


Abstract
We evaluated whether dobutamine stress 99mTc-tetrofosmin quantitative gated SPECT (D-QGS) could predict improvement of cardiac function by carvedilol therapy in patients with dilated cardiomyopathy (DCM). Methods: The study included 30 patients with idiopathic DCM and a left ventricular ejection fraction (LVEF) of <45%. D-QGS was performed in all patients to measure LVEF at rest and during dobutamine infusion (10 μg/kg/min). LVEF and left ventricular end-diastolic volume (LVEDV) were determined by echocardiography, plasma brain natriuretic peptide (BNP) was measured, and the New York Heart Association (NYHA) functional class was estimated at baseline and after 1 y of combined treatment with an angiotensin-converting enzyme (ACE) inhibitor, diuretic, and the β-blocker carvedilol. After treatment, the echocardiographic LVEF improved by >5% in 15 patients (group A) but did not improve in the remaining 15 patients (group B). Results: The baseline LVEF, LVEDV, plasma BNP, and NYHA functional class were similar in both groups. However, there was a greater increase of LVEF (ΔLVEF) with dobutamine infusion during D-QGS in group A than that in group B (12.0% ± 5.8% vs. 2.7% ± 4.2%, P < 0.0001). When a cutoff value of 6.6% for ΔLVEF was used to predict the improvement of LVEF by carvedilol therapy, the sensitivity was 86.7%, the specificity was 86.7%, and the accuracy was 86.7%. LVEDV, plasma BNP, and NYHA functional class all showed superior improvement in group A compared with group B. Conclusion: ΔLVEF measured by D-QGS was significantly larger in patients who responded to carvedilol than that in nonresponders. These findings indicate that D-QGS can be used to predict improvement of cardiac function and heart failure symptoms by carvedilol therapy in patients with idiopathic DCM.
Since Waagstein et al. (1) reported that several patients with decompensated congestive heart failure (CHF) showed clinical improvement after administration of β-blockers, various studies have demonstrated that β-blockers can have a beneficial effect in selected patients with CHF (2–5). Several reports have suggested that cardiac 123I-metaiodobenzylguanidine scintigraphy can be used to predict the effect of β-blocker therapy on CHF (6,7). However, it is generally still difficult to predict whether a patient with CHF will respond favorably to β-blocker therapy.
Dobutamine increases cardiac contractility and cardiac output, increases arterial blood pressure, and reduces total peripheral vascular resistance (8). Dobutamine gated blood-pool scintigraphy has been used to predict the improvement of cardiac function by β-blocker therapy in patients with dilated cardiomyopathy (DCM) (9). There have also been several reports about the prediction of functional improvement due to β-blocker therapy by using dobutamine stress echocardiography in patients with DCM (10,11).
99mTc-Labeled perfusion tracers allow the simultaneous assessment of myocardial perfusion and left ventricular (LV) function by quantitative gated SPECT (QGS) (12–14). Several studies have suggested that dobutamine stress 99mTc QGS can be used to predict myocardial viability and can identify areas of stunned myocardium in patients with ischemic cardiomyopathy (15,16). However, to our knowledge, there have been no reports concerning the use of dobutamine stress 99mTc QGS to predict functional improvement due to β-blocker therapy in patients with DCM.
Accordingly, this study was performed to determine whether dobutamine stress 99mTc-tetrofosmin QGS (D-QGS) could predict the improvement of cardiac function by carvedilol treatment in patients with DCM.
MATERIALS AND METHODS
Study Population
Thirty patients, comprising 21 men and 9 women (mean age ± SD, 55 ± 10 y; range, 38–72 y), who presented with recently diagnosed (<2 mo) idiopathic DCM were included in the study. A detailed history and physical were obtained from all patients before enrollment. Chest radiography, standard electrocardiography, echocardiography, and cardiac catheterization (including coronary angiography and left ventriculography) were performed in all patients. Patients with acute or chronic myocarditis, significant coronary artery stenosis, or valvular disease were excluded. All patients were in New York Heart Association (NYHA) functional class II or III and had an echocardiographic LV ejection fraction (LVEF) < 45%.
All patients were being treated with an angiotensin-converting enzyme (ACE) inhibitor and a loop diuretic. Treatment with digitalis and vasodilators was also allowed. The study was approved by the ethics review board of our institution, and written informed consent was obtained from each subject.
Study Protocol
The initial dose of carvedilol was 1.25–2.5 mg/d, and this was increased over 3–5 mo to reach the maintenance dose of 20 mg/d. Baseline echocardiography and D-QGS were performed in all patients. After the 1-y follow-up period, echocardiography was repeated in all patients. There was an increase of LVEF by >5% in 15 patients (group A), whereas the other 15 patients showed <5% improvement of LVEF (group B).
The plasma brain natriuretic peptide (BNP) concentration was also measured, and the NYHA functional class was determined at baseline and after 1 y of carvedilol treatment.
Echocardiography
Echocardiography was performed using standard methods by 2 independent and experienced echocardiographers who had no knowledge of the study. LV end-diastolic volume (LVEDV) and LVEF were calculated using the modified method of Simpson (17). The interobserver and intraobserver variation of these measurements was small (LVEDV: r = 0.90, P < 0.001, and r = 0.94, P < 0.0001, respectively; LVEF: r = 0.90, P < 0.001, and r = 0.93, P < 0.0001, respectively).
D-QGS
SPECT was performed with a dedicated single-head imaging system (Millennium MPR; General Electric Medical Systems). The energy output, uniformity, and linearity of the system were constantly corrected. Sixty-four equidistant projections were acquired over a 180° arc from the 45° right anterior oblique projection to the 45° left posterior oblique projection using a 64 × 64 matrix. Standard acquisition of electrocardiographically (ECG)-gated images was performed in 64 steps at 20 s per step using the step-acquisition mode. Rapid-acquisition of ECG-gated images was also performed in 64 steps at 10 s per step using the same mode, with the camera acquiring data at each azimuth stop as well as during rotation between stops. Eight frames per cardiac cycle were acquired in each projection. 99mTc-Tetrofosmin (740 MBq) was injected intravenously at rest, and standard acquisition of ECG-gated resting images was done after 30 min. Immediately after the completion of standard-acquisition imaging, the dobutamine stress ECG-gated SPECT study with rapid acquisition was started. Dobutamine (10 μg/kg/min) was infused over 15 min and rapid acquisition of ECG-gated images was performed during the final 640 s of dobutamine infusion. The blood pressure and ECG were monitored at 1-min intervals during dobutamine infusion.
Standard-acquisition images were used to assess tracer uptake and to measure the LV volume and LVEF at rest. Nongated images were created by summing all of the gated images obtained in the standard-acquisition mode and were used to assess tracer uptake. Rapid-acquisition images were used to assess the LV volume and LVEF during dobutamine infusion. In a preliminary study, we confirmed that resting LVEDV measured on standard-acquisition images was correlated with resting LVEDV measured on rapid-acquisition images (r = 0.947, P < 0.0001). There was also a significant correlation between resting LVEF measured on standard-acquisition images and rapid-acquisition images (r = 0.965, P < 0.0001).
Transaxial slices (6.4-mm thick) were reconstructed with a Butterworth filter (order, 10.0; critical frequency, 0.40 cycle/cm for standard-acquisition and rapid-acquisition data) by the filtered backprojection method (ramp filter) on a computer (GENIE; General Electric Medical Systems) using automatic processing software for SPECT (Cedars Auto SPECT) (12). Automatic LV function analysis software (Cedars QGS) (13,14) was used to calculate the LVEF.
The percentage change of LVEF during dobutamine infusion (ΔLVEF) was calculated as the LVEF during the dobutamine infusion minus the resting LVEF. Representative LV functional images obtained by D-QGS are shown in Figure 1.

Representative LV functional images obtained by D-QGS. Outer cage and solid surface represent endocardial surface at end-diastole and end-systole, respectively. Wall motion is diffusely hypokinetic at rest based on standard-acquisition ECG-gated images. During dobutamine stress, however, wall motion improves toward normal.
Total Defect Score (TDS) on 99mTc-Tetrofosmin SPECT Images
The resting 99mTc-tetrofosmin SPECT images of each patient were divided into 20 segments, using a previously described method (9,18–20). Short-axis images obtained at the base, middle, and apex of the ventricles were divided into 6 segments. The apical part of the vertical long-axis image was also divided into 2 segments. Regional tracer uptake was assessed semiquantitatively using a 4-point scoring system (0 = normal uptake; 1 = mildly reduced uptake; 2 = moderately reduced uptake; 3 = significantly reduced uptake). Then, the TDS was calculated as the sum of all segmented defect scores.
Plasma BNP Concentration
Blood samples were collected into test tubes containing ethylenediaminetetraacetic acid after each patient had rested in the supine position for at least 30 min. Plasma was separated by centrifugation and was frozen at −84°C. Then the plasma concentration of BNP was measured using a specific immunoradiometric assay.
Data Analysis and Statistics
Statistical analysis was performed using Statview software (Abacus Concepts) and a Macintosh computer (Apple Computer, Inc.). Numeric results are expressed as the mean ± SD. Comparison of baseline data between the 2 groups was done by the χ2 test. Differences between continuous variables were evaluated using the unpaired t test. Changes of NYHA functional class were assessed using the Wilcoxon matched pairs signed ranks test. The effects of carvedilol treatment were assessed by the paired t test for within-group comparisons and by ANOVA for between-group changes. Linear regression analysis was used to determine the relationship between continuous variables. The cutoff value of ΔLVEF that predicted the improvement of LVEF was identified by receiver-operating-characteristic analysis. In all analyses, P < 0.05 was considered statistically significant.
RESULTS
Clinical Characteristics
There were no significant differences of hemodynamic characteristics or cardiac medications between the 2 groups on entry into the study. At baseline, the echocardiographic LVEDV, LVEF, plasma BNP concentration, and NYHA functional class were similar in both groups (Table 1). All patients were clinically stable and no major events occurred during the follow-up period.
Demographics and Clinical Characteristics
Cardiac 99mTc-Tetrofosmin SPECT
Table 1 provides a summary of the TDS data for both groups determined by cardiac 99mTc-tetrofosmin SPECT. The TDS was similar in both groups.
Echocardiographic Findings at Baseline and After Treatment
The changes of LVEDV and LVEF are summarized in Table 2. In group A, LVEDV decreased significantly between baseline (197 ± 44 mL) and after 1 y of carvedilol therapy (162 ± 34 mL) (P < 0.01). In contrast, group B showed no significant difference of LVEDV between baseline and 1 y of treatment. After carvedilol therapy, the LVEDV of group A was significantly smaller than that of group B (P < 0.01). In group A, by definition, LVEF was significantly increased after 1 y of treatment relative to the baseline value (from 32% ± 8% to 47% ± 10%, P < 0.0001). In contrast, there was no significant change of LVEF in group B after 1 y. Furthermore, the LVEF of group A was significantly larger than that of group B after 1 y (P < 0.0001).
Changes in LVEDV, LVEF, NYHA Functional Class, and Plasma BNP in Both Groups
NYHA Functional Class at Baseline and After Treatment
The NYHA functional class data are summarized in Table 2. Patients in both groups showed significant improvement of their functional class after 1 y of carvedilol therapy compared with the baseline status (group A, P < 0.001; group B, P < 0.01). However, the NYHA functional class after treatment was better in group A than that in group B (P < 0.05).
Plasma BNP Concentration at Baseline and After Treatment
Plasma BNP concentrations are also shown in Table 2. In group A, the plasma BNP concentration decreased significantly after 6 mo of carvedilol therapy compared with the baseline value (from 234 ± 179 pg/mL to 134 ± 94 pg/mL, P < 0.01). In contrast, there was no significant difference between the baseline and 1-y values in group B.
Baseline D-QGS Findings
Dobutamine significantly increased the heart rate (from 68 ± 11 beats/min at rest to 84 ± 14 beats/min during infusion, P < 0.0001) and the systolic blood pressure (from 120 ± 12 mm Hg at rest to 136 ± 16 mm Hg during infusion, P < 0.0001) in both groups combined. There were no significant intergroup differences of the changes in heart rate and systolic blood pressure.
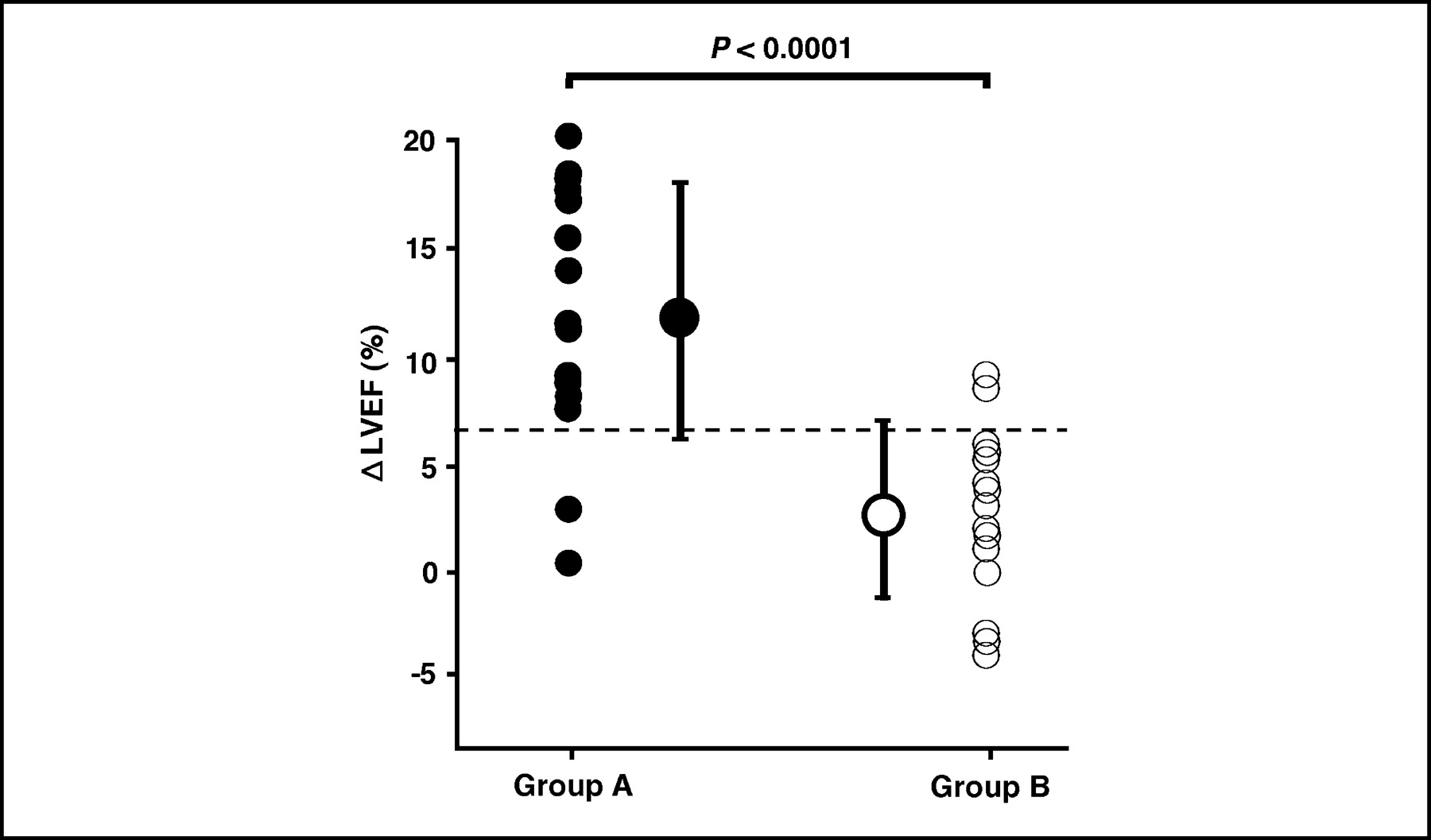
The changes of LVEF measured by QGS are summarized in Table 3. Echocardiographic LVEF was correlated with resting LVEF measured by QGS (r = 0.956, P < 0.0001) (Fig. 2A), and echocardiographic LVEDV was correlated with resting LVEDV measured by QGS (r = 0.913, P < 0.0001) (Fig. 2B). In both groups, LVEF was increased by dobutamine infusion (group A: from 31.3% ± 8.3% to 43.3% ± 9.9%, P < 0.0001; group B: from 33.0% ± 7.5% to 35.7% ± 7.8%, P < 0.05), but the change was greater in group A than that in group B (P < 0.05). In addition, ΔLVEF was larger in group A than that in group B (12.0% ± 5.8% vs. 2.7% ± 4.2%, P < 0.0001) (Table 3; Fig. 3). When a ΔLVEF cutoff value of 6.6% was used to predict improvement of LVEF at 1 y, the sensitivity was 86.7%, the specificity was 86.7%, and the accuracy was 86.7%.

Relationship between echocardiographic LVEF and resting LVEF measured by QGS (A) and echocardiographic LVEDV and resting LVEDV measured by QGS (B).

ΔLVEF at baseline. •, group A; ○, group B.
Changes of LVEF Measured by QGS in Both Groups
Relationship Between ΔLVEF and Change of Echocardiographic LVEF
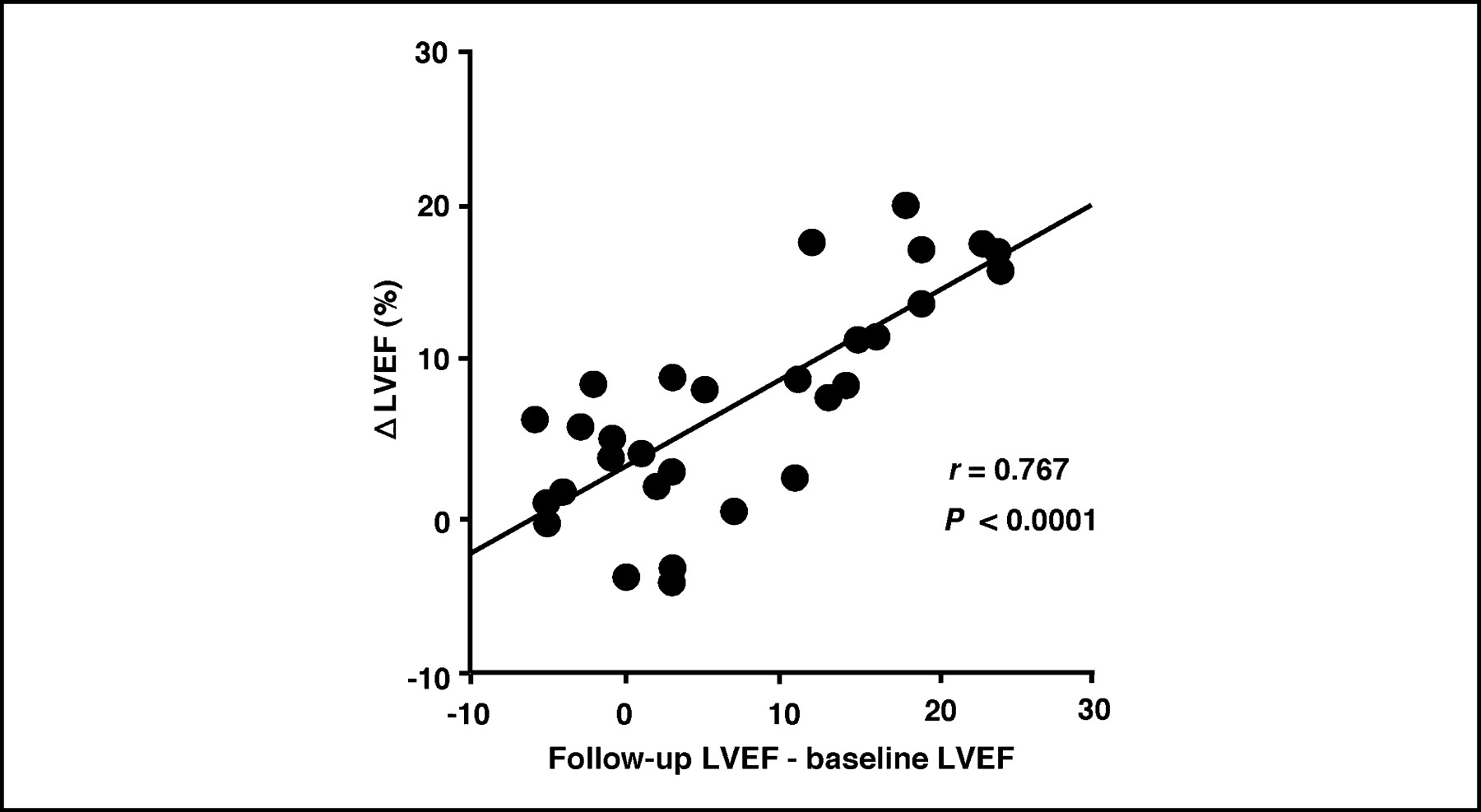
There was a significant correlation between the percentage change of LVEF caused by dobutamine infusion during D-QGS (ΔLVEF) and the changes of echocardiographic LVEF after 1 y of treatment (r = 0.767, P < 0.0001) (Fig. 4).

Relationship between percentage change of LVEF with dobutamine infusion during D-QGS (ΔLVEF) and echocardiographic change of LVEF after follow-up.
DISCUSSION
Idiopathic DCM is characterized by dilation of the ventricles and decreased systolic function, and it generally has a poor prognosis. The 1-y mortality rate of patients with idiopathic DCM is as high as 25%, and the 5-y mortality rate ranges from 20% to 50% (21). However, a significant proportion of these patients may improve spontaneously over time (22,23). This high mortality rate combined with the possibility of late spontaneous improvement in cardiac function creates a management dilemma. Therefore, the ability to identify patients with idiopathic DCM who are likely to show myocardial recovery would be valuable.
Earlier detection of this disease and introduction of treatment with β-blockers may have led to the recent improvement of the prognosis (2–5). The beneficial actions of β-blockers on DCM include (a) enhancement of the myocardial energy available for synthetic and reparative processes; (b) improvement of diastolic relaxation, filling, and compliance; (c) inhibition of sympathetically mediated vasoconstriction via prostaglandin and renin; (d) protection against catecholamine-induced myocardial damage and necrosis; and (e) upregulation of β-adrenergic receptors to restore catecholamine responsiveness (24,25). It has also been reported that β-blockers have hemodynamic and energetic benefits (26) as well as enhancing cell-mediated immunity and improving T-cell function (27). Furthermore, the third-generation β-blocker carvedilol reduces the occurrence of apoptosis in cardiac myocytes as well as reducing the heart rate (28). Carvedilol is also reported to have a cardioprotective effect, since it decreases elevated oxidative stress in failing human myocardium (29). These beneficial effects lead to a reduction in the risk of death and the risk of hospitalization due to cardiovascular causes (4,5). However, it is still difficult to predict whether patients with CHF will respond to treatment with β-blockers.
In this study, improvement of LV function was seen in 15 of 30 patients (50%) with DCM. In keeping with previous findings, this relatively high improvement rate may be related to the earlier use of ACE inhibitors and β-blockers. In clinical studies, it is difficult to identify responders to treatment among patients with DCM. Cross et al. (30) reported a better prognosis in nonischemic cardiomyopathy patients who responded to therapy with an increase of LVEF by at least 5% during follow-up compared with that of patients who did not respond. Therefore, we used a 5% change of LVEF during a 1-y follow-up period to divide our subjects into responders and nonresponders. Assessment of LVEF at the end of the study was done by echocardiography without using gated SPECT because this method is more cost-effective. Moreover, the LV volume and LVEF measured by echocardiography were significantly correlated with the same parameters measured by gated SPECT in our study, justifying the use of echocardiographic LVEF for follow-up.
The plasma BNP level is a useful prognostic indicator in patients with CHF (31) since BNP is a ventricular hormone (32). Plasma BNP is reported to show correlations with abnormalities of LVEF and LV end-diastolic pressure (32) as well as with LV mass (33). The decrease of BNP after carvedilol treatment was presumably due to a decreased LV filling pressure, improvement of LV remodeling, or both. The decrease of BNP during carvedilol therapy may also have reflected the improvement of LV diastolic function secondary to effects of this drug on cardiac hypertrophy and fibrosis. In this study, plasma BNP showed a significantly greater decrease in the responders than that in the nonresponders. Therefore, the plasma BNP response to carvedilol treatment may be useful for predicting functional improvement in patients with DCM. Moreover, the responders also showed an improvement in symptoms of heart failure, as measured by changes of the NYHA functional class. When we evaluated exercise tolerance (6-min walking distance) at baseline and after 1 y of carvedilol therapy in 14 patients (7 each from responder and nonresponder groups), a marked improvement of this parameter was observed in both groups and there was no significant intergroup difference (data not shown).
Dobutamine has potent inotropic activity with minimal chronotropic, arrhythmogenic, or vascular effects (8), and it causes a relatively greater increase of coronary blood flow than that of other inotropic agents at the same level of myocardial oxygen consumption (34). Myocardial viability can be assessed by using low-dose dobutamine infusion to produce functional improvement of regions with resting dyssynergy, and the response of wall motion measured by echocardiography during dobutamine infusion can predict the recovery of stunned and hibernating myocardium in patients with ischemic heart disease (35). There have also been several reports relating to the prediction of functional recovery after β-blocker therapy by dobutamine stress echocardiography in patients with DCM (10,11). Moreover, we previously showed that dobutamine gated blood-pool scintigraphy could be used to predict improvement of cardiac function by β-blocker therapy in patients with idiopathic DCM (9). In that study, the contractile reserve (LVEF) measured by low-dose dobutamine (5, 10, and 15 μg/kg/min) gated blood-pool scintigraphy before treatment was associated with the improvement of LVEF on echocardiographic follow-up.
Myocardial perfusion tracers, such as 99mTc, allow simultaneous assessment of myocardial perfusion and LV function by QGS. Automated techniques for defining the endocardial boundaries and performing quantitative 3-dimensional assessment of regional ventricular function throughout the cardiac cycle by QGS are now available (12–14). Dobutamine stress 99mTc QGS has been used to assess myocardial viability and to identify areas of stunned myocardium in patients with ischemic cardiomyopathy (15,16). Because of recent developments in computer analysis, it is easier to assess LV function by dobutamine stress 99mTc QGS than by dobutamine stress echocardiography. However, to our knowledge, dobutamine stress 99mTc QGS has not been used previously to predict functional improvement after β-blocker therapy in patients with DCM. This study demonstrated that D-QGS could predict the improvement of cardiac function due to carvedilol therapy in patients with DCM. We found that cardiac function can be expected to improve over the long term when the ΔLVEF (determined by D-QGS) is >6.6%. Moreover, we found a significant correlation between ΔLVEF and the long-term echocardiographic changes of LVEF. The exact mechanism responsible for the recovery of systolic function during dobutamine infusion is unclear. Differences in the extent of downregulation of the myocardial β-adrenergic system may play a role because a diminished β-adrenergic contractile reserve was reported to predict the clinical outcome in patients with DCM (36). Therefore, our findings suggest that β-adrenergic stimulation of contraction may be the predominant factor explaining the improvement of ΔLVEF.
The severity of DCM is often assessed by myocardial perfusion imaging (37). However, myocardial perfusion SPECT findings are quite varied in DCM patients, since uptake is not homogeneous and defects can be patchy, small, or large (38). Myocardial perfusion SPECT may also reflect myocardial fibrosis in patients with DCM (39), and it has been reported to identify responders to resynchronization therapy (40). In the present study, we performed myocardial perfusion SPECT with 99mTc-tetrofosmin and calculated the TDS in all of our patients, but there was no significant difference of TDS between the responder and nonresponder groups. Thus, perfusion imaging could not predict the improvement of cardiac function after carvedilol treatment in our patients, suggesting that it is important to evaluate ΔLVEF by D-QGS when treating DCM.
There are 2 methods of evaluating LV function in patients with heart failure. Assessment of regional function (wall motion score index) is useful for evaluation of ischemic cardiomyopathy with asynergy of the LV wall motion (15), whereas assessment of global function (LVEF) is more useful for evaluation of nonischemic cardiomyopathy without asynergy (9). Therefore, we investigated the improvement of echocardiographic LVEF during follow-up of our patients with DCM.
The small number of patients included in this study was a limitation. In addition, all of our patients were clinically stable and no major events occurred during follow-up. In general, it is unusual to observe such a good short-term outcome in patients with DCM, suggesting that our subjects probably had mild-to-moderate heart failure rather than severe failure. In the future, we need to evaluate whether D-QGS can predict the improvement of cardiac function by carvedilol therapy in a larger group of patients.
CONCLUSION
ΔLVEF measured by D-QGS was significantly larger in patients who responded to carvedilol therapy than that in nonresponders. In addition, there was a significant correlation between ΔLVEF and the long-term changes of echocardiographic LVEF. These findings indicate that D-QGS can be used to predict the improvement of cardiac function by carvedilol treatment in patients who have idiopathic DCM.
Footnotes
Received Mar. 14, 2004; revision accepted June 2, 2004.
For correspondence or reprints contact: Shu Kasama, MD, Department of Cardiovascular Medicine, Gunma University School of Medicine, 3-39-15, Showa-machi, Maebashi, Gunma 371-0034, Japan.
E-mail: s-kasama{at}bay.wind.ne.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Additive Effects of Spironolactone and Candesartan on Cardiac Sympathetic Nerve Activity and Left Ventricular Remodeling in Patients with Congestive Heart Failure
- Effects of torasemide on cardiac sympathetic nerve activity and left ventricular remodelling in patients with congestive heart failure
- Comparative effects of valsartan and enalapril on cardiac sympathetic nerve activity and plasma brain natriuretic peptide in patients with congestive heart failure