


Abstract
The cell-membrane folate receptor is a potential molecular target for tumor-selective drug delivery, including radiolabeled folate-chelate conjugates for diagnostic imaging. We report here the initial clinical study of such an agent, 111In-diethylenetriaminepentaacetic acid (DTPA)-folate, evaluated for diagnosis of ovarian malignancy. Methods: Thirty-five women were enrolled in a phase I/II clinical study, with 33 completing the surgical follow-up required by the study protocol for definition of disease status. Patients either had a pathologically proven malignancy or were scheduled for surgery for suspected new ovarian cancer (n = 26), recurrent ovarian cancer (n = 5), or endometrial cancer (n = 2). 111In-DTPA-folate was administered as an intravenous bolus, and whole-body images were obtained at 30 min, 4 h, and (for the first 19 patients) 24 h after injection; SPECT also was done at the delayed imaging times. For 19 of the patients, unlabeled free folic acid was injected before administration of 111In-DTPA-folate to also assess the impact of folate loading on tracer biodistribution. Masked and unmasked readings of the images by 2 nuclear medicine physicians were compared with the pathologic findings after surgery. Results: Among 33 patients who had surgical intervention, 14 had new or recurrent malignant tumors. All of 7 newly diagnosed ovarian carcinomas were identified by both masked readers (sensitivity, 100%). The sensitivity for detection of 7 recurrent malignancies was 38% for masked readings and 85% for unmasked readings, indicating that correlation with anatomic imaging studies (CT) was highly important in diagnosis of these lesions. Eighteen of the studied patients were found to have benign masses; for this limited population, the specificity of 111In-DTPA-folate scintigraphy was 76% and 82% for the masked and unmasked analyses, respectively. Conclusion: 111In-DTPA-folate is safe, and possibly effective, for scintigraphy differentiating between malignant and benign ovarian masses.
Approximately 23,000 women in the United States were diagnosed with ovarian cancer in 2002, and only about 50% of these women will survive more than 5 y (1). One of the reasons for low survival is the difficulty in diagnosing this cancer. Current anatomic imaging procedures (e.g., transvaginal ultrasonography) are effective in locating masses. However, they cannot differentiate between benign and malignant lesions. The serum tumor marker CA-125 is elevated in 80% of women with epithelial ovarian cancers. However, only 50% of patients with stage I cancer have elevated levels of this marker. In addition, a significant proportion of healthy women or women with benign disease have elevated CA-125 levels (2,3). Because of the risk of tumor rupture and peritoneal seeding, fine-needle aspiration generally is not used for evaluation of ovarian masses. Patients with suspected ovarian cancer must therefore undergo invasive surgical procedures for diagnosis.
The NIH Consensus Conference on Ovarian Cancer emphasized that preoperative knowledge of whether a mass is benign or malignant is important to ensure proper surgical management (4). For a mass known to be malignant, full laparotomy by a qualified gynecologic oncologist is necessary to stage the cancer and to perform optimal debulking or resection. By comparison, for a benign mass, a less invasive laparoscopic approach can be performed by a general gynecologist for diagnosis or removal of the mass. An additional problem in the management of ovarian cancer relates to the diagnosis of recurrent disease; serial CT scans, taken over several months, are required to monitor for changes in suspected tumor growth. An accurate diagnostic imaging procedure might allow more rapid detection, reduced costs, and proper surgical management of ovarian cancer.
PET with 18F-FDG has numerous current clinical applications in the differentiation of benign and malignant masses, based on the elevated rates of glycolysis that are observed in many cancers (5). However, a clear clinical role has yet to be established for 18F-FDG in the initial diagnosis and staging of ovarian cancer (6–8). Results have been mixed for the reported use of 18F-FDG PET in primary untreated ovarian cancer and for the assessment of patients for recurrence of ovarian carcinoma. 18F-FDG PET may have a role as an adjunct to conventional imaging techniques in the assessment of macroscopic disease; however, CT, ultrasonography, and 18F-FDG PET currently are clearly inferior to laparoscopy for detection of microscopic disease in patients with ovarian cancer (6–8).
More than 90% of ovarian and endometrial cancers express a high-affinity folate receptor, involved in cellular folate accumulation by receptor-mediated endocytosis, that is absent from most normal tissues (9–14). Accordingly, these tumors are excellent candidates for molecular targeting through the folate receptor system. Folic acid, a small essential vitamin, can be conjugated to various agents through relatively simple chemistry while retaining affinity for the folate receptor. In preclinical studies, folic acid conjugates have been used for tumor targeting of toxins (15–17), chemotherapeutic agents (18–20), paramagnetic compounds (21,22), and radionuclides (67Ga, 111In, and 99mTc) (23–28).
One such radiopharmaceutical, 111In-diethylenetriaminepentaacetic acid (DTPA)-folate, has been evaluated in preclinical studies and shown to be an excellent imaging agent for targeting folate-receptor-expressing tumor xenografts (25,26). The present study was undertaken to provide an initial assessment of the safety, biodistribution, and possible efficacy of this radiopharmaceutical as a diagnostic imaging agent for ovarian cancer in humans.
MATERIALS AND METHODS
Radiopharmaceutical Preparation
DTPA was conjugated to folic acid as described previously (25) and was supplied as part of a kit-formulated radiopharmaceutical drug product. The 111In-DTPA-folate radiopharmaceutical was compounded from the 111In(III) chloride commercially marketed in the United States for use in compounding 111In-satumomab pendetide. The DTPA-folate conjugate was labeled with 111In at room temperature according to a compounding protocol based on that described by Mathias and Green (29). The radiochemical purity of each preparation of 111In-labeled conjugate was determined by thin-layer chromatography as described previously (25,26,29). All doses of 111In-DTPA-folate exceeded 92% radiochemical purity at the time of administration and were used within 4 h of radiolabeling.
Patient Studies
Study Protocol.
The study protocol was approved by the institutional review board at each participating institution. Each subject gave written, informed consent before inclusion in the study. Eligible subjects were women aged 18 y or older with one of the following: an ovarian mass, demonstrated by CT or ultrasonography, that was suspected to represent ovarian cancer and for which pathologic evaluation after laparotomy, laparoscopy, or percutaneous biopsy was planned; suspected recurrent ovarian or endometrial cancer, demonstrated by CT or ultrasonography, and for which pathologic evaluation after laparotomy, laparoscopy, or percutaneous biopsy was planned; or pathologically proven ovarian or endometrial cancer (primary, metastatic, or recurrent), with at least one site of measurable disease demonstrated by CT or MRI. Pregnant and lactating patients were excluded, as were those with a history of congestive heart failure, unstable angina, or recent myocardial infarction (within 6 mo); septicemia, severe infection, or acute hepatitis; inadequate bone marrow, renal, or hepatic function; known or suspected kidney disease; or a Zubrod performance score greater than 2. In addition, patients were ineligible if they had taken nonsteroidal anti-inflammatory medication within the previous 5 d, could not stop taking folic acid supplements 2 d before imaging, or had any preexisting medical condition that precluded the intravenous administration of fluids required by the protocol.
Patients were studied in 8 groups that received varying amounts of DTPA-folate, 111In, and preinjected folic acid (Table 1). Preliminary estimates of radiation absorbed dose were made from mouse biodistribution data and the results of a prior study of 3 healthy women who received a 3.7-MBq dose of 111In-DTPA-folate (30). The initial group of 3 patients in the present study received a 37-MBq dose of 111In-DTPA-folate and underwent limited imaging, confirming that an administered dose of 185 MBq would be acceptable for use in the remaining 7 groups. The radiation absorbed dose estimates calculated from the human biodistribution data of the present study will be reported later.
Dosing Groups for 111In-DTPA-Folate
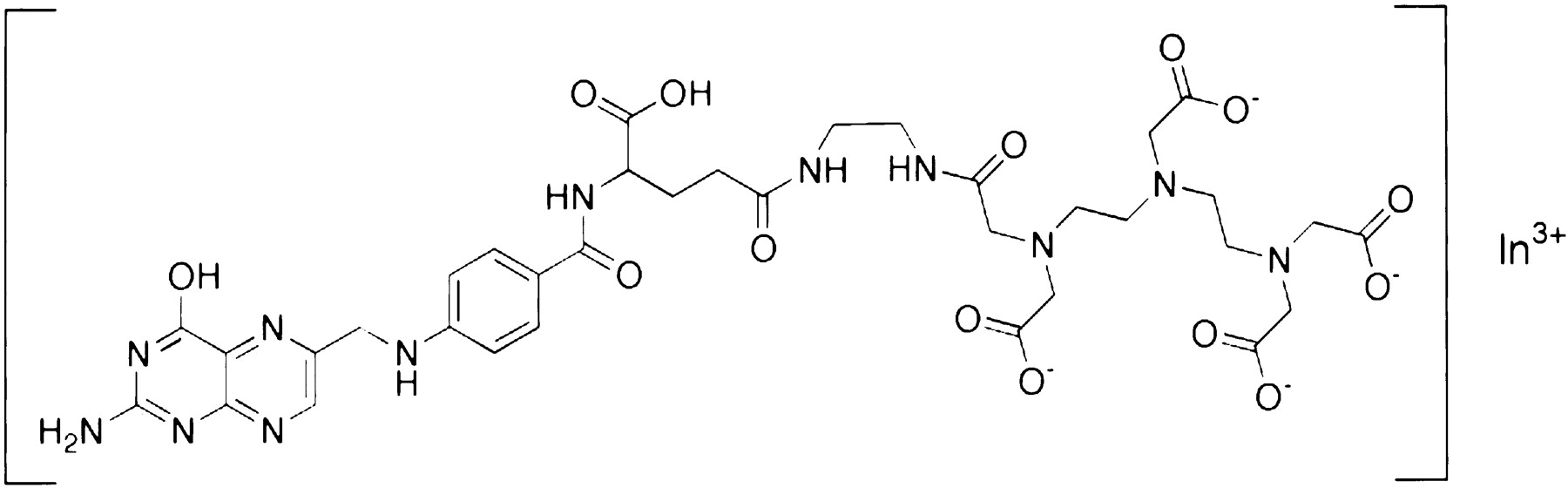
111In-DTPA-folate (Fig. 1) was administered by bolus intravenous injection through a peripheral venous catheter. Before administration of the radiopharmaceutical, a venous blood sample was drawn for determination of serum folate. An infusion of 1 L of 0.9% saline solution began 30 min before radiopharmaceutical administration and continued for 5 h. Patients who were pretreated with free folic acid were given the injection intravenously 1–2 min before injection of the radiopharmaceutical. Patients were monitored over the entire course of the imaging study for signs of adverse reactions.

Structural formula of 111In-DTPA-folate.
Imaging Procedure.
Anterior and posterior whole-body planar scintigrams were obtained at 30 min, 4 h, and (for the first 19 patients) 24 h after injection with a dual-detector gamma camera equipped with medium-energy parallel-hole collimators. Whole-body scanning was performed at a maximum speed of 8 cm/min with an optimal total imaging time of 30 min. SPECT images of the pelvis were obtained at the 4- and 24-h imaging times as well. SPECT images were collected using a dual- or triple-head camera with 120 total projections over 360°. The scanning duration was 30 s per step. Images were acquired in a 128 × 128 matrix. SPECT images were reconstructed by filtered backprojection; a Butterworth filter (order, 5; cutoff, 0.035 cycles per centimeter) or similar Wiener filter was used.
The images were interpreted, independently, by 2 nuclear medicine physicians and were evaluated for abnormal uptake of 111In-DTPA-folate. In the first reading, the physicians were unaware of clinical history, including CT, sonographic, or MR images. In the second reading, designed to mirror the typical clinical setting, both physicians were given access to clinical information and prior imaging studies that would normally be available during presurgical scan interpretation. Images were scored as showing definitely increased uptake (++), faint uptake (+), or no abnormal uptake (0), with the positive interpretation for malignancy being based on focal increased uptake of radiotracer at sites not corresponding to obvious normal anatomic structures.
After the imaging was completed, surgery was performed by a gynecologic oncologist, and resected tissue was examined by a pathologist to confirm the presence or absence of neoplastic tissue. The pathology report was used as the reference standard for comparison with the scintigraphic imaging analysis.
RESULTS
Patient Demographics
Thirty-five women (mean age, 55 y; age range, 31–78 y) with suspected ovarian or endometrial malignancy were enrolled in the study. All except 2 patients, who had their surgeries canceled, completed the study. The mean (±SD) baseline serum folic acid concentration was 15.2 ± 0.5 ng/mL (range, 3.4–52.9 ng/mL). For all patients completing the study, the tissue removed during surgery was pathologically evaluated (1 patient [patient 19] underwent only fine-needle biopsy). The data from this analysis are reported in Table 2. Eighteen of the analyzed masses (54%) proved to be benign. Among the 14 patients (42%) with malignancies, 7 new ovarian malignancies and 7 recurrent cancers (5 ovarian and 2 endometrial) were identified. One additional patient had a mass that was rated a borderline malignancy.
Final Pathologic Classifications for 33 Patients
Safety Data
The single-dose intravenous injection of 111In-DTPA-folate was well tolerated by all patients. Eight of the 35 patients had minor adverse reactions during the study, with 5 of these observed reactions possibly being related to administration of the 111In-DTPA-folate drug product. Of the 5 subjects who had adverse reactions, a rash developed in 2, 1 had a warm sensation in the chest immediately after injection, 1 indicated discomfort in her kidneys, and 1 had shortness of breath while walking. All these reactions spontaneously resolved without sequelae. There were no serious adverse reactions or changes in vital signs.
Efficacy of Imaging
Imaging Parameters.
Planar images were obtained at 30 min primarily for dosimetry evaluation; these images were dominated by renal and urinary bladder activity and were not further evaluated for detection of lesions. Images obtained at 4 and 24 h provided comparable diagnostic information; accordingly, the 24-h imaging time was eliminated after the first 19 patients to simplify the phase II component of the protocol. As predicted from preclinical biodistribution studies in mice (26), uptake of 111In-DTPA-folate was evident in the kidneys of all patients. The partial retention of 111In-DTPA-folate by the kidneys is presumed to be due to the presence of folate receptors in the proximal tubules (24,26,27,31,32). In some patients, increased 111In uptake was also observed in the liver and spleen.
In animal studies, tumor-to-background contrast was optimized by coinjection of a low dose of free folic acid with the 111In-DTPA-folate (26). In this initial clinical study, images were evaluated qualitatively, with patients who had received a low-dose preinjection of free folate being compared with patients who had not. Although the interpatient variability could not be controlled, preinjection of free folate did appear to reduce tissue background activity; however, the free folate preinjection did not appear to appreciably improve 111In-DTPA-folate tumor-to-background contrast. Definitive assessment of the effects of folate loading would require repeated studies of individual patients, which unfortunately was not practical within the limits of the present study.
Newly Diagnosed Pelvic Masses.
The scintigraphic results for 26 patients presenting with a new pelvic mass are summarized in Tables 3 and 4. Seven of the newly detected masses were malignant tumors (6 ovarian and 1 endometrial). The mass in 1 patient was classified as a borderline malignancy, and the remaining 18 were benign pelvic masses. Representative scintigrams from patients with malignant and benign lesions are shown in Figure 2.
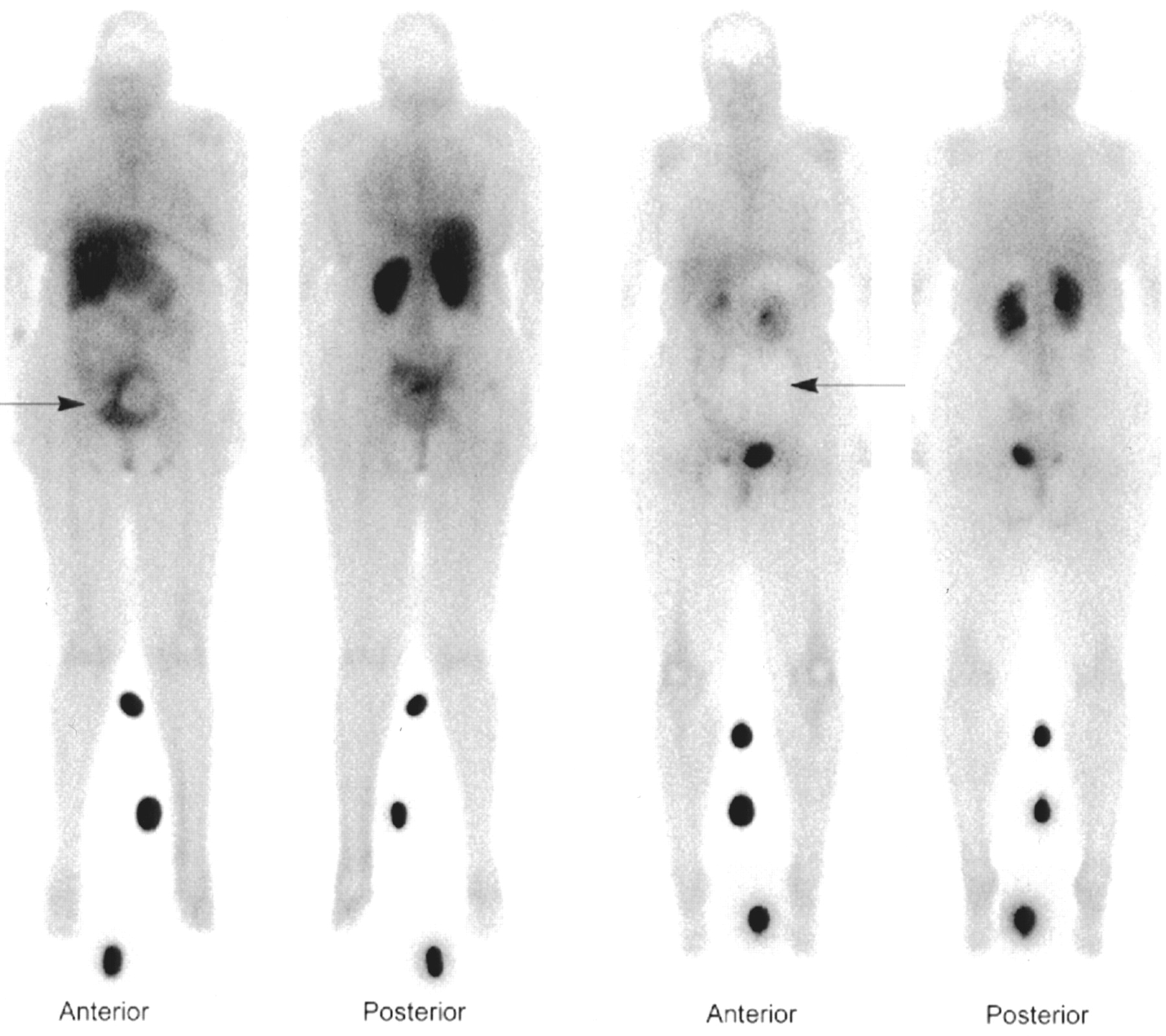
Anterior and posterior planar scintigrams obtained 4 h after administration of 111In-DTPA-folate. The 2 leftmost images, of patient 15, demonstrate increased tracer uptake (arrow) corresponding to solid tumor component in rim of poorly differentiated adenocarcinoma of left ovary. The 2 rightmost images, of patient 9, show region of focally decreased activity (arrow) corresponding to simple serous benign cyst. (Foci of increased activity between legs of each patient are reference sources used for dosimetry calculations.)
Patient Characterization and Image Scoring for Newly Detected Tumor Masses
Summary of 111In-DTPA-Folate Imaging Results from Patients Presenting with Newly Detected Abdominal Masses
Both readers scored all 7 malignant tumors as having increased uptake of 111In-DTPA-folate (sensitivity, 100%). The masked and unmasked interpretations of these studies were identical (Table 4). The 1 borderline-malignant tumor (patient 6) was scored as showing faint uptake by reader A on the masked and unmasked readings. Reader B scored the borderline-malignant tumor as showing no uptake on the masked reading and did not complete the unmasked reading.
Of the 18 benign masses, 11 were scored by both readers, on both masked and unmasked readings, as showing no uptake (Table 4). Two additional masses (patients 27 and 29) were scored as showing no uptake by one or both readers. One benign mass (patient 12) was scored by both readers as having definitely increased uptake of 111In-DTPA-folate on SPECT images, on both masked and unmasked analyses. This mass was classified pathologically as adenomatoid tumor/hilar Leydig cell hyperplasia. Another benign mass (patient 23) was scored consistently by both readers as showing faint uptake. Variable scoring was recorded on the remaining 3 benign masses. For patient 17, with a mature cystic teratoma, both readers scored the images as showing definitely increased uptake on the masked readings but as showing no uptake when the reading was unmasked. Only 2 benign masses were scored differently by the readers (patients 22 and 34; Table 3).
The specificities for the masked analysis of the 111In-DTPA-folate images were 78% and 75% for readers A and B, respectively (Table 4). For the unmasked readings, their corresponding specificities were 82% and 81%, respectively.
The agreement between the nuclear medicine physicians on the readings of newly diagnosed masses was excellent (92%), with all but 4 sets of images being scored identically, including both masked and unmasked readings (43/47 readings; 5 incomplete image sets excluded). The overall accuracies of 111In-DTPA-folate imaging for distinguishing malignant and benign lesions in patients with newly diagnosed ovarian masses, excluding the borderline malignancy, were 83% (40/48) and 89% (41/46) for masked and unmasked readings, respectively.
Recurrent Malignancies.
Seven patients with suspected recurrent ovarian or endometrial cancers were studied (Table 5), and subsequent pathologic examination showed all 7 to have recurrent malignant disease (5 ovarian and 2 endometrial). In the masked readings, only 2 of the malignancies were scored as showing increased uptake. The remaining 5 image sets were scored as showing no or faint uptake. When the readers were later unmasked, they scored 4 of the malignancies as showing increased uptake, 2 as showing slight uptake, and only 1 as showing no uptake. The average sensitivity values of both readers for recurrent ovarian and endometrial tumors were 38% and 85% for masked and unmasked analyses, respectively (Table 6). The agreement between the nuclear medicine physicians on the readings of recurrent ovarian and endometrial masses was quite high (92%), with all but 1 set of images having been scored identically, including both masked and unmasked readings (11/12 readings; 2 incomplete image sets excluded).
Patient Characterization and Image Scoring for Recurrent Malignancies
Summary of Results from Patients with Recurrent Ovarian and Endometrial Malignancies
One patient with recurrent ovarian cancer (patient 33) had a 4 × 6 cm mass seen on CT and shown by pathology to represent poorly differentiated adenocarcinoma. This patient’s 111In-DTPA-folate images were interpreted as negative. Of note, however, this patient was under treatment and, uniquely, was in the midst of a third cycle of chemotherapy at the time of the imaging study.
Another patient (patient 31) presented with a recurrent 2 × 3 cm mass adjacent to the spleen. This mass was not included in the field of view of the first SPECT study. The later SPECT study included the upper abdomen and was interpreted as showing definitely increased uptake on the unmasked readings.
DISCUSSION
The objectives of this study were to demonstrate the safety of 111In-DTPA-folate and to test the feasibility of selectively targeting human ovarian malignancy with a radiolabeled folate-chelate conjugate. In 1991, the folate receptor was confirmed to be a clinically valuable and specific marker for ovarian cancer (9). Subsequent to that finding, folate receptors have been shown to be overexpressed on the cell surfaces of several different types of human cancer (9,10,33,34). The folate receptor has been found to be expressed at very high levels in >90% of ovarian carcinomas and at high-to-moderate levels in some brain, lung, and breast carcinomas (10,11,35,36). Cancers of the endometrium, kidney, colon, and hematopoietic cells of myeloid lineage have also been found to frequently overexpress the folate receptor (9–12,33,37). The folate receptor gene was recently mapped to region 11q13, a chromosomal locus that is amplified in >20% of tissue samples from breast and head/neck tumors (38,39).
111In-DTPA-folate scintigraphy was evaluated in 2 types of patients: those with newly detected ovarian masses and those with suspected recurrent ovarian or endometrial cancer. Presurgical differentiation between benign and malignant lesions is critical to effective surgical management of patients with newly detected ovarian masses. Similarly, early detection of recurrent cancer is necessary for successful treatment. Recurrent ovarian cancer often presents as small foci that are difficult to detect by conventional imaging techniques. In addition, diagnosis of recurrent disease generally requires multiple CT scans, taken over several months, to detect evidence of tumor growth. A rapid and accurate diagnostic method that would allow for early detection of malignant lesions is clearly needed for improved surgical management of ovarian cancer (3).
The images obtained with 111In-DTPA-folate were read, both with and without masking, by 2 nuclear medicine physicians at each of the 3 clinical sites, and the readings were compared with surgical and pathologic findings. For newly detected ovarian masses, the sensitivity for detection of malignancy was 100% in this relatively small group of subjects. All malignant lesions showed definitely increased uptake of the radiotracer. One mass, determined by pathology to be a borderline malignancy (serous mass), was scored as showing faint uptake by one reader and no uptake by the other. Specificity was lower than sensitivity but was considered acceptable at approximately 80%. Images were scored as showing increased uptake, faint uptake, or no uptake. To minimize the risk of false-negative readings, faint uptake was considered positive for malignancy for purposes of estimating sensitivity and specificity.
One benign mass (patient 12) was incorrectly identified (false-positive) by both readers in both masked and unmasked readings. Pathologically, this lesion was diagnosed as adenomatoid tumor/hilar Leydig cell hyperplasia.
The sensitivity of 111In-DTPA-folate imaging in patients with recurrent or suspected recurrent ovarian or endometrial masses was considerably lower than the 100% for patients with newly diagnosed malignancies. The significant improvement in sensitivity in this patient subset with unmasked readings, from 38% to 85%, indicates that correlation with anatomic imaging studies (e.g., CT) is important in diagnosis of recurrent tumor. The poor sensitivity for unmasked readings was considered a result of the small size of the recurrent tumors, by comparison with newly diagnosed tumors, and the unpredictability of the location of recurrent tumors.
CONCLUSION
The overall observations from this initial clinical study with 111In-DTPA-folate are promising. The agent appeared to be safe and exhibited rapid target-tissue uptake and nontarget-tissue clearance, such that images obtained 4 h after injection could be scored with confidence. Interobserver agreement in image interpretation was high. Differentiation between benign and malignant masses was good in patients with suspected new disease, even when the 111In-DTPA-folate studies were read in the absence of other diagnostic imaging results that would normally be clinically available. Assessment of patients with recurrent ovarian and endometrial carcinomas was more difficult. Poor results were obtained with masked 111In-DTPA-folate image interpretation in patients with recurrent disease; however, the diagnostic accuracy was considerably improved by the ability to correlate 111In-DTPA-folate results with complementary findings from anatomic imaging studies. Our results indicate that 111In-DTPA-folate is safe, and possibly effective, for imaging of ovarian malignancy, perhaps allowing presurgical differentiation between malignant and benign ovarian masses. Further clinical evaluation of this and other folate-conjugated radiotracers may be appropriate.
Acknowledgments
The authors acknowledge the contributions of the staff at each of the 3 study sites and the supportive sponsorship of Endocyte, Inc., West Lafayette, IN. This study was partially supported by grants R43-CA73260 and R01-CA70845 from the National Cancer Institute.
Footnotes
Received May 8, 2002; revision accepted Jan. 13, 2003.
For correspondence or reprints contact: Barry A. Siegel, MD, Mallinckrodt Institute of Radiology, 510 S. Kingshighway Blvd., St. Louis, MO 63110.
E-mail: siegelB{at}mir.wustl.edu
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Identification of a PET Radiotracer for Imaging of the Folate Receptor-{alpha}: A Potential Tool to Select Patients for Targeted Tumor Therapy
- Molecular Imaging of Ovarian Cancer
- Development and Pre-clinical Evaluation of New 68Ga-NOTA-folate Conjugates for PET Imaging of Folate Receptor-positive Tumors
- Imaging the Folate Receptor on Cancer Cells with 99mTc-Etarfolatide: Properties, Clinical Use, and Future Potential of Folate Receptor Imaging
- A Folate Receptor-{alpha}-Specific Ligand That Targets Cancer Tissue and Not Sites of Inflammation
- Folic Acid Conjugates for Nuclear Imaging of Folate Receptor-Positive Cancer
- In Vivo Assay of Folate Receptors in Nonfunctional Pituitary Adenomas with 99mTc-Folate SPECT/CT
- A New 18F-Labeled Folic Acid Derivative with Improved Properties for the PET Imaging of Folate Receptor-Positive Tumors
- Pemetrexed Improves Tumor Selectivity of 111In-DTPA-Folate in Mice with Folate Receptor-Positive Ovarian Cancer
- SPECT Study of Folate Receptor-Positive Malignant and Normal Tissues in Mice Using a Novel 99mTc-Radiofolate
- In vivo quantitation of rare circulating tumor cells by multiphoton intravital flow cytometry
- Effects of Antifolate Drugs on the Cellular Uptake of Radiofolates In Vitro and In Vivo
- Synthesis and Preclinical Evaluation of a Folic Acid Derivative Labeled with 18F for PET Imaging of Folate Receptor-Positive Tumors