


Abstract
Septal penetration of high-energy photons affects quantitative results in imaging of 123I-labeled tracers. We investigated acquisition protocols (collimator choice and energy window setting) and correction methods for estimating the heart-to-mediastinum (H/M) ratio in cardiac 123I-metaiodobenzylguanidine (MIBG) imaging. Methods: Four hours after 123I-MIBG injection, 40 patients successively underwent planar anterior chest imaging with the medium-energy (ME) (ME method) and low-energy high-resolution (LEHR) (LEHR method) collimators. A 20% energy window was used for both collimators. Another 40 patients were imaged successively with the ME collimator and a 20% window (ME method), the low-medium-energy (LME) collimator and a 20% window (LME20 method), and the LME collimator and a 15% window (LME15 method). The H/M ratios obtained by the LEHR, LME20, and LME15 methods were corrected using their correlations with the H/M ratio obtained by the ME method (empiric correction). The 123I-dual-window (IDW) correction was also applied to remove the influence of high-energy photons. Results: Without correction, severe underestimation of the H/M ratio was shown for the LEHR method using the ME method as a standard, and this underestimation increased with increasing H/M ratios. Underestimation substantially decreased using the LME20 method and further using the LME15 method. Empiric correction reduced the error in the H/M ratio by the LEHR method, but the error was still evident. After empiric correction, the H/M ratios with the LME collimator were comparable to those with the ME collimator. The IDW correction only partially reduced underestimation by the LEHR method and caused a small overestimation for the LME15 method. Conclusion: The use of an LME collimator appears to be acceptable for cardiac 123I-MIBG imaging as an alternative to an ME collimator, and the application of a 15% energy window is recommended when an LME collimator is used. Empiric correction is also expected to improve exchangeability between H/M ratios calculated with ME and LME collimators. Neither the use of an LEHR collimator nor the use of IDW correction is recommended.
- 123I-metaiodobenzylguanidine (MIBG)
- collimator
- energy window
- heart-to-mediastinum (H/M) ratio
- septal penetration
A radioiodinated analog of norepinephrine, 123I-metaiodobenzylguanidine (123I-MIBG) accumulates in the sympathetic nerve endings. Cardiac sympathetic imaging with 123I-MIBG has been used to assess disease severity and prognosis in patients with heart failure (1). Recently, its utility has been well recognized in the evaluation of neurodegenerative disorders such as Parkinson disease and dementia with Lewy bodies (2,3). Because the cardiac sympathetic nerve system is diffusely impaired in many patients with heart failure or neurodegenerative disorders, quantitative assessment plays an essential role in cardiac 123I-MIBG imaging. The heart-to-mediastinum (H/M) ratio is calculated as the ratio of count density for the left ventricle to that for the upper mediastinum from anterior planar images and is widely used as a simple, quantitative index of cardiac 123I-MIBG uptake. However, estimates of the H/M ratio are substantially affected by the acquisition protocol and data processing method and vary largely among institutions (4,5). This large variation disturbs the widespread use of cardiac 123I-MIBG imaging, and standardization is being pursued (6–9).
Among technical factors, collimator choice profoundly affects the estimation of the H/M ratio (10,11). Low-energy (LE) collimators are commonly applied to cardiac 123I-MIBG imaging because of their wide availability (6). Because 123I emits high-energy photons of more than 400 keV in addition to 159-keV photons, penetration of the thin septa of an LE collimator may degrade image quality and quantitative accuracy (12–15). The lung accumulates 123I-MIBG to differing degrees, and septal penetration causes contamination of mediastinum counts by lung activity, leading to an underestimation of the H/M ratio (10). Medium-energy (ME) collimators have thicker septa and lower transparency than LE collimators. The use of an ME collimator improves quantitative accuracy in 123I imaging at the expense of spatial resolution (12–15) and is recommended for estimation of H/M ratios (6) because H/M ratios are computed using relatively large regions of interest (ROIs) and depend more on quantitative accuracy in large regions than on spatial resolution.
The use of a low-medium-energy (LME) collimator is another option for 123I imaging. This collimator has characteristics that are intermediate between LE and ME collimators—that is, lower spatial resolution and less septal penetration than an LE collimator and higher spatial resolution and more septal penetration than an ME collimator. Phantom studies have suggested that the H/M ratio is underestimated by the use of an LME collimator, compared with an ME collimator, but the degree of underestimation is small (7,8). Normal values have been reported for 2 groups—LE and LME/ME—according to the collimator used, neglecting differences between the LME and ME collimators (9).
In this study, we imaged each patient after the injection of 123I-MIBG successively with ME and low-energy high-resolution (LEHR) collimators or with ME and LME collimators and calculated the H/M ratio for each collimator. One of the aims of this study was to determine the degree of underestimation of the H/M ratio for LME and LEHR collimators. Additionally, the effect of the energy window width was evaluated in imaging with an LME collimator. In a previous study, the H/M ratio obtained with an LE collimator was corrected using an equation determined by phantom experiments (9). We attempted to correct the H/M ratio obtained with the LEHR or LME collimator and evaluated the utility of correction methods using the value obtained with the ME collimator as a standard reference. First, we corrected the H/M ratio using an empiric equation that was based on the relationship of the values obtained by different acquisition methods. To remove contamination by high-energy photons, the 123I-dual-window (IDW) method has been proposed. The IDW method assesses the degree of contamination based on counts in an energy window set at a high energy level, and previous studies have indicated its utility in estimating the H/M ratio (7,8,16). In the present study, we also evaluated the utility of the IDW method in estimating the H/M ratio.
MATERIALS AND MEDHODS
Subjects
Eighty patients who underwent cardiac 123I-MIBG scintigraphy for evaluation of neurodegenerative disorders were enrolled in this study. They consisted of 2 groups: LEHR and LME. Patients in the LEHR group (16 men and 24 women; mean age ± SD, 72.6 ± 8.3 y) were examined with a LEHR collimator, and those in the LME group (24 men and 16 women; mean age ± SD, 71.5 ± 9.2 y) were examined with an LME collimator. Twelve and 4 patients in the LEHR and LME groups, respectively, had hypertension, and no other significant cardiac disorder was known. The study protocol was approved by the institutional review board of the host institution. All patients gave written informed consent before participating in the study.
Imaging Procedures
Patients in the LEHR group were examined using a dual-head γ-camera with a 1.59-cm-thick sodium iodide crystal (e.cam+; Siemens) at the Kitasato University East Hospital, and those in the LME group were examined using a dual-head γ-camera with a 0.95-cm-thick crystal (e.cam or e.cam Signature; Siemens) at the Kitasato University Hospital. ME and LEHR collimators, provided by Siemens, and an LME general-purpose collimator, provided by Siemens Japan, were used. The physical characteristics of the 3 collimators are presented in Table 1.
Physical Characteristics of Collimators
The patients were injected with 123I-MIBG (Fujifilm RI Pharma) in the supine position. The injected dose was 128.1 ± 10.9 and 134.0 ± 5.2 MBq in the LEHR and LME groups, respectively. For the synthesis of 123I-MIBG, 123I was produced using the 124Xe (p, 2n) 123Cs reaction. This method yields higher purity than methods based on the 124Te (p, 2n) 123I reaction or the 127I (p, 5n) 123Xe reaction (17). Anterior planar imaging and SPECT of the chest were performed 15 min and 4 h after injection for routine clinical evaluation.
For the study purpose, anterior chest views were acquired by 2 or 3 different methods at 4 h after injection. In the LEHR group, images were acquired first with the ME collimator (ME method) and then with the LEHR collimator (LEHR method). A 20% photopeak window was set at 159 keV for both methods. In the LME group, imaging was performed first with the ME collimator and a 20% photopeak energy window (ME method), next with the LME collimator and a 20% window (LME20 method), and then with the LME collimator and a 15% window (LME15 method). In all methods, an additional energy window was set at 235 keV (width, 50%) to assess the degree of contamination from high-energy photons (7,8). Other imaging parameters were as follows: matrix, 256 × 256; zoom factor, 1; and acquisition time, 5 min. When changing collimators, the imaging table was moved, and after the completion of the collimator change, the imaging table was returned to the original position. The patient lay still on the imaging table from the start to the end of imaging by the 2 or 3 methods to ensure consistency in positioning.
Data Analysis
ROIs were placed for the heart and upper mediastinum on the photopeak image obtained with the ME collimator. An irregular ROI was manually drawn over the left ventricle as the heart ROI. A rectangular ROI of 12 × 20 pixels was placed in the upper mediastinum, avoiding lung activity, as the mediastinum ROI. The H/M ratio was defined as the ratio of the mean count in the heart ROI to the mean count in the mediastinum ROI. Using the same ROIs, we computed H/M ratios from the images acquired by the LEHR, LME20, or LME15 method. Because the use of an ME collimator is recommended for calculating the H/M ratio (6), the error was calculated using the H/M ratio by the ME method as a standard and defined as the H/M ratio by the LEHR, LME20, or LME15 method minus the H/M ratio by the ME method. Additionally, H/M ratios by the LEHR, LME20, or LME15 method were corrected on the basis of their relationship with those by the ME method observed in this study to remove systematic errors by the LEHR, LME20, and LME15 methods and obtain values comparable to those by the ME method (empiric correction). The H/M ratios by the ME method were plotted against those by the LEHR method, and linear regression analysis was performed by the least-squares method. The H/M ratio by the LEHR method was converted using the obtained regression equation to an equivalent of the ratio by the ME method. Similar corrections were performed for the H/M ratios by the LME20 and LME15 methods.
Moreover, heart and mediastinum counts were corrected for contamination from high-energy photons by the IDW method, and H/M ratios were calculated from the counts after IDW correction. For IDW correction, counts in the high-energy subwindow corrected for the difference in the window width were subtracted from those in the photopeak window. The IDW correction was applied to the results obtained with the ME collimator and those obtained with the LEHR or LME collimator, and the error was estimated using the IDW-corrected H/M ratio by the ME method as a standard.
ROIs in the LEHR group were set by a technologist of Kitasato University East Hospital, and those in the LME group were set by another technologist of Kitasato University Hospital. A physician confirmed appropriateness of ROI setting in both groups. The physician was responsible for nuclear medicine practice, including acquisition of data and processing of cardiac 123I-MIBG imaging, in both hospitals. When calculating the H/M ratio in clinical practice, the technologists referred to the same samples of ROIs in patients with various degrees of cardiac 123I-MIBG accumulation. For quality control, the physician checked ROIs in all patients and instructed the modification inappropriate ROIs.
Statistical Analysis
Linear regression analysis was performed by the least-squares method to assess the relationships between the H/M ratios by different methods and those between the H/M ratios by the ME method and errors by the LEHR, LME20, or LME15 method.
RESULTS
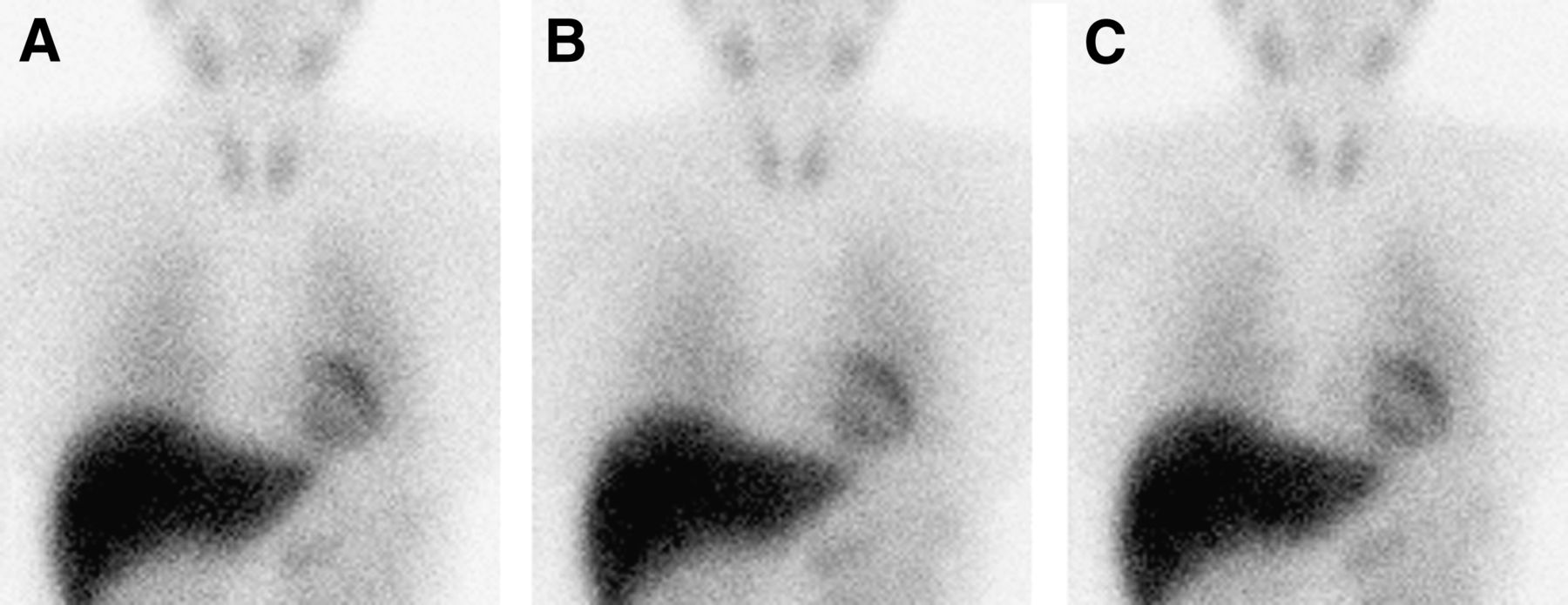
In the LEHR group, background count was larger and image contrast was poorer on the images acquired by the LEHR method than on those acquired by the ME method (Fig. 1). Such difference in image quality was not visually apparent in the LME group (Fig. 2).
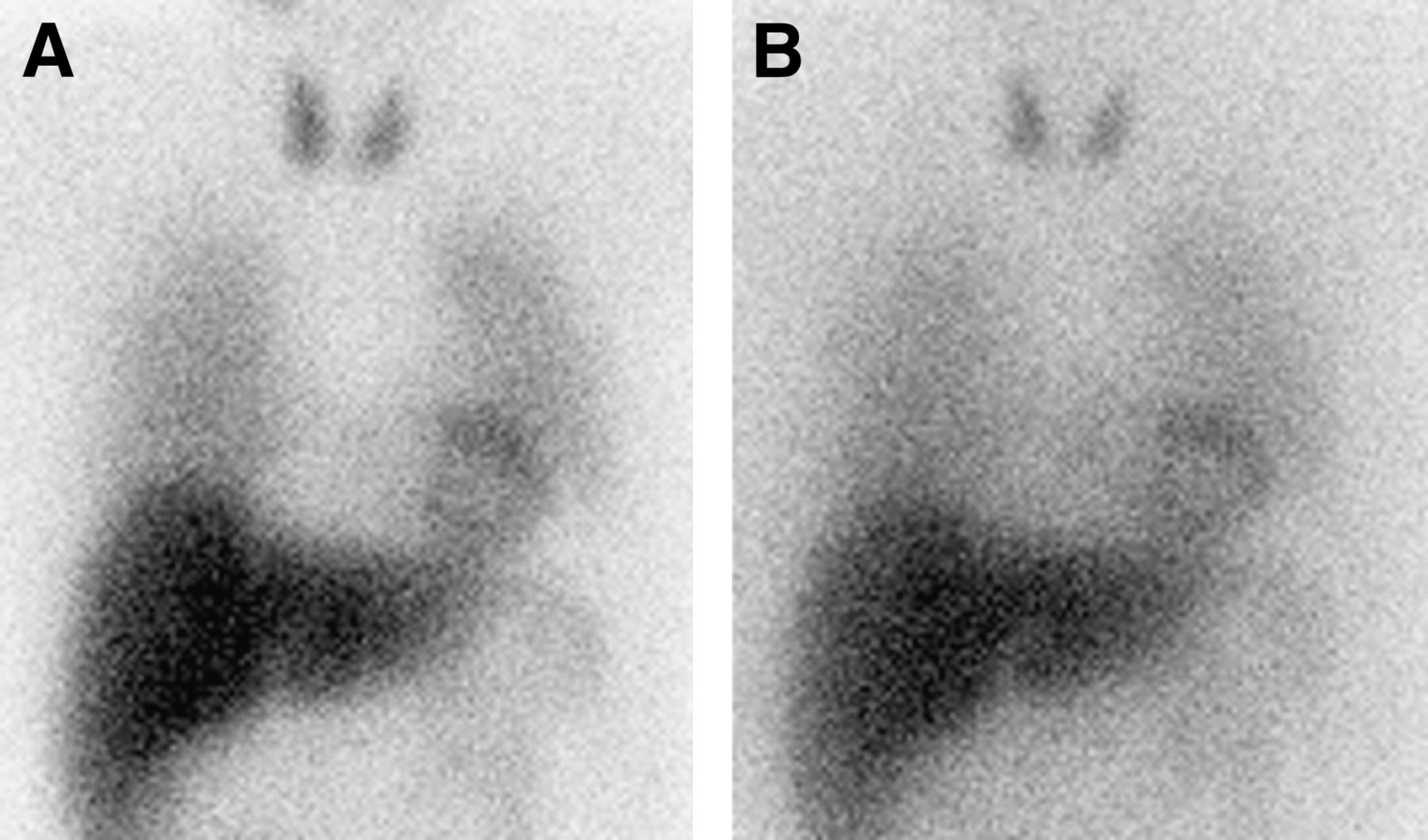
Anterior chest images acquired using ME (A) and LEHR (B) methods in a 79-y-old man. H/M ratio was calculated as 3.41 and 2.13 by ME and LEHR methods, respectively.

Anterior chest images acquired using ME (A), LME20 (B), and LME15 (C) methods in a 75-y-old woman. H/M ratio was calculated as 3.70, 3.39, and 3.60 by ME, LME20, and LME15 methods, respectively.
The means and SDs of the H/M ratios and errors for the various methods are presented in Table 2 (LEHR group) and Table 3 (LME group).
Results of Estimation of H/M Ratios in LEHR Group
Results of Estimation of H/M Ratios in LME Group
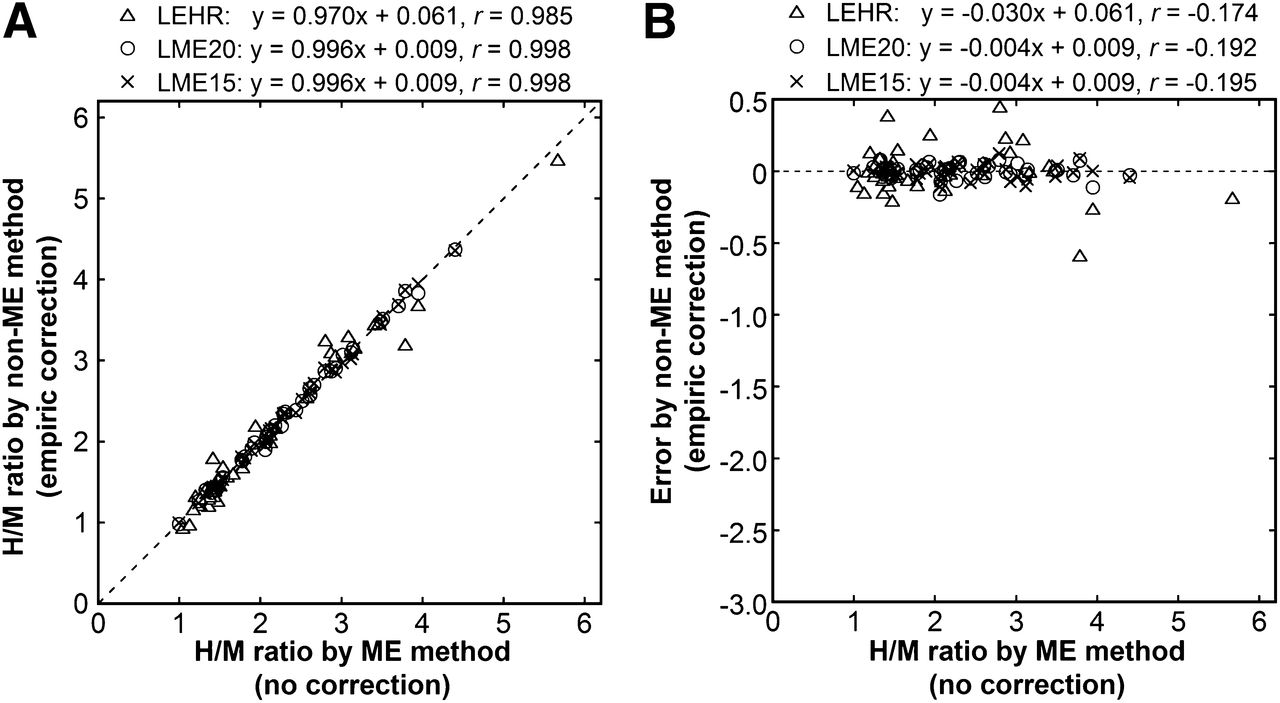
The H/M ratio by the LEHR method was positively correlated with but substantially smaller than that by the ME method (Fig. 3A). Underestimation was mild at low H/M ratios but severe at high H/M ratios, and the error by the LEHR method was negatively correlated with the H/M ratio by the ME method (Fig. 3B).
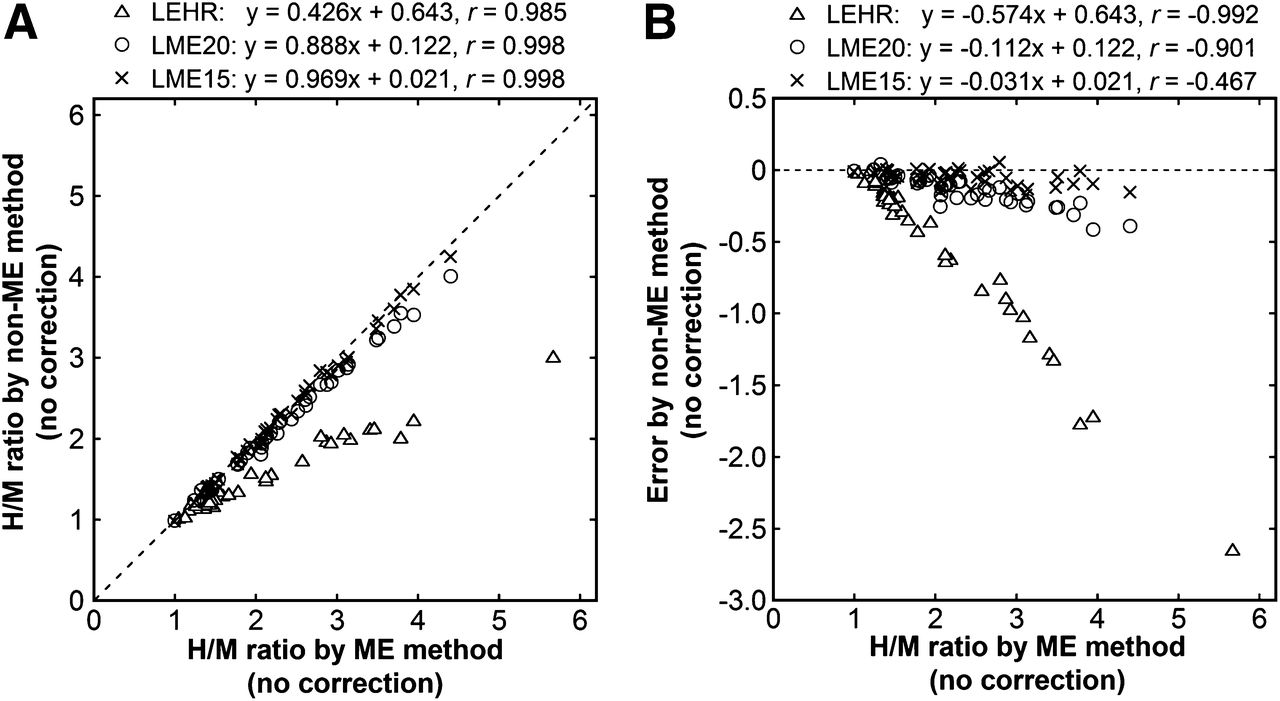
Estimation of H/M ratios with no correction. (A) H/M ratios by non-ME methods, including LEHR, LME20, and LME15 methods, are plotted against those by ME method. Broken line represents line of identity. Regression equations and correlation coefficients are presented. (B) Errors by non-ME methods are plotted against H/M ratios by ME method.
The H/M ratio was also underestimated by the LME20 method (Fig. 3A), and the error was relatively large at high H/M ratios (Fig. 3B). However, underestimation was much smaller for the LME20 method than for the LEHR method. Use of the LME15 method further depressed underestimation of the H/M ratio. The H/M ratio by the LME15 method was highly correlated with the H/M ratio by the ME method, and the regression equation was close to the line of identity (Fig. 3A). The error by the LME15 method was limited irrespective of the H/M ratio (Fig. 3B).
For the plots of the H/M ratios by the ME method over those by the LEHR method, the regression equation was determined as y = 2.278x − 1.403, and empiric correction was performed using this equation. Naturally, the correction removed systematic underestimation of the H/M ratio by the LEHR method (Fig. 4A). The error was reduced but still evident (Fig. 4B), with an SD of 0.18 (Table 2) and a range of −0.58 to 0.45.
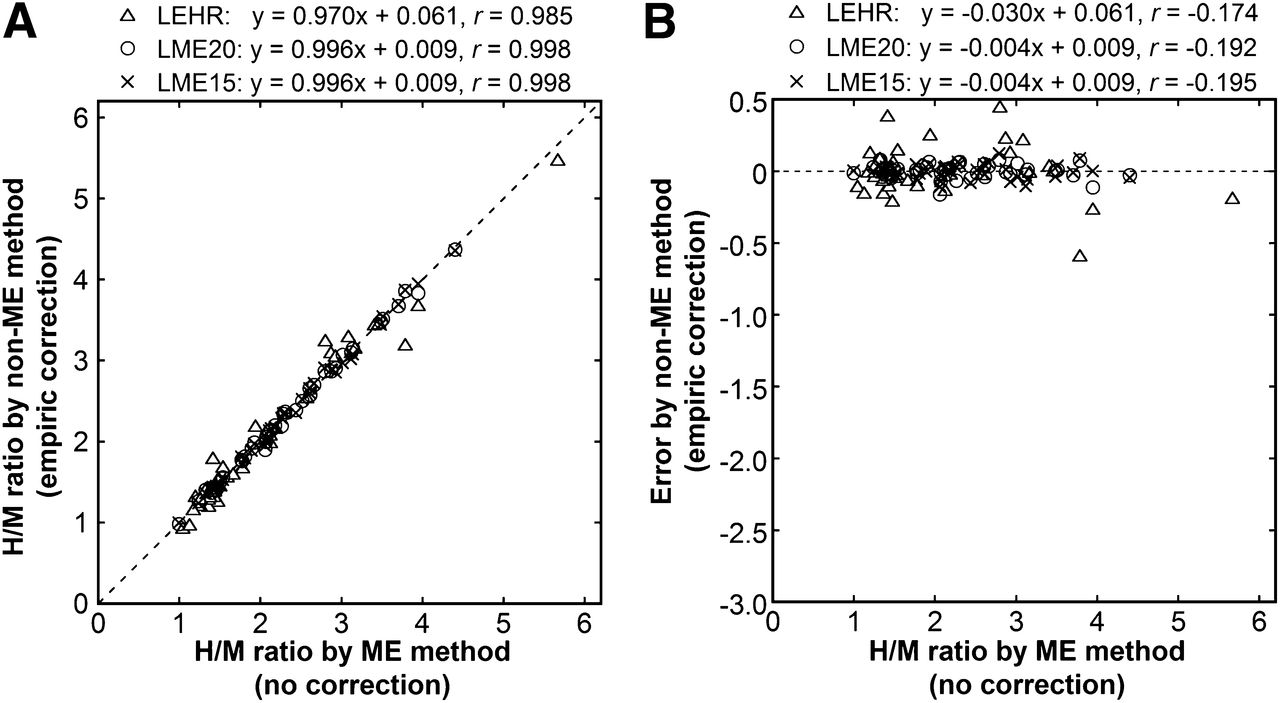
Estimation of H/M ratios with empiric correction. (A) H/M ratios by non-ME methods, including LEHR, LME20, and LME15 methods, are plotted against those by ME method. H/M ratios by non-ME methods were corrected using empiric equation. Broken line represents line of identity. Regression equations and correlation coefficients are presented. (B) Errors by non-ME methods are plotted against H/M ratios by ME method.
The regression equations of the plots of the H/M ratios by the ME method over those by the LME20 and LME15 methods were y = 1.122x − 0.128 and y = 1.029x − 0.012, respectively. When the H/M ratios by the LME20 and LME15 methods were corrected using the corresponding empiric equations, the obtained values were close to the H/M ratio by the ME method (Fig. 4A). The error was negligible irrespective of the H/M ratio (Fig. 4B), and the SD of the error was 0.05 for both methods (Table 3). The range of the error was −0.16 to 0.08 and −0.11 to 0.12 for the LME20 and LME15 methods, respectively.
The IDW correction increased the H/M ratios (Tables 2 and 3). The increase was relatively small but still evident for the ME method. The IDW correction partially reduced underestimation of the H/M ratio by the LEHR method (Fig. 5); however, underestimation was larger for the LEHR method with IDW correction than for the LME20 and LME15 methods with no correction. The IDW-corrected H/M ratio by the LME20 method was almost identical to that by the ME method (Fig. 5A), and the error was negligible irrespective of the H/M ratio (Fig. 5B). For the LME15 method, mild overestimation was noted after IDW correction (Fig. 5A) and was more pronounced at high H/M ratios (Fig. 5B).
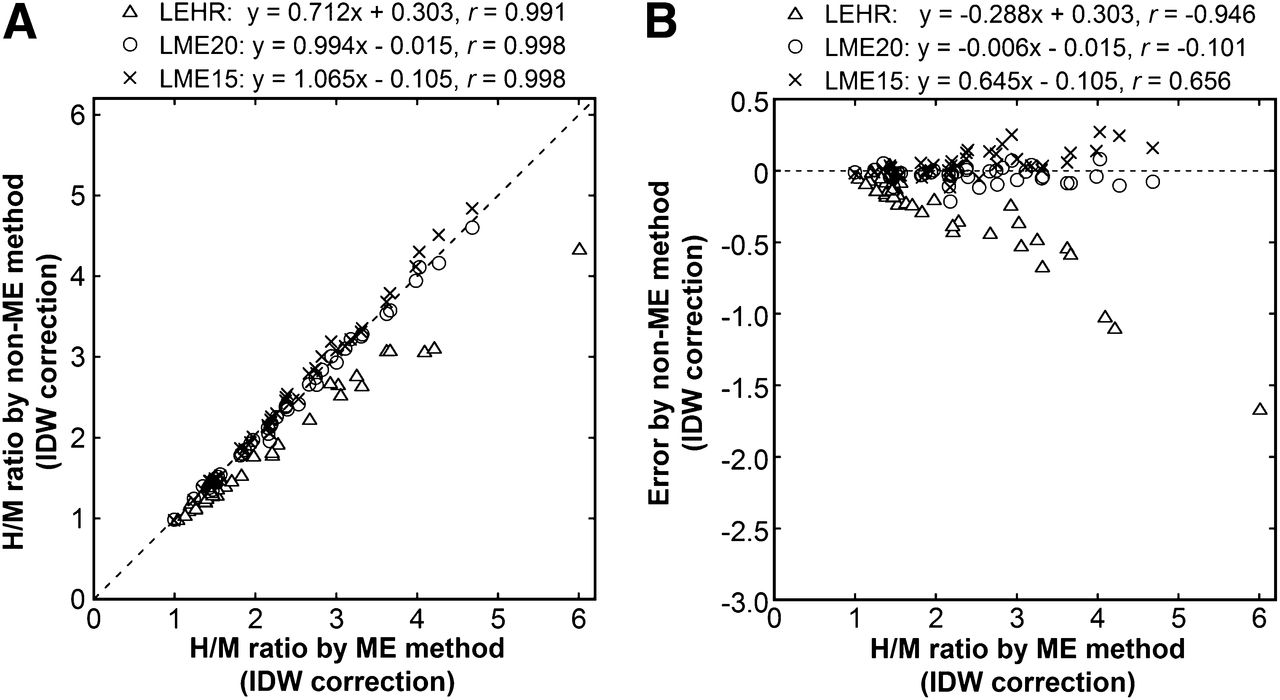
Estimation of H/M ratios with IDW correction. (A) H/M ratios by non-ME methods, including LEHR, LME20, and LME15 methods, are plotted against those by ME method. H/M ratios by ME and non-ME methods were corrected by IDW method. Broken line represents line of identity. Regression equations and correlation coefficients are presented. (B) Errors by non-ME methods are plotted against H/M ratios by ME method.
DISCUSSION
In the present study, we acquired late images of cardiac 123I-MIBG imaging with ME and LEHR collimators in 40 patients and with ME and LME collimators in another 40 patients and compared H/M ratios between collimators. Phantom studies have indicated that septal penetration degrades accuracy in estimating the H/M ratio using an LEHR collimator and that an ME collimator provides better accuracy (10,11). Underestimation of the H/M ratio using LEHR collimators has been demonstrated by successive imaging of a given patient with LEHR and ME collimators. The H/M ratios were 1.81 ± 0.29 and 2.66 ± 0.74 for LEHR and ME collimators, respectively, in one study conducted on 8 patients (10), and 1.86 ± 0.23 and 2.56 ± 0.46 for LEHR and ME collimators, respectively, in another study conducted on 10 patients (7). In the present study, we confirmed severe underestimation using an LEHR collimator in a larger patient population. Such underestimation makes it difficult to compare values obtained in different facilities using different collimators (4,5). We also assessed the relationship between cardiac accumulation and underestimation. In data analysis, because of better accuracy using an ME collimator, we regarded the H/M ratio obtained with the ME collimator as the standard reference and calculated the error resulting from the use of the LEHR or LME collimator instead of assessing the difference against the average. The error by the LEHR method was negatively correlated with the H/M ratio by the ME method. The more severe underestimation in patients with better cardiac accumulation decreases differences in H/M ratios between patients with different degrees of cardiac accumulation and may distort the ability of cardiac 123I-MIBG imaging to detect and grade impairment of cardiac sympathetic nerve function.
When the width of the photopeak energy window was 20%, the LME collimator provided mildly smaller H/M ratios than the ME collimator, indicating mild underestimation due to septal penetration. This underestimation was not observed for patients with low cardiac accumulation but increased with increasing cardiac accumulation. Because the underestimation was small, the use of an LME collimator as an alternative to an ME collimator appears to be acceptable when an ME collimator is not available; however, the difference in estimated H/M ratios may have a small but substantial impact on clinical classification of the status of cardiac sympathetic nerve function in patients with mild or moderate impairment. Although normal values have been reported without discrimination between the LME and ME collimators (9), determination of normal values for each collimator appears to be desirable.
Reduction in the width of the energy window from 20% to 15% decreased the difference in estimated H/M ratios between the ME and LME collimators. The H/M ratios were underestimated with the LME collimator and a 15% window, when compared with the ME collimator and a 20% window; however, the degree of underestimation was limited. This likely occurred because narrowing of the photopeak window decreases the contribution of counts derived from high-energy photons to counts detected in the photopeak window. Although the window width is generally 20% in cardiac 123I-MIBG imaging (6), the use of a 15% window is recommended when an LME collimator is used. This adjustment of the energy window appears to allow an exchange of H/M ratios between ME and LME collimators.
We attempted to correct the H/M ratios obtained with LEHR and LME collimators and evaluated the accuracy of the correction using the values obtained with the ME collimator as the standard. In a previous study, a conversion equation was based on phantom experiments, and the H/M ratio obtained with an LE collimator was corrected using the equation (9). The correction improved normality of the distribution of normal data and discrimination between probable Alzheimer disease and probable dementia with Lewy bodies; however, no validation using standard values has been reported. In the present study, we determined a conversion equation for each acquisition protocol empirically based on the patient data. When the LEHR collimator was used for data acquisition, a large variation in errors remained after correction despite disappearance of systematic error, and the mean − 2SDs and mean + 2 SDs of the error were −0.34 and 0.34, respectively. Although the effect of septal penetration depends on the intensity of accumulation in the lung and liver and relative positions of the organs, such factors were neglected in our empiric correction as in the previous phantom-based correction, which appears to be responsible for the residual errors.
For the LME collimator, empiric correction yielded successful results and improved exchangeability between H/M ratios determined with the ME and LME collimators. Excellent agreement between mean values is natural because the creation and validation of the conversion equation were performed in the same patient population; however, the small variation in errors is noteworthy. The mean − 2 SDs and mean + 2 SDs of the error were −0.10 and 0.10, respectively, for both energy windows. For the LME collimator, the degree of and variation in underestimation of the H/M ratios were small even without correction, which appears to have contributed to the success of the simple correction. In the future, the correction method should be validated in different patient populations. Additionally, the conversion equation needs to be determined for each collimator. Determination of a conversion equation using a phantom (9) offers convenience and may provide acceptable accuracy for LME collimators provided by different manufacturers.
The triple-energy-window (TEW) method is a representative method for scatter correction and may remove scatter counts derived from both 159-keV photons and high-energy photons in 123I imaging. However, previous studies have demonstrated that TEW correction yields inconsistent results in estimating H/M ratios, and the application of the TEW method to cardiac 123I-MIBG imaging has not been recommended (10,11). Instead, the IDW method neglects scatter counts from 159-keV photons and attempts to eliminate the effect of high-energy photons alone. The IDW correction has been shown to reduce collimator-dependent differences in H/M ratios (7,8,16). In the present study, the IDW correction increased the H/M ratios, probably due to a reduction in the contamination of mediastinum counts by high-energy photons. This correction partially reduced underestimation of the H/M ratio with the LEHR collimator; however, considerable underestimation remained. When the LME collimator was used, the IDW correction reduced errors with a 20% window but caused overestimation for a 15% window. Taken together, these results indicate that the reliability of the IDW correction is questionable, and it is not recommended for use in estimation of H/M ratios.
The ME collimator restricts septal penetration but usually has low spatial resolution. The H/M ratios are calculated from counts in relatively large ROIs, and quantitative accuracy is more important than spatial resolution. Thus, the ME collimator is suitable for the estimation of H/M ratios (6,10,11). In cardiac SPECT with 123I-labeled tracers, however, spatial resolution is more important to obtain high-quality images (18). In cardiac 123I-MIBG imaging, although H/M ratios representing global cardiac sympathetic nerve function usually play a chief role in interpretation, SPECT enables the detection of regional impairment and may be more important than the calculation of H/M ratios in some applications such as investigation of arrhythmias (19). The selection of an optimal collimator in cardiac 123I-MIBG imaging might depend on the relative priority of the calculation of H/M ratios and SPECT in a given application, possibly resulting in selection of an LME collimator, based on its better spatial resolution, instead of an ME collimator. Additionally, some nuclear medicine facilities lack ME collimators. Although the use of an ME collimator is recommended to estimate H/M ratios, the use of an LME collimator appears to be acceptable for practical reasons. It generates minimal error in estimated H/M ratios, and the use of a 15% energy window and empiric correction further reduce the error. We cannot recommend the use of an LEHR collimator because of inaccuracy in estimating H/M ratios and low quality of SPECT images (18).
The LEHR and LME groups were studied in different hospitals, which is a major limitation of the present study. The distribution of the H/M ratios obtained with the ME collimator differed between the LEHR and LME groups, and the LEHR group included many patients with severely decreased H/M ratios. The thickness of the scintillator of the γ-camera differed between the groups, and its effect should be investigated in the future. Additionally, the actual clinical impact of the relatively small inaccuracy in estimated H/M ratio remains to be determined for the LME collimator.
CONCLUSION
In the present study, we compared the H/M ratios from cardiac 123I-MIBG imaging between acquisition protocols and evaluated the utility of correction methods. The use of an LME collimator appears to be acceptable depending on clinical situations, and the application of a 15% energy window is recommended to reduce underestimation of H/M ratios when an LME collimator is used. Empiric correction is also expected to improve exchangeability between the H/M ratios calculated with ME and LME collimators. The use of an LEHR collimator is not recommended, although empiric correction partially reduces the error in estimated H/M ratio. The IDW correction does not provide successful results.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank radiological technologists of the Department of Radiology, Kitasato University Hospital, and the Department of Radiology, Kitasato University East Hospital, for their cooperation in the present study.
Footnotes
Published online Mar. 27, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 27, 2012.
- Accepted for publication November 26, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}