


Abstract
Small-vessel disease with dementia, which is the most frequent type of vascular dementia (VaD), often shows a cerebral blood flow (CBF) distribution with no obvious focal abnormalities and is therefore difficult to evaluate objectively. In this study, we combined CBF SPECT with 3-dimensional fractal analysis (3D-FA) to quantitatively assess the heterogeneity of CBF distribution and with 3-dimensional stereotactic surface projections (3D-SSP) to evaluate the distribution of CBF. We then evaluated the clinical validity of these techniques for the imaging diagnosis of VaD. Methods: The subjects consisted of 17 patients who were diagnosed as having VaD due to small-vessel disease (VaD group) on the basis of a full clinical examination, including history, neuropsychologic tests, neurologic examination, and neuroimaging methods, and 20 healthy volunteers (control group). CBF SPECT was performed with 99mTc-hexamethylpropyleneamine oxime, and the reconstructed images were subjected to image processing by 3D-FA and 3D-SSP. Based on the results, the fractal dimension (FD) was compared between the VaD and control groups, and the distribution pattern of CBF was examined in the VaD group. Results: The mean FD values in the VaD group and the control group were 1.093 ± 0.153 and 0.853 ± 0.062 (mean ± SD), respectively. The mean FD value in the VaD group was significantly higher than that in the control group (P < 0.0001). 3D-SSP analysis in the VaD group showed that there were 2 abnormal patterns: One was globally reduced blood flow in the whole cerebral cortex, and the other was a reduction mainly confined to the frontal region. Conclusion: CBF SPECT images showed higher mean FD values in the VaD group than in the control group, suggesting a difference in the heterogeneity of CBF. Image processing with 3D-SSP successfully revealed that reduced cortical blood flow could be divided into 2 patterns. Because image analysis techniques, such as 3D-FA and 3D-SSP, allowed the simple and objective evaluation of CBF in patients with VaD, these methods seem to be useful for detailed examination of the blood flow pattern detected by CBF SPECT in patients with VaD.
- vascular dementia
- cerebral blood flow
- fractal analysis
- 3-dimensional stereotactic surface projections
- SPECT
Three-dimensional assessment of cerebral blood flow (CBF) abnormality can easily be performed in daily clinical practice with SPECT, allowing us to detect the lesion of reduced CBF corresponding to the neurologic symptoms in patients with dementia before any morphologic changes are observed on CT or MRI.
Cerebral functional imaging studies of patients with vascular dementia (VaD) have revealed various findings, including patchy reduction of CBF without any specific pattern (1) or reduction of CBF in the frontal lobes (2–4). CBF abnormalities are relatively easy to detect with CBF SPECT in the case of VaD due to large cortical infarcts. But VaD is difficult to diagnose, as no diagnostic scheme has both high sensitivity and high specificity. For example, the National Institute of Neurological Disorders and Stroke-Association International pour la Recherse et l’Enseignement en Neuroscience (NINDS-AIREN) criteria (5) have been reported to have only 58% sensitivity and Hachinski’s ischemic score (6) has been reported to have only 43% sensitivity with respect to pathologic diagnosis (7). VaD has also been classified into several subtypes. Among these subtypes, small-vessel disease with dementia is the most common VaD (8,9). The patients classified in the group having small-vessel disease with dementia often show no apparent focal abnormalities on CBF SPECT images. Although detecting reduced blood flow or metabolism in the cerebral cortex is important for making an early diagnosis, one cannot always detect such a reduction with visual evaluation alone. To solve this problem, more objective indices have been introduced, such as quantification of CBF with arterial blood collection (10) and the accumulation ratio relative to the cerebellum. One study (11) showed the usefulness of semiquantitative SPECT in the diagnosis of dementia. However, it is generally difficult to quantify CBF with arterial blood collection in clinical practice because this method is invasive and requires many personnel and a long test time. The conventional region-of-interest analysis has various problems, such as acquisition of information only in the region of interest, difficulty in locating the lesion, poor reproducibility, and too much subjectivity. The recent introduction of statistical techniques for the analysis of cerebral functional images has revealed the possibility of detecting changes that are missed by conventional region-of-interest analysis. Minoshima et al. (12,13) have developed 3-dimensional stereotactic surface projections (3D-SSP) to map the lesions with reduced CBF in a statistical manner. However, the method is not totally free from visual inspection. Three-dimensional fractal analysis (3D-FA) is a new technique to measure the heterogeneity of CBF in a mathematic manner. In this study, we applied 3D-FA to the CBF SPECT images of patients with VaD due to small-vessel disease, which was difficult to diagnose by visual analysis. We also evaluated the spatial distribution of lesions with abnormal CBF using 3D-SSP.
MATERIALS AND METHODS
Subjects
The subjects consisted of 17 patients with VaD (6 men and 11 women; VaD group) and 20 healthy volunteers (9 men and 11 women; control group). The clinical characteristics of the subjects are shown in Table 1. They were all right-handed and underwent CBF SPECT between June 2000 and February 2002. The NINDS-AIREN criteria (5), the Diagnostic and Statistical Manual of Mental Disorders (14), Hachinski’s ischemic score (6), and Erkinjuntti’s criteria (15) were used for making the diagnosis of VaD to ensure comprehensive examination. The clinical features for VaD included sudden onset, stepwise progression, prolonged plateaus, periods of spontaneous improvement, and onset or worsening in relation to stroke or episode of hypoperfusion. The soft, focal neurologic signs or symptoms strongly supported the diagnosis of VaD. VaD subtype classifications were based on results of neuroimaging and clinical evaluation (15). Probable VaD was diagnosed in all 17 patients, and all were classified into the group having small-vessel disease with dementia because MRI showed small infarcts with a diameter of 3–15 mm in the basal ganglia, thalamus, pons, and deep white matter (seen as low-intensity areas on T1-weighted images and high-intensity areas on T2-weighted images), whereas there were no obvious lesions in the cortex. The 20 healthy volunteers underwent CBF SPECT for examination of vertigo or headache but had no abnormal CT or MRI findings and no evident neuropsychologic abnormalities on the basis of a full clinical examination, including history, neuropsychologic tests, and neurologic examination. The Mini-Mental State Examination (MMSE) (16) was performed within 3 mo of CBF SPECT to evaluate the cognitive function of the subjects.
Clinical Characteristics of Control Group and VaD Group
In the preliminary study, we compared the heterogeneity between CBF SPECT images with 99mTc-hexamethylpropyleneamine oxime (HMPAO) and PET images with 18F-FDG in another group, which consisted of 17 patients (13 men and 4 women with a mean age of 56.9 ± 14.6 y) who visited our hospital for investigation of memory impairment. 18F-FDG PET has been used for imaging the demented state, in which there is a greater reduction of glucose metabolism than of blood flow. Images obtained by both 99mTc-HMPAO CBF SPECT and 18F-FDG PET performed at approximately the same time (average interval, 7 d) were processed by 3D-FA to calculate the fractal dimension (FD). Informed consent was obtained from the subjects or from their families when they could not fully understand the nature and importance of the test.
Data Acquisition
99mTc-HMPAO was created by reconstituting HMPAO with 740 MBq (20 mCi) of fresh 99mTc-pertechnetate. 99mTc-HMPAO was injected intravenously while the subject rested supine on the scanning bed with the eyes closed in a quiet examination room. SPECT was done with a 4-head gamma camera (GAMMA VIEW SPECT 2000H; Hitachi Medical Corp., Tokyo, Japan), using a low-energy high-resolution parallel-hole collimator (17). The in-plane and axial resolution after reconstruction was 10.0 mm in full width at half maximum. SPECT acquisition was done at 8 s per step, with 128 collections over 360°, and data were recorded in a 64 × 64 matrix.
The raw SPECT data were transferred to a nuclear medicine computer (HARP 3; Hitachi Medical Corp.). The data were prefiltered with a Butterworth filter (cutoff frequency, 0.20 cycles per pixel; order, 10) and reconstructed into transaxial sections of 4.0-mm-thick images in planes parallel to the orbitomeatal line. Chang’s attenuation correction was applied to the reconstructed images using an attenuation coefficient of 0.08 cm−1.
PET was performed using a HEADTOME-V scanner (Shimadzu Corp., Kyoto, Japan) with a spatial resolution of 4.0 mm in full width at half maximum. The subjects rested supine on the scanning bed with the eyes closed in a quiet examination room. An individual transmission scan with a 68Ge/68Ga line source was obtained for each patient and used for subsequent attenuation correction of emission scan data. 18F-FDG (370 MBq) was injected intravenously, and after 45 min, data were acquired over a scanning period of 20 min using a 128 × 128 matrix. The final slice thickness was 3.125 mm.
3D-FA
In this study, fractal analysis was used to assess the heterogeneity of SPECT images. Fractal geometry allows structures to be quantitatively characterized in geometric terms even if their form is irregular and fragmented, because fractal geometry deals with the geometry of hierarchies and random processes. This type of analysis is most useful for characterizing branching structures, such as the pulmonary airways and blood vessels (18,19). Spatial changes of regional blood flow and metabolism in living organs are measurable using fractal analysis with PET and SPECT (20–23). Studies have shown that the observed variance increases along with the number of subregions studied in an organ (20) and that such resolution-dependent variance can be described by fractal analysis (20,23,24). Studies have also shown that biologic systems display considerable spatial and temporal heterogeneity, such as heterogeneity in CBF, myocardial blood flow, and pulmonary blood flow (24–28).
In fractal geometry, the relationship between a measure (M) and the scale (a) is expressed as:
 Eq. 1 where k is a scaling constant and D is called the FD (18).
Eq. 1 where k is a scaling constant and D is called the FD (18).
The cutoff value for the maximum radioactivity was set at 11 levels from 35% to 50% at equal intervals on the reconstructed images, and the number of voxels with a radioactivity exceeding the cutoff value was calculated in each case. The cutoff value of the maximal radioactivity was defined as a and the total number of voxels measured was defined as M (a), as shown in Equation 1. Then, the number of voxels and the cutoff value were transformed into natural logarithms and their relationship was graphed. The graph was drawn with the logarithm of the cutoff value on the horizontal axis and that of the number of voxels with a radioactivity above the cutoff on the vertical axis. The slope of the regression line on this graph corresponded to the FD.
3D-SSP
3D-SSP created with the Neurological Statistical Image Analysis Software (NEUROSTAT) developed by Minoshima et al. (12,13) from the University of Washington were used to evaluate the spatial distribution of abnormal CBF. One study on cerebral glucose metabolism measured by PET showed that metabolism was reduced in the posterior part of the cingulate gyrus before changes were detected at other sites in patients with very early Alzheimer’s disease (AD) (29). These changes at various sites have come to be detected more easily and objectively with 3D-SSP. NEUROSTAT anatomically normalizes the individual SPECT data to the standard brain and compares the regional voxel data with the normal SPECT database, calculating the z score ([normal mean − individual value]/normal SD) for each voxel of the cerebral surface, and displays the sites at which voxel value is statistically reduced. For anatomic standardization, a reference line (the line connecting the anterior commissure and posterior commissure) was detected and was transferred to the coordinate system of the standard brain according to the Talairach-Tournoux atlas (30). The individual image was then transformed to fit the standard brain through linear and nonlinear transformation. 3D-SSP extracts 3-dimensional functional information from the gray matter using pixels preset to cover the whole brain surface after the brain image of each subject is transformed to the standard brain image through anatomic standardization. Normalization was performed by whole-brain counting.
Statistical Analysis
The significance of differences in the FD value between the control group and the VaD group was assessed by the Mann-Whitney test. Correlations between CBF SPECT and 18F-FDG PET images were determined by calculating Spearman rank correlation. Results were expressed as mean ± SD, and statistical significance was defined as P < 0.01.
RESULTS
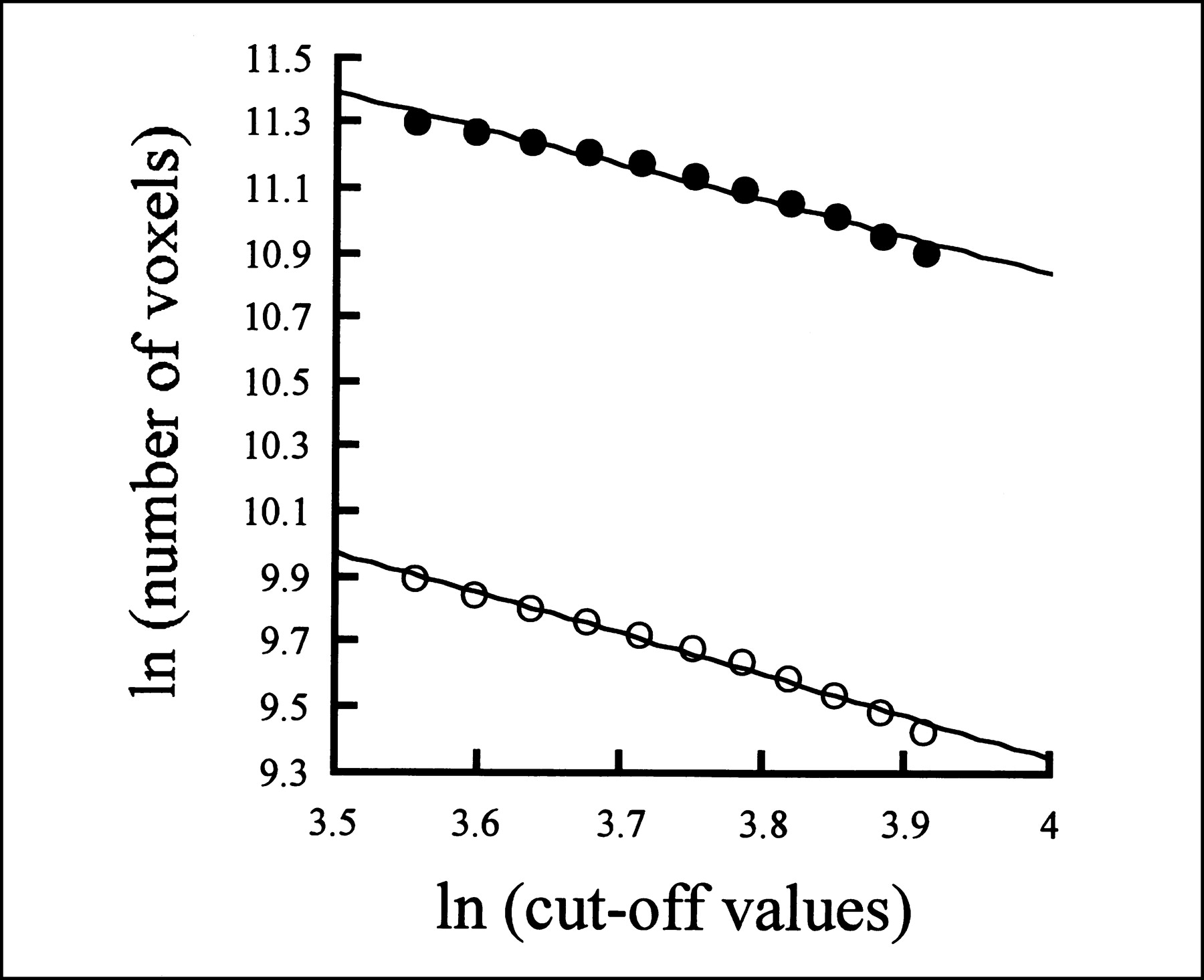
The age and sex ratios did not significantly differ between the VaD group and the control group, though the control group consisted of younger subjects than did the VaD group. The MMSE score of the VaD group was 18.6 ± 4.5 (mean ± SD), which was significantly lower than the score of 26.5 ± 2.6 found for the control group. Figure 1 shows a 62-y-old woman who underwent examination for memory impairment. Fractal analysis was performed on her CBF SPECT and 18F-FDG PET images, and the FD value was determined to be 1.109 for the 18F-FDG PET image and 1.278 for the CBF SPECT image. Although the number of voxels with a count exceeding a specific threshold differed between the 2 images, the lines corresponding to the FD were parallel and had almost the same gradient. When we compared FD data between 99mTc-HMPAO CBF SPECT and 18F-FDG PET images (Fig. 2), a significant correlation was shown by Spearman rank correlation analysis (r = 0.619; P < 0.01), suggesting that 99mTc-HMPAO CBF SPECT images may show similar heterogeneity to 18F-FDG PET images.

Comparison of FD calculated for 99mTc-HMPAO CBF SPECT image and FD calculated for 18F-FDG PET image of 62-y-old woman who underwent examination for memory impairment. Horizontal axis shows natural logarithm of cutoff values, and vertical axis shows natural logarithm of number of voxels in area surrounded by contour obtained with radioactivity above cutoff value. Slope of regression line on this graph corresponds to FD. • = FD value for 18F-FDG PET image (y = −1.109x + 15.29; r = 0.988); ○ = FD value for 99mTc-HMPAO CBF SPECT image (y = −1.278x + 14.46; r = 0.995).
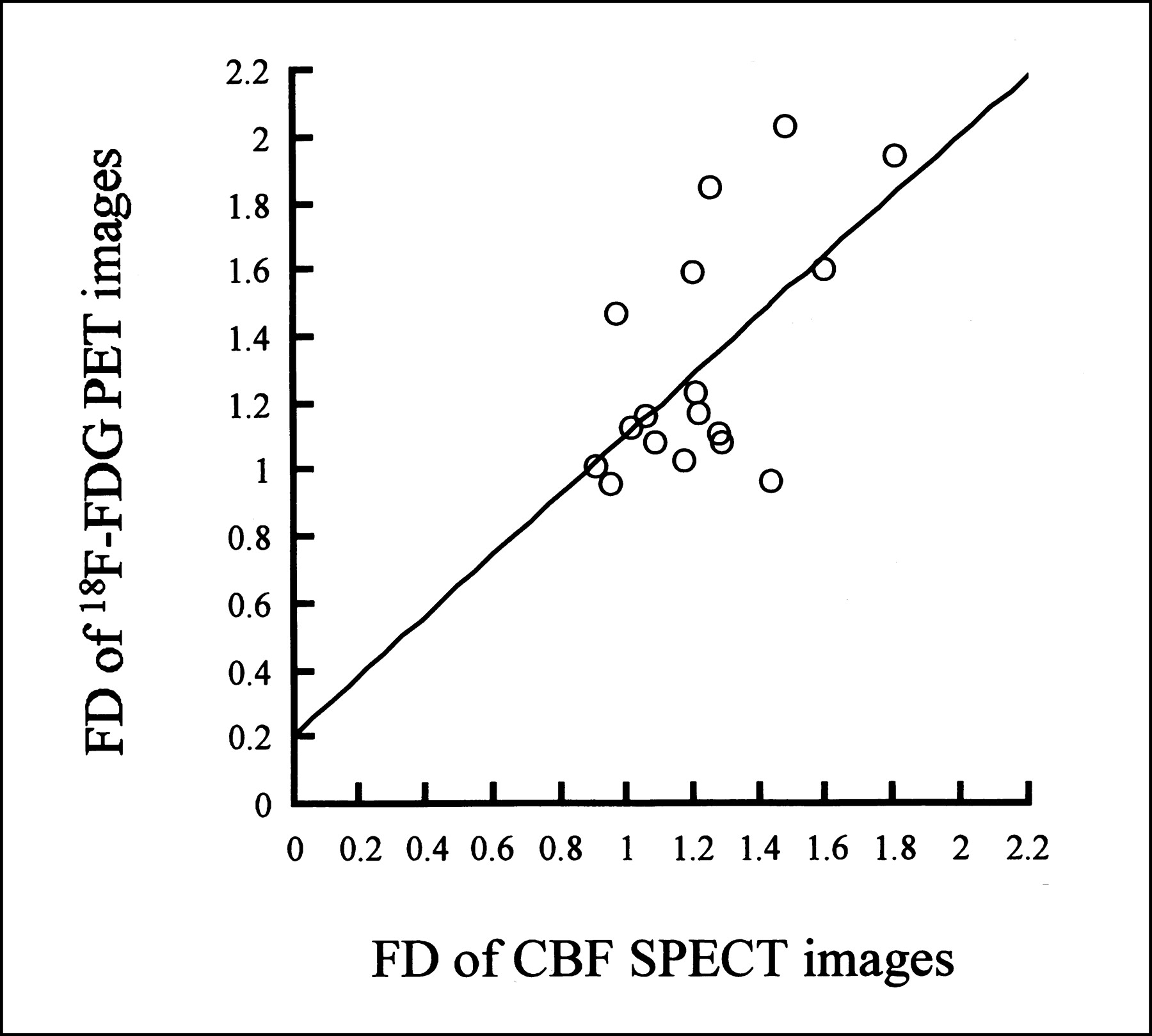
Scatter plots of FD data between 99mTc-HMPAO CBF SPECT and 18F-FDG PET images in VaD group. Spearman rank correlation analysis showed significant correlation between FDs of the 2 images (y = 0.902x + 0.211; r = 0.619; P < 0.01).
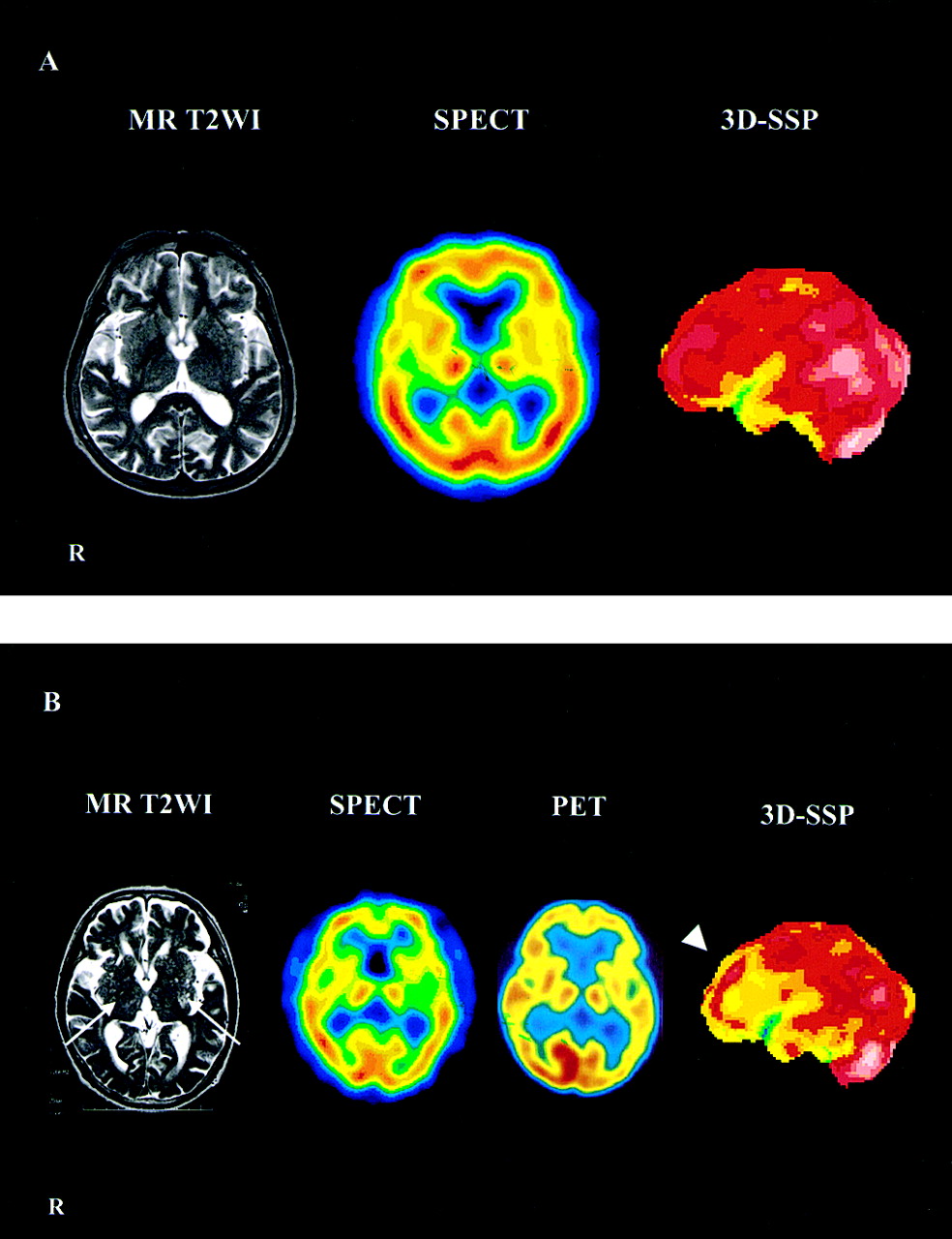
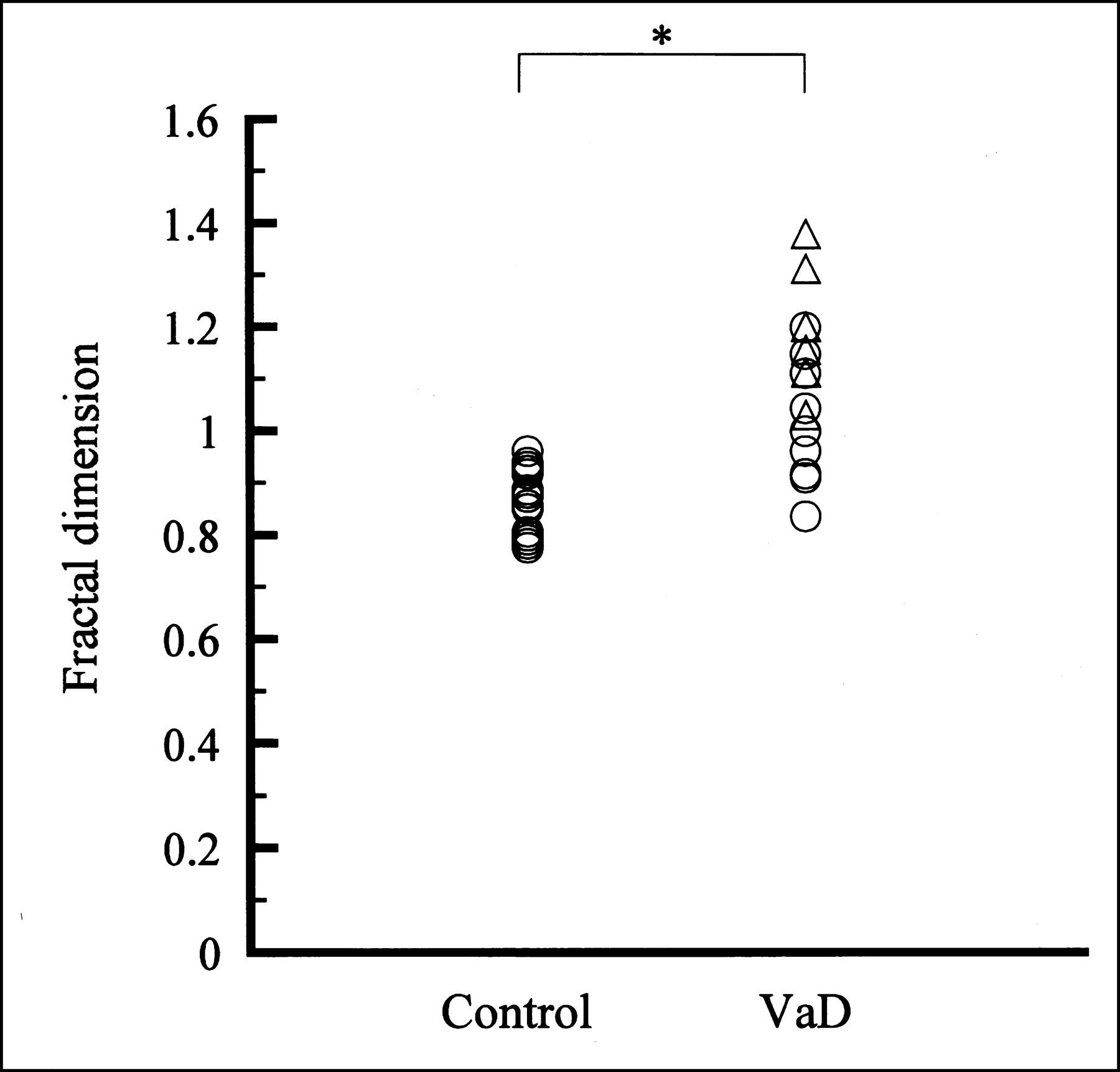
Figure 3 shows T2-weighted MR images, SPECT images, and 3D-SSP images of representative subjects from the control and VaD groups. The VaD patient has multiple small, bilateral infarcts in the basal ganglia on the T2-weighted MR image, diffuse reduction of CBF on the SPECT and PET images, and a reduction mainly confined to the frontal region on the 3D-SSP image. Figure 4 compares FD data between the VaD and control groups. The mean FD values of the VaD and control groups were 1.093 ± 0.153 and 0.853 ± 0.062, respectively, showing a significant difference between the 2 groups (P < 0.0001). In addition, the VaD group was divided into 2 groups based on an MMSE score of 20, and we then compared the mean FD values among the control group, the VaD group with a mild MMSE score decline (MMSE ≥ 20, n = 10), and the VaD group with a moderate to severe MMSE score decline (MMSE < 20, n = 7) (Fig. 4). When divided at the FD value of 0.977 (mean + 2 SDs in the control group), the control group and the VaD group with a moderate to severe MMSE score decline (MMSE < 20) could be clearly separated.

T2-weighted MR images (left), SPECT or PET images (center), and 3D-SSP images (right) of representative subjects from control and VaD groups. (A) Images of 70-y-old man from control group. His FD was 0.799, and his MMSE score was 29. (B) Images of 75-y-old man from VaD group. His FD was 1.151, and his MMSE score was 15. In VaD, T2-weighted MR images revealed multiple small, bilateral infarcts in basal ganglia (arrows), SPECT and PET images showed diffuse decrease in CBF, and 3D-SSP image showed reduction mainly confined to frontal region (arrowhead). T2WI = T2-weighted image.
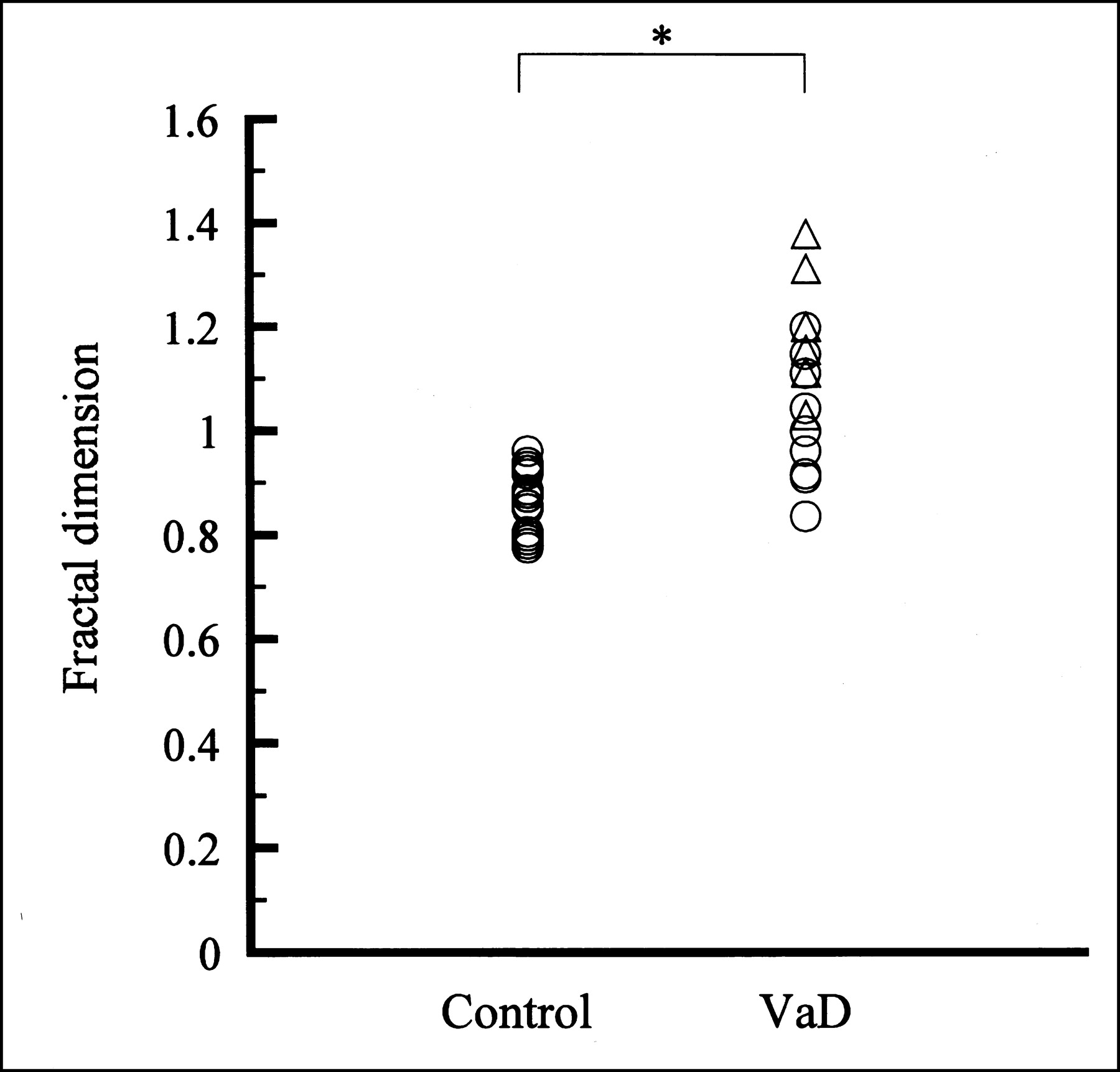
Comparison of FD between control group (n = 20) and VaD group (n = 17). Mann-Whitney test showed significant difference in FD between the 2 groups (P < 0.0001). ▵ = 7 patients with VaD at MMSE score of less than 20. *P < 0.0001.
Table 2 lists the individual age, sex, FD value, MMSE score, and sites of reduced blood flow on the 3D-SSP z score maps of the 17 patients in the VaD group. The z score maps showed that the reduction of CBF in VaD could be divided into 2 abnormal patterns: global reduction and a decrease in the frontal region only. Figure 5 shows representative 3D-SSP z score maps from patients with a global reduction of CBF (patient 1, Fig. 5A) and with reduction confined to the frontal region of CBF (patient 8, Fig. 5B). The image of reduced CBF in the frontal region was obtained from the same subject as shown in Figure 3.

Representative 3D-SSP z score maps from patients with diffuse reduction of CBF and reduction mainly confined to frontal region of CBF. (A) Diffuse reduction of CBF (arrows) (patient 1). (B) Decrease in frontal region (arrowheads) (patient 8).
Clinical Characteristics of Each VaD Patient
DISCUSSION
VaD is one of the major diseases responsible for senile dementia. Dementia is relatively difficult to diagnose in persons with an MMSE score of 20–25. The borderlines among so-called age-related cognitive impairment, mild cognitive impairment that is considered as the transition to the initial stage of dementia, and dementia itself remain unclear (31). A patient with VaD due to small-vessel disease may well be difficult to differentiate from a healthy volunteer by neuroimaging studies, but such a patient would presumably not resemble a healthy volunteer clinically. Cerebral functional imaging techniques that have been used to assist in diagnosis, such as PET and SPECT, are helpful for understanding the pathology of VaD. However, evaluation based only on morphologic criteria should be considered with caution, as demonstrated by the report of Loeb et al. (32) that CT showed no differences in the site and size of cerebral infarction between demented and nondemented groups.
PET is superior to SPECT with respect to sensitivity and spatial resolution. PET images obtained with 18F-FDG have been widely used for the diagnosis of AD because of a higher spatial resolution than those obtained with 15O gas or H215O. A correspondence between 99mTc-HMPAO SPECT and 18F-FDG PET has been found in AD (33). In this study, before 3D-FA was applied to CBF SPECT images, the FD value obtained from images processed by 3D-FA was examined for its correlation with that obtained from similarly processed 18F-FDG PET images. The FD value obtained from the former images correlated significantly with that from the latter images, suggesting that the heterogeneity of accumulation was similar on both 99mTc-HMPAO CBF SPECT and 18F-FDG PET images. This finding indicates that the FD value determined by 99mTc-HMPAO CBF SPECT images may also reflect cerebral metabolism and that SPECT can be used at medical institutions not equipped for PET.
Many studies have examined the cerebral metabolic dynamics of VaD using functional imaging techniques (34,35). One study showed reduced CBF and a reduced cerebral metabolic rate of oxygen in the white matter and cortex of patients with Binswanger’s disease, a clinical type of VaD (36). Other SPECT studies have shown that CBF was diffusely reduced (1) or that it was mainly reduced in the frontal lobes of patients with VaD (2–4). Thus, the findings have varied and no definite conclusions have been obtained. Cerebral blood flow and metabolism are generally reduced at sites of cerebrovascular damage. In patients with dementia, reduced CBF and metabolism may not be limited to the sites of cerebrovascular damage but may extend to wider areas. The 17 patients in the VaD group had small-vessel disease with dementia, according to the VaD classification of NINDS-AIREN (5). Small-vessel disease with dementia includes multiple lacunar strokes and Binswanger’s disease. Other types in the VaD classification include multi-infarct dementia characterized by extensive infarcts in the cortex and frequent dementia symptoms; hypoperfusion; hemorrhagic dementia; and, less frequently, strategic single-infarct dementia, which were not examined in the present study. Although CBF SPECT is generally evaluated visually, visual detection of CBF heterogeneity or other CBF distribution abnormalities in VaD due to small-vessel disease is often difficult. Therefore, CBF SPECT images were statistically analyzed to assess the heterogeneity and distribution of CBF in the present study.
CBF SPECT images of the VaD group were quantitatively more heterogeneous and had a higher FD value than those of the control group. Nagao et al. reported that AD patients showed a more heterogeneous CBF than did healthy volunteers (26). The mean FD values for the healthy volunteers and AD patients were 0.52 ± 0.09 and 0.74 ± 0.33, respectively, with a significant difference between the 2 groups. The difference in the FD value of the control group between studies was probably due to different settings of the Butterworth filter for pretreatment (cutoff frequency, 0.25 cycles per pixel). It is necessary to compare the heterogeneity of CBF in VaD and AD to examine whether the 2 diseases can be distinguished by the FD value.
We also used 3D-SSP to evaluate CBF distribution in patients with VaD. A line of 6 pixels directed from the surface into the brain is set for each site on the brain surface, and the highest pixel count is used as the value for that site. Therefore, 3D-SSP could be used in patients with VaD due to small-vessel disease who had no cortical infarction but, instead, had infarcts in the perforator vessel system. Although it is difficult to visually detect reduced blood flow in VaD on ordinary orbitomeatal line tomograms, the changes could be delineated with 3-dimensional cerebral surface images in 8 projections. 3D-SSP z score mapping revealed 2 patterns of reduced CBF, a global reduction and a reduction confined to the frontal region (Table 2). For example, patient 4 showed a high FD value of 1.373 and heterogeneous CBF. The 3D-SSP z score map showed reduced CBF in the frontal region, with an MMSE score of 10. This result is consistent with previous reports that CBF was reduced diffusely with no specific pattern in VaD (1) or, conversely, that CBF was reduced in the frontal lobes (2–4). In contrast to AD, VaD often shows reduced blood flow in the anterior region. In fact, 5 of our 17 patients had reduced blood flow mainly in the frontal region. Although not examined in the present study, symptoms associated with frontal lobe dysfunction have been reported in patients with VaD (37). Attention should be paid to differentiation from frontotemporal dementia (38) or Parkinson’s disease with dementia, which resemble VaD with respect to reduced blood flow in the frontal region. The 17 patients with VaD due to small-vessel disease even showed reduced blood flow in the cortex, with no morphologic abnormalities. This finding indicates that the statistical image analysis could detect reduced CBF, which was probably due to functional impairment as a remote effect (diaschisis) secondary to the disconnection between the deep cerebrum and cortex (39,40). Although the data are not presented here, a comparison of the VaD and control groups showed a global reduction in CBF on 3D-SSP in the VaD group.
Voxel-by-voxel analytic techniques may be sensitive to image quality, which may reflect differences in instruments and imaging conditions. The FD value is influenced by the collimator type and the image reconstitution filters. Therefore, a database of images should carefully be created under the same conditions. A database of normal images has to be constructed to prepare diagnostic statistical images for comparison with images from patients. In preparing such a normal database, one needs to determine to what extent the definition of “normal” and the parameters of the database should be unified, including number of subjects, age, sex, radioactive agent used, imaging devices and conditions, and method of reconstruction. Although it is desirable to prepare a normal database with images taken from age-matched healthy volunteers for each age group, it was impossible to collect a sufficient number of such images for the present study.
CONCLUSION
The present study suggested that the FD value calculated by 3D-FA may be an objective index of the heterogeneity of CBF in VaD and may be useful for easily and objectively evaluating VaD patients and healthy volunteers. In addition, the use of 3D-SSP allowed clearer visualization of the CBF distribution in VaD. Statistical image-analysis methods to enhance the determination of etiology are promising tools to characterize the CBF pattern in VaD, which is not easy to diagnose through conventional visual analysis.
Acknowledgments
We thank Yukio Nakamura, Hiroaki Matsuzawa, Kouichi Fujino, and Tomoko Fukunaga for helping us to perform the nuclear medicine examinations and for evaluating cognitive function.
Footnotes
Received Jun. 17, 2002; revision accepted Oct. 31, 2002.
For correspondence or reprints contact: Takuya Yoshikawa, MD, Department of Internal Medicine and Therapeutics, Osaka University Graduate School of Medicine (A8), 2-2, Yamadaoka, Suita City, Osaka, 565-0871, Japan.
E-mail: yoshi{at}tracer.med.osaka-u.ac.jp




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}