapy response at graft (SUVmax, 5.1) but progression in sternum (SUVmax, 5.2). CRP decreased from 33 to 15 mg/L, and WBC increased from 2.6 to 4.0 g/L.
Correlation with Laboratory Markers
Between baseline and follow-up, median CRP decreased from 33 mg/L (range, 0.80–217 mg/L) to 6.8 mg/L (range, 0.8–123 mg/L) (P < 0.001). CRP increased in 3 patients (12%), was stable in 1 patient (4%), and decreased in 21 patients (84%). Median WBC also decreased between baseline and follow-up: from 7.51 g/L (mean, 2.99–12.4 g/L) to 6.54 g/L (mean, 3.43–11.42 g/L) (Table 1).
The difference in CRP and SUVmax between baseline and follow-up correlated in the subgroup of patients who had only a graft infection and no other metabolically active focus (Fig. 4A) (n = 11; R2 = 0.67; P = 0.002). There was no correlation in the subgroup of patients with additional metabolically active foci (n = 14; R2 = 0.17; P = 0.139).

Linear regression plot of difference and relative change between baseline and follow-up 18F-FDG PET/CT compared with difference in CRP. (A) Results among patients with PVGI and no other sites of infection (n = 11). (B) Results among patients with PVGI plus additional metabolically active foci.
Impact of Follow-up PET/CT on Patient Management
In 19 of 25 patients (76%), antibiotic treatment was continued on the basis of the follow-up 18F-FDG PET/CT results; in 2 patients (8%), treatment was stopped; in 4 patients (16%), antibiotic treatment was changed. In 8 patients (32%; 7 patients with decreasing CRP and 1 patient with increasing CRP), the results of follow-up 18F-FDG PET/CT had a further impact on management: In 2 patients, progression of the graft infection was detected, followed by surgical intervention. In 2 patients, focal 18F-FDG uptake in the colon was noted and subsequent colonoscopy demonstrated recurrence of rectal carcinoma in one and diverticulitis in the other. In one patient, 18F-FDG PET/CT correctly identified acute ischemic stroke, which was clinically silent but confirmed by subsequent MR imaging of the brain. Finally, 18F-FDG PET/CT detected morphologic progression of spondylodiskitis in one patient (Fig. 5), who underwent bone biopsy for further evaluation of the infection. Univariable logistic regression analysis did not find any factor significantly associated with clinical outcome (data not shown).

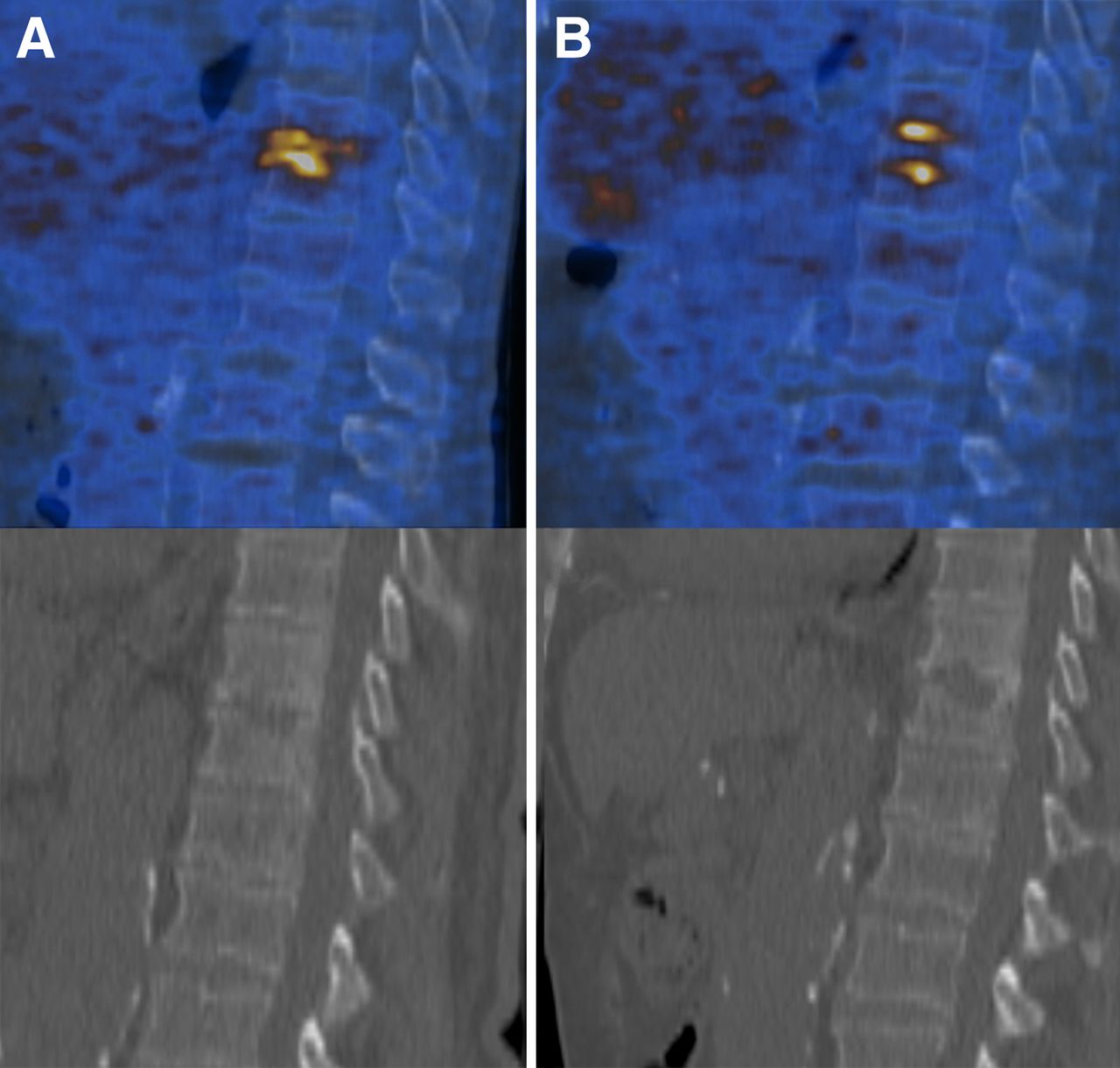
The patient in Figure 3 also had spondylodiskitis. (A) 18F-FDG avidity (SUVmax, 7.0) is seen on baseline 18F-FDG PET/CT in September 2012. (B) 18F-FDG activity is similar (SUVmax, 6.9) on follow-up 18F-FDG PET/CT in June 2013, but CT displays progression of osteolysis. 18F-FDG PET/CT findings resulted in change in patient treatment, as bone biopsy was performed to further evaluate infection.
DISCUSSION
18F-FDG PET/CT allows for the monitoring of PVGI and treatment response. It appears to be superior to blood biomarkers and can detect alternative metabolically active sites. 18F-FDG PET/CT had an impact on clinical management in all patients, resulting in either continuation or change of antimicrobial therapy. In the subgroup of patients with a PVGI and no other sites of infection, we found a significant correlation between the absolute difference and relative change in CRP and SUVmax between baseline and follow-up imaging.
There are only limited data on imaging-guided therapy control in infections (17). At present, routine use of 18F-FDG PET/CT is not recommended for therapy control in infectious processes in general (23) and PVGI in particular. In PVGI, we would expect SUVmax to decrease after the start of antibiotic therapy. Immediately after surgery, we would expect SUVmax to increase because of hyperperfusion; but if repeated debridements at the infection site are performed over time, we would expect SUVmax to decrease in response to therapy. Indeed, we could show that median SUVmax in vascular grafts decreased between baseline and follow-up. However, we could not calculate predictors of clinical outcome because only 2 patients had a complete response to therapy during the study. Hence, we used CRP and WBC as an approximation of therapy response. So far, there are no data on CRP and monitoring of treatment response in PVGI. What we expect is that leukocytes and inflammatory markers may add to the diagnosis of PVGI. Langerhuus et al. evaluated potential biomarkers for aortic graft infections in a pig model and found that CRP (sensitivity, 86%; specificity, 75%) was superior to WBC and tumor necrosis factor–α (24). CRP seemed to be a valuable indicator of therapy control in our patients with PVGI as the only site of infection at baseline, as we found a significant correlation between the course of CRP and SUVmax changes in this subgroup. This observation is in line with the current body of literature, which indicates that a decrease in CRP in patients with vasculitis correlates with a decrease in metabolic activity (25). However, further follow-up and outcome studies are required, as long-term antibiotic treatment may hamper the sensitivity of PET/CT in detecting infection during follow-up.
Notably, more than a third of the patients with PVGI in our cohort had developed additional sites of 18F-FDG uptake by the time of follow-up. Thus, we suggest that 18F-FDG PET/CT provides additional information to guide therapeutic decisions. Such newly discovered metabolically active sites impair routine follow-up parameters such as increasing or stable CRP and WBC, which may be falsely interpreted as nonsuccess of the PVGI treatment. In patients with PVGI and additional metabolically active foci on baseline or follow-up 18F-FDG PET/CT, the correlation between the change in CRP and SUVmax was not significant. Therapy control based on clinical parameters alone seems to be inferior to that based on 18F-FDG PET/CT, especially if one infectious focus responds well to treatment but another does not.
The main limitation of this study was that we did not evaluate different types of index operations, grafts, or pathogens as independent predictors because of the small number of patients. However, the results of our study are rather homogeneous. Furthermore, we did not compare our findings to other imaging possibilities—such as labeled leukocyte scintigraphy—that may also be helpful in following up PVGI (26).
CONCLUSION
18F-FDG PET/CT represents a useful tool in monitoring therapy of PVGI and has an impact on patient management. By providing quantitative data on the course of the graft infection and whole-body imaging data, PET/CT differentiates between response to therapy of the graft infection and other infectious foci. Further long-term studies are needed to determine the exact value and response to therapy of 18F-FDG/PET/CT in PVGI, taking into account the costs and limited availability of PET/CT in routine practice.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study (ClinicalTrials.gov identifier NCT01821664) was financed within the framework of VASGRA as supported by the Swiss National Science Foundation (grant 320030_144277/1), the Promedica Foundation (grant 1080/A), the Vontobel Foundation, and the Rozalia Foundation, as well as by a “Filling the Gap” grant from the University of Zurich for protected research time. The funders had no role in the design of the study, data collection or analysis, the decision to publish, or preparation of the manuscript. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We are grateful to our patients for their commitment, and we thank Bettina Ruehe, Christian Rüegg, Aline Wolfensberger, Ulrich Matt, Lyubov Chaykovska, and Marie-Carmen Romero-Toledo for excellent patient care. We also thank Caroline Müller and Simone Bürgin for serving as our study nurses, and Christine Laich and Andrea Thoma for administrative assistance. The members of VASGRA are Guido Bloemberg, Barbara Hasse, Lars Husmann, Mario Lachat, Dieter Mayer, Zoran Rancic, Alexandra Scherrer, Rainer Weber, and Annelies Zinkernagel.
Footnotes
↵* Contributed equally to this work.
Published online May 14, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 20, 2015.
- Accepted for publication April 27, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}