


Abstract
The aim of this retrospective study was to compare the heart-to-mediastinum ratio (HMR) of 123I-metaiodobenzylguanidine (123I-MIBG) uptake obtained using a multipinhole cadmium–zinc–telluride (CZT) camera with that obtained using conventional planar imaging. Methods: Forty consecutive heart failure patients underwent planar acquisition 4 h after 123I-MIBG injection (191 ± 41 [mean ± SD] MBq). To localize the heart using the CZT camera, 99mTc-tetrofosmin (358 ± 177 MBq) was administered and dual-isotope acquisition was performed. The HMRs were calculated with conventional planar imaging (HMRplanar), with anterior reprojection images using the CZT camera (HMRreproj), and with transaxial reconstructed images using the CZT camera (HMRtransaxial). In a phantom study, we estimated a linear model fitting the CZT camera data to the planar data, and we applied it to provide corrected CZT camera–determined HMRs in patients (cHMRreproj and cHMRtransaxial). Results: Thirty-four men and 6 women (71 ± 9 y old) with ischemic (22 patients) and nonischemic (18 patients) heart failure completed the study. For 22 of the 40 patients (55%), the New York Heart Association classification was class II and the ejection fraction was 35% ± 9%. HMRreproj (1.12 ± 0.19) and HMRtransaxial (1.35 ± 0.34) were lower than HMRplanar (1.44 ± 0.14) (P < 0.0001 and P < 0.01, respectively). cHMRreproj (1.54 ± 0.09) and cHMRtransaxial (1.45 ± 0.14) were significantly different (P < 0.0001). Lin concordance correlation and Bland–Altman analysis demonstrated an almost perfect concordance and a high agreement between HMRplanar and cHMRtransaxial (P was not significant) but not between HMRplanar and cHMRreproj (P < 0.0001). Conclusion: This study demonstrated that determination of the late HMR of cardiac 123I-MIBG uptake using dual-isotope (123I and 99mTc) acquisition on a multipinhole CZT camera was feasible in patients with heart failure. However, this determination should be performed using transaxial reconstructed images and linear correction based on phantom data acquisitions.
Impairment of cardiac sympathetic innervation assessed with 123I-metaiodobenzylguanidine (123I-MIBG) has been recognized as an independent prognostic factor in patients with heart failure (1–6). The late heart-to-mediastinum ratio (HMR) of 123I-MIBG is a major predictor of sudden death and cardiac events in patients with heart failure. An HMR of less than 1.6 is associated with an increased risk (6). At present, calculation of the HMR requires a planar static image of the thorax. This technique is well standardized and reproducible using a conventional Anger camera (7,8). Recently, dedicated cardiac SPECT cameras using cadmium–zinc–telluride (CZT) detectors dramatically transformed the routine of myocardial perfusion imaging in patients with known or suspected coronary artery disease. These cameras have a better count detection sensitivity, resulting in decreased acquisition times and injected radiopharmaceutical doses, and improved energy resolution, permitting better photon energy discrimination for dual-isotope imaging.
Myocardial perfusion imaging obtained using cardiac CZT cameras has been well validated against that obtained using the conventional Anger camera for the diagnosis of coronary artery disease (9–12). Only a few studies have evaluated myocardial sympathetic innervation imaging with these new-generation detectors (13–16). With the Discovery NM 530c (DNM-530c; GE Healthcare), Gimelli et al. (13,14) assessed regional left ventricular denervation. D’estanque et al. (15) reported the impact of scatter correction in dual-isotope (201Tl/123I-MIBG) cardiac SPECT protocols for the assessment of trigger zones, defined as areas of autonomic nervous system dysfunction in viable myocardium that may contribute to the genesis of ventricular arrhythmia. In the ADRECARD study, Bellevre et al. (16) recently demonstrated that determination of the late HMR of 123I-MIBG uptake using a parallel-collimator CZT camera (DSPECT; Biosensors International) was feasible in patients with heart failure. The 2 commercially available CZT cameras differ in sensitivity (4-fold improved with DNM-530c and nearly 7-fold improved with DSPECT) and spatial resolution (6.7 mm with DNM-530c and 8.6 mm with DSPECT), leading to images with different degrees of sharpness and contrast-to-noise ratios (11,17,18).
Until now, there have been no reports on the use of the DNM-530c, a multipinhole CZT SPECT camera, for determination of the HMR of 123I-MIBG uptake. As previously emphasized (19,20), quantification of the HMR is influenced by the type of collimators used and the number of scattered photons. Consequently, the value of the HMR is expected to depend on the type of CZT camera used. Hence, a study to validate the multipinhole dedicated cardiac CZT camera is needed.
The aim of this study was to compare the late HMR of 123I-MIBG uptake determined using dual-isotope CZT acquisition (DNM-530c) with that determined using conventional planar imaging in patients with heart failure.
MATERIALS AND METHODS
Phantom Studies
To estimate the effectiveness of the DNM-530c camera in measuring the HMR, we performed several phantom acquisitions using an anthropomorphic torso phantom (Data Spectrum) with a cardiac insert. The liver and mediastinum compartments were filled with 123I activities of 20 MBq (17.5 kBq/mL) and 5 MBq (0.6 kBq/mL), respectively. Ten consecutive acquisitions were performed over 10 min using a conventional Anger camera (Infinia; GE Healthcare) and a CZT camera (DNM-530c). The cardiac insert was repeatedly unloaded from 1.75 (11 kBq/mL) to 1.5, 1.25, 1.1, 0.94, 0.75, 0.5, 0.35, 0.25, and 0.1 MBq to obtain a wide range of HMRs of 123I, as previously described (16,20).
Patient Population
All procedures in studies involving human participants were performed in accordance with the ethical standards of the institutional or national research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This retrospective study was approved by the Hospital Ethics Committee for Medical Research (CIER 03/01/2016). Informed written consent was obtained from all individual participants included in the study. Data from 40 consecutive patients who had clinically stable ischemic or nonischemic heart failure (left ventricular ejection fraction [LVEF], <45%) and were referred to our institution from May 2011 to May 2016 were retrospectively evaluated. Patients with a recent (<21 d) history of unstable angina or acute myocardial infarction were excluded from the study.
Conventional Anger Camera Protocol (Planar Imaging)
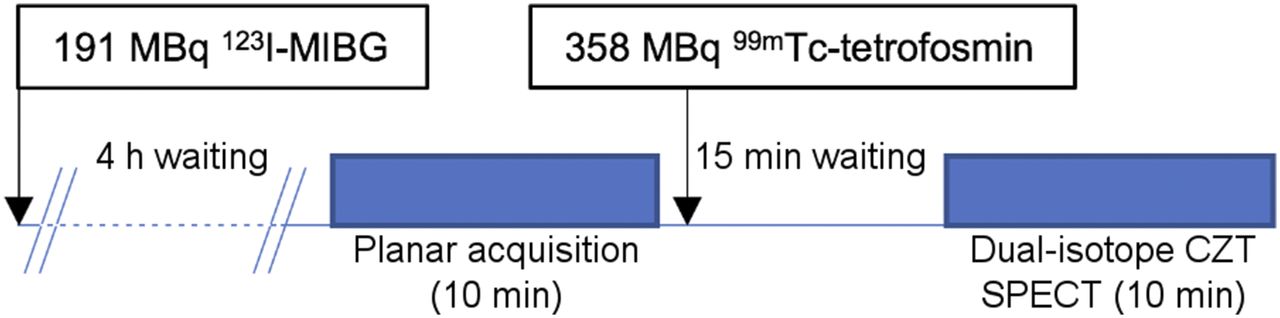
The imaging protocol (Fig. 1) was performed according to the recommendations of the EANM Cardiovascular Committee and the European Council of Nuclear Cardiology (7). 123I-MIBG (191 ± 29 [mean ± SD] MBq, depending on the patient’s weight) was administered 30 min after blockade of the thyroid by oral administration of Lugol solution. Four hours after injection, a late planar image was first obtained on a conventional γ-camera system, a dual-head γ-camera (Infinia) equipped with low-energy high-resolution collimators. Planar images were acquired in the anterior view over 10 min (128 × 128 matrix) using a symmetric energy window (159 ± 10 keV).

Imaging study protocol. First acquisition was single-isotope planar acquisition using conventional camera. Second acquisition was dual-isotope acquisition using CZT camera.
Dual-Isotope (123I-MIBG/99mTc-Tetrofosmin) CZT Acquisition Protocol (DNM-530c)
99mTc-tetrofosmin (358 ± 177 MBq) was administered for myocardial perfusion imaging to localize the heart within the thorax. After 15 min, the 99mTc image helped focus the detectors on the cardiac area. A 10-min list-mode simultaneous dual-radionuclide (99mTc and 123I) gated scan was then performed using a dedicated cardiac CZT SPECT camera (DNM-530c). DNM-530c is equipped with 19 stationary CZT detectors, each equipped with a pinhole collimator, that simultaneously image 19 cardiac views; each detector is composed of four 5-mm-thick elements of 32 × 32 pixels (pixel size, 2.46 × 2.46 mm) (17). List-mode acquisition permits the retrospective selection of 99mTc and 123I energy windows set to 140 keV (−10 to +5%) and 159 keV (−5 to +10%), respectively. No scatter correction was performed.
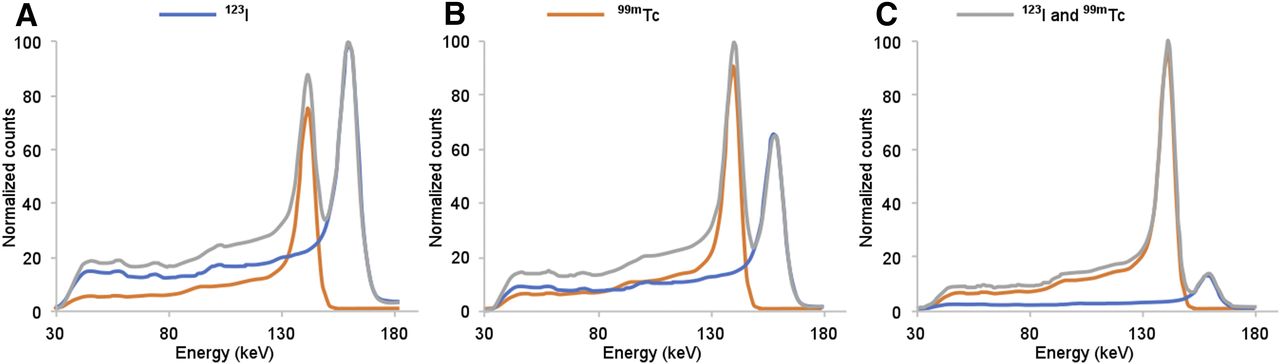
Previous studies using phantom data acquired separately for 99mTc and 123I showed that 99mTc cross-talk into the 123I window was negligible when a simultaneous CZT SPECT acquisition was performed (21,22). To ensure that different 99mTc/123I ratios did not have an impact on energy resolution, we acquired a set of energy spectra (single 123I, single 99mTc, and dual 123I/99mTc) using linear sources with three 99mTc/123I ratios (0.5:1, 1:1, and 5:1) and a constant activity of 123I (24 MBq) (Fig. 2).
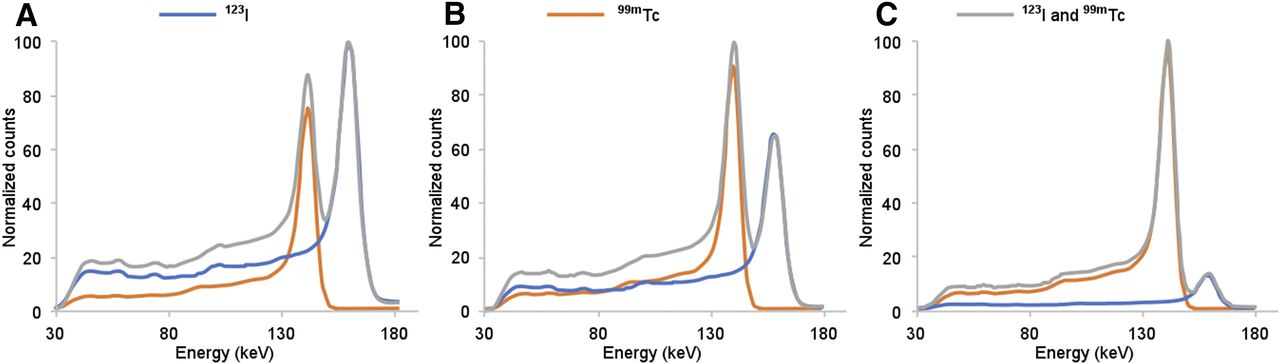
Single 123I (24 MBq), single 99mTc, and simultaneous (123I and 99mTc) energy spectra using linear sources and DNM-530c. Low tailing effect and downscatter of 123I toward 99mTc (and absence of 99mTc scatter toward 123I) were seen in dual-isotope condition, whatever the ratio of 99mTc activity to 123I activity: 0.5:1 (A), 1:1 (B), or 5:1 (C).
Analysis of HMR of 123I-MIBG Uptake
The HMR was calculated from the planar images (HMRplanar). Myocardial and mediastinal counts were obtained by drawing regions of interest (ROIs) manually on the left ventricle and over the upper mediastinum area (7).
Using SPECT data, we tested 2 different methods for assessing the HMR of 123I-MIBG uptake. First, the HMR was calculated with a reprojected anterior view of SPECT images reconstructed using the vendor’s console (HMRreproj). The reprojection of tomographic data assumed an ideal parallel-hole collimation and did not simulate attenuation or scatter. An ROI encompassing the left ventricle was drawn manually on the 99mTc-tetrofosmin images and automatically copied to the 123I-MIBG images. A mediastinum ROI (42 pixels) was then drawn on the 123I-MIBG images.
Second, the HMR was calculated with transaxial reconstructed SPECT images (HMRtransaxial). A myocardial elliptic volume of interest (VOI) was drawn manually to encompass the whole heart on the 99mTc-tetrofosmin images. This VOI was automatically copied from the 99mTc-tetrofosmin images to the 123I-MIBG images. A mediastinum VOI (300 voxels) was manually drawn on the 123I-MIBG images.
HMR Correction Factor
Many factors affecting the HMR of 123I-MIBG uptake differed between the Infinia and DNM-530c cameras, including the type of collimator (parallel-hole low-energy high-resolution with Infinia vs. multipinhole with DNM-530c), energy window, energy resolution (which was better with DNM-530c [∼9% with Infinia vs. ∼5% with DNM-530c]), and detector material stopping power (84% for 9.5-mm NaI(Tl) vs. 78% for 5-mm CZT for 159-keV photons). To take into account the difference between DNM-530c and Infinia, we applied to the HMR quantification a correction factor based on phantom acquisitions. To extract a correction factor from the analysis, we used a linear regression equation obtained in the phantom study. We calculated a corrected HMRreproj (cHMRreproj) and a corrected HMRtransaxial (cHMRtransaxial) for each patient in the validation group for further comparison with the HMRplanar values (16,23).
LVEF 99mTc-Tetrofosmin SPECT with DNM-530c
As previously reported (22), the presence of 123I did not have an impact on LVEF assessment within the 99mTc energy window in the dual-isotope condition for DNM-530c. Accordingly, the LVEF was assessed using Quantitative Gated SPECT software (Cedars-Sinai Medical Center).
Statistical Analysis
The normal distribution of data was tested with the Shapiro–Wilk test. Paired HMRs determined using Infinia and DNM-530c were compared using the Student t test for paired samples. Correlations among HMRplanar, HMRreproj, and HMRtransaxial were assessed using linear regression and Pearson correlation analysis. Concordance among HMRplanar, HMRreproj, and HMRtransaxial values was tested using the Lin concordance correlation coefficient (CCC) (24) and Bland–Altman analysis (25). The Lin CCC is essentially equivalent to the κ-coefficient but is applicable to continuous data. It evaluates both accuracy and precision, indicating how far measurement pairs are away from the line of identity. The Lin CCC scale ranges from 0 (no agreement) to +1 (perfect agreement), where 0.21–0.40 indicates fair concordance, 0.41–0.60 indicates moderate concordance, 0.61–0.80 indicates substantial concordance, and 0.81–0.99 indicates almost perfect concordance. A 2-tailed P value of less than or equal to 0.05 was considered statistically significant. Statistical analysis was performed using R version 3.3.2 (R Foundation for Statistical Computing).
RESULTS
Phantom Study
The HMRs obtained from the phantom acquisitions are shown in Table 1. HMRreproj (2.82 ± 1.5) and HMRtransaxial (3.51 ± 1.94) were higher than HMRplanar (2.34 ± 0.8) (P was not significant and P = 0.01, respectively). However, Bland–Altman plots demonstrated that HMRreproj and HMRtransaxial were underestimated for low HMRs and overestimated for high HMRs. The corrections used for the calculation of cHMRreproj and cHMRtransaxial were determined by linear regression between CZT and planar HMRs in the phantom study: cHMRreproj = 0.4715 × HMRreproj + 1.0416 (r = 0.98) and cHMRtransaxial = 0.4106 × HMRtransaxial + 0.8987 (r = 0.99), respectively.
HMRs from Phantom Acquisitions
Population
Among the 40 consecutive patients (34 men and 6 women; mean age, 71 ± 9 y; mean LVEF, 35% ± 9%) with heart failure included in the study, 22 (55%) had ischemic heart failure and 18 (45%) had nonischemic heart failure. Patient characteristics are shown in Table 2. The New York Heart Association functional classifications were class I for 13 patients, class II for 22 patients, and class III for 5 patients. End-diastolic and end-systolic volumes and LVEF obtained using 99mTc-tetrofosmin SPECT were 171 ± 87 mL, 117 ± 67 mL, and 36% ± 17%, respectively.
Patient Characteristics
HMR Quantification in Patients: DNM-530c Versus Planar Imaging
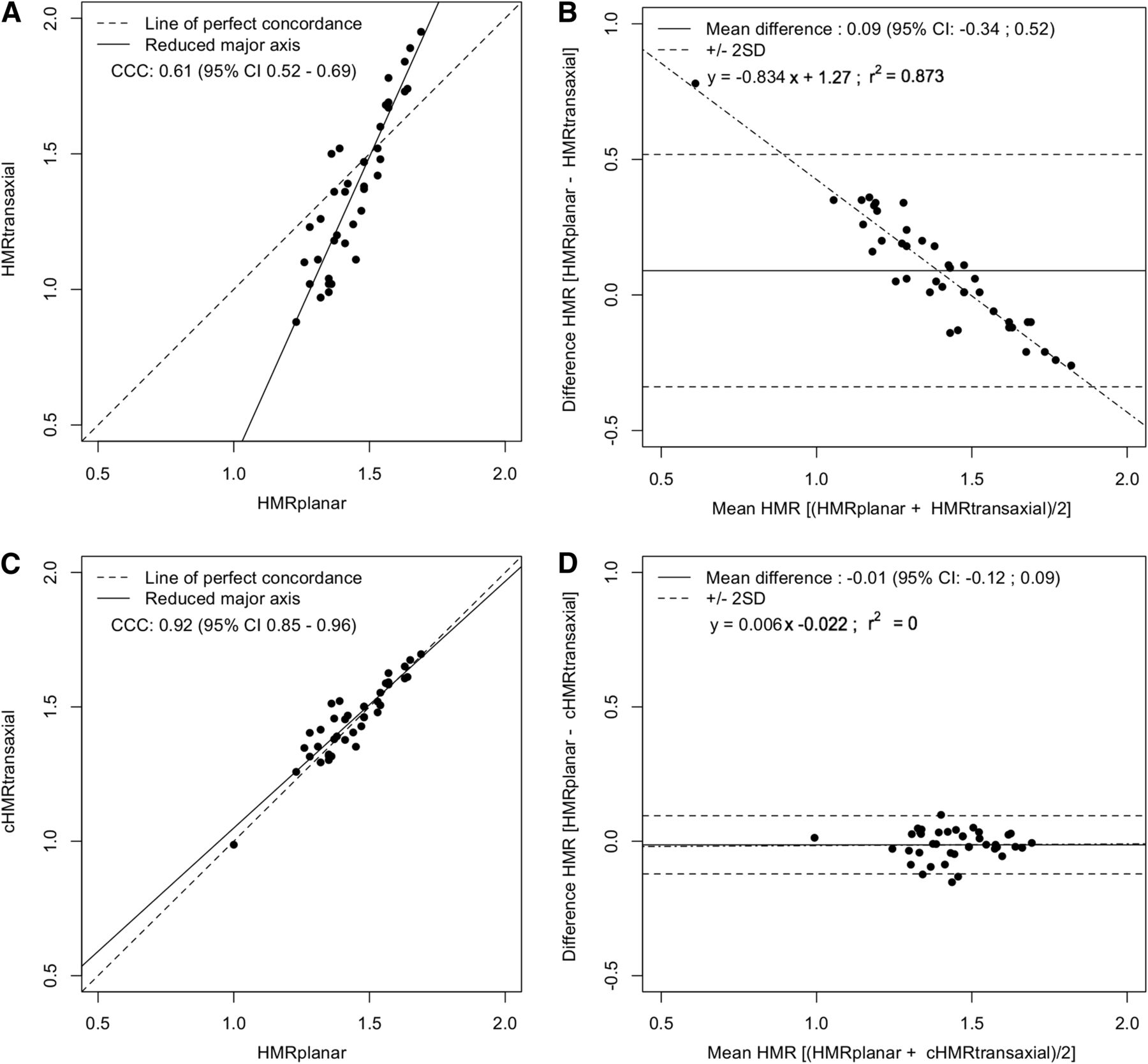
In our population, HMRreproj (1.12 ± 0.19) and HMRtransaxial (1.35 ± 0.34) were significantly lower than HMRplanar (1.44 ± 0.14) (P < 0.0001 and P < 0.05, respectively). Figures 3A and 4A show the Lin CCCs between HMRreproj and HMRplanar (Fig. 3A) and between HMRtransaxial and HMRplanar (Fig. 4A); these data demonstrated only a fair concordance between HMRreproj and HMRplanar (CCC, 0.24) but demonstrated a substantial concordance between HMRtransaxial and HMRplanar (CCC, 0.61). Bland–Altman plots (Figs. 3B and 4B) demonstrated a poor agreement between HMRreproj and HMRplanar (Fig. 3B) and between HMRtransaxial and HMRplanar (Fig. 4B), leading to an underestimation of values by DNM-530c. Figure 5 shows Infinia and DNM-530c images.
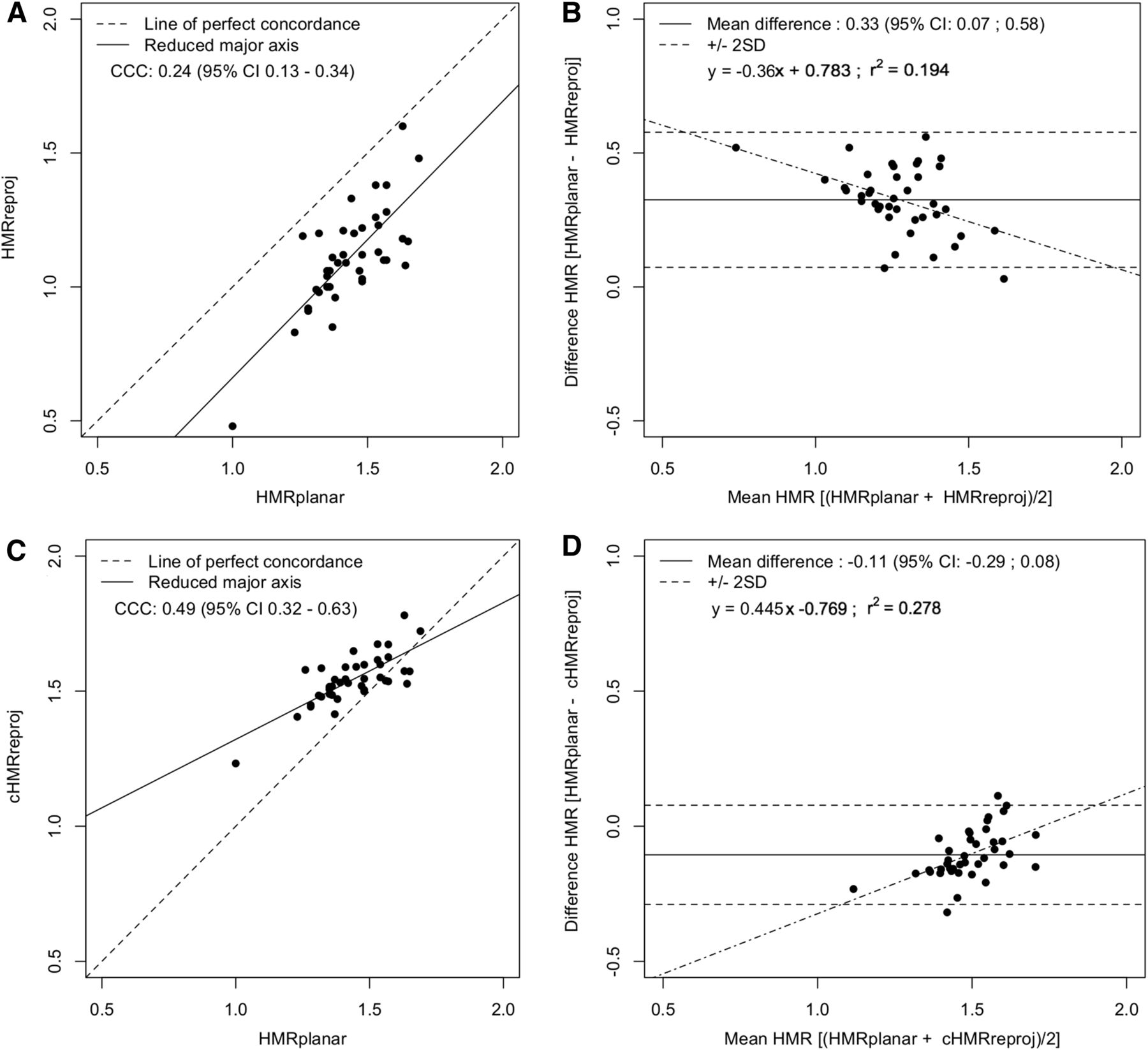
Lin CCC plots (A and C) and Bland–Altman plots (B and D) showing agreement between HMRreproj and HMRplanar (A and B) and between cHMRreproj and HMRplanar (C and D).
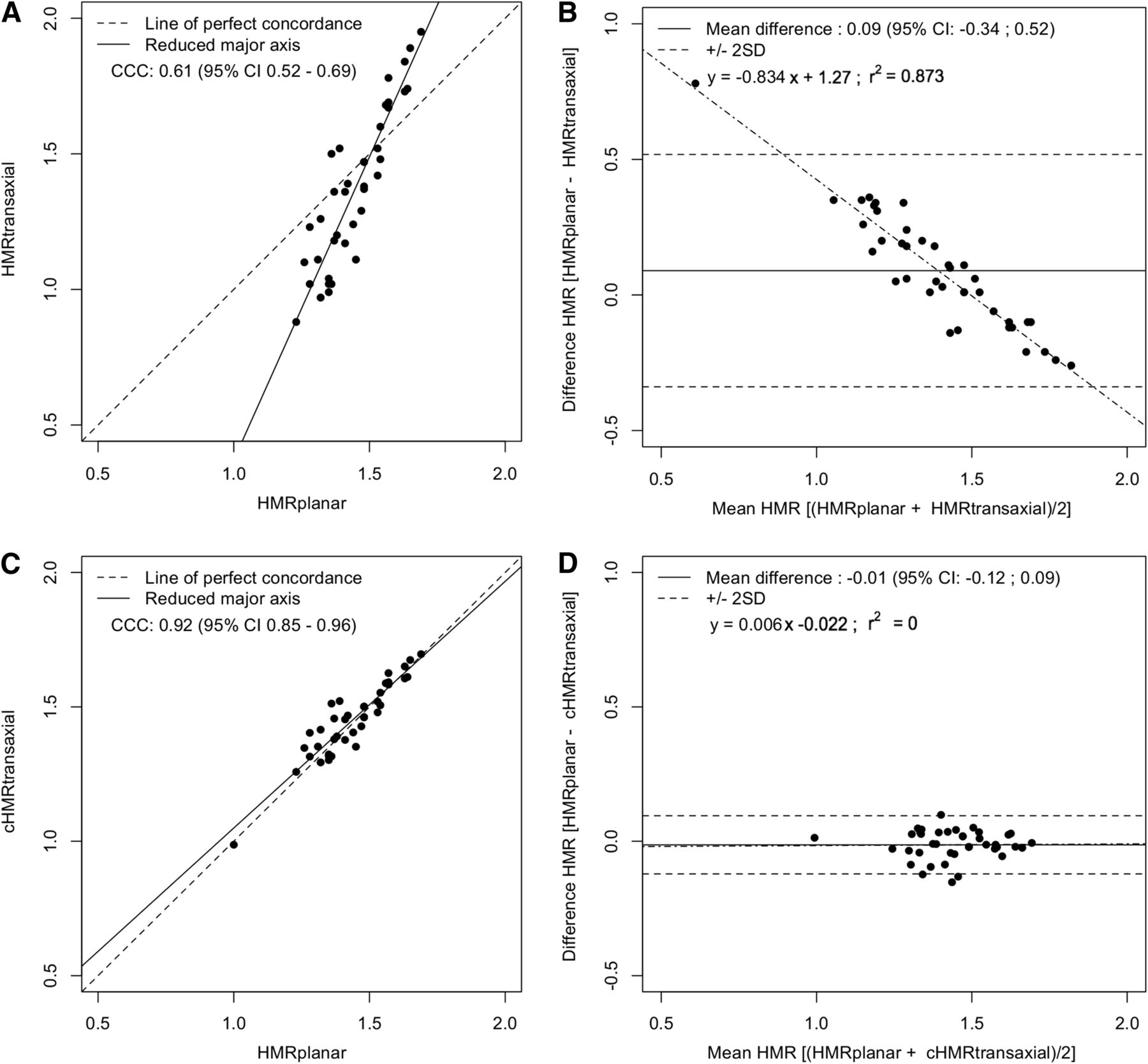
Lin CCC plots (A and C) and Bland–Altman plots (B and D) showing agreement between HMRtransaxial and HMRplanar (A and B) (P < 0.01) and between cHMRtransaxial and HMRplanar (C and D).
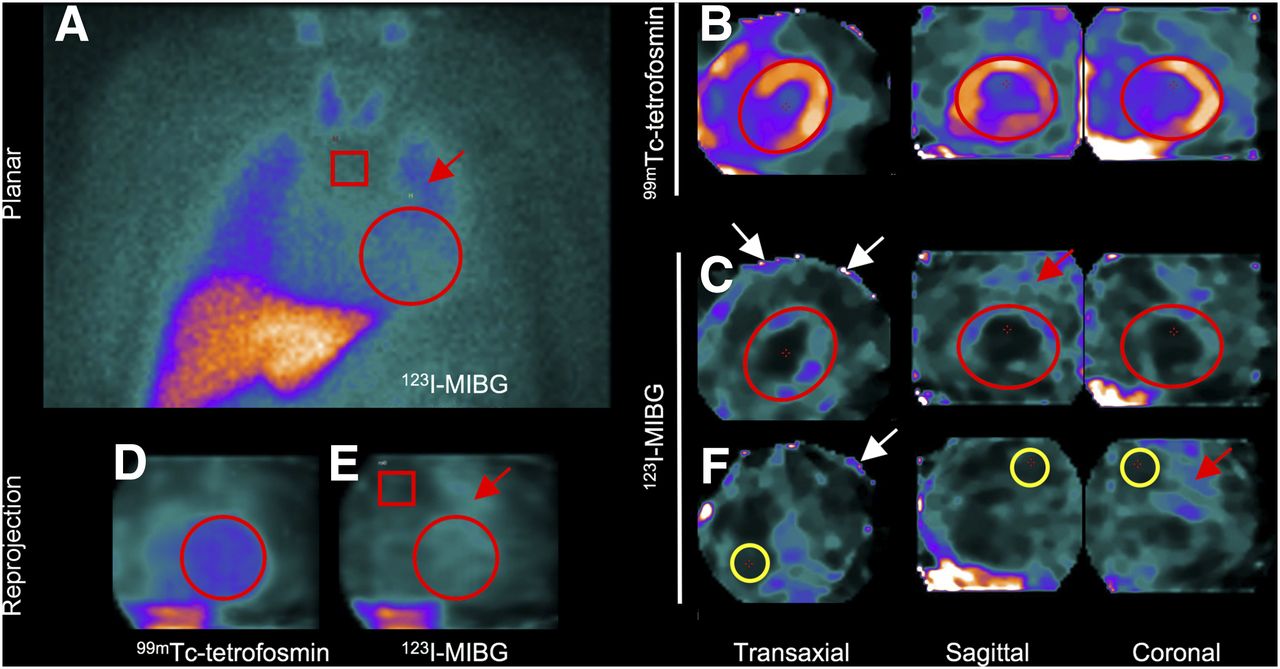
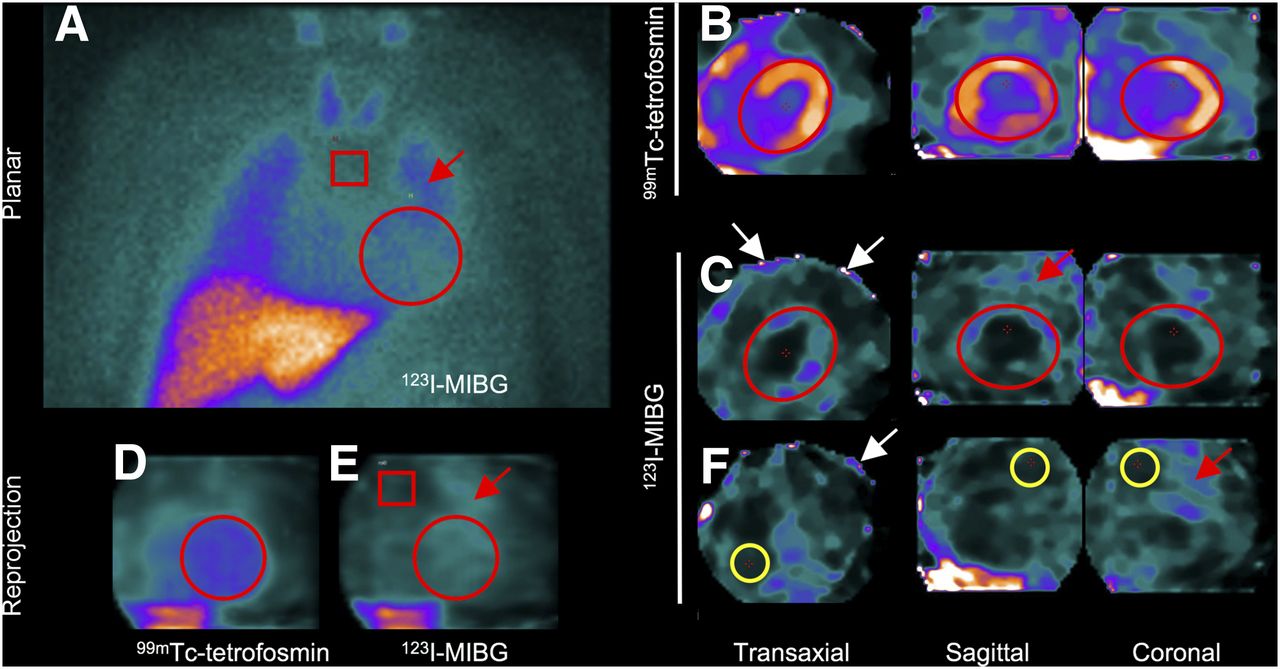
Patient 4 with ischemic heart failure (LVEF, 44%). HMRs calculated using conventional planar imaging (HMRplanar, 1.38) (A) and using DNM-530c with anterior reprojection images (HMRreproj, 0.96) (E) and with transaxial reconstructed images (HMRtransaxial, 1.2) (C and F). 99mTc image allowed positioning on heart of ROI (D) or VOI (B) and was pasted onto 123I image (E or C, respectively). (F) Mediastinum VOI on 123I acquisition. HMRreproj and HMRtransaxial were lower than HMRplanar. Lung activity (red arrows) and truncation artifacts (white arrows) were close to heart.
HMR Quantification in Patients: Corrected DNM-530c Versus Planar Imaging
cHMRreproj (1.54 ± 0.09) but not cHMRtransaxial (1.45 ± 0.14) was significantly higher than HMRplanar (1.44 ± 0.14) (P < 0.0001 and P was not significant, respectively). As shown in Figure 3C, there was a moderate concordance between cHMRreproj and HMRplanar (CCC, 0.49). Bland–Altman plots (Fig. 3D) showed a moderate agreement between cHMRreproj and HMRplanar. The mean difference between the HMRs from the 2 techniques was 0.11, but the difference increased significantly as a function of the mean HMR value.
In contrast, as shown in Figure 4C, there was an almost perfect concordance between cHMRtransaxial and HMRplanar (CCC, 0.92). Bland–Altman plots (Fig. 4D) showed a high agreement between cHMRtransaxial and HMRplanar. The mean difference between the HMRs from the 2 techniques was 0.01, with a narrow 95% confidence interval, and was stable over the whole range of HMRs.
DISCUSSION
Late HMR determination using the Anger camera is well standardized, and its prognostic value is widely recognized. In this retrospective study, we determined the HMR of 123I-MIBG uptake using a multipinhole dedicated cardiac CZT camera (DNM-530c) in patients with heart failure and low LVEF. To our knowledge, this is the first dual-isotope study combining 123I-MIBG and 99mTc-tetrofosmin with a multipinhole CZT camera to assess cardiac neuronal function in heart failure. Late HMRs (HMRreproj and HMRtransaxial) in patients were significantly lower than HMRplanar, but the latter showed high agreement with cHMRtransaxial. Our results are consistent with findings from the ADRECARD study (16), which was conducted using another model of the dedicated cardiac CZT camera, with different spatial resolution and sensitivity (17,26).
Difference Between Planar and CZT SPECT HMRs
First, to better understand the camera responses in 123I-MIBG imaging, we compared planar and DNM-530c phantom acquisitions and found that the noncorrected HMRs obtained with DNM-530c underestimated low values and overestimated high values of 123I-MIBG uptake. Accordingly, HMRs in patients were significantly lower with DNM-530c than with the Anger camera, as these patients with heart failure had decreased 123I-MIBG uptake.
The collimators used and the stopping power of the detector material may have an impact on the quantification of the 123I-MIBG HMR (20,27). Inoue et al. (23) found that a correction factor is necessary to improve exchangeability between HMRs calculated using medium-energy collimators and those calculated using low- to medium-energy collimators. Nakajima et al. (28–30) demonstrated that the linear regression equation for low-energy and medium-energy collimators in a phantom study can be used for standardizing the measurement of HMR in 123I-MIBG imaging. In the present study, after correction, there was still a significant difference between cHMRreproj and HMRplanar (P < 0.0001), but there was no difference between cHMRtransaxial and HMRplanar (P was not significant).
Using a different model of camera with mobile CZT detector columns and parallel tungsten collimators (DSPECT), Bellevre et al. (16) extracted a planar equivalent image by projecting and summing all of the elementary 2-dimensional images that shared the same angle on 1 large-field-of-view virtual plane (16). After applying a similar correction based on linear regression between SPECT and planar phantom acquisitions, they found a high agreement between the 123I-MIBG HMR obtained using the CZT camera and that obtained using planar imaging. In contrast, the moderate concordance between cHMRreproj and HMRplanar that we found using anterior reprojection images likely was related to the multipinhole collimation, which is responsible for a truncation artifact (31) that interferes with the mean counts of the myocardial ROI (Fig. 5) and for a larger nonuniformity with DNM-530c than with the Anger camera (31). This limitation was overcome through the use of reconstructed transaxial images instead of reprojection images for the measurement of corrected 123I-MIBG HMR with DNM-530c in our population.
Dual-Isotope Acquisition
In the present study, we performed simultaneous dual-isotope DNM-530c acquisitions with 99mTc-tetrofosmin (358 ± 177 MBq) and 123I-MIBG (191 ± 29 MBq). This dual-isotope acquisition allowed the simultaneous assessment of cardiac innervation and function. A previous phantom study demonstrated that under a simultaneous dual-isotope condition, the presence of 123I did not have an impact on LVEF assessment within the 99mTc energy window for both dedicated CZT cameras (22). In addition, a simultaneous dual-isotope protocol provides a clearer 99mTc-tetrofosmin image and a perfect registration for defining the heart contours on the 99mTc-tetrofosmin image and therefore accurately measures cardiac 123I-MIBG uptake (16). As shown in Figure 2, the amount of 99mTc activity had an impact on the 99mTc/123I ratio but did not interfere with the energy resolution of the detector, modifying only the magnitude and not the width of the photopeak.
Finally, the acquisition of both SPECT and planar images using the Anger camera usually requires 30–45 min. In contrast, acquisition with CZT cameras usually requires 10 min; the latter is much more convenient in patients with heart failure.
Study Limitations
Because of the narrow field of view, the cardiac acquisition did not encompass the upper mediastinum. Consequently, the mediastinal ROI or VOI was positioned in the middle mediastinum on DNM-530c images, whereas the mediastinal ROI was set on the upper mediastinum when a conventional Anger camera was used (7). On the other hand, the size and placement (manual or automated) of the left ventricular ROI did not affect the delayed HMR of 123I-MIBG when conventional planar imaging was used (8). Therefore, further studies including a phantom-based cross-calibration are needed to standardize the placement of the mediastinal ROI or VOI using the different models of available cardiac CZT cameras (30). Finally, dual-isotope acquisition increases the radiation burden. In this retrospective study, the injected 99mTc-tetrofosmin activity was gradually decreased over time as it became clear that the CZT camera allowed the injection of small amounts of perfusion tracer without a compromise in image quality.
CONCLUSION
The present study demonstrated that determination of the late HMR of cardiac 123I-MIBG uptake using dual-isotope (123I and 99mTc) acquisition on a multipinhole CZT camera (DNM-530c) is feasible in patients with heart failure. However, this determination should be performed using transaxial reconstructed images and a linear correction based on phantom data acquisitions.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Amélie Lansiaux, Sylvie Petit, Mathilde Thélu, and the nuclear medicine technicians at Lille, France, for their technical assistance.
Footnotes
Published online Jun. 23, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 6, 2017.
- Accepted for publication June 13, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}