


Abstract
This study was undertaken to test whether the octapeptide of cholecystokinin (regular CCK-8) and pharmacy-compounded CCK-8 produce similar results with regard to gallbladder function. Methods: Twenty patients with suspected gallbladder disease were enrolled into quantitative cholescintigraphy. Each patient was infused for10 min with 3 ng/kg/min of regular CCK-8 and pharmacy-compounded CCK-8, sequentially, with a 30-min interval between the beginning of infusion. The gallbladder ejection fraction, latent period, ejection period, and ejection rate were measured with both agents. Results: Both regular CCK-8 and pharmacy-compounded CCK-8 produce similar, but not identical, results with close correlation between them with reference to all of the measured functions of the gallbladder. There is neither potentiation nor inhibition of the first dose on the effects of the second dose of CCK-8. Conclusion: Pharmacy-compounded CCK-8 functions much similar to that of regular CCK-8 as long as an interval of at least 30 min is allowed between doses.
- pharmacy-compounded octapeptide of cholecystokinin
- sincalide
- gallbladder ejection fraction
- chronic cholecystitis
Measurement of the gallbladder ejection fraction (GBEF) is a popular diagnostic technique in the evaluation of patients with varieties of hepatobiliary diseases, especially in those with biliary dyskinesia (1). A fatty meal or exogenous cholecystokinin (CCK) is used as the stimulus for induction of gallbladder (GB) emptying (2,3). The entire molecule of CCK-33 or its terminal 8-amino-acid fragment (CCK-8) can be chosen for GB stimulation. Usually, a 60-min duration of GB data collection with the fatty meal or a 30-min duration with intravenous administration of CCK-8 is necessary to generate valid results. Because a fatty meal produces a much greater variability in the GBEF than CCK-8, hormone is preferred (4). In the United States, sincalide (CCK-8) (Kinevac; Bracco Diagnostic, Inc., Princeton, NJ) is the only product approved by the Food and Drug Administration (FDA) for clinical use. In September 2001, the manufacturer sent a letters to all nuclear medicine physicians stating future nonavailability of sincalide because of its production difficulty. This has created a panic within the nuclear medicine community, resulting in either stockpiling of the available sincalide vials or reluctantly switching to fatty meal stimulation. Many state-based pharmacies now have come forward to supply the compounded product on prescription order written by a physician. Doubts have been expressed as to the potency and reliability of results obtained with the pharmacy-compounded CCK-8 (5). We undertook this project to compare GB function measured with the FDA-approved regular CCK-8, sincalide (hereafter referred to as RCCK-8), and the pharmacy-compounded new CCK-8 (hereafter referred to as NCCK-8) in a paired study. Such a comparison is necessary not only to establish the biologic potency of the pharmacy-compounded product, but also to test whether the results established previously with sincalide (RCCK-8) are directly transferable when an identical dose of the pharmacy-compounded NCCK-8 is used in clinical practice.
MATERIALS AND METHODS
Patients
Twenty-one patients were enrolled into the study. Each patient’s physician requested a hepatobiliary study. Because of a technical difficulty, data on 1 patient had to be excluded from analysis. The remaining 20 patients (14 women, 6 men) were 22–81 y old (mean, 51 y old) and weighed 60.9–105.5 kg (mean, 76.8 kg). Liver function tests were normal in 13, abnormal in 2 (bilirubin values of 2.8 mg and 2.1 mg%), and not obtained in the remaining 5 patients (Table 1). An ultrasound study on each patient showed a normal GB in 16, gallstones in 2, and polyps in 2. The purpose of the study was explained to the patients and their informed consent was obtained on a form approved by the hospital interprofessional committee (Institutional Review Board).
Comparison of RCCK-8 with NCCK-8 for Measurement of GB Function
Study Protocol
A standard technique was used to acquire and analyze the data (6). After an overnight fast or 6–10 h of fasting, each patient received 111–185 MBq (3–5 mCi) 99mTc-disofenin intravenously while lying supine underneath a large-field-of-view gamma camera fitted with a low-energy, all-purpose, and parallel-hole collimator. Hepatic-phase images were obtained at 1-min intervals for 60 min and recorded on a 128 × 128 × 16 computer matrix. GB-phase images were obtained at 1-min intervals for an additional 60 min, for a total duration of study of 120 min. During the GB phase, RCCK-8 and NCCK-8 were infused sequentially, each at a dose rate of 3 ng/kg/min for 10 min (Fig. 1). Infusion of RCCK-8 was begun first in 10 patients, followed by infusion of NCCK-8. In the other 10 patients, infusion of NCCK-8 was begun first, followed by infusion of RCCK-8. The first infusion was begun at 63 min (CCK-1) and the second infusion was begun at 93 min (CCK-2) after injection of the radiotracer. An individual NCCK-8 vial was obtained from a pharmacy in Eugene, Oregon, which received its supply from Oregon Central Pharmacy (Professional Compounding Centers of America, Houston, TX). Both CCK-8 doses were infused through an infusion pump (Medfusion; Medex Inc., Duluth, GA). To facilitate easy calculation with the custom-designed hepatobiliary software, each 30 min of GB data was acquired separately on the computer. Patients were instructed to inform the technologist of any reaction or symptoms (pain, nausea, gas, and so forth) experienced during each 30 min of GB-phase imaging.
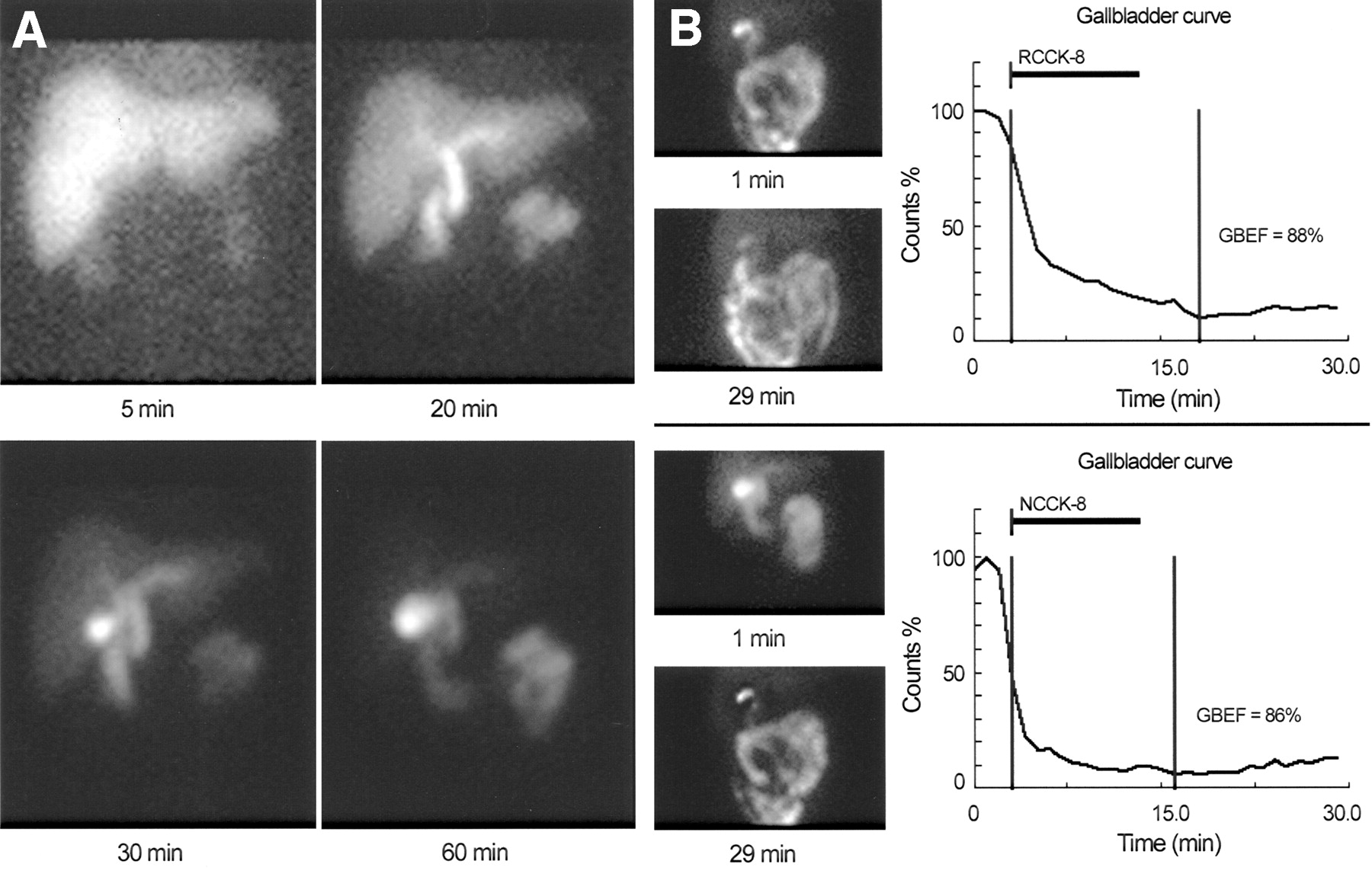
Hepatic-phase (A) and GB-phase (B) images show normal filling and emptying, respectively. Note that GB empties to same extent with identical dose of RCCK-8 (GBEF = 88%) and NCCK-8 (GBEF = 86%). Software automatically adjusts length of solid bar below CCK-8 to match duration of its infusion.
Data Analysis
Both hepatic-phase and GB-phase counts were decay corrected, and functional parameters were measured using custom-designed semiautomatic hepatobiliary software (Fig. 1). From the hepatic-phase data, hepatic extraction fraction, excretion half-time, and differential hepatic bile flow into the GB versus the small intestine were calculated. From the GB-phase data, GBEF, latent period ([LP] time from beginning of infusion to onset of GB emptying), ejection period ([EP] time from beginning to end of GB emptying), and ejection rate ([ER] % GBEF/EP) were calculated for each dose of CCK-8 as described (6). The maximum counts just before and the first minimum counts immediately after each CCK-8 infusion were used to calculate the GBEF, LP, EP, and ER for each dose of the hormone. A GBEF value of ≥50% was considered as normal. The mean values with RCCK-8 and NCCK-8 were tested by a paired t test, and with P < 0.05 considered significant.
RESULTS
GB Functional Parameters
Hepatic-phase images showed a normal pattern of bile formation and flow in all 20 patients. Seven patients (32%) had a normal GBEF (>50%) with both RCCK-8 and NCCK-8. Because the study included patients with varied severity of GB disease, individual GBEF values ranged from 2% to 92%. The mean (±SD) GBEF value was 41% ± 31% with regular CCK-8 and 46% ± 38% with pharmacy-compounded CCK-8 (Fig. 2). The mean LP, EP, and ER were 2 ± 2 min, 17 ± 5 min, and 3%/min ± 3%/min with RCCK-8, respectively. Corresponding values with NCCK-8 were 2 ± 2 min, 16 ± 6 min, and 3%/min ± 3%/min (Table 1). None of the corresponding mean values was significantly different (P > 0.05) between NCCK-8 and RCCK-8. The correlation coefficients between the 2 agents were 0.85 for GBEF, 0.69 for EP, and 0.91 for ER. Three of the patients with GBEF values lower than normal (<50%) with RCCK-8 had normal GBEF values (>50%) with NCCK-8. In these 3 patients, the GBEF value was lower than the normal value of 50% by 5%, 13%, and 20% (Figs. 2 and 3, upper left quadrant). There were no allergic reactions attributable to either RCCK-8 or NCCK-8 preparation.
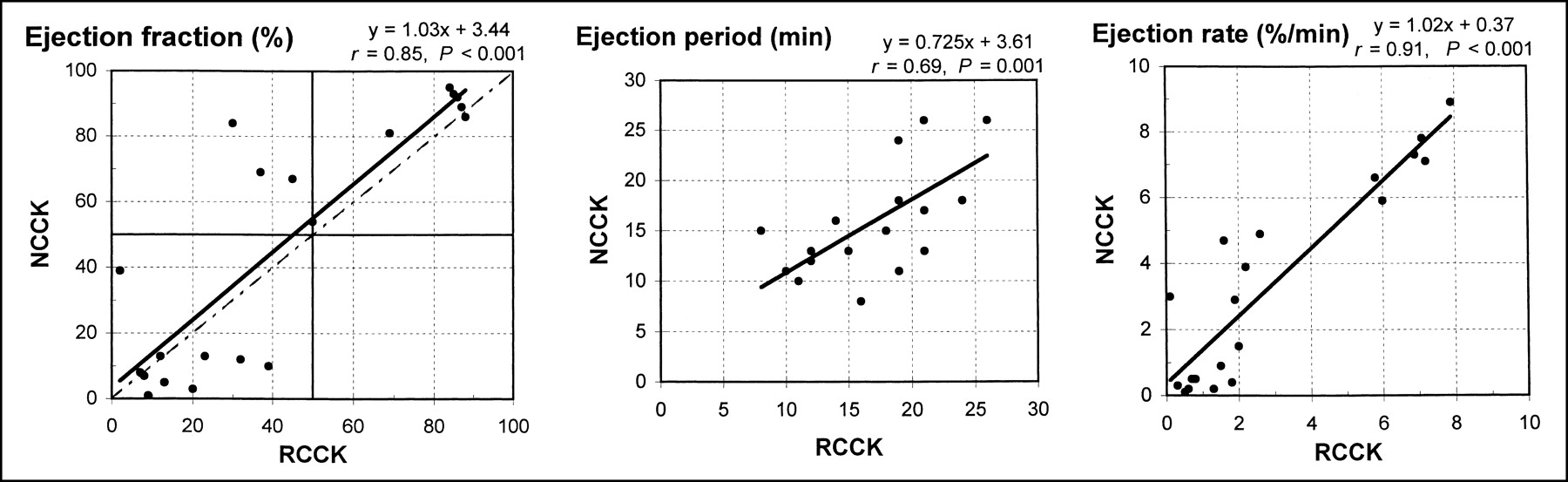
Correlation of GBEF (r = 0.85), EP (r = 0.69), and ER (r = 0.91) obtained with 10-min infusion of 3 ng/kg/min of either RCCK-8 or NCCK-8. Regression line (solid line) and line of identity (broken line) are shown. GBEF value of ≥50% is considered normal. In ejection fraction plot, lower left and upper right quadrants show concordant GBEF with both doses; in same plot, upper left quadrant shows 3 patients with discordant results, where GBEF value was >50% with NCCK-8 but <50% with RCCK-8.
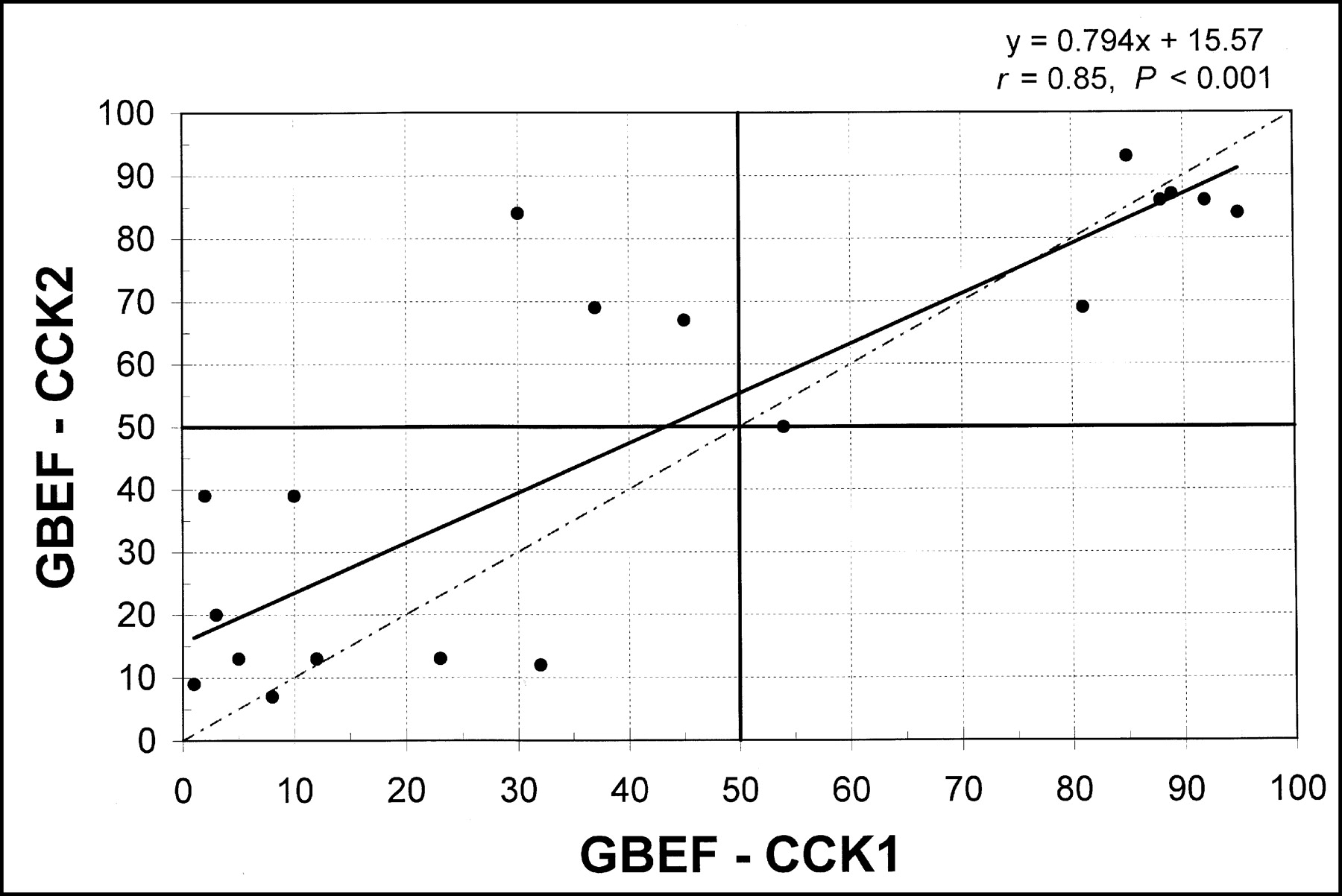
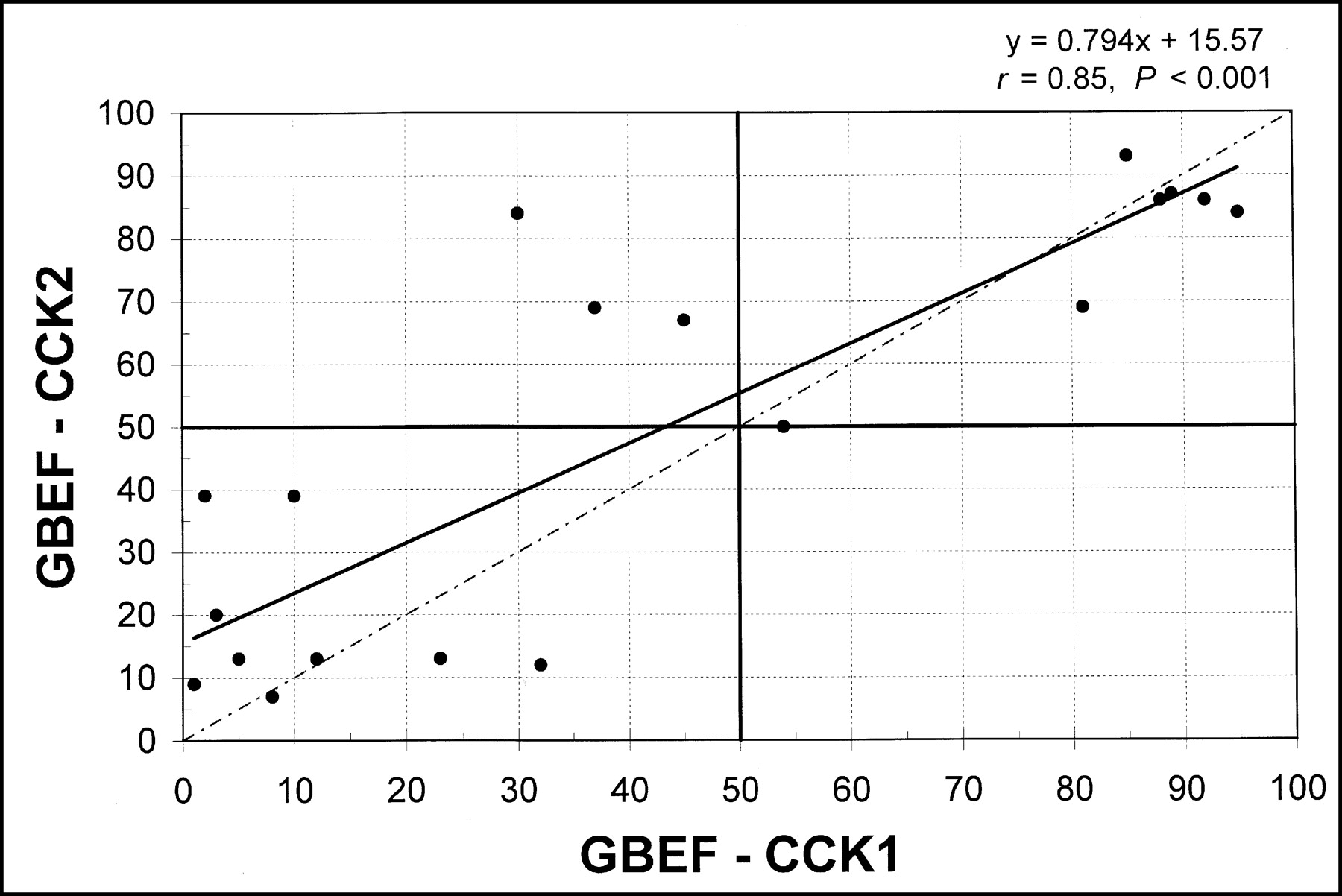
Correlation of GBEF obtained with 2 sequential doses of CCK-8 (CCK-1 and CCK-2). Regression line (solid line) and line of identity (broken line) are shown. Note close correlation (r = 0.85) between 2 doses.
Influence of First Dose on Results of Second Dose of CCK-8
There was no significant difference between the 2 mean values obtained with CCK-1 and CCK-2 (Table 1). To test whether administration of the first dose of CCK-8 either potentiated or inhibited the effect of the second CCK-8 dose, the GBEF values for CCK-1 were plotted on the x-axis and the corresponding values for CCK-2 were plotted on the y-axis in Figure 3. Most of the values were distributed along the line of identity and showed good correlation between CCK-1 and CCK-2 (r = 0.85).
DISCUSSION
CCK consists of 33–39 amino acids in its molecule, which can be cleaved at many different locations resulting in fragments of 4, 8,12, or 18 amino acids. The fragment that connects with the C-terminal tetrapeptide retains most of the biologic activity of the parent molecule (1). An octapeptide of CCK (sincalide) was first synthesized and its dosage established in 1973 using oral cholecystography (7). Originally, the agent was approved by the FDA for use with oral cholecystography and for induction of pancreatic enzyme secretion. The package insert for Kinevac (8) recommends a dosage of 0.02 μg (20 ng) or 0.04 μg (40 ng) per kilogram, given intravenously in 30–60 s. This dose rate was found to be too high for cholescintigraphy. A dose-escalation study using quantitative cholescintigraphy showed the GB peak emptying response at 0.01 μg/kg (10 ng/kg) infused slowly over 3 min (3.3 ng/ kg/min). A dose rate higher than this produced abdominal pain and a lower ejection fraction in healthy subjects (9). Because a longer duration of CCK-8 infusion may simulate a fatty meal, some prefer continuous infusion for 30, 45, or 60 min (10,11).
Our results show that both regular CCK-8 (sincalide) and pharmacy-compounded CCK-8 are biologically potent and produce a similar, but not identical, degree of emptying when an identical total dose of the hormone is infused. Comparison of GB functional parameters obtained with regular CCK-8 and pharmacy-compounded CCK-8 show close correlation with reference to LP, EP, GBEF, and ER. The slight difference in response between the 2 agents is probably due to variation in biologic response of the GB and not due to any potency difference between the 2 agents, because such variations do occur even when the same agent is administered twice, sequentially (4).
The serum half-life of CCK is 2.5 min (6). Exogenous hormone, therefore, clears from blood quite rapidly and reaches basal levels within 20–25 min after cessation of its infusion. Our results show that the GB empties as long as the serum CCK-8 level is maintained above the threshold for its contraction and stops emptying when the serum level falls below the threshold (Fig. 1). Emptying is resumed with reinfusion of the hormone. The first 3-min counts obtained before beginning the CCK-8 infusion establish the basal volume of the GB. As the serum CCK-8 level rises with the onset of infusion, the GB begins to empty, usually within 2 min (LP). The GB begins to empty almost immediately, but the computer recognizes the minimum LP as 1 min because the data were acquired at an interval of 1 frame per minute. The mean EP of 16 min with RCCK-8 and 17 min with NCCK-8 indicates that the GB continues to empty bile throughout the duration of infusion plus an additional 6–7 min after cessation of the CCK-8 infusion. In patients with spasm of the sphincter of Oddi, CCK-induced paradoxical filling of the GB occurs usually at the end of the EP (between 15 and 30 min). Therefore, it is necessary to collect GB data for an additional 15–20 min after cessation of the CCK-8 infusion to be able to detect spasm of the sphincter of Oddi (1,6).
The sequential-dose CCK-8 technique enables measurement of the GBEF as many times as one desires with a single dose of 99mTc-labeled hepatic iminodiacetic acid. The GB empties to the same extent each time when 2 or 4 identical doses of CCK-8 are administered sequentially (12,13). Because the serum half-life is only 2.5 min, the CCK-8 level falls off rapidly below the threshold for contraction, and the first dose does not seem to leave significant residual in serum to influence the results of the subsequent doses, as long as 30 min are allowed between doses (Fig. 1). Therefore, it should be possible to study the effects of graded doses of the same hormone (dose-escalation study) or the effects of drugs on the GB or sphincter of Oddi using the sequential-dose CCK-8 technique.
Over the years, we have infused 3.3 ng/kg/min of CCK-8 for 3 min and considered the lower limit of normal range to be 35% ejection fraction. Many investigators have published excellent results with cholecystectomy performed on the basis of the GBEF obtained with a 3-min infusion (14–16). For this study, we chose a CCK-8 dose rate of 3 ng/kg/min and a 10-min duration of infusion. The dose rate of 3 ng/ kg/min is very close to the peak physiologic rate of 3.3 ng/kg/min (9). The 10-min duration is a compromise between the 3-min and the 30-, 45-, or 60-min infusion. A 10-min infusion does not prolong the total duration of GB data collection beyond 30 min.
A normal GB shows a linear, not a gaussian, type of response to CCK-8 infusion (4,10,11). Therefore, a lower cutoff limit value has to be chosen arbitrarily instead of using a traditional mean ± 2 SD. We have shown recently that a GBEF value of 50% may represent a lower limit of the normal value with a 10-min infusion of regular CCK-8 at a dose rate of 3 ng/kg/min (4). Our goal in this project was to compare the results obtained with regular CCK-8 with those obtained with pharmacy-compounded CCK-8 in patients with suspected GB disease. In those patients with a GBEF value of >50%, normalcy may be assumed. Seven of 20 patients in our study had a normal GBEF with both agents. Three patients showed ≥50% GBEF with 1 agent but not with the other (Figs. 2 and 3, left upper quadrant). All 3 patients had a GBEF value of ≥50% with pharmacy-compounded CCK-8 and <50% with regular CCK-8. In all 3 patients, the normal range of 50% was missed by a narrow margin of 5%, 13%, and 20%.
Many state pharmacies have come forward to fill the unexpected gap created by the nonavailability of regular CCK-8 and have contributed greatly toward the betterment of patient welfare by supplying compounded CCK-8 in a timely manner. The total quantity of pharmacy-compounded CCK-8 required with a 10-min infusion is >3 times the amount required with a 3-min infusion, but the total cost of the individual dose has remained approximately the same. Competition among many compounding pharmacies around the country is likely to reduce the price further. Because pharmacy-compounded CCK-8 is not approved by the FDA for routine use, patients are informed and their signature is obtained on a consent form approved by the hospital Institutional Review Board. Because sincalide (regular CCK-8) is also not approved by the FDA for cholescintigraphy, informing the patients and obtaining their consent is just as applicable for sincalide as it is for the pharmacy-compounded CCK-8. Obtaining an informed consent is quite simple and is similar to getting a patient’s signature for a treadmill test or adenosine infusion for nuclear cardiology studies. Because both agents show comparable biologic potency and results, selection of 1 agent over the other for routine clinical studies should be based on the cost and timely availability.
CONCLUSION
Pharmacy-compounded CCK-8 and regular CCK-8 (sincalide) function in a like manner and 1 agent can substitute for the other for routine clinical studies during cholescintigraphy.
Acknowledgments
We thank Dr. Paul H. Brown (Department of Radiology, Oregon Health and Sciences University, Portland, OR) for providing statistical analysis and Figures 2 and 3 and Bob Crummett (Tuality Community Hospital/Tuality Healthcare, Hillsboro, OR) for preparing Figure 1.
Footnotes
Received Sep. 3, 2002; revision accepted Nov. 27, 2002.
For correspondence or reprints contact: Gerbail T. Krishnamurthy, MD, Nuclear Medicine Department, Tuality Community Hospital, 335 S.E. 8th Ave., Hillsboro, OR 97123.
E-mail: gtkrishna{at}aol.com
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Hepatobiliary Scintigraphy in 2014
- Hepatobiliary Scintigraphy in 2014
- Reply: Sincalide-Stimulated Cholescintigraphy: What Is the Standard?
- Corn Oil Emulsion: A Simple Cholecystagogue for Diagnosis of Chronic Acalculous Cholecystitis
- Constancy and Variability of Gallbladder Ejection Fraction: Impact on Diagnosis and Therapy
- Measurement of Gallbladder Ejection Fraction