


Abstract
The presence of myocardial viability is predictive of improvement in regional left ventricular (LV) function after revascularization. Studies on predicting improvement in global LV function are scarce, and the amount of viable myocardium needed for improvement in LV ejection fraction (LVEF) after revascularization is unknown. Moreover, whether the presence of viability is associated with relief of heart failure symptoms after revascularization is uncertain. Hence, the aims were to define the extent of viable myocardium needed for improvement in LVEF and to determine whether preoperative viability testing can predict improvement in heart failure symptoms. Methods: Patients (n = 47) with ischemic cardiomyopathy (mean LVEF ± SD, 30% ± 6%) undergoing surgical revascularization were studied with 18F-FDG SPECT to assess viability. Regional and global function were measured before and 3–6 mo after revascularization. Heart failure symptoms were graded according to the New York Heart Association (NYHA) criteria, before and 3–6 mo after revascularization. Results: The number of viable segments per patient was directly related to the improvement in LVEF after revascularization (r = 0.79, P < 0.01). Receiver operating characteristic curve analysis revealed that the cutoff level of four viable segments (representing 31% of the left ventricle) yielded the highest sensitivity and specificity (86% and 92%, respectively) for predicting improvement in LVEF. Furthermore, the presence of four or more viable segments predicted improvement in heart failure symptoms after revascularization, with positive and negative predictive values of 76% and 71%, respectively. Conclusion: The presence of substantial viability (four or more viable segments, 31% of the left ventricle) on FDG SPECT is predictive of improvement in LVEF and heart failure symptoms postoperatively.
Identification of viable yet jeopardized myocardium helps in selecting patients for whom poor left ventricular (LV) function (ejection fraction), secondary to chronic ischemic heart disease, may improve after revascularization (1,2). Many studies, using various modalities, have focused on prediction of functional recovery, mainly regional, after revascularization (3–8). In contrast, studies focusing on predicting improvement in global LV function (which may be more relevant in the clinical setting) are scarce (3–5,8). The available evidence suggests that improvement in LV ejection fraction (LVEF) can be expected only when a substantial amount of viable myocardium is present before revascularization. However, the exact relationship between improvement in LVEF and the amount of viable myocardium is unclear, as emphasized recently by Rahimtoola (9).
Bonow (10) recently suggested that, besides improvement in LVEF after revascularization, improvement in heart failure symptoms should be used to assess the clinical benefit of revascularization. Thus far, mainly patients with relatively preserved LV function (LVEF > 35%) presenting with angina pectoris instead of heart failure symptoms have been studied, as was recently pointed out in a panel report from the Wintergreen meeting of the American Society of Nuclear Cardiology (11). Hence, we studied a large group of patients with severely depressed LV function (mean LVEF ± SD, 30% ± 6%) who presented mainly with heart failure symptoms, and we evaluated the relationship between the preoperative extent of viable myocardium and the postoperative improvement in LVEF and whether preoperative viability testing allows prediction of postoperative improvement in heart failure symptoms.
The technique used to evaluate myocardial viability was 18F-FDG SPECT. Cardiac FDG imaging with SPECT and 511-keV collimators has been evaluated by several centers during the last 5 y (12–15).
MATERIALS AND METHODS
Study Population
Forty-seven patients with coronary artery disease and ischemic cardiomyopathy (40 men, 7 women; age range, 43–76 y; mean age, 61 y; LVEF range, 14%–39%; mean LVEF, 30% ± 6%) who were scheduled for surgical revascularization were enrolled in the study. The reasons for revascularization were heart failure in 38 patients and angina pectoris in 9. The decision for revascularization was made independently from the SPECT data.
All but one patient had a previous infarction (>1 mo before entry into the study), and 36 exhibited pathologic Q waves on the electrocardiogram (24 anterior, 7 inferior, and 5 both). All patients had significant coronary artery disease on angiography (>50% reduction in luminal diameter of at least one major epicardial coronary artery). They had an average of 2.7 ± 0.5 stenosed vessels. Five patients had diabetes mellitus type II, which was well regulated by oral hypoglycemic medication. All patients were stable during the study; none had unstable angina or myocardial infarction between revascularization and the scintigraphic studies or after the intervention. The mean interval between the SPECT study and revascularization was 2.2 ± 1.3 mo. Patients with 3–4+ (moderate to severe) mitral regurgitation were excluded. Each patient gave informed consent to the study protocol, which was approved by the ethical committees of the participating hospitals.
Study Protocol
Regional Perfusion.
Myocardial perfusion was assessed by resting 201Tl SPECT (performed within 15 min after tracer injection) or 99mTc-tetrofosmin SPECT. Data were stored in a 64 × 64, 16-bit matrix. From the raw scintigraphic data, 6-mm-thick (1 pixel) transaxial slices were reconstructed by filtered backprojection. The slices were not corrected for attenuation. Further reconstruction yielded long- and short-axis projections perpendicular to the heart axis.
Regional Glucose Use.
Myocardial glucose use was evaluated by FDG SPECT during hyperinsulinemic euglycemic clamping. The details of the FDG SPECT studies have been described elsewhere (12,15). For the detection of 511-keV photons, specially designed collimators were used (van Mullekom; Nuclear Fields, Boxmeer, The Netherlands) (12,15). Reconstruction of data was identical to that for the perfusion studies. The perfusion study and the FDG SPECT study were performed on the same day. Cardiac medication was continued during the study. Medication consisted of β blockers, angiotensin-converting enzyme inhibitors, nitrates, calcium antagonists, diuretics, and aspirin and was left unchanged after the revascularization.
SPECT Image Analysis.
The perfusion and FDG SPECT data were analyzed quantitatively as described elsewhere (12,15). Briefly, circumferential profiles (60 radii, highest pixel activity per radius) from the available short-axis slices were generated (after alignment of the perfusion and FDG short-axis slices) and displayed in a polar map format. The polar maps were divided into 13 segments (using segments similar to those for echocardiography).
Segmental activities were compared with normal databases, and perfusion defects were detected (when segmental activities were less than two SDs below normal). The segments exhibiting a perfusion defect were subdivided into matches (concordantly reduced perfusion and FDG uptake) or mismatches (reduced perfusion with increased FDG uptake), as described previously (12,15). Dysfunctional segments (detected by resting echocardiography) were considered viable either when perfusion was normal or when a perfusion–FDG mismatch was present; dysfunctional segments with a perfusion–FDG match were considered nonviable (12,15). Matches were subdivided into nontransmural matches (tracer activities ≥ 60%) and transmural matches (tracer activities < 60%) (16). Although the nontransmural matches are a mixture of subendocardial scars and viable (normal) tissue, improvement in the function of these segments was recently shown to be not likely (16). Therefore, both subcategories were classified as nonviable.
Analysis of Regional Function Before and After Revascularization.
Regional contractile function was evaluated by resting echocardiography before revascularization. Four standard views of the left ventricle were recorded on videotape: parasternal long- and short-axis views and apical two- and four-chamber views. The images were reviewed off-line, and consensus was reached by two observers unaware of the SPECT data. For exact alignment of the echo data and SPECT data, the left ventricle was divided into 13 comparable segments as previously reported (12,15): one apical segment, six distal segments (anterior, anterolateral, inferolateral, inferior, inferoseptal, and anteroseptal), and six basal segments (comparable with the distal segments). Both inward wall motion and wall thickening were analyzed. Each segment was assigned a wall motion score of 0–3, with 0 = normal, 1 = hypokinetic (decreased endocardial excursion and systolic wall thickening), 2 = akinetic (absence of endocardial excursion and systolic wall thickening), and 3 = dyskinetic (paradoxic outward movement in systole). Follow-up echocardiography was performed 3–6 mo (mean, 4.3 ± 1.8 mo) after revascularization. Improvement in wall motion by one grade or more was considered the gold standard for viability (on a regional basis). Improvement from dyskinesia to akinesia was not considered an improvement in function. The observers were unaware of whether the echocardiograms had been obtained before or after revascularization.
Analysis of Global Function Before and After Revascularization.
LVEF (before and 3–6 mo [mean, 4.3 ± 1.8 mo] after revascularization) was assessed by equilibrium radionuclide ventriculography. Radionuclide ventriculography was performed at rest with the patients supine after administration of 740 MBq 99mTc. Images were acquired with a small-field-of-view gamma camera (Orbiter; Siemens Corp., Iselin, NJ) oriented in the 45° left anterior oblique position with a 5°–10° caudal tilt. The LVEF was calculated from the 45° left anterior oblique view by an automated technique, whereas the radionuclide ventriculography program required supervision to ensure adequate discrimination and separation between the left atrium and the left ventricle and correct positioning of the background ROI near the left ventricle. Improvement in global function after revascularization was defined as an increase of at least 5% in LVEF. This cutoff criterion had been used previously (4). Thus, the gold standard for viability on a global basis (patient basis) was considered an improvement of at least 5% in LVEF after revascularization. The observers who supervised the automated program were unaware of whether the radionuclide ventriculograms had been obtained before or after revascularization.
Assessment of Symptoms Before and After Revascularization.
Functional status was assessed according to the New York Heart Association (NYHA) criteria (for symptoms of heart failure) and according to the Canadian Cardiovascular Society (CCS) classification (for angina pectoris). For each patient, the functional status before and 3–6 mo after revascularization was determined by interviews and physical examinations conducted by an investigator who was unaware of the SPECT and LVEF data.
Statistical Analysis
Descriptive results are expressed as mean ± SD. Patient data were compared using the Student t test for paired and unpaired data when appropriate. Proportions were compared using χ2 analysis. Simultaneous comparison of more than two mean values was performed using one-way ANOVA. The relationship between the number of dysfunctional and viable (or nonviable) segments and the change in LVEF after revascularization was determined by linear regression analysis. Multivariate logistic regression analysis was performed to determine which variable best predicted improvement in LVEF after revascularization. Subsequently, receiver operating characteristic (ROC) analysis was performed to determine the optimal number of dysfunctional yet viable segments on SPECT, allowing discrimination between patients with and without improvement in LVEF after revascularization. The optimal number of segments was defined as that providing the maximal sum of sensitivity and specificity. P < 0.05 was considered significant.
RESULTS
Functional Outcome and Relationship with SPECT
Segments.
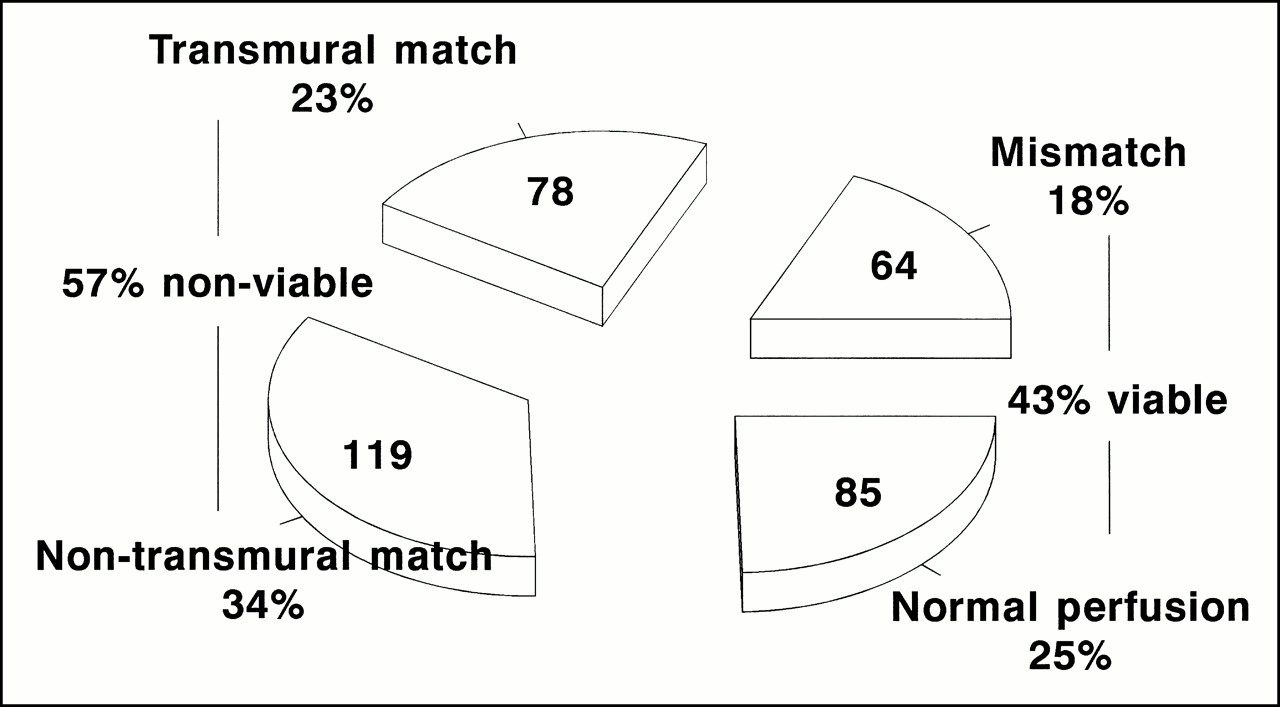
Of the 611 segments analyzed by echocardiography, 265 had normal wall motion and 346 had abnormal wall motion before revascularization. Of the 346 dysfunctional segments, 184 were hypokinetic and 162 were akinetic or dyskinetic. The mean number of abnormal segments per patient was 7.4 ± 2.3. Eighty-five dysfunctional segments had normal perfusion, whereas 261 segments had a perfusion defect; 64 perfusion defects showed increased FDG uptake (mismatched pattern), and 197 had concordantly decreased FDG uptake (matched pattern, with 78 transmural matches and 119 nontransmural matches) (Fig. 1). Thus, according to the viability criteria for SPECT, 149 segments (43%) were viable.
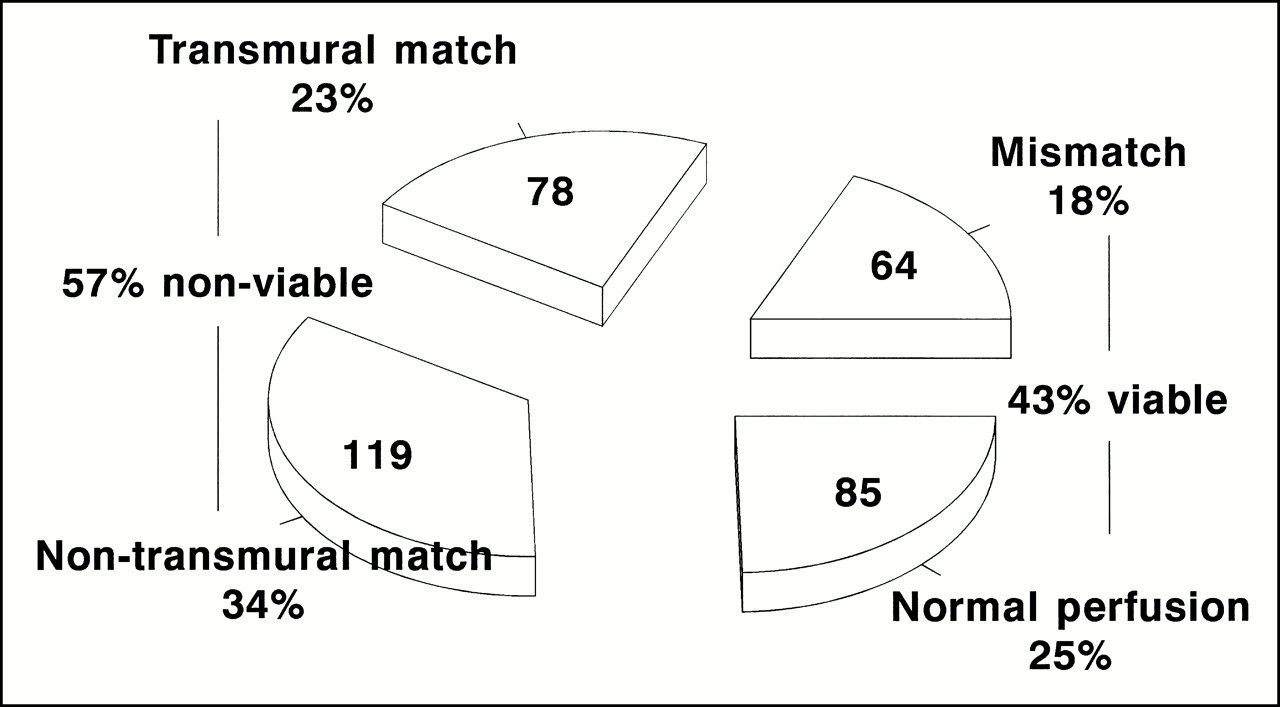
Pie chart showing distribution of various patterns on SPECT in the 346 dysfunctional, revascularized segments.
Of the 346 dysfunctional segments, 124 improved in function after revascularization, 200 remained unchanged, and 22 deteriorated. Of note, function improved in 64 of the segments with normal perfusion, in 41 mismatches, in 15 nontransmural matches, and in 4 transmural matches. The accuracy in predicting improvement on a regional basis is shown in Table 1.
Accuracy of SPECT in Assessing Improvement in Regional and Global LV Function
A significant relationship existed between the number of viable segments on SPECT and the magnitude of improvement in LVEF after revascularization (Fig. 2), suggesting that the extent of viability determined the magnitude of improvement in LVEF after revascularization. In addition, a weak inverse relationship existed between the number of nonviable segments and the magnitude of improvement in LVEF (y = 9.2 − 1.4x, r = 0.45, P < 0.05).
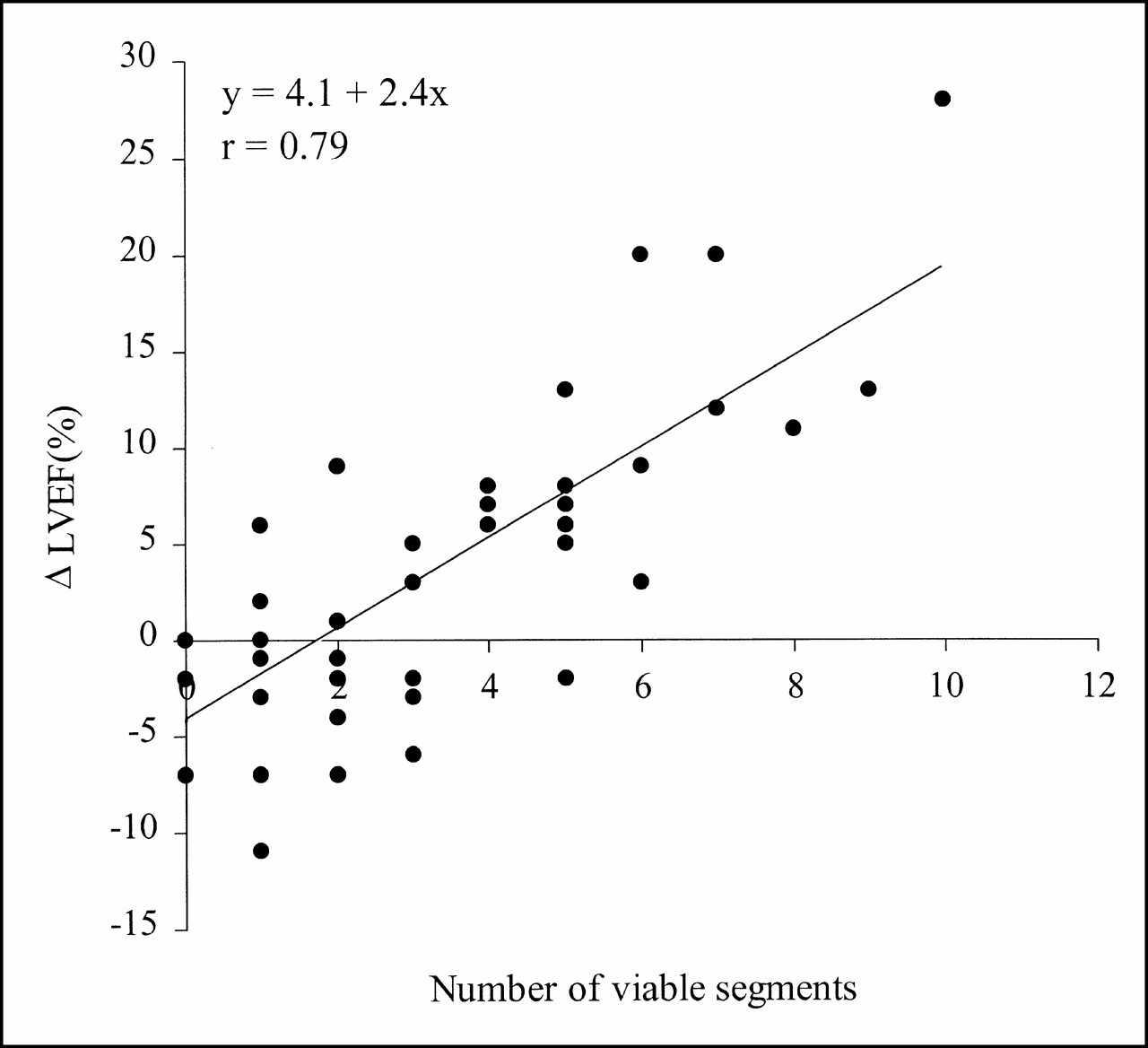
Scatterplot showing significant relationship between number of viable segments on SPECT and improvement in LVEF after revascularization (y = 4.1 + 2.4x, r = 0.79, P < 0.001).
Patients.
Twenty-one patients (45%) showed improvement in LVEF (≥5%) after revascularization. The characteristics of the two groups are shown in Table 2. No significant differences between the two groups were noted, except for the number of viable segments on SPECT, the number of nonviable segments on SPECT, and the history of a Q-wave myocardial infarction. Multivariate analysis (including sex, age, Q-wave myocardial infarction, angina class [CCS], heart failure class [NYHA], number of stenosed coronary arteries, LVEF, number of viable segments, and number of nonviable segments) showed that the number of viable segments was the only predictor of improvement in LVEF after revascularization; the number of nonviable segments (or the combination of both) did not contribute significantly.
Clinical Data Before Revascularization
Prediction of Improvement in LVEF After Revascularization.
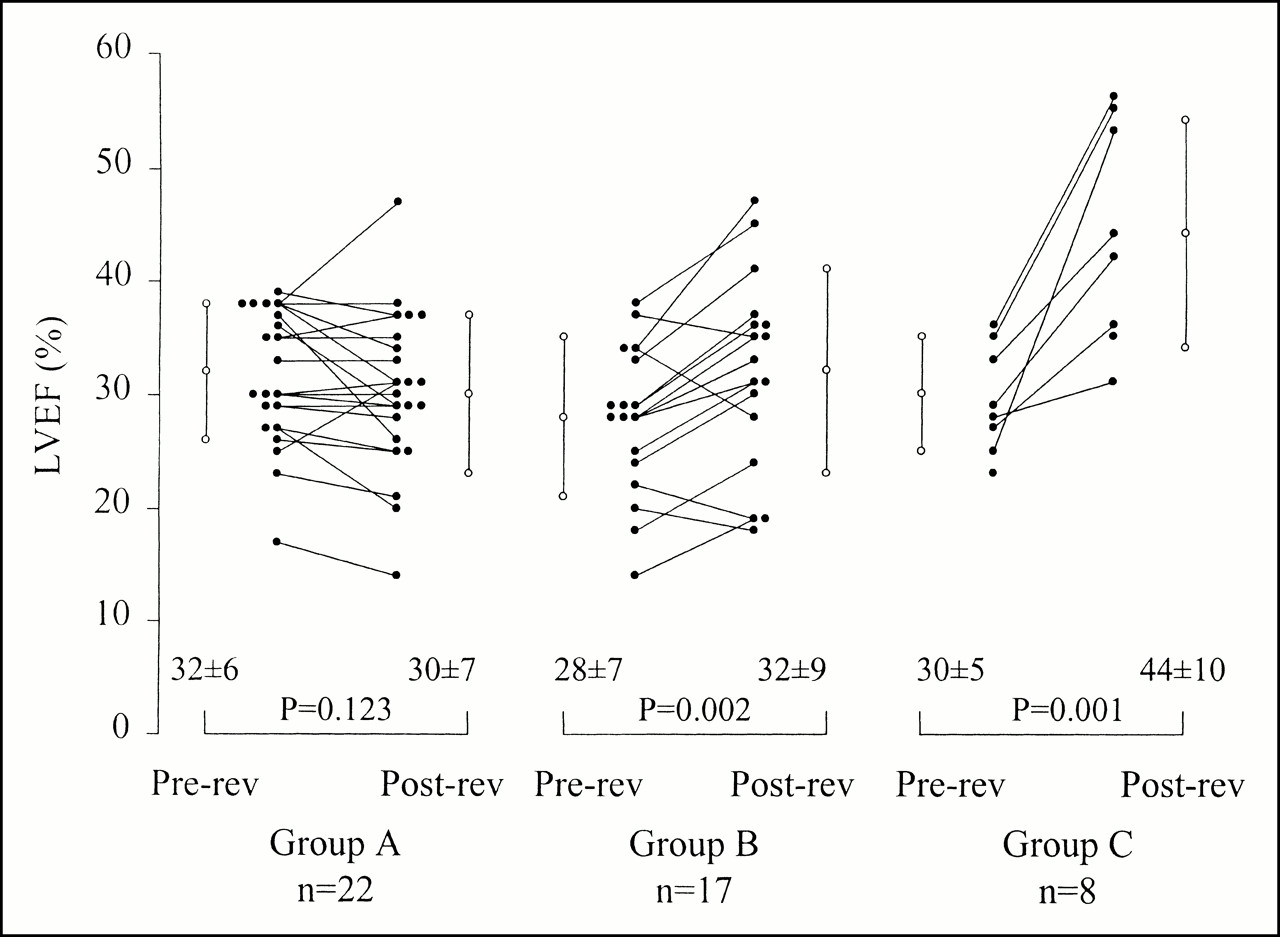
ROC curve analysis showed that the cutoff level of four dysfunctional but viable segments yielded the highest sensitivity and specificity (Fig. 3); with this cutoff level, a sensitivity of 86% and a specificity of 92% were obtained (Table 1). Accordingly, patients were divided into three groups with a similar baseline LVEF. Group A consisted of 22 patients with minimal or no evidence of viability before revascularization (less than three viable segments; mean, 1.0 ± 0.8). Group B consisted of 17 patients with intermediate viability before revascularization (between three and five viable segments; mean, 4.1 ± 0.8). Group C consisted of 8 patients with a large area of viable tissue (six or more viable segments; mean, 7.4 ± 1.4). Figure 4 shows the individual changes in LVEF of the patients in the different groups. The largest increase in LVEF was observed in group C (from 30% ± 5% to 44% ± 10%, P = 0.001); 7 (88%) of 8 patients showed a significant increase in LVEF (mean increase, 16% ± 6%). Patients in group B showed a modest improvement in LVEF (from 28% ± 7% to 32% ± 9%, P = 0.002); 12 (71%) of 17 patients showed a significant improvement in LVEF (mean increase, 7% ± 2%, P < 0.01 vs. group C). No increase in LVEF was observed in group A (from 32% ± 6% to 30% ± 7%, P = not significant [NS]). Only 2 (9%) of 22 patients showed a significant improvement in LVEF.

ROC curve analysis showing that cutoff level of four dysfunctional but viable segments yielded highest sensitivity and specificity to predict functional outcome on patient basis.

Scatterplot of changes in LVEF after surgery grouped according to extent of preoperative viability. Mean preoperative LVEF was not significantly different in the three groups. Group A = less than three viable segments; Group B = between three and five viable segments; Group C = six or more viable segments; rev = revascularization.
Improvement in Symptoms Versus Viability
Angina Pectoris.
Nine patients presented with primarily angina pectoris. Three of them had four or more viable segments on SPECT (one patient with six viable segments, one with five, one with four, two with three, two with two, and two with none), and in all nine patients the CCS score improved by one or more grades. The mean CCS score decreased from 3.2 ± 0.4 to 1.2 ± 0.4 (P < 0.05) after revascularization.
Heart Failure Symptoms.
Thirty-eight patients (81%) presented with primarily heart failure symptoms; 37 were in class 3 or 4. The patients were again divided into three groups, with a comparable NYHA score before revascularization (3.1 ± 0.5 [group A], 3.3 ± 0.5 [group B], 3.4 ± 0.5 [group C], P = NS). Group A consisted of 18 patients with minimal or no evidence of viability before revascularization (less than three viable segments). Group B consisted of 13 patients with intermediate viability before revascularization (between three and five viable segments). Group C consisted of 7 patients with a large area of viable tissue (six or more viable segments). Figure 5 shows the individual changes in NYHA score of the patients in the different groups. The largest improvement in NYHA score was observed in group C (from 3.4 ± 0.5 to 1.7 ± 0.8, P = 0.001); 6 (86%) of 7 patients showed an improvement in NYHA classification. Patients in group B showed slightly less improvement in NYHA score (from 3.3% ± 0.5% to 2.2% ± 1.0%, P = 0.003); 8 (62%) of 13 patients showed an improvement in NYHA classification. No increase in NYHA score was observed in group A (from 3.1 ± 0.5 to 2.9 ± 0.8, P = NS). Still, 7 (39%) of 18 patients showed a significant improvement in NYHA classification. Importantly, the mean changes in NYHA classification were significantly different between the three groups (P < 0.05). With four or more viable segments on SPECT considered predictive of improvement in heart failure symptoms, SPECT had a positive predictive value of 76% and a negative predictive value of 71% (Table 3).
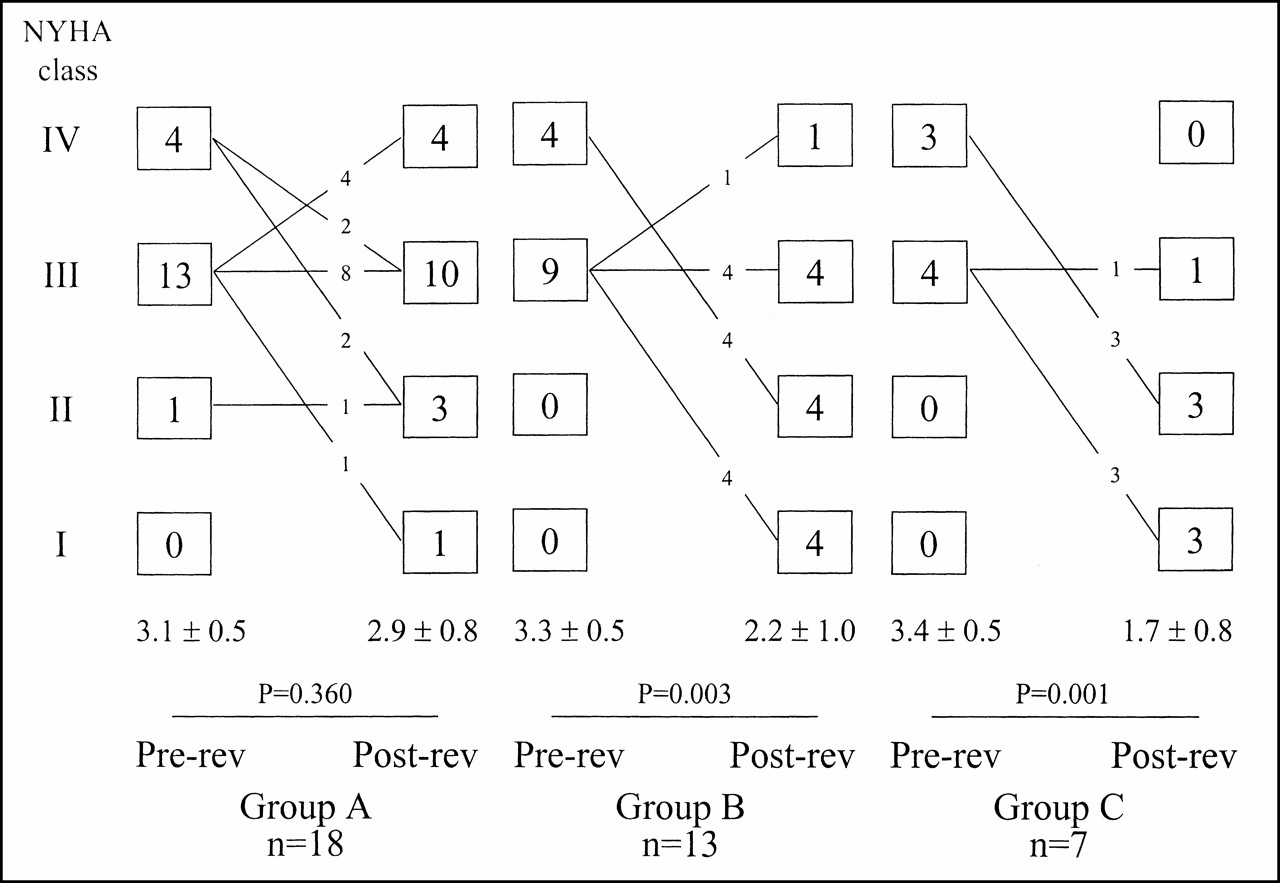
Change in NYHA classification of patients after surgery; patients are grouped according to extent of preoperative viability. Mean preoperative NYHA score was comparable in the three groups. Group A = less than three viable segments; Group B = between three and five viable segments; Group C = six or more viable segments; rev = revascularization.
Relationship Between Viability and Improvement in NYHA Score After Revascularization
Relationship Between Improvement in Heart Failure Symptoms and Improvement in LVEF
Of the 22 patients with an improvement in LVEF, 16 presented with heart failure symptoms, and 12 (75%) of these 16 improved their NYHA score by one grade or more. Their mean score improved from 3.3 ± 0.5 to 1.8 ± 0.8 (P < 0.01). In contrast, of the 26 patients without an improvement in LVEF, 22 presented with heart failure symptoms, and only 7 (32%) of these 22 improved their NYHA score. The mean score was 3.2 ± 0.5 before revascularization and 2.9 ± 0.8 after revascularization (P = NS).
DISCUSSION
The most important findings of this study can be summarized as follows. First, the magnitude of improvement in LVEF is directly related to the extent of dysfunctional but viable tissue. Second, using the cutoff value of four dysfunctional but viable segments, an accurate prediction of improvement in LVEF after revascularization is possible. Third, the presence and extent of viability is predictive of the improvement in heart failure symptoms after revascularization.
Prediction of Improvement in LVEF After Revascularization
Prediction of improvement in regional function after revascularization has been shown previously (3–8). Most previous studies, however, included patients with a relatively preserved LV function and did not systematically study patients who had severely depressed LVEF and presented with heart failure symptoms (11,17). In this study, focusing on patients who had a more depressed LV function and presented with heart failure symptoms, we showed a high sensitivity (85%) and specificity (80%) for predicting improvement in regional LV function after revascularization. These results are in line with the literature on FDG PET (17) and previous FDG SPECT data (15).
Clinically more important is the prediction of improvement in global LV function. Our results showed that three features were predictive of improvement in LVEF: the number of viable segments on SPECT, the number of nonviable segments on SPECT, and the history of a Q-wave myocardial infarction. Multivariate analysis showed that the number of viable segments was the only predictor of improvement in LVEF after revascularization. This finding was reflected in a strong relationship between the number of viable segments on SPECT and the magnitude of improvement in LVEF after revascularization (Fig. 2), as was also shown by Pagano et al. (18). Subsequent ROC curve analysis pointed out that the cutoff value of four dysfunctional but viable segments on SPECT yielded the optimal trade-off between sensitivity and specificity for predicting improvement in LVEF: 86% and 92%, respectively. This finding underscores that a substantial amount of viable myocardium (31% of the left ventricle) needs to be present to result in improvement in LVEF and hence to justify a revascularization procedure in patients with a relatively high risk for procedural or periprocedural complications (19). The results agree with observations by Tillisch et al. (3) showing improvement in LVEF in patients with two or more viable segments on FDG PET (using a seven-segment model, i.e., 29% of the left ventricle). The results also agree with our previous work on a different patient population (with comparable baseline characteristics) using dobutamine echocardiography (20). Accurate identification of patients whose LVEF can improve also has important prognostic consequences, because LVEF is directly related to long-term prognosis (21).
Prediction of Improvement in Heart Failure Symptoms After Revascularization
Bonow (10) recently suggested that recovery of LV function after revascularization may not be the optimal endpoint for assessing benefit from revascularization. Also, the clinical relevance (in terms of improving quality of life) of an improvement in LVEF by 5% or more is unclear. In this study, improvement in heart failure symptoms was observed mainly in patients in whom LVEF improved; this observation suggests that an improvement in LVEF by 5% or more is clinically relevant, because alleviation of heart failure symptoms may result. Moreover, this study showed that the presence of substantial viability was highly predictive of improvement in heart failure symptoms after revascularization: patients with a small extent of viable tissue on SPECT exhibited no improvement in heart failure symptoms, whereas patients with an intermediate and a large extent showed a significant improvement. These data are in line with previous findings (22,23). Eitzman et al. (22), in a retrospective analysis, showed that heart failure symptoms did improve in patients for whom FDG PET showed viability and who underwent revascularization. In addition, Di Carli et al. (23) found, similarly to us, that the magnitude of improvement in heart failure symptoms after revascularization was related to the preoperative extent of viability (assessed by FDG PET).
FDG Imaging with SPECT
Traditionally, FDG is imaged with PET. During the past few years, several centers have gained experience with high-energy SPECT using FDG and 511-keV collimators (12–15). Three studies (from different centers) have independently shown good agreement between FDG SPECT and FDG PET for the detection of myocardial viability (12–14). Moreover, we recently showed that FDG SPECT was capable of predicting improvement in regional contractile function after revascularization, yielding diagnostic accuracy comparable with that of FDG PET (15). The main disadvantage of FDG PET is the relatively limited availability of PET equipment at a time when the need for viability studies is growing because of the increasing number of patients presenting with symptoms of heart failure (24). The advantage of FDG SPECT is that widespread availability of SPECT cameras may allow routine FDG imaging in the future. The 511-keV collimators have now become commercially available. Moreover, although a cyclotron unit remains necessary, the relatively long half-life of FDG (110 min) allows transportation of this tracer over substantial distances.
Limitations
Several limitations of this study need to be addressed. First, no control angiography was performed after revascularization. Therefore, vessel or graft patency remains uncertain. Early graft occlusion may have prohibited some viable segments from recovering.
Second, functional follow-up was performed 3–6 mo after revascularization. Evidence from the literature supports both early and late recovery. LaCanna et al. (6) have shown immediate recovery after revascularization. However, others have shown that improvement may occur up to 1 y after revascularization (25,26). In a recent report, we showed that some viable segments on FDG imaging did not recover until 14 mo after revascularization (27). This delayed improvement in function may be related to the presence of more severe ultrastructural damage. Therefore, the recovery process (both for heart failure symptoms and for contractile function) may not have been completed at 3–6 mo follow-up, and longer follow-up studies are needed.
Third, long-term prognosis was not addressed in this study. It will be of interest to evaluate the long-term outcome of the patients with viable myocardium who did not improve in LVEF or heart failure symptoms. Recent data by Samady et al. (28) indicated that even in the absence of LVEF improvement, an event-free long-term prognosis may still be possible. However, in that study, improvement in LVEF was evaluated somewhat soon after revascularization; a later assessment may have shown recovery of LVEF in some patients with a favorable prognosis.
Finally, we did not perform stress testing before or after revascularization. Therefore, improvement in exercise-induced ischemia cannot be assessed from our data.
CONCLUSION
The number of viable segments per patient was directly related to the improvement in LVEF after revascularization (r = 0.79, P < 0.01); this parameter was also the only predictor of improvement in LVEF after revascularization. Analysis of receiver operating characteristic curves revealed that the cutoff level of four viable segments (representing 31% of the left ventricle) yielded the highest sensitivity and specificity (86% and 92%, respectively) for predicting improvement in LVEF. Furthermore, the presence of at least four viable segments predicted improvement in heart failure symptoms after revascularization, with positive and negative predictive values of 76% and 71%, respectively.
Footnotes
Received Jan. 13, 2000; revision accepted May. 16, 2000.
For correspondence or reprints contact: Jeroen J. Bax, MD, Department of Cardiology, Leiden University Medical Center, Rijsburgerweg 10, 2333 AA Leiden, The Netherlands.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effect of myocardial revascularisation on left ventricular systolic function in patients with and without viable myocardium: should non-viable segments be revascularised?
- Administration of Cardiac Stem Cells in Patients With Ischemic Cardiomyopathy: The SCIPIO Trial: Surgical Aspects and Interim Analysis of Myocardial Function and Viability by Magnetic Resonance
- Prognosis of patients with ischaemic cardiomyopathy after coronary revascularisation: relation to viability and improvement in left ventricular ejection fraction
- Stunning, Hibernation, and Assessment of Myocardial Viability
- Assessment of Myocardial Viability in Patients with Heart Failure
- Impact of Diabetes Mellitus on Prediction of Clinical Outcome After Coronary Revascularization by 18F-FDG SPECT in Patients with Ischemic Left Ventricular Dysfunction
- Prediction of beneficial effect of {beta} blocker treatment in severe ischaemic cardiomyopathy: assessment of global left ventricular ejection fraction using dobutamine stress cardiovascular magnetic resonance
- Electromechanical Properties of Perfusion/Metabolism Mismatch: Comparison of Nonfluoroscopic Electroanatomic Mapping with 18F-FDG PET
- Extensive Left Ventricular Remodeling Does Not Allow Viable Myocardium to Improve in Left Ventricular Ejection Fraction After Revascularization and Is Associated With Worse Long-Term Prognosis
- Radionuclide techniques for the assessment of myocardial viability and hibernation
- Pulsed wave tissue Doppler imaging for the quantification of contractile reserve in stunned, hibernating, and scarred myocardium
- Prognostic Value of Rest 201Tl-Dipyridamole Stress 99mTc-Sestamibi Gated SPECT for Predicting Patient-Based Clinical Outcomes After Bypass Surgery in Patients with Ischemic Left Ventricular Dysfunction
- Dobutamine-Induced Contractile Reserve in Stunned, Hibernating, and Scarred Myocardium in Patients with Ischemic Cardiomyopathy
- Perfusion and Contractile Reserve in Chronic Dysfunctional Myocardium: Relation to Functional Outcome After Surgical Revascularization
- Does CABG Improve Left Ventricular Ejection Fraction in Patients with Ischemic Cardiomyopathy, and Does It Matter?