


Abstract
Despite early detection programs, many patients with prostate cancer present with intermediate- or high-risk disease. We prospectively investigated whether 11C-acetate PET/CT predicts lymph node (LN) metastasis and treatment failure in men for whom radical prostatectomy is planned. Methods: 107 men with intermediate- or high-risk localized prostate cancer and negative conventional imaging findings underwent PET/CT with 11C-acetate. Five underwent LN staging only, and 102 underwent LN staging and prostatectomy. PET/CT findings were correlated with pathologic nodal status. Treatment-failure–free survival was estimated by the Kaplan–Meier method. The ability of PET/CT to predict outcomes was evaluated by multivariate Cox proportional hazards analysis. Results: PET/CT was positive for pelvic LN or distant metastasis in 36 of 107 patients (33.6%). LN metastasis was present histopathologically in 25 (23.4%). The sensitivity, specificity, and positive and negative predictive values of PET/CT for detecting LN metastasis were 68.0%, 78.1%, 48.6%, and 88.9%, respectively. Treatment failed in 64 patients: 25 with metastasis, 17 with a persistent postprostatectomy prostate-specific antigen level greater than 0.20 ng/mL, and 22 with biochemical recurrence (prostate-specific antigen level > 0.20 ng/mL after nadir) during follow-up for a median of 44.0 mo. Treatment-failure–free survival was worse in PET-positive than in PET-negative patients (P < 0.0001) and in those with false-positive than in those with true-negative scan results (P < 0.01), suggesting that PET may have demonstrated nodal disease not removed surgically or identified pathologically. PET positivity independently predicted failure in preoperative (hazard ratio, 3.26; P < 0.0001) and postoperative (hazard ratio, 3.07; P = 0.0001) multivariate models. Conclusion: In patients planned for or completing prostatectomy, 11C-acetate PET/CT detects LN metastasis not identified by conventional imaging and independently predicts treatment-failure–free survival.
Although many patients in the United States with newly diagnosed prostate cancer have low-risk disease, 40%–50% have intermediate- or high-risk localized disease (1,2). Up to 20% of these patients have metastatic disease, usually in lymph nodes (LNs). Identification of LN involvement is important for treatment planning (3,4). These patients typically undergo CT or MR imaging. However, neither is sensitive for detecting nodal metastasis unless the nodes are enlarged (4). In a recent meta-analysis, the sensitivity of CT and MR imaging was 39%–42% for detecting pelvic LNs (5). MR imaging with ultrasmall superparamagnetic iron oxide contrast material (which is not available in the United States) and diffusion-weighted MR imaging appear to have improved sensitivity (6), but experience is still limited.
Because of the unreliability of imaging, nomograms based on clinical parameters, such as prostate-specific antigen (PSA), T stage, and Gleason score, are used to estimate the risk of nodal metastasis (3,7,8) and may justify omission of lymphadenectomy in patients with an estimated risk of less than 5% since there is an 8%–20% complication rate for lymphadenectomy (9,10). This approach is not ideal, however, as in some cases the disease will be under-staged.
PET allows for detection of characteristic biochemical attributes of malignant cells and is not dependent on size criteria alone. PET with 18F-FDG effectively stages many cancers but has limited utility for initial staging of prostate cancer because urinary excretion may obscure nodal uptake; additionally, most prostate cancers have low rates of glucose metabolism, and 18F-FDG uptake is similar in prostate cancer, benign prostatic enlargement, and inflammation (11,12).
Because of these limitations, other radiopharmaceuticals have been investigated for prostate cancer imaging, including 11C-acetate (11,13). Acetate enters the biochemical pathways of fatty acid metabolism, which are consistently upregulated in prostate cancer cell lines (14), and 11C-acetate has minimal urinary excretion (15). Although multiple studies have demonstrated promising results with 11C-acetate PET for diagnosing local and distant disease after initial treatment failure (16–20), less is known about its value for initial prostate cancer staging (21).
The purpose of this prospective study was to investigate PET/CT with 11C-acetate for nodal staging and as a biomarker for prediction of treatment failure in patients with newly diagnosed intermediate- or high-risk disease, for whom radical prostatectomy was planned and conventional staging was negative for metastasis.
MATERIALS AND METHODS
This study was conducted within a larger prospective study (http://www.clinicaltrials.gov, NCT00121212) investigating 11C-acetate PET/CT for staging of disease in patients with newly diagnosed prostate cancer for whom radical prostatectomy or radiation therapy was planned. The study was approved by the institutional review board at Washington University. All subjects gave written informed consent.
Patients and Eligibility Criteria
The patient flow diagram of the study is shown in Figure 1. From October 2003 to November 2009, 177 men with newly diagnosed biopsy-proved prostate cancer who were judged to be at intermediate or high risk for nodal metastasis and had negative abdominopelvic CT (or pelvic MR imaging) and bone scintigraphy findings underwent 11C-acetate PET/CT. Intermediate- or high-risk patients were defined as those with a Gleason score of 7 and a PSA level of at least 10 ng/mL, a Gleason score of at least 8 and any PSA level, or any Gleason score and a PSA level of more than 20 ng/mL. Patients were excluded from this analysis if they elected to have primary radiation therapy (n = 59), had hormonal therapy before PET/CT (n = 7), or were lost to follow-up after PET/CT (n = 4). The remaining 107 patients for whom radical prostatectomy was planned comprise the cohort of this report. All these patients underwent CT (rather than MR imaging) for preenrollment staging.

Patient flow diagram.
11C-Acetate PET/CT
PET/CT was performed on either a Biograph Duo (n = 110) or a Biograph 40 (n = 67) scanner (Siemens). 11C-acetate, 1.48 GBq for studies on the Biograph Duo and 0.74 GBq for studies on the Biograph 40, was administered intravenously. Approximately 10–15 min after injection, a 10- to 20-s CT topogram was obtained from the skull base through the pelvis. On the basis of the topogram, the tube current for the CT scan was adjusted so that the effective current was between 95 and 111 mAs. The tube voltage was 130 kVp (Biograph Duo) or 120 kVp (Biograph 40). Reconstructed images were of slices 5 mm thick. Immediately after the CT scan, emission images beginning at the pelvis and proceeding cranially were obtained. Emission images ranged from 2 to 5 min in duration for each of the 6–8 bed positions.
Image Interpretation
Each PET/CT study was reviewed preoperatively by an experienced nuclear radiologist and a genitourinary radiologist, first independently and then jointly. Their consensus interpretation was used for this analysis. The radiologists were aware of the diagnosis of prostate cancer, Gleason score, and PSA level, as defined by the study eligibility criteria. Considering the normal biodistribution of 11C-acetate, the radiologists graded the presence or absence of metastasis on PET/CT imaging (pelvic or distant LN or distant organ metastasis) on a 5-point ordinal scale from 0 to 4, where 0 is definitely normal and 4 is definitely abnormal. Scans graded 2–4 were considered PET-positive. In addition, all PET images were evaluated semiquantitatively by determination of the maximum standardized uptake value within the prostate gland.
Treatment and Pathologic Evaluation
To allow for assessment of the impact of PET on patient management, neither patients nor their treating physicians were masked to the results of 11C-acetate PET/CT. The information was available for clinical decision making, such that patients could be diverted from prostatectomy if PET demonstrated metastasis that was confirmed before surgery by biopsy. The management of each patient was documented by medical record review.
The surgical approach, laparoscopic or open, and lymphadenectomy boundaries were left to the discretion of the surgeon. However, lymphadenectomy involved, at a minimum, removal of nodes within the obturator fossae (external iliac artery anteriorly, pelvic sidewall laterally, obturator nerve inferiorly, and Cooper ligament distally). Nodal metastatic status was based on the pathology findings from final biopsy or lymphadenectomy. The pathologists did not know the results of PET/CT.
Follow-up and Assessment of Treatment Failure
Patients were followed every 3–6 mo postoperatively with physical examination and serum PSA measurement.
Treatment failure was defined as one of the following events: pathologic diagnosis of metastasis by biopsy or surgery, a persistently detectable PSA level of more than 0.20 ng/mL at least 4 wk after surgery, or subsequent biochemical recurrence with a PSA level of more than 0.20 ng/mL and rising (with the failure event dated to the first occurrence). The time to treatment failure was defined as the time from PET/CT until the failure event. Patients given adjuvant therapy without biochemical recurrence, because of high pathologic T stage or positive margins in the prostatectomy specimen, were not considered to have experienced treatment failure. For assessment of treatment-failure–free survival, patients who did not have treatment failure were censored at the last follow-up date. Seven patients died after either their date of disease progression or their last follow-up visit; thus, none of these deaths was considered to be within the study interval.
Statistical Analysis
The 11C-acetate PET/CT findings of LN metastasis were correlated with the histologic findings on a per-patient basis to calculate the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for PET detection of nodal metastasis. Continuous and categoric variables between PET-positive and PET-negative patients (with respect to nodal or distant metastasis) were compared by a Kruskal–Wallis test and the Fisher exact test, respectively. Treatment-failure–free survival for PET-positive and PET-negative patients was examined using Kaplan–Meier analysis and a log-rank test. Univariate predictors of treatment failure included biopsy Gleason score, percentage biopsy core–positive, PSA level, clinical stage, PET positivity, prostate maximum standardized uptake value, pathologic Gleason score, pathologic stage, and surgical margin status. Preoperative and postoperative multivariate Cox proportional hazards analyses evaluated the independent predictive ability of PET status while controlling for these covariates. The assumption of proportionality was tested and met for Cox analysis. A P value of less than 0.05 was considered statistically significant for all study outcomes, and all statistical tests were 2-sided. SAS software, version 9 (SAS Institute Inc.), was used to perform statistical analyses.
RESULTS
The demographic, clinical, and pathologic data of the patients are summarized in Table 1. Median age was 61 y, and median PSA level was 11.8 ng/mL. Clinical T stage was T1 in 66.7% of patients, and biopsy Gleason scores were 8–10 in 58.9%.
Clinical and Pathologic Demographic Information
11C-Acetate PET/CT Findings
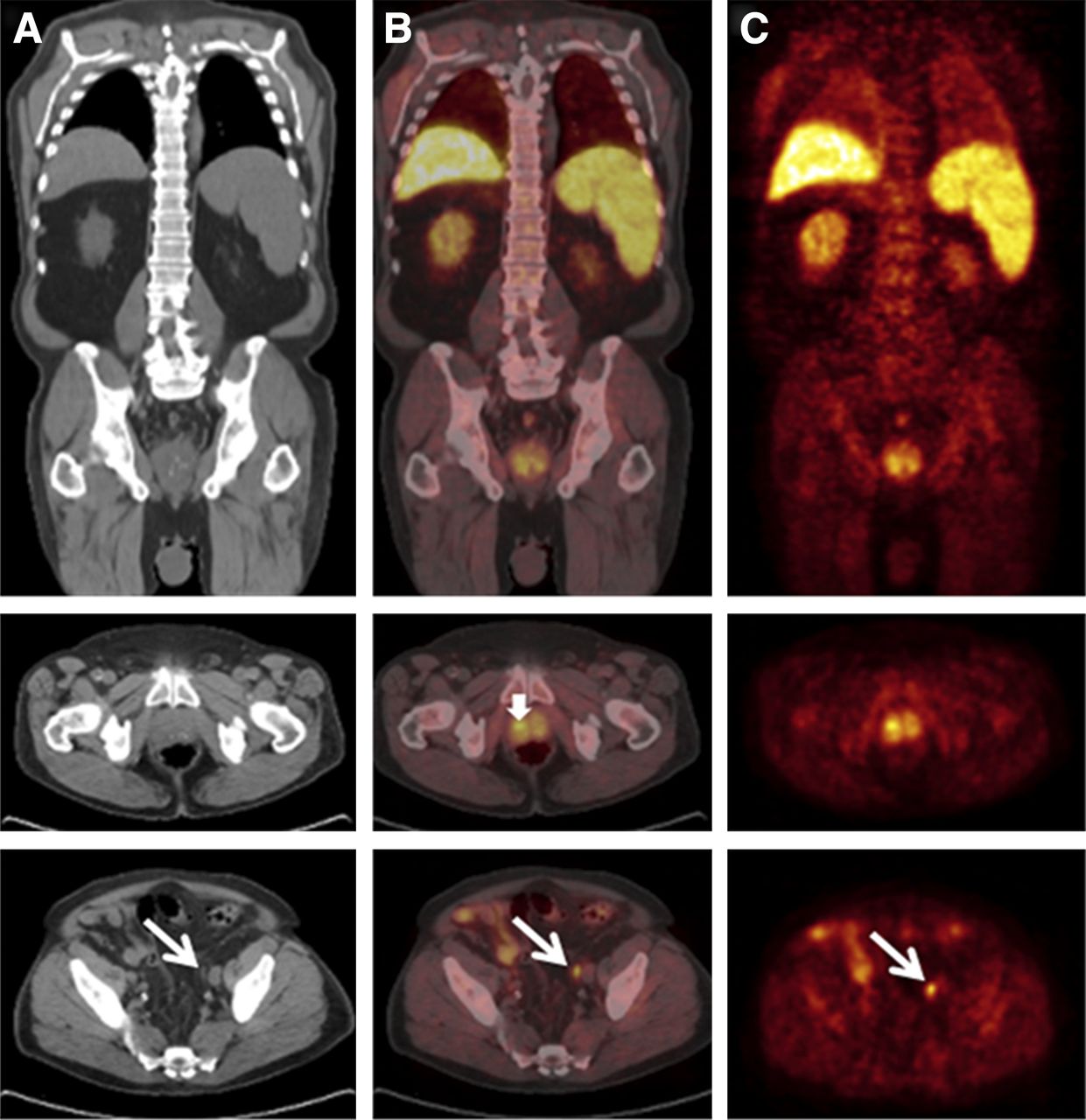
A representative scan with 11C-acetate PET/CT–positive findings in both the prostate gland and a pelvic LN is shown in Figure 2.
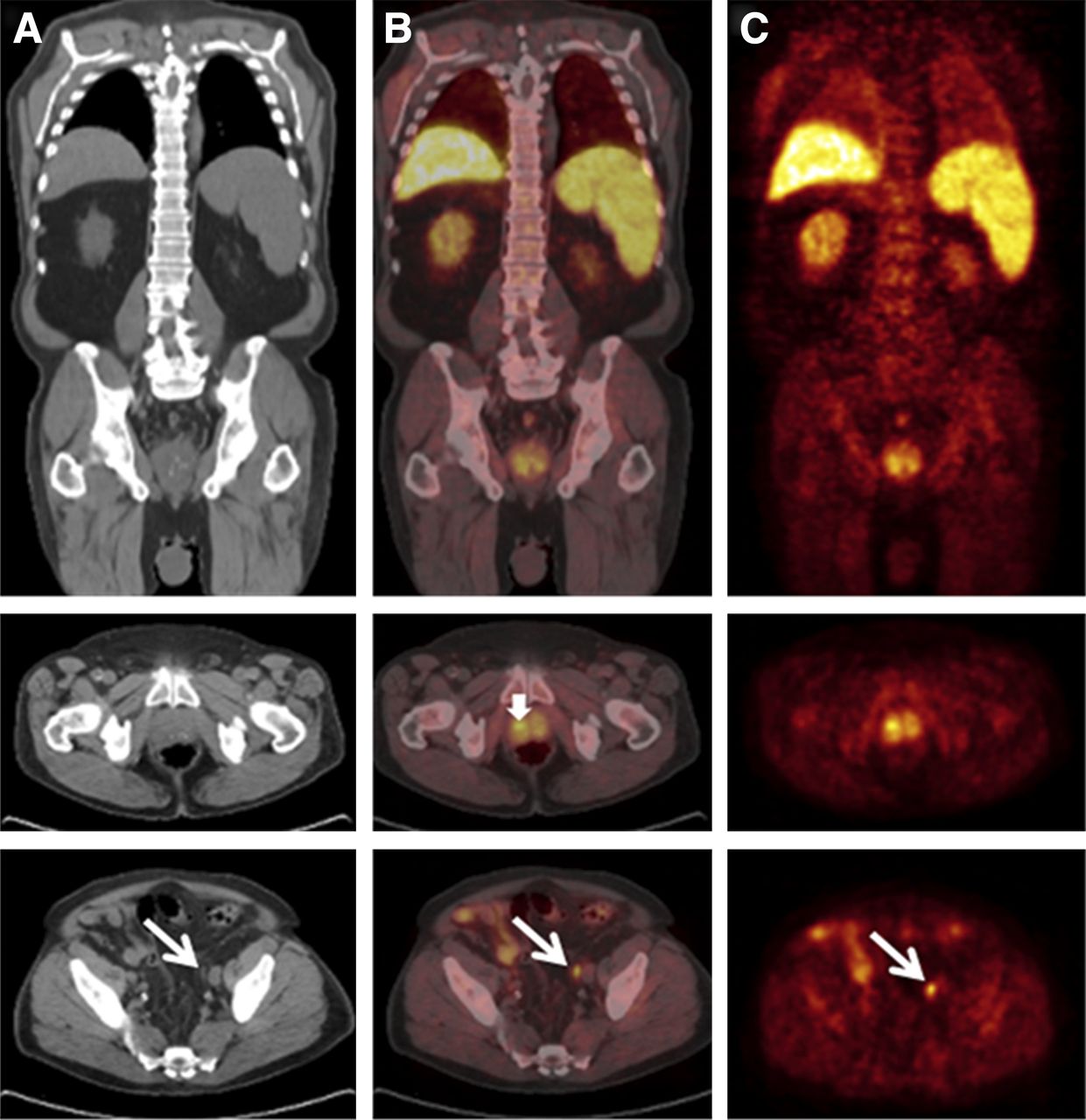
Representative 11C-acetate CT (A), PET/CT (B), and PET (C) images of patient with prostate cancer in 4 quadrants and unsuspected LN metastasis. Gleason score was 8, and PSA level was 6.4 ng/mL. Diffusely increased 11C-acetate uptake was noted within prostate gland and was most intense in right lobe (maximum standardized uptake value, 8.4; short arrow). Long arrows point to normal-sized left external iliac LN, which was proved to harbor metastatic disease.
On the 11C-acetate PET/CT images, focally or diffusely increased activity, presumably representing abnormal tracer uptake in the primary tumor, was recorded in the prostate gland in 103 of the 107 patients (96.3%). The mean maximum standardized uptake value (±SD) in these 103 prostate glands was 5.4 ± 1.8. In no instance was 11C-acetate PET/CT positive in LNs but negative in the prostate gland.
11C-acetate PET/CT demonstrated metastasis in 36 (33.6%) of 107 patients. Of these, 35 had LN metastasis (32 in pelvic LNs only, 2 in pelvic LNs and a distant node [1 supraclavicular and 1 paratracheal], and 1 in pelvic LNs and bone), and 1 patient had bone metastasis only. The 2 patients with PET findings of bone metastasis were negative for skeletal foci on MR imaging and underwent prostatectomy as planned; both were considered to have experienced treatment failure on the basis of a persistently increased PSA level after prostatectomy. As is shown in Table 1, the 36 PET-positive patients were more likely than the 71 PET-negative patients to have higher prostatectomy Gleason scores and a higher pathologic stage but otherwise had similar clinical features.
Pathology Findings
One-hundred two patients underwent prostatectomy and lymphadenectomy, and 5 underwent LN sampling only (1 with fine-needle aspiration of distant nodes only and 4 with pelvic lymphadenectomy). Four of the 5 patients with only nodal sampling had metastasis and were defined as having had a treatment failure. The remaining patient had negative pathology findings but opted for radiation therapy (and was excluded from the treatment failure analysis). Of the 102 patients undergoing prostatectomy and lymphadenectomy, 21 (20.6%) had nodal metastasis.
11C-Acetate PET/CT LN Staging
On a per-patient basis, the overall sensitivity, specificity, PPV, and NPV of PET/CT for detection of LN metastasis were 68.0%, 78.1%, 48.6%, and 88.9%, respectively (Table 2).
Correlation of PET/CT and Pathologic Results for Nodal Metastasis (Per-Patient Basis)
Treatment-Failure–Free Survival Analysis
Failure Events
The cohort for treatment failure analysis consisted of 106 patients; 1 patient with positive PET findings had a negative result from LN biopsy, opted for radiotherapy, and was excluded from the failure analysis. Treatment failure occurred in 64 of the 106 patients: 4 diverted from prostatectomy with biopsy-confirmed metastasis, 21 with confirmed nodal metastasis at lymphadenectomy, and 17 with persistently detectable PSA after prostatectomy. Of the remaining 64 patients, 22 had biochemical recurrence during a median follow-up of 44.0 mo (range, 1.2–93.5 mo). Three patients received adjuvant therapy for positive margins without biochemical recurrence and were not considered to have experienced treatment failure at that time.
Univariate Analysis
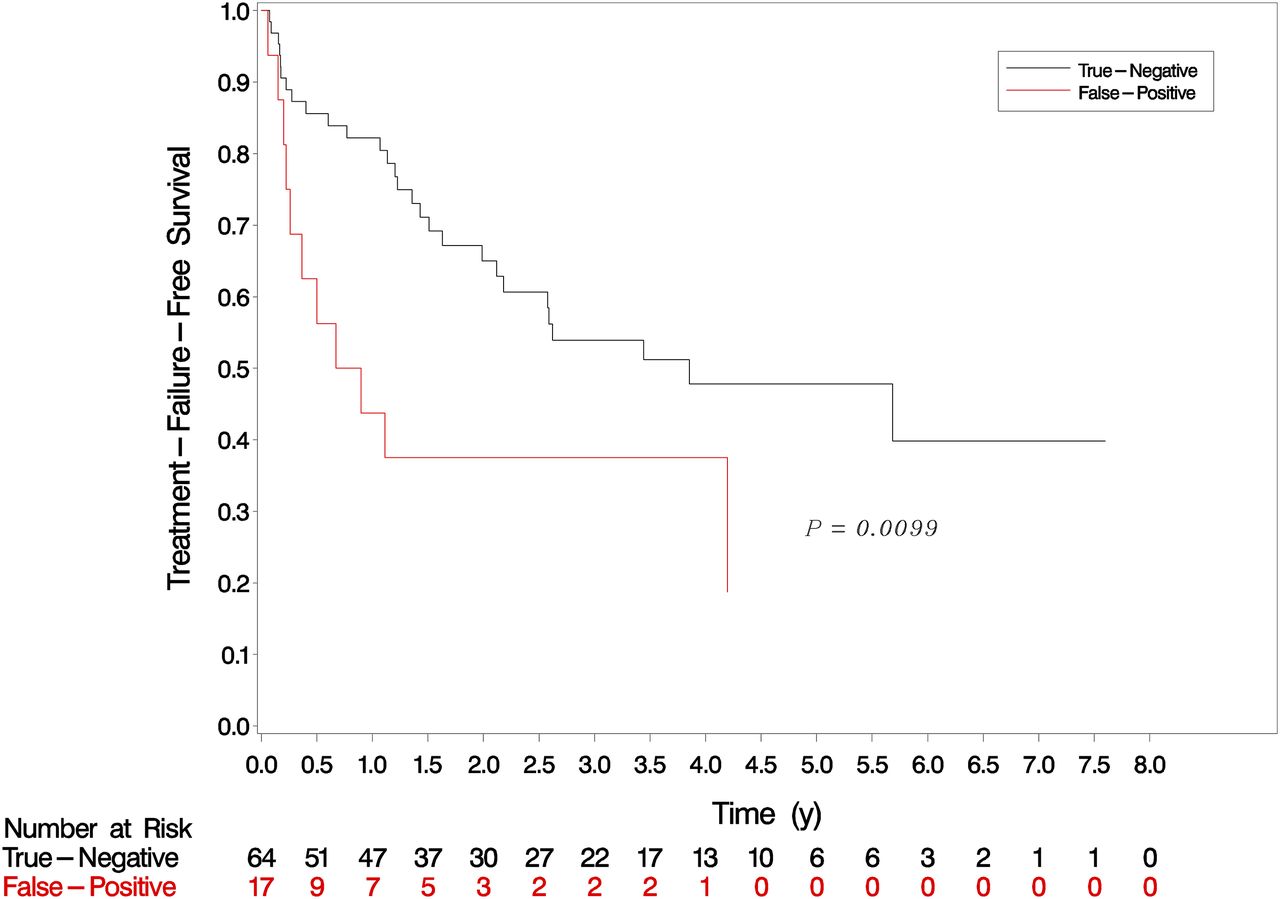
On univariate analysis, factors predicting treatment failure are shown in Table 3. PET/CT positivity for any site of metastasis was significantly associated with poorer treatment-failure–free survival on univariate analysis (hazard ratio, 3.830; P < 0.001) (Fig. 3). The 3-y failure probabilities of PET-negative and PET-positive patients are 51% and 82%, respectively. The median treatment-failure–free survival for PET-positive patients was 1.3 mo, whereas that for PET-negative patients was 31.5 mo. Patients with false-positive PET/CT findings (relative to the pathologic reference standard) had worse treatment-failure–free survival than patients with true-negative PET/CT findings (P < 0.01), suggesting that PET/CT may have demonstrated nodal disease not removed at surgery or not identified in the pathologic specimen (Fig. 4).
Univariate Model for Predicting Treatment Failure

Treatment-failure–free survival of patients who were PET-positive and PET-negative for metastatic disease at any site.

Treatment-failure–free survival stratified by PET/CT results referenced to nodal pathology results.
Multivariate Analysis
On the preoperative multivariate Cox proportional hazards model (Table 4), PET metastasis was significantly associated with a 3.26-fold (95% confidence interval, 1.86–5.72; P < 0.0001) increased risk of treatment failure while controlling for other known preoperative factors (PSA, clinical stage, biopsy Gleason score, and percentage cores positive).
Preoperative Multivariate Cox Proportional Hazards Model for Predicting Treatment Failure (n = 98)
On the postoperative multivariate Cox proportional hazards model (Table 5), PET metastasis was significantly associated with a 3.07-fold (95% confidence interval, 1.73–5.46; P = 0.0001) increased risk of treatment failure while controlling for other postoperative factors (PSA, pathology stage, pathology Gleason score, and surgical margins).
Postoperative Multivariate Cox Proportional Hazards Model for Predicting Treatment Failure (n = 101).
DISCUSSION
Accurate LN staging is important for management of patients with newly diagnosed prostate cancer. CT, the current standard imaging modality, relies primarily on nodal size to identify nodal metastasis and is neither sufficiently sensitive nor sufficiently specific (22). Conventional MR imaging and diffusion-weighted MR imaging have similar limitations (23).
Our study indicated that in patients with negative CT findings, 11C-acetate PET/CT can detect LN metastasis with a sensitivity and specificity of 68% and 78%, respectively. Although the PPV of PET/CT based on pathologic correlation was only 49%, the Cox proportional hazards model for predicting treatment failure showed that patients with an apparent false-positive PET result had a significantly worse prognosis than did those with true-negative PET results, suggesting that the relatively low PPV might be due to inadequate lymphadenectomy or lack of pathologic identification of positive nodes.
Several other studies using either 11C-acetate PET or 11C-choline PET have confirmed the potential of PET for diagnosing metastatic prostate cancer (13). Neither tracer has significant urinary excretion, and both enter into the biochemical pathways of fatty acid metabolism, which are consistently upregulated in prostate cancer cell lines (13). 11C-choline is incorporated into cellular membranes as phosphatidylcholine through overexpression of fatty acid synthetase, whereas 11C-acetate participates in cytoplasmic lipid synthesis, which is believed to be increased in tumors (24).
Compared with other studies using 11C-acetate PET, ours uniquely evaluated the staging of newly diagnosed prostate cancer prospectively by comparing PET with pathologic nodal status as the reference standard. Multiple other studies have evaluated the effectiveness of 11C-acetate PET in prostate cancer (14–21,25). However, most of these studies have focused on patients with recurrent disease, have included heterogeneous patient populations (local recurrence, nodal disease, bone or visceral metastasis) or reference standards, and have been limited by small sample sizes. These studies did not have extensive confirmatory pathologic evaluation of PET-positive disease and relied on the tracer uptake value or follow-up findings to infer that PET positivity represents a true-positive finding (21,25).
11C-choline PET has been studied more extensively for preoperative LN staging. De Jong et al. (26), in examining 67 patients with newly diagnosed prostate cancer who underwent 11C-choline PET/CT, found a sensitivity of 80% and specificity of 96% for detecting nodal metastasis. However, only 24 patients in the study underwent lymphadenectomy, and scan results were assumed to be true-negative on the basis of the clinical scenario in 14 without pathology or to be true-positive in 10 patients who declined surgery and had gross disease seen on preoperative CT scans. Approximately half the patients with nodal metastasis had lymphadenopathy already detectable by standard imaging (CT or MR) and therefore would have been excluded from our study. Also, the patients appeared to be at higher risk for nodal metastasis than ours, with an average PSA level of 34 (range, 3–500) ng/mL, a PSA level greater than 20 ng/mL in 60% of patients, and cT2/3 disease in 75%. Schiavina et al. (27), in examining the 11C-choline PET images of 57 patients with newly diagnosed prostate cancer who had previous negative results on bone scintigraphy and underwent extended pelvic lymphadenectomy, found a sensitivity of 60% and specificity of 97.6%. This sensitivity was similar to that found in our study with 11C-acetate PET (60% vs. 68%), whereas the specificity and PPV were higher than in our study (97.6% vs. 78% and 90% vs. 48%, respectively). However, their patient population overall was at lower risk for nodal metastasis than our population and included more patients with biopsy Gleason scores of 5 or 6 (22 of 57) and fewer with biopsy Gleason scores of 8–10 (8 of 57), likely explaining their high specificity rates. Their higher PPV may also reflect the use of a standardized approach to extended pelvic lymphadenectomy rather than allowing for surgical discretion, as in our study. Whether the differences in sensitivity, specificity, and PPV between these studies are also attributable to differences in performance of these 2 tracers is unclear. Besides differential uptake of 11C-acetate intracellularly and 11C-choline in the cellular membrane, clinically relevant distinctions between these 2 tracers have not been elucidated at this time. However, a single small study indicated that they may be equivalent (28). Similar results for LN metastasis detection have been reported for PET/CT performed with 18F-fluorocholine derivatives (29).
In addition to providing anatomic localization of metastatic disease, the results of 11C-acetate PET/CT were also found in our study to be independently predictive of failure of planned or completed radical prostatectomy in both preoperative and postoperative multivariate models. To our knowledge, this was the first study in which the results of initial staging PET were correlated to treatment failure in prostate cancer patients. Most of the patients with PET/CT-positive disease experienced treatment failure early, either immediately perioperatively or within a few months of surgery. By 1 y, 79% of PET/CT-positive patients had experienced treatment failure, as opposed to 26% of PET/CT-negative patients. 11C-acetate PET/CT may allow for better treatment counseling in patients with high-risk prostate cancer. Knowing that their PET/CT findings were positive, 5 of our patients elected to undergo biopsy before having definitive surgery. Four of these patients were confirmed to have metastasis and received radiotherapy or hormonal therapy, sparing them the potential complications of surgery. 11C-acetate PET/CT may also help to identify patients likely to benefit from multimodality therapy. Currently, studies on neoadjuvant therapy before radical prostatectomy focus on clinical parameters (PSA, biopsy Gleason score, and clinical stage) and are investigational (30,31). Although clinical parameters may identify patients with a high risk of metastasis, they do not provide confirmation of metastasis as PET/CT may.
Although our study avoided some of the pitfalls of past 11C-acetate and 11C-choline PET studies, it was not without limitations. First, patients and surgeons were deliberately not masked to the results of the 11C-acetate PET/CT studies in order to gain an appreciation of the real-world utility of this technology, and this choice may have introduced verification bias. Second, treating urologists were allowed to individualize the limits of lymphadenectomy on the basis of, at least in part, the PET findings. This choice may have contributed to the low PPV of our PET results.
PET/CT for initial staging of prostate cancer is not without drawbacks. Because of the short half-life of 11C (20 min), the widespread use of 11C-acetate (and 11C-choline) is largely limited to centers with on-site cyclotrons. Despite this limitation, it is of interest that 11C-choline recently was approved by the U.S. Food and Drug administration at a single site for use as an adjunct for evaluation of patients with suspected recurrent prostate cancer (32). Newer radiopharmaceuticals labeled with 18F (half-life, 110 min) would overcome this limitation, but none has yet been commercialized (33,34). Additionally, the routine use of PET/CT staging would add a substantial cost to the management of prostate cancer. Only carefully designed studies can determine whether the benefits of PET/CT with 11C-acetate or another radiopharmaceutical for detecting LN metastasis and predicting treatment failure outweigh the expense of the procedure. Until then, pelvic LN dissection, although invasive, remains the gold standard for diagnosing LN disease.
CONCLUSION
Although pelvic lymphadenectomy is the gold standard for diagnosing nodal metastasis, 11C-acetate PET/CT is more sensitive than current imaging methods for staging of men with medium- to high-risk prostate cancer. It may guide initial treatment planning by prompting surgeons to perform a more extended pelvic lymphadenectomy. In patients for whom prostatectomy is planned or has been completed after negative findings on conventional imaging, 11C-acetate PET/CT independently predicts treatment-failure–free survival.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by National Institutes of Health grants CA101734 and P30 CA091842 and the Alvin J. Siteman Cancer Center Biostatistics Core and Imaging and Response Assessment Core. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵† Deceased.
Published online Mar. 7, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 11, 2012.
- Accepted for publication November 26, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preoperative Stating of Pelvic Lymph Nodes in Prostate Cancer Patients via Endorectal Magnetic Resonance Imaging
- Evaluating Acetate Metabolism for Imaging and Targeting in Multiple Myeloma
- 11C-Acetate-PET/CT Compared to 99mTc-HDP Bone Scintigraphy in Primary Staging of High-risk Prostate Cancer
- What Medical, Urologic, and Radiation Oncologists Want from Molecular Imaging of Prostate Cancer
- Evaluation of Prostate Cancer with 11C-Acetate PET/CT
- A Phase I/II Study for Analytic Validation of 89Zr-J591 ImmunoPET as a Molecular Imaging Agent for Metastatic Prostate Cancer
- Misinterpretation of 18F-FDG Studies in Oncology
- Molecular Imaging of Prostate Cancer with PET