


Abstract
Cardiac resynchronization therapy (CRT) by biventricular pacing is indicated in patients with severe heart failure and left bundle branch block who remain symptomatic despite optimal medical therapy. The relationship between baseline resting perfusion pattern and hemodynamic response to CRT has not been fully investigated. We tested the usefulness of perfusion gated SPECT for baseline evaluation and follow-up of these patients. Methods: In 20 patients, we performed gated SPECT before CRT and at the 3-mo follow up. Left ventricular (LV) ejection fraction (EF), end-diastolic (ED) and end-systolic (ES) volume indexes (VI), and wall motion score index (WMSI) were measured and compared with clinical outcome. Results: One patient died before follow-up. The 19 remaining patients were classified into 1 of 2 groups according to the presence (group A) or absence (group B) of a significant severe perfusion defect at baseline before CRT. At the 3-mo follow-up, 6 of 10 group A and 8 of 9 group B patients had an improvement in New York Heart Association class. In both groups, quality of life, 6-min walking distance, and WMSI significantly improved. In group A, no significant change was registered in LVEF, LVEDVI, or LVESVI. In group B, LVEF increased from 23.1% ± 8% to 27.1% ± 11% (P < 0.03) and LVEDVI and LVESVI decreased from 159 ± 70 mL to 135 ± 68 mL (P < 0.02) and from 127 ± 67 mL to 104 ± 65 mL (P < 0.01), respectively. Conclusion: Perfusion gated SPECT appears useful to characterize and follow up candidates for CRT. Despite clinical improvement, patients with severe resting perfusion defects do not show significant improvement in LVEF or reduction in LV volumes.
In heart failure patients with intraventricular conduction disturbances, cardiac resynchronization therapy (CRT) by synchronous biventricular pacing has been proposed as a valuable therapeutic addition if symptoms persist despite optimal medical treatment (1–3). It would be desirable to identify those who will benefit from this expensive treatment. Besides a correct clinical indication, other indicators of a potentially favorable outcome include long QRS duration, clear left ventricular (LV) dilatation, and presence of mitral regurgitation (4–6). Conversely, ischemic heart disease and older age have been found to be significant predictors of absence of response (6) and a slight prevalence of patients with ischemic cardiomyopathy among those who do not benefit from CRT has been reported (5,7). Recently, Duncan et al. demonstrated that patients with idiopathic dilated cardiomyopathy show significantly more extensive LV reverse remodeling than do those with ischemic cardiomyopathy (8). Therefore, it could be of interest to verify whether the assessment of myocardial perfusion could play a role in the characterization of potential candidates for CRT. Furthermore, the use of myocardial perfusion imaging in these patients could be encouraged by the fact that the state-of-the-art technique for this modality is gated SPECT with 99mTc-labeled perfusion agents, which allows the simultaneous evaluation of LV perfusion and function. Gated SPECT has been demonstrated to be a reproducible method to assess LV volumes and ejection fraction (EF) and can also evaluate changes in regional wall motion with reasonable accuracy (9–12). Because it is important to objectively assess treatment results in patients undergoing CRT, gated SPECT could be helpful for characterizing baseline LV functional parameters and for following up their evolution. This study aimed to evaluate the role of myocardial perfusion imaging in the characterization of candidates for CRT and the feasibility of using gated SPECT functional and volumetric data for their baseline assessment and follow-up.
MATERIALS AND METHODS
We studied 20 consecutive patients with advanced heart failure (New York Heart Association [NYHA] class ≥ III, LVEF < 35%) and left bundle branch block with QRS duration > 120 ms, scheduled for CRT because of persisting symptoms despite optimal medical therapy. Table 1 summarizes patient characteristics on enrollment. Resting gated SPECT was performed before implantation and was repeated 3 mo later, together with clinical evaluation, including 6-min walking distance and quality of life (QOL) assessment with the Minnesota Living with Heart Failure questionnaire (13). The optimized medical treatment of each patient remained unchanged during the study. Our Ethics Committee approved the protocol, and patients gave informed consent to participate.
Patient Demographics at Baseline
Gated SPECT
Gated SPECT acquisition began 60 min after 99mTc-sestamibi injection (740 MBq) at rest, using a double-head camera equipped with high-resolution collimators, a 180° rotation arc, 32 projections, 8 frames per heart cycle, and 64 × 64 matrices. LV end-diastolic (ED) and end-systolic (ES) volumes were calculated using the Quantitative Gated SPECT program (Cedars-Sinai Medical Center) (9) and were expressed as indexes by dividing them by the body surface. LVEF was calculated from the LV volumes as usual. Regional function was scored by a consensus of 2 observers unaware of any other data, using a 4-point scheme (1 = normal function, 2 = hypokinesis, 3 = akinesis, and 4 = dyskinesis) on a 16-segment model, and the wall motion score index (WMSI) was calculated by dividing the total score by the number of segments (11). Perfusion defects were quantified as percentage of LV wall, with the defect threshold set at 50% of peak uptake, to identify the likely nonviable myocardium (14,15).
Biventricular Pacing
A permanent biventricular transvenous pacing system (ContaKTR; Guidant) was implanted in the patients. The atrioventricular delay was optimized by determining the longest LV filling time and the highest cardiac output using Doppler echocardiography (16). Appropriate biventricular capture was confirmed on the basis of QRS morphology.
Statistical Analysis
Results are expressed as mean ± SD. Variables were compared with the Student t test for paired or unpaired samples, the Wilcoxon matched-pair test, or the Mann–Whitney U test, as appropriate. A P value < 0.05 was considered statistically significant.
RESULTS
Before implantation, LVEF was 22.4% ± 7.2%; LVED volume index (VI), 163 ± 62 mL; LVESVI, 130 ± 61 mL; and WMSI, 2.6 ± 0.3. Implantation was successful and without complication in all patients. QRS width decreased from 139 ± 15 ms to 122 ± 8 ms (P < 0.00001). A significant perfusion defect (mean, 24% ± 12.5% of the LV wall) was detected in 11 patients, 7 with a diagnosis of ischemic cardiomyopathy. The location of the defect was anteroseptal or anteroapical in 5 patients and inferior or inferolateral in 6. One patient with ischemic cardiomyopathy and an extensive perfusion defect died 2 mo after implantation because of pump failure and was therefore excluded from further analysis. Of the remaining 19 patients who could undergo the 3-mo follow-up study, 10 had a significant perfusion defect (group A) and 9 had a normal myocardial perfusion pattern (group B) in the baseline evaluation before CRT. Table 2 compares the main characteristics of the 2 groups, which differed only in terms of quality of life (worse in group A).
Baseline Findings of Patients with (Group A) Versus Those Without (Group B) Resting Perfusion Defect
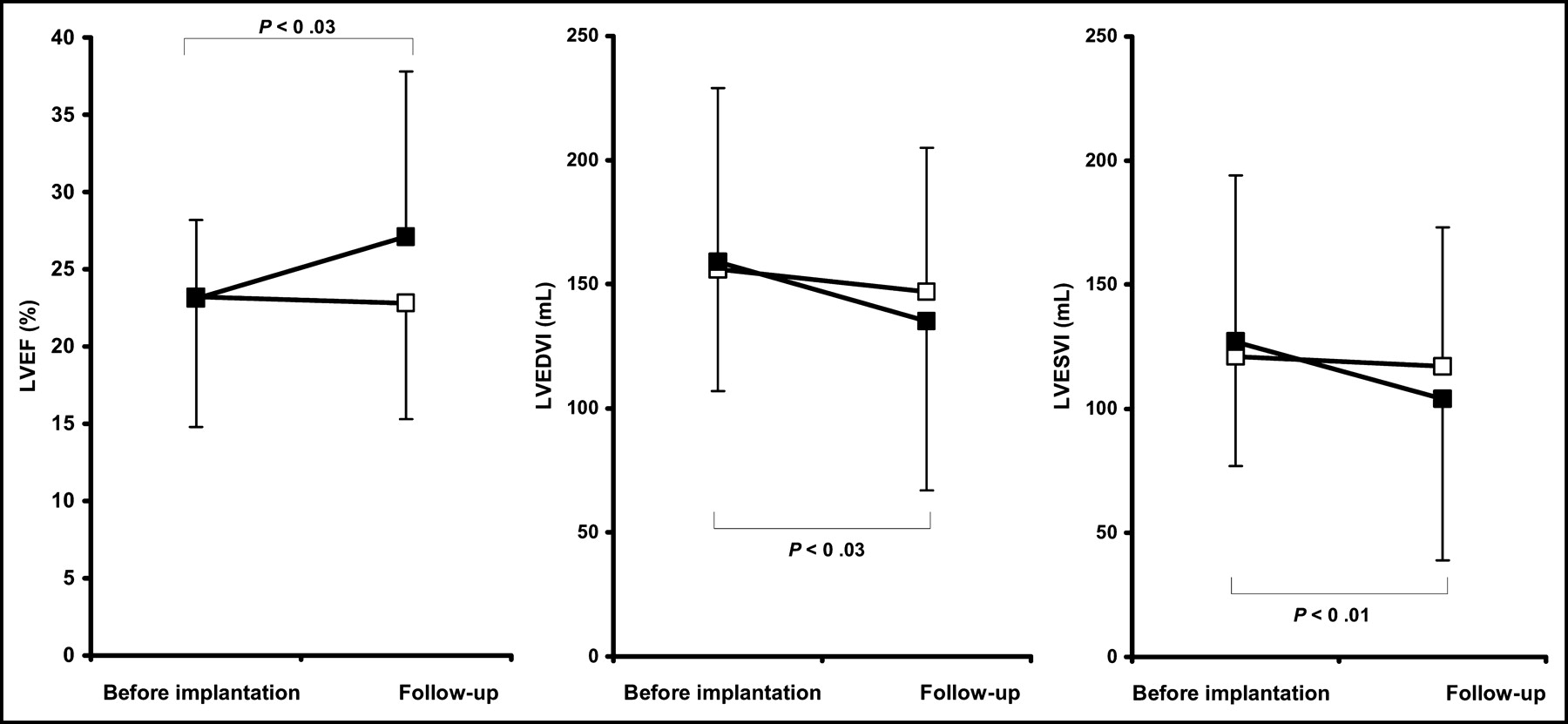
At the 3-mo follow-up, an improvement in NYHA class was registered in 6 of 10 patients of group A and in 8 of 9 of group B. Both groups showed a significant improvement in the QOL score, a significant increase in the 6-min walking distance, and a significant improvement in regional wall motion (Fig. 1). The QOL score of group A remained significantly higher and the 6-min walking distance became significantly shorter than the corresponding values of group B. The reduction in WMSI was clearly larger in group B than in group A (Fig. 1). In group A, the LVEF, LVEDVI, and LVESVI did not change significantly during CRT (Fig. 2). Conversely, in group B, the LVEF increased from 23.1% ± 8% to 27.1% ± 11% (P < 0.03), and LVEDVI and LVESVI decreased from 159 ± 70 mL to 135 ± 68 mL (P < 0.02) and from 127 ± 67 mL to 104 ± 65 mL (P < 0.01), respectively (Fig. 2).
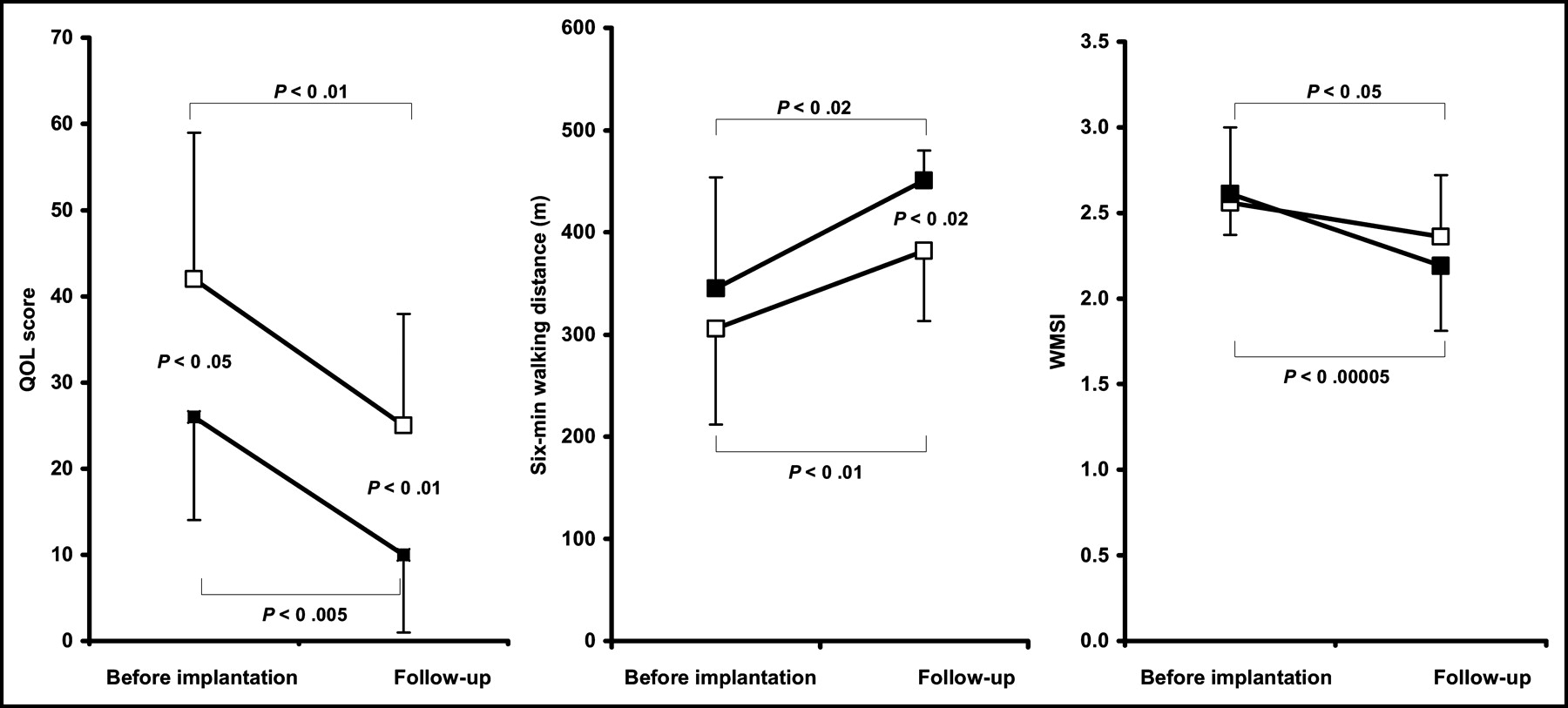
Evolution of QOL score, 6-min walking distance, and WMSI in group A (□) versus group B (▪).
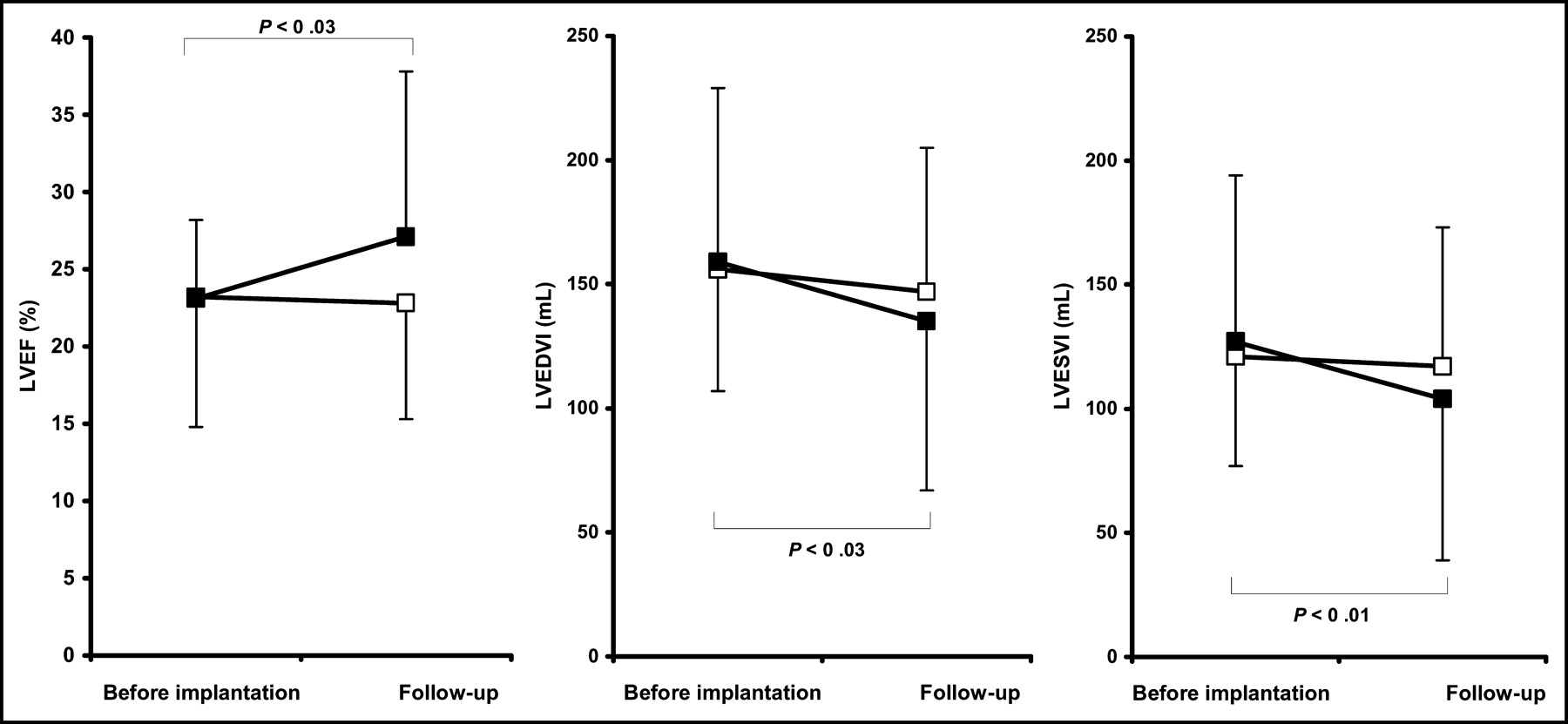
Evolution of LVEF, LVEDVI, and LVESVI in group A (□) versus group B (▪).
DISCUSSION
Although the value of CRT in advanced heart failure has been demonstrated, a proportion of patients responds suboptimally to treatment. To identify those patients, electrophysiologic characterization of the potential candidates was emphasized when CRT was proposed. Preimplantation QRS duration and its shortening under CRT were considered most important parameters for predicting response (5,17), but their value has been questioned (6). Other factors, such as LV dimensions and concomitant mitral regurgitation, were considered potential predictors of patient outcome under CRT (4–6). Also, the possible role of the cause of congestive heart failure in determining the response to CRT was examined. In a study on acute hemodynamic changes induced by CRT, Mansourati et al. did not register any difference between patients with dilated cardiomyopathy and those with ischemic cardiomyopathy (18). In a prospective study involving a patient population with heart failure of mixed causes who underwent CRT, Lunati et al. did not identify any epidemiologic or clinical variable able to predict the patients who would not have a satisfactory response to treatment (19). Other studies, however, suggested a possible role of cause on the basis of the observation that ischemic cardiomyopathy occurs slightly more frequently in patients without improvement under CRT (5,7). Reuter et al. found that ischemic heart disease, together with older age and absence of mitral regurgitation, was a significant predictor of absence of response to CRT (6). In a recent study, Duncan et al. demonstrated significantly less extensive LV reverse remodeling in patients with ischemic cardiomyopathy than in those with idiopathic dilated cardiomyopathy (8). So far, however, only scanty data are available about myocardial perfusion in candidates for CRT, and the data demonstrate mainly that CRT does not cause major changes in myocardial blood flow in patients with dilated cardiomyopathy but causes homogenization of glucose metabolism (20). To our knowledge, our study is the first that evaluates the relationship between resting perfusion pattern and response to CRT.
According to our results, severe resting uptake defects can be encountered in a series of consecutive patients with severe heart failure of mixed cause. Almost all patients with a history of ischemic cardiomyopathy had a clear resting-uptake defect, likely caused by prior infarction. Extensive hypoperfusion was observed in 4 other patients with nonischemic cardiomyopathy. This finding has various possible explanations: concomitant undiagnosed coronary artery disease cannot be excluded. Alternatively, both nonischemic fibrotic changes and abnormalities of resting perfusion have been reported in patients with dilated cardiomyopathy (21,22). Furthermore, an apparent decrease in tracer uptake because of the partial-volume effect could play a role in regions with severe regional dysfunction and wall thinning (23). Also, the presence of abnormal wall motion because of left bundle branch block could contribute to the finding of decreased tracer uptake, although no isolated septal defect was observed in our series. Independently of the actual cause, the finding of a severe uptake defect could reasonably be related to more severe disease in these patients. The main result of our study, however, is that in patients with a significant resting perfusion defect, the clinical improvement under CRT seems more limited and, most important, is not accompanied by a significant improvement in LV volumes or in LVEF, with just a limited reduction of regional asynergy. Conversely, with a single exception, the patients without abnormal findings in the preimplantation resting perfusion scan showed noteworthy clinical improvement, which was confirmed by a significant decrease in LV volumes and an increase in global LV function. If confirmed, this observation would have major clinical implications, because although epidemiologic data indicate that the combination of severe LV failure and advanced bundle branch block is relatively rare among patients with coronary artery disease (24), ischemic cardiomyopathy must be considered the most important cause of heart failure, particularly in older patients (25).
A second interesting result of our study is that gated SPECT appears a feasible technique for the assessment of baseline LV function and of its long-term changes in patients undergoing CRT. For this aim, echocardiography has, so far, been the most frequently used method (8,26–28), and its role was reinforced by the introduction of tissue Doppler imaging to select the optimal pacing site and to evaluate changes in the synchronicity of LV contraction (16,29,30). However, the feasibility of echocardiography may be limited because of acoustic window problems and the reproducibility of volumetric measurements may be inadequate. Thus, radionuclide angiography was used for LVEF measurement in another recent multicenter study about CRT (31). On the other hand, simultaneous measurement of LV volumes and function is possible and easily feasible using gated SPECT (9). With the exception of patients with severe arrhythmia, all patients can undergo the technique, and the robustness and reproducibility of LV volume measurements using gated SPECT have been demonstrated (10). A single examination could both evaluate abnormalities in the perfusion pattern, which could be relevant to the outcome of CRT, and assess the functional status of the LV to objectively demonstrate its evolution.
In our population, gated SPECT allowed reliable evaluation of both global and regional changes in LV function during CRT. The improvement in LVEF and decrease in LV volumes agree with prior reports and are closely related to clinical evolution. Volumetric reduction was registered in all patients with clinical improvement. These data suggest that gated SPECT effectively evaluates LV functional evolution in patients undergoing CRT and confirms the presence of reverse remodeling in patients who respond to treatment (8,30).
The small number of patients and the lack of comparison with other established imaging methods are the most important limitations of this study. The threshold used to define a significant perfusion defect was selected to identify probably nonviable myocardium (14,15). Therefore, the possible interactions between the presence of viable hibernating myocardium and CRT were not considered. In heart failure patients in whom myocardial hibernation is the likely cause of LV dysfunction, coronary revascularization is the treatment of choice (32). Evaluation of myocardial perfusion to exclude inducible ischemia or hibernation should be considered in heart failure patients with suspected coronary artery disease before CRT is considered. Further studies are needed to clarify this issue.
CONCLUSION
Severe resting perfusion defects encountered in candidates for CRT apparently do not preclude a positive clinical response to CRT but are related to a more limited objective improvement of LV volumes and function. Gated SPECT functional data can characterize the baseline status of patients with severe heart failure and ensure an objective basis for their follow-up during CRT.
Footnotes
Received Aug. 28, 2003; revision accepted Oct. 16, 2003.
For correspondence or reprints contact: Roberto Sciagrà, MD, Nuclear Medicine, Department of Clinical Physiopathology, University of Florence; Viale Morgagni 85, 50134 Florence, Italy.
E-mail: r.sciagra{at}dfc.unifi.it
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging for Planning of Cardiac Resynchronization Therapy
- Impact of Myocardial Scarring on Outcomes of Cardiac Resynchronization Therapy: Extent or Location?
- Prediction of Cardiac Resynchronization Therapy Response: Value of Calibrated Integrated Backscatter Imaging
- Nuclear Imaging in Cardiac Resynchronization Therapy
- Can LV Dyssynchrony as Assessed with Phase Analysis on Gated Myocardial Perfusion SPECT Predict Response to CRT?
- Extent of Viability to Predict Response to Cardiac Resynchronization Therapy in Ischemic Heart Failure Patients
- Revascularization in Severe Left Ventricular Dysfunction: The Role of Viability Testing
- Optimisation of cardiac resynchronisation therapy: addressing the problem of "non-responders"
- The year in cardiac imaging
- Dobutamine Stress 99mTc-Tetrofosmin Quantitative Gated SPECT Predicts Improvement of Cardiac Function After Carvedilol Treatment in Patients with Dilated Cardiomyopathy