


Abstract
The purpose of this prospective study was to assess the role of SPECT/multislice low-dose (Msl) CT as a constituent in the imaging algorithm of nononcologic patients referred for 99mTc-methylene diphosphonate bone scintigraphy (BS). Methods: SPECT/CT was performed using a novel hybrid system, which incorporates a γ-camera and a multislice low-dose CT, on 76 consecutive nononcologic patients with nonspecific scintigraphic findings, which required further correlation with morphologic data. Results: SPECT/MslCT was of added clinical value in 89% of the patients. Characterizing scintigraphic lesions by their morphologic appearance, SPECT/MslCT reached a final diagnosis in 49 of 85 (58%) nonspecific scintigraphic bone lesions found in 59% (45/76) of patients, obviating the need to perform additional imaging. In another 30% of patients (23/76), SPECT/MslCT data optimized the patients' imaging algorithm as the performance of a full-dose CT, MRI, or labeled-leukocyte scintigraphy as the next imaging was based on its findings combined with the patient's clinical presentation. Conclusion: SPECT/MslCT is a clinically relevant constituent in the imaging algorithm of nononcologic patients referred for BS.
Most published data on the role of hybrid imaging of PET or SPECT and CT has been dedicated to oncologic indications, probably because CT is a common constituent in the imaging algorithm of cancer patients (1–9). Previous reports have addressed the benefit of the fusion of SPECT with CT using various tumor-seeking radiopharmaceuticals—including 111In- somatostatin analogs, 131I, 123I-α-methyl tyrosine, and 99mTc-tetrofosmin—in patients with neuroendocrine tumors, thyroid, head and neck, and brain malignancies (4,10–15). Recent studies investigated the added value of SPECT/CT compared with SPECT alone in differentiating benign and malignant bone lesions on 99mTc-methylene diphosphonate (99mTc-MDP) bone scintigraphy (BS) (16–18).
Various SPECT/CT hybrid systems are now available, encouraging a step forward in the investigation of clinical fields, which may benefit from integrated radiology and nuclear medicine assessment (1). In the case of 99mTc-MDP BS, the limited specificity of BS is a burden not only when the dilemma is differentiation between malignant and benign lesions but also when nonmalignant conditions dictate a need to perform further correlation with conventional imaging to reach final a diagnosis. In the current study, SPECT/multislice low-dose (Msl) CT was performed on nononcologic patients referred for BS, in whom correlation with morphologic data was needed for accurate diagnosis after performing planar and SPECT BS. The hybrid system used was a novel SPECT/CT system composed of an inline dual-head γ-camera and a multislice low-dose CT (Hawkeye 4; GE Healthcare).
MATERIALS AND METHODS
This was a prospective study performed over a 6-mo period, starting in January 2006. SPECT/MslCT BS was performed on 76 patients (41 males, 35 females; mean age ± SD, 47.4 ± 20.7 y; age range, 7–89 y; 40 patients were >50 y old). Indications for BS were pain (n = 61), trauma (n = 7), suspected infection or inflammation (n = 6), and fever of unknown origin (n = 2). This study cohort represents consecutive nononcologic patients with nonspecific scintigraphic findings, which required further correlation with morphologic data. Nonspecific findings were focal sites of increased 99mTc-MDP uptake detected on planar and SPECT data anywhere in the central or peripheral skeleton, with unclear diagnosis. Lesions located in the lower vertebral column—the diagnosis of which was unclear on planar images but was clarified on SPECT—such as osteophytes and facet joint disease, were considered nonspecific scintigraphic lesions that required further assessment by CT. Institutional review board approval was obtained, and patients (or guardians in the case of minors <18 y old) signed a written consent to add MslCT acquisition to the BS study protocol.
SPECT/MslCT Technique
SPECT/MslCT was performed using a novel SPECT/CT hybrid system, the Infinia/Hawkeye 4 (GE Healthcare). This system incorporates the Infinia dual-head camera with an integrated low-dose, four 5-mm slice-thickness CT. SPECT was performed in H mode, with a matrix size of 128, an angle step of 6°, and a time per frame of 16 s. To improve resolution and signal-to-noise characteristics, SPECT data were reconstructed using a novel collimator–detector response method (Evolution software package; GE Healthcare), which incorporates a quantitative model of collimator–detector response function of the acquisition system into an iterative reconstruction algorithm (19).
The CT part of the system (MslCT) has a fixed anode, oil-cooled x-ray tube that operates at 140 kV and up to 2.5 mA. The x-ray tube and detector array, located on the slip-ring gantry of the γ-camera, rotate together in a fixed geometry at 2.6 rpm for opposing detector (H mode) scans (2.0 rpm for 90° L-mode scans). Multiple slices can be obtained in axial or helical modes, 4 slices acquired simultaneously with beam coverage of 2 cm in each gantry rotation and reconstructed online to a 512 × 512 image matrix. CT is acquired within 4.5–5 min. Hawkeye 4 acquisition is associated with an additional radiation exposure of 2 mSv. Fusion of SPECT and CT data was performed on the Xeleris workstation (GE Healthcare).
Image Interpretation and Data Analysis
SPECT/MslCT images were interpreted in a consensus reading by 2 nuclear medicine physicians and a musculoskeletal radiologist. The reviewing physicians commented on whether SPECT/MslCT reached a final diagnosis and whether additional imaging was warranted. In the latter case, the imaging approach most appropriate for further work-up was suggested, either diagnostic full-dose CT, MRI, or labeled-leukocyte scintigraphy.
RESULTS
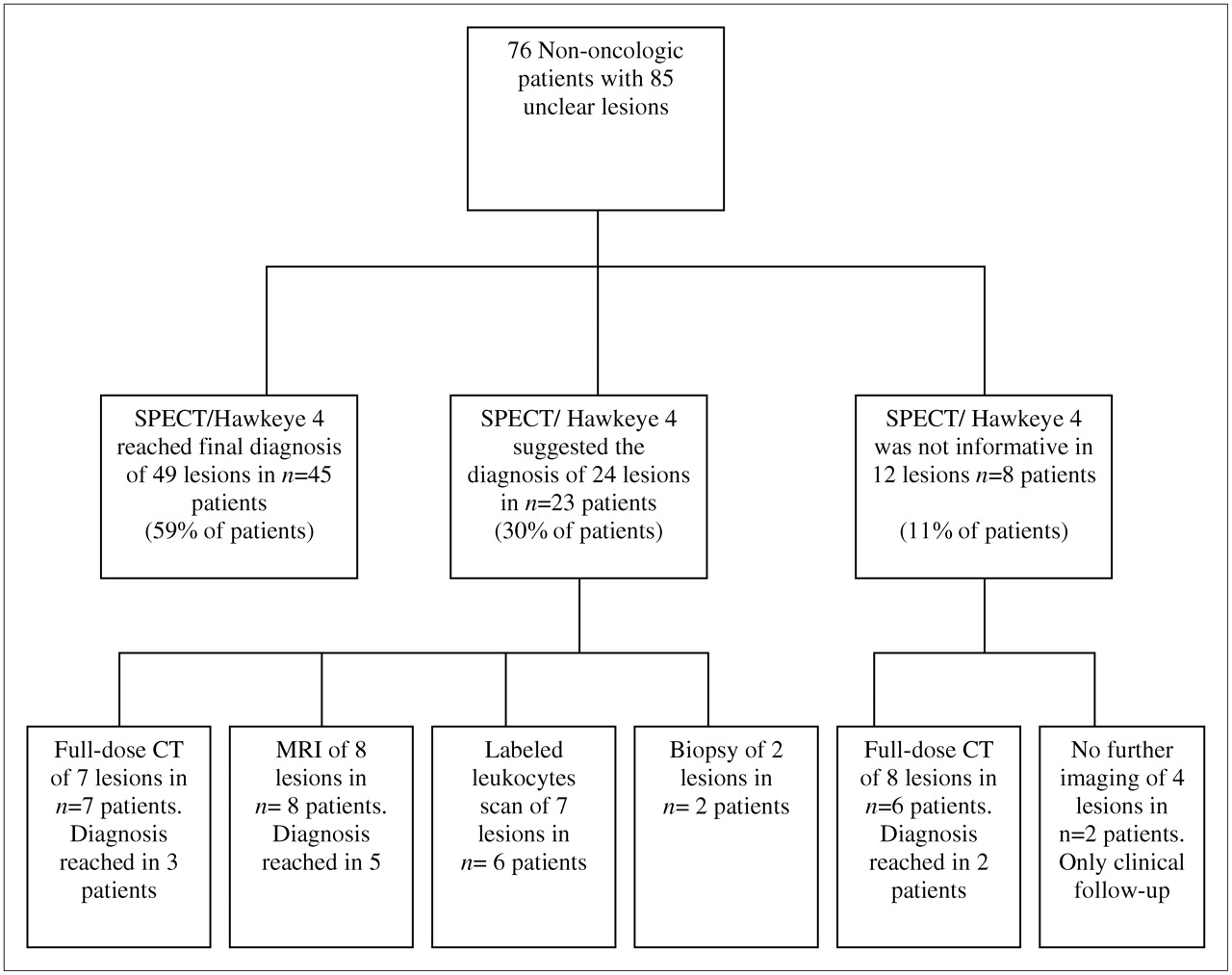
Figure 1 illustrates the imaging algorithm of the study cohort. SPECT/MslCT was performed in an attempt to determine the diagnosis of 85 nonspecific sites of uptake detected by SPECT, including 68 lesions relevant to the patient's clinical presentation and 17 incidental lesions. In 45 of the latter patients (59% of 76 patients and 58% of 85 nonspecific lesions), the final diagnosis was reached by the morphologic data of MslCT and no further imaging was required. The lesions diagnosed by MslCT data were fractures, osteochondral lesions, nonossifying fibroma, enchondroma, fibrous dysplasia, herniation pit, spurs, posterior osteophytes, osteoid osteoma, bursitis, osteoarthrosis, exostosis, spondylolysis, hemilumbarization, and vertebral collapse (Figs. 2–4⇓).

Imaging algorithm of 76 nononcologic patients who underwent 99mTc-MDP SPECT/MslCT.

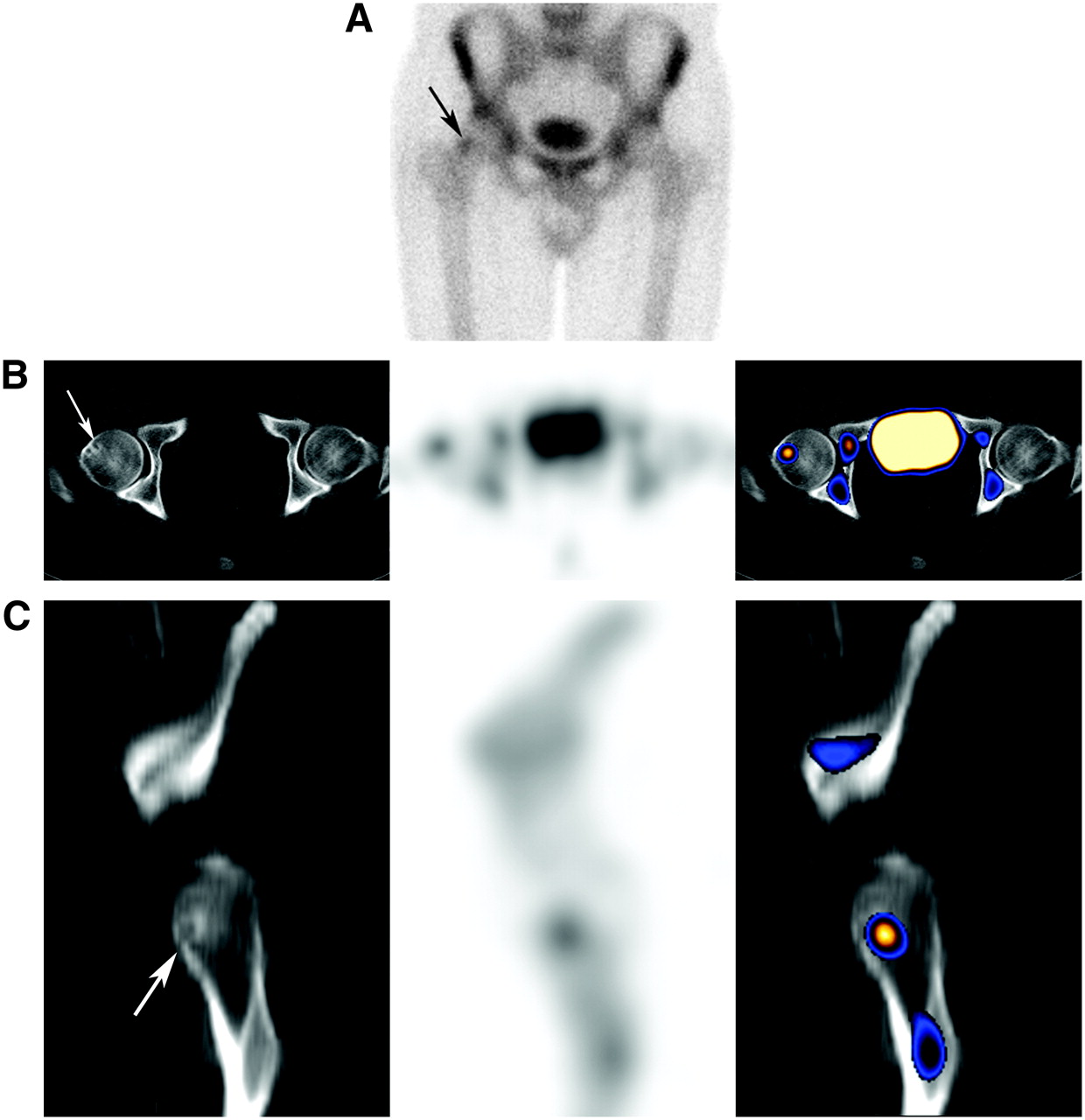
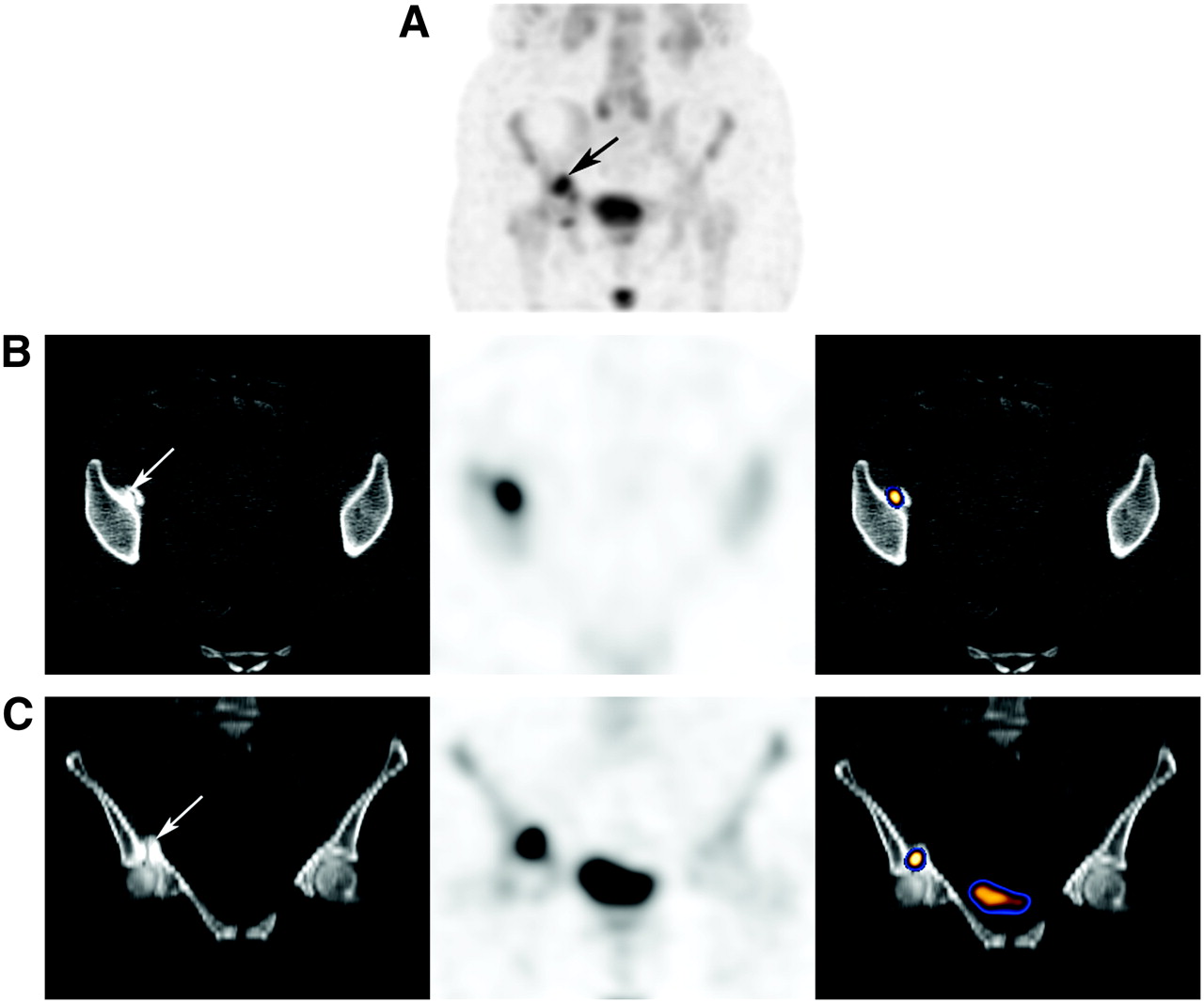
Diagnosis of nonspecific scintigraphic abnormality in 39-y-old patient referred for BS due to painful right hip joint. (A) On planar images, focal increased uptake was detected in right femoral head (arrow). Transaxial (B) and sagittal (C) SPECT/CT slices; from left to right: MslCT, SPECT, and fused images. CT finding, which corresponds in location with scintigraphic abnormality, is that of a lobulated radiolucency with a thin sclerotic border in superolateral aspect of femoral head characteristic of a herniation pit (arrows).

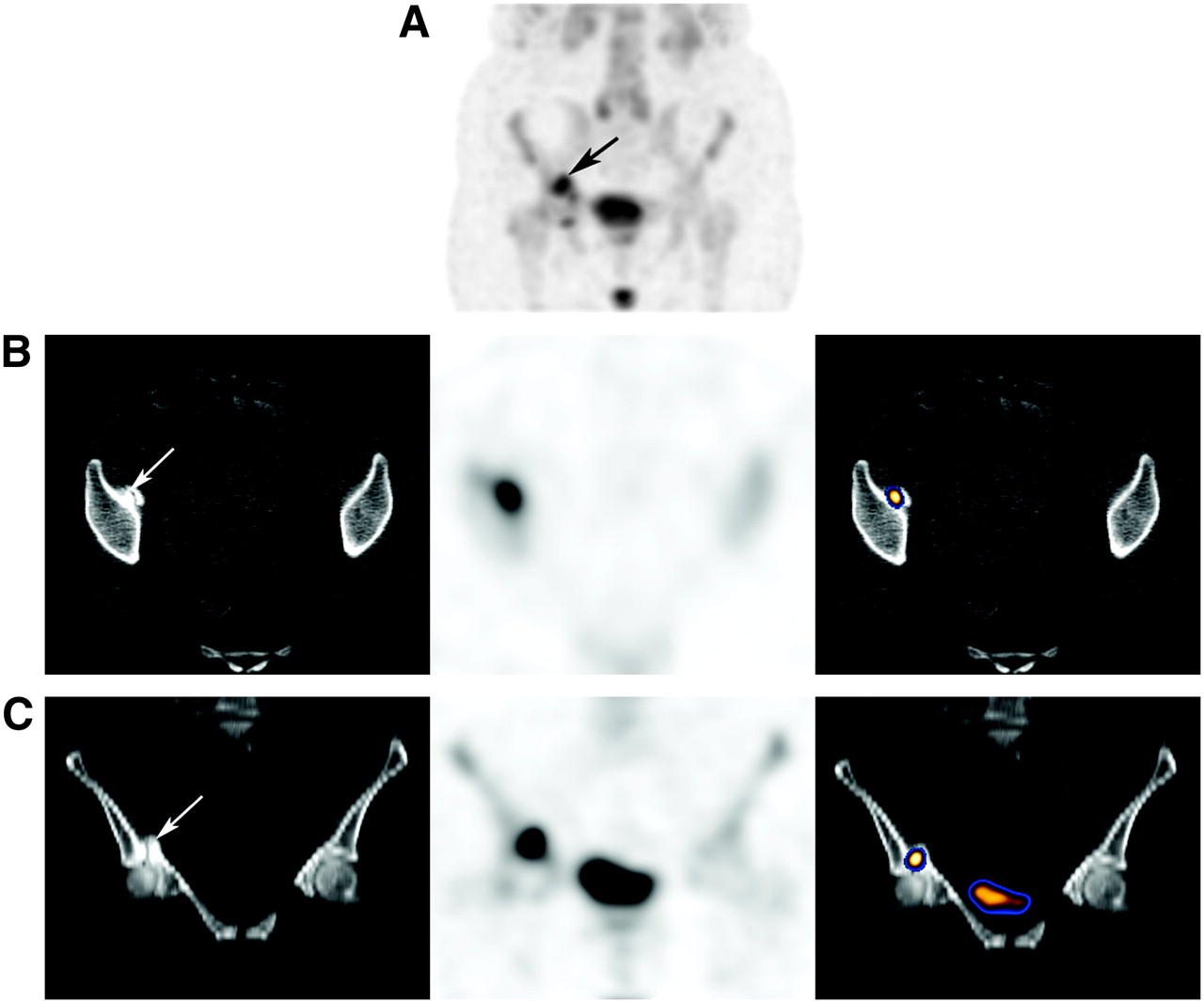
Diagnosis of incidental scintigraphic abnormality in 48-y-old patient referred for BS due to painful right hip joint. Transaxial SPECT/CT slices; from left to right: MslCT, SPECT, and fused images. Incidental focal increased uptake was detected in left iliac bone. CT finding, which corresponds in location with scintigraphic abnormality, is that of a calcified chondroid matrix representing a nonsymptomatic enchondroma (arrow). Cause of patient's right hip pain was idiopathic osteoporosis (not shown).
Diagnosis of nonspecific scintigraphic abnormality in 72-y-old patient referred for aggravated right hip pain. (A) SPECT maximum-intensity-projection image detecting increased uptake at right hip joint region (arrow). Transaxial (B) and coronal (C) SPECT/CT slices; from left to right: MslCT, SPECT, and fused images. CT finding that corresponds in location with scintigraphic abnormality is a fracture through an osteophyte of acetabulum (arrows).
Of the remaining 31 patients, the addition of MslCT was not found to be of any added clinical value in 8 (11%) patients, as no clear morphologic abnormality was detected to clarify the nature of the scintigraphic abnormality (5 patients) or when the quality of the CT data was not sufficient to suggest diagnosis (3 patients). For 24 lesions (28%) detected in the other 23 patients (30%), MslCT data were beneficial by accurately localizing the nonspecific lesions to the cortex or to the intramedullary bone component or by detecting morphologic abnormalities in the corresponding location with the unclear scintigraphic lesions resulting in a suggested diagnosis—although the musculoskeletal radiologist believed that further confirmation by additional imaging or that a more detailed morphology was necessary. In the latter group of 23 patients, combining SPECT/MslCT findings and the patient's clinical presentation achieved optimization of the individual patient's imaging algorithm by guiding the more appropriate next imaging approach. Additional full-dose CT was suggested for more detailed morphology in 3 patients who planned to undergo surgery (Fig. 5), in 2 patients in whom it was difficult to clearly assess the borders of lesions and the presence of accompanying abnormality in the adjacent soft tissue on MclCT data, and in 2 patients in whom diagnosis remained unclear, although MclCT data detected cortical changes. MRI was suggested when an intramedullary abnormality was suspected, and labeled-leukocyte scintigraphy was suggested in suspected infection. Imaging assessment, which followed SPECT/MslCT, reached a diagnosis in 16 of the 31 patients (52%). In addition to 45 patients in whom MslCT reached a diagnosis, full-dose CT data reached a diagnosis in 5 patients (7% of the study patients). MRI was beneficial as the next imaging modality after SPECT/MslCT in the case of migratory osteoporosis, early stages of infection, and malignant involvement of the marrow.
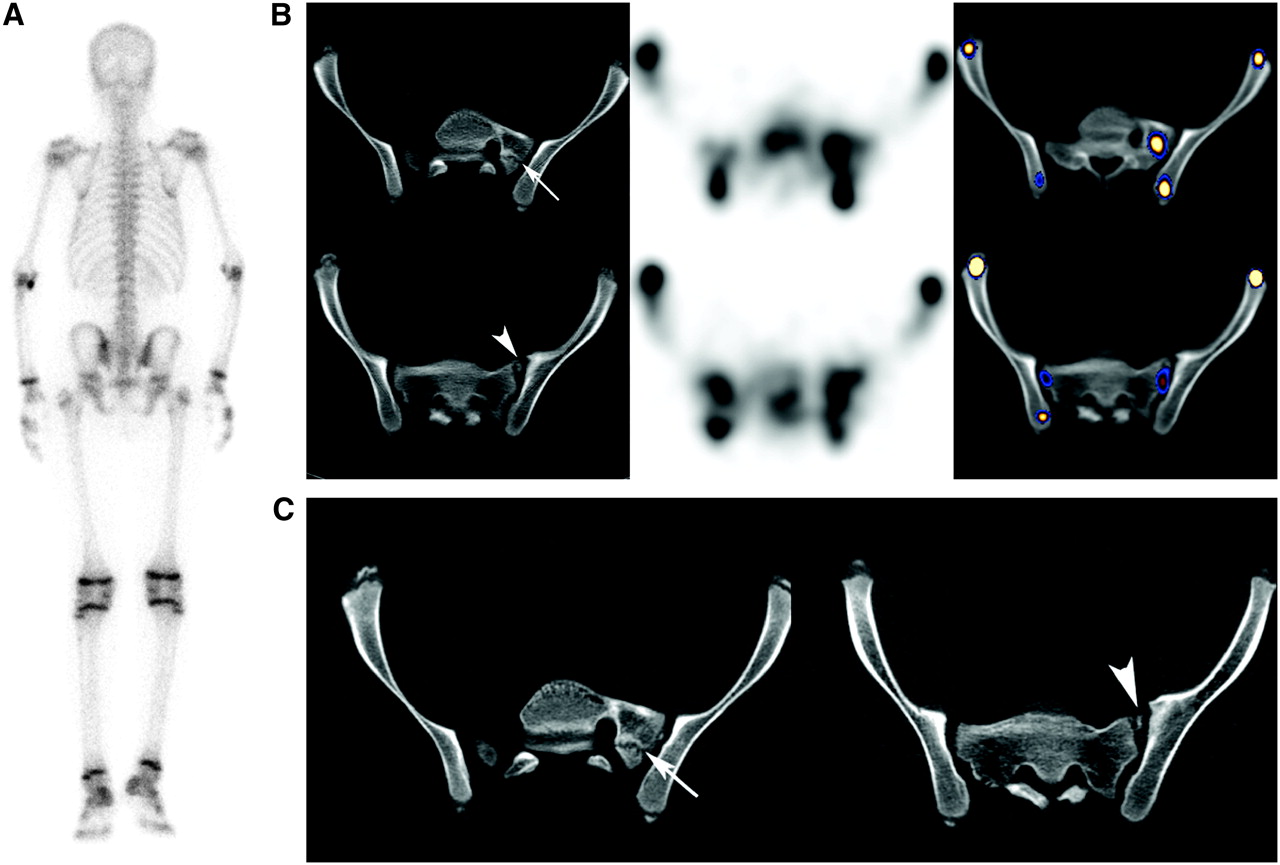
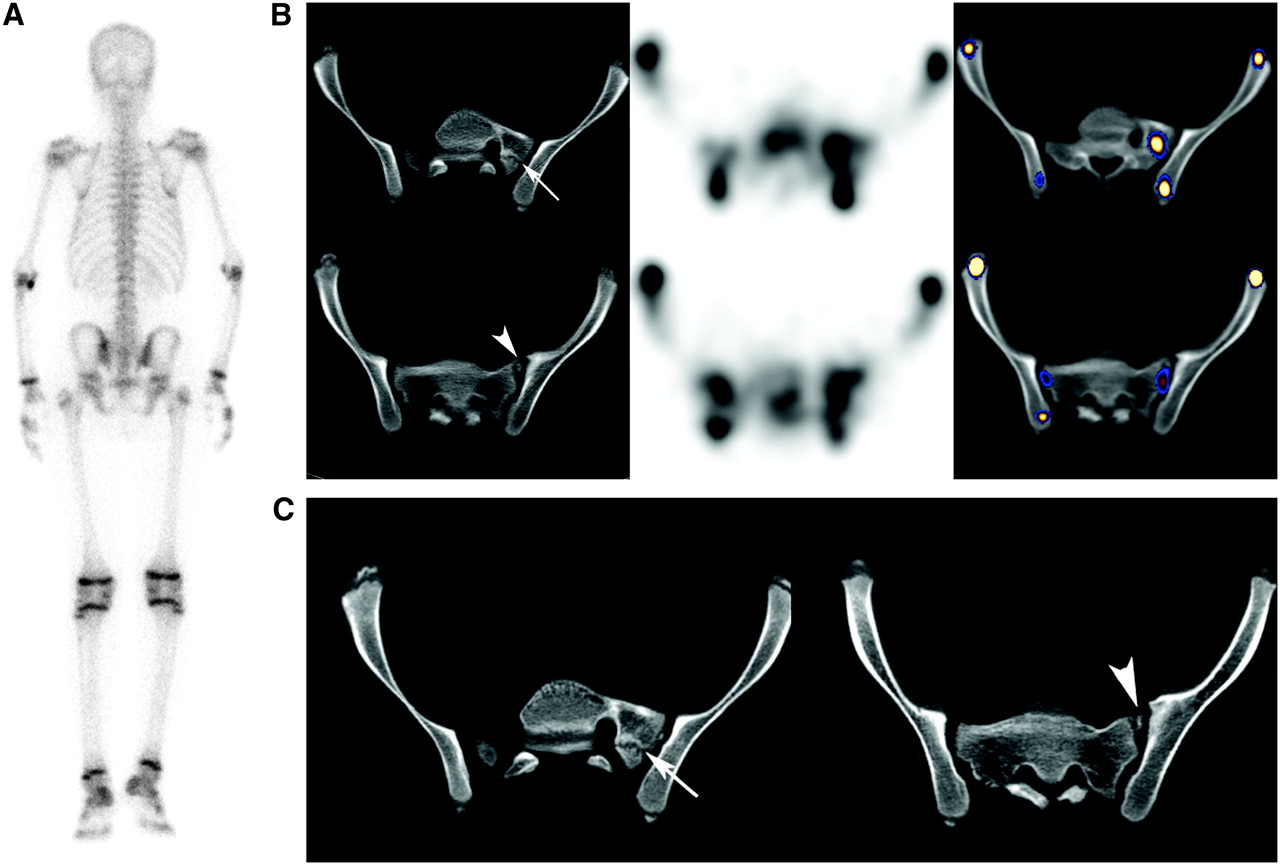
Comparison between MslCT and full-dose diagnostic CT data in 14-y-old patient referred with low-back pain. (A) Planar image identifies focal uptake in right sacroiliac region. (B) Transaxial SPECT/CT slices; from left to right: MslCT, SPECT, and fused images. Increased uptake appears to be located in hemisacralization of L5 on the left (upper row, arrow) with fragmentation (bottom row, arrowhead). (C) Radiologist suggested additional diagnostic full-dose CT for more detailed morphology before surgery. Although full-dose CT data were of a superior quality, MslCT and diagnostic CT revealed similar bone abnormalities. The site of hemisacralization is marked by an arrow and that of fragmentation is marked by an arrowhead.
DISCUSSION
The positive influence of fusion of functional and anatomic data on patient management has been widely investigated particularly in the field of oncology (1). Recent studies investigated the added value of SPECT/CT compared with SPECT alone in differentiating benign and malignant bone lesions on 99mTc-MDP BS (16–18). Horger et al. et al. used a hybrid camera combining SPECT with low-dose single-slice CT (the first Hawkeye generation), which correctly classified 85% of unclear scintigraphic bone lesions compared with only 36% using SPECT alone (16). Utsunomiya et al. performed SPECT/CT on 45 oncologic patients using a gantry-free SPECT scanner and an 8-detector-row CT scanner, which were juxtaposed such that the CT table could move with the patient directly from the CT scanner into the SPECT scanner. Afterward, both image datasets were retrospectively registered on a separate workstation. Their findings demonstrated an improved diagnostic confidence in differentiating malignant from benign bone lesions using the fused SPECT/CT images compared with SPECT alone or side-by-side reading of separate sets of scintigraphic and CT images (17). Romer et al. evaluated 52 indeterminate scintigraphic bone lesions in 44 cancer patients using a hybrid system composed of a γ-camera and a dual-slice reduced-dose (130 keV, 40 mA·s) spiral CT. Fused images clarified >90% of these lesions (18).
Before the era of 18F-FDG PET/CT, assessment of malignant bone involvement was one of the most common indications for BS. Nowadays, BS is no longer performed as a routine on many patients with 18F-FDG–avid tumors. Yet, 99mTc-MDP BS is still a common nuclear medicine procedure on oncologic and nononcologic patients. Patients are being referred to BS for nonmalignant indications due to orthopedic, rheumatologic, metabolic, infectious conditions and so forth. As BS is nonspecific, lesions with increased 99mTc-MDP uptake often require further morphologic data. Moreover, the high sensitivity of BS results in a high rate of incidental findings, which are not necessarily related to the patient's clinical presentation, introducing a “new” challenge in the interpretation of BS (Fig. 3). There is an ongoing effort to improve the specificity of BS. SPECT has been shown to improve the specificity of planar BS, particularly when detecting scintigraphic lesions in the lower vertebral column (20–22). It is less successful in doing so in other skeletal regions. The patients enrolled in the current study were consecutive nononcologic patients in whom skeletal scintigraphic lesions detected on planar images remained nonspecific also on SPECT.
In contrast to cancer patients who often have contemporaneous CT available for correlation, nononcologic patients referred for BS may not have CT, as was the case in the current study cohort. Several novel SPECT/CT hybrid systems are now available. The CT component may be a single-slice low-dose CT, multislice low-dose CT, reduced-dose diagnostic CT, or full-dose diagnostic CT. In the current study, we have used a novel hybrid system with 4-slice, low-dose CT. Although MslCT data are inherently inferior to those obtained by full-dose diagnostic CT, performance of integrated SPECT/MslCT was found to be of added clinical value in 89% of patients referred for BS due to nonmalignant indications. It provided sufficient morphologic data allowing an instant final diagnosis in 59% of patients with unclear scintigraphic bone lesions (Figs. 2–4⇑). In the latter patients, SPECT/MslCT was the final imaging modality performed, obviating the need to refer the patients for additional imaging. In another 17% of patients, the musculoskeletal radiologist suggested the performance of additional full-dose diagnostic CT after MslCT for diagnosis or for better morphologic details. Even then, adding a full-diagnostic CT was not always of clinical relevance (Fig. 5). In only 7% of the study patients did full-dose CT performed after MslCT provide clinically relevant data, which was not gained by MslCT.
It appears that in only 50 of the 76 study patients (66%) did CT—either MslCT or full-dose diagnostic CT—reach diagnosis. It should be borne in mind that the sensitivity of CT varies with different skeletal abnormalities. It is relatively less sensitive for detection of abnormalities initiating in the intramedullary bone component, migratory osteoporosis, early stages of infection, malignant bone involvement, and so forth. The ability to reach diagnosis for skeletal lesions using a nondiagnostic reduced mA·s CT has been previously reported (18,23). As a stand-alone imaging procedure of bone abnormalities, the use of a reduced-dose CT with an advantageous lower radiation exposure was encouraged on the basis of the inherent high contrast between normal and abnormal bone, which may be identified also on reduced-dose CT images (23).
Because CT is not always the optimal imaging modality of skeletal abnormalities, combining the patient's clinical presentation with SPECT/low-dose CT data may be beneficial in guiding the performance of MRI or labeled leukocytes and obviating the performance of a futile full-dose CT. In addition to the 59% of patients in whom SPECT/MslCT reached diagnosis, it assisted in optimization of the patients' imaging algorithm in another 30% of patients.
CONCLUSION
SPECT/MslCT is a clinically relevant constituent in the imaging algorithm of patients referred for BS because of nononcologic indications. In 59% of patients, final diagnosis of nonspecific SPECT lesions was reached instantly, obviating the need to perform additional imaging, and, in another 30% of patients, it guided the choice of the next imaging modality.
Acknowledgments
The authors thank Osnat Zak, MSc, and Eli Stern, BSc, GE Healthcare, Haifa, Israel, for their assistance in preparation of the manuscript.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 18, 2006.
- Accepted for publication November 14, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}