


Abstract
We investigated the postoperative prognostic value of preoperative myocardial SPECT for predicting clinical outcomes, including event-free survival and functional improvement. Methods: A total of 123 patients with ischemic heart disease and left ventricular dysfunction were enrolled. The ratio of men to women was 103:20, and the mean (±SD) age was 61 ± 8 y. The disease involved 3 vessels in 95 patients, 2 vessels in 27 patients, and 1 vessel in 1 patient. Rest 201Tl-dipyridamole stress 99mTc-sestamibi gated 24-h-delayed SPECT was performed before and 3–4 mo after bypass surgery. With a 20-segment model, a dysfunctional segment was defined as that with systolic wall thickening of <20%. Dysfunctional but viable segments were defined for each viability predictor, including rest thallium uptake of >60%, reversibility score (rest perfusion minus stress perfusion) of >7, systolic wall thickening of >10%, and 24-h-delayed thallium uptake of >60%. Global left ventricular functional improvement was defined as a 5% increase in the left ventricular ejection fraction (LVEF) or a 10-mL decrease in the end-systolic volume (ESV). A long-term follow-up evaluation was performed by chart reviews and telephone interviews over a period of up to 6 y. Cardiac events were defined as cardiac death, myocardial infarction, or heart failure requiring hospitalization. Results: After bypass surgery, the LVEF was improved from 36.4% ± 8.8% (mean ± SD) to 44.3% ± 11.1%, and the ESV was improved from 96.6 ± 46.7 mL (mean ± SD) to 75.1 ± 44.0 mL. Global left ventricular function was improved in 96 patients but not improved in 27. Rest thallium uptake (≥4 segments) and reversibility (≥5 segments) were found to be significant variables in the receiver-operating-characteristic (ROC) curve analysis, with area-under-the-curve (AUC) values of 0.755 (P < 0.05) and 0.735 (P < 0.05), respectively. The values for preserved systolic wall thickening and delayed thallium uptake had no statistical significance. Using a multivariate logistic function, we created a single variable consisting of rest thallium uptake and reversibility; this variable had better prediction power than any other single variable (AUC value for the ROC curve, 0.794). Patients with a higher logistic function value (≥0.84) showed better event-free survival than did those with a lower logistic function value (<0.84) (log-rank test, P < 0.05). Conclusion: The number of viable segments should be >4 for rest 201Tl SPECT or >5 for the reversibility parameter for the prediction of global functional improvement in a patient-based evaluation. With a logistic function created from these parameters, the long-term clinical prognosis after bypass surgery could be predicted by the presence of viability on preoperative rest-stress myocardial SPECT.
The aim of revascularization includes improvement in left ventricular function (1), enhancement of the quality of life (2), freedom from angina symptoms, and increase in survival (3). Among these, clinical outcome related to functional improvement after revascularization is expected only in patients who have viable myocardium (4). Therefore, various imaging methods that can identify viable myocardium have been used in patients with ischemic left ventricular dysfunction. Assessment of cellular membrane integrity with 201Tl or 99mTc-sestamibi (5), assessment of myocardial metabolism with 18F-FDG PET (6), and assessment of the contractile response with dobutamine stress echocardiography (7) are the methods most widely used for the identification of viable myocardium.
Myocardial SPECT yields parameters of myocardial perfusion that can predict postoperative functional improvement, such as rest thallium absolute uptake (8–10) or ischemia represented in the form of a reversible decrease in perfusion (9,11). In addition to perfusion information, gated SPECT can assess wall motion and systolic wall thickening, which also have been reported to be a predictor of viability (12–15). The simultaneous objective quantification of regional perfusion and function can be achieved with an automatic image-processing algorithm. Measurements of perfusion and function with such an algorithm on gated SPECT have been reported to be both valid and reproducible (16,17).
Numerous published studies have focused on the predictor of postoperative segmental function instead of global left ventricular dysfunction. However, whether a patient should undergo bypass surgery depends on the individual gain represented by the clinical outcome. Thus, studies focusing on predicting postoperative improvement in global left ventricular function or clinical outcome are needed. An increase in the left ventricular ejection fraction (LVEF) (18–21) or a decrease in the end-systolic volume (ESV) (22,23) can be adopted as a marker of global functional improvement, with event-free survival being used as another endpoint in patient-based viability studies.
The aims of this study were to evaluate the predictive value of viability markers from gated SPECT for the prediction of clinical outcomes after bypass surgery and to find a way to represent the predictive accuracy of each variable in combination. We evaluated the amount of viable myocardium needed to allow for an improvement in global myocardial function.
MATERIALS AND METHODS
Patients
A total of 123 patients with coronary artery disease and left ventricular dysfunction were enrolled in this study (ratio of men to women, 103:20; mean (±SD) age, 61 ± 8 y). The preoperative LVEF was 36% ± 9% (mean ± SD; range, 13%–49%), and 75 patients had severe left ventricular dysfunction (LVEF, <40%). On coronary angiography, 95 patients had 3-vessel disease, 27 patients had 2-vessel disease, and 1 patient had 1-vessel disease. Twenty-two patients had a history of prior infarction. All of the patients underwent coronary artery bypass grafting (CABG). Preoperative SPECT was performed 19 ± 23 d (mean ± SD) before and postoperative SPECT was performed 108 ± 25 d after CABG (range, 77–195 d).
There were no acute complications during or after CABG. The patency of the grafted vessels was confirmed by follow-up coronary angiography 1 y after CABG.
Myocardial SPECT
Rest 201Tl-dipyridamole stress 99mTc-sestamibi gated 24-h 201Tl redistribution SPECT was performed before CABG. Patients refrained from consuming caffeine-containing beverages for 24 h and fasted for 4 h before the study. At 10 min after an injection of 111 MBq of 201Tl, the rest SPECT image was acquired. Afterward, dipyridamole at 0.56 mg/kg was continuously injected over 4 min for the stress study. At 3 min after the completion of the stress study, 925 MBq of 99mTc-sestamibi were injected. Gated SPECT with 99mTc-sestamibi was performed 90 min after the stress study. For 51 patients who had a perfusion defect on the rest SPECT images, 24-h 201Tl redistribution SPECT was performed on the next day.
SPECT was performed with a dual-head γ-camera equipped with a low-energy high-resolution collimator (Vertex EPIC; ADAC Laboratories). Thirty-two step-and-shoot images were acquired at intervals of 3° for 25 s per step. For gating, 16 frames per cardiac cycle with prefixed R-R intervals and 40% windows were used. Images were reconstructed with a Butterworth filter at a cutoff frequency of 0.35 and order 10 for 201Tl and at a cutoff frequency of 0.45 and order 10 for 99mTc-sestamibi. Rest 201Tl-dipyridamole stress 99mTc-sestamibi gated SPECT was repeated 3 mo after CABG with the same protocol as that used for the preoperative study.
The reconstructed images were analyzed by use of an automatic quantifying software package (AutoQUANT; ADAC Laboratories) without manual intervention. For the regional analysis, a 20-segment model was adopted. Stress and rest segmental perfusion and 24-h delayed redistribution were quantified and expressed as percentages of maximal uptake. The reversibility score was defined as rest perfusion minus stress perfusion (representing the number of reversible segments). Segmental wall thickening was expressed as a percentage of the end-diastolic wall thickness. The LVEF and ESV were also measured by quantitative gated SPECT.
Viability Assessment
Patient-based global viability was defined as either an improvement in the LVEF of >5% or a decrease in the ESV of >10 mL. For prediction of this global viability, segmental viability was defined operationally by use of the dysfunctional segment, which was defined as preoperative systolic wall thickening of <20% (24). A segment with rest perfusion or 24-h delayed redistribution of >60% was regarded as a viable segment in rest SPECT and delayed SPECT. A segment with a reversibility score (rest perfusion minus stress perfusion) of >7 was regarded as a viable segment in terms of perfusion reversibility. A segment with systolic wall thickening of >10% was regarded as viable. The number of viable segments for each criterion was tested as a predictor for patient-based global viability.
To extract a single predictor for viability from the significant parameters, a logistic probability function was calculated as follows:
 where α is the intercept, β is the coefficient for each variable, X is the quantified score for each variable, and i is the assignment number of each variable. The predictive value of this single logistic parameter was also tested.
where α is the intercept, β is the coefficient for each variable, X is the quantified score for each variable, and i is the assignment number of each variable. The predictive value of this single logistic parameter was also tested.
Patient Monitoring
The clinical significance of the single logistic probability also was evaluated as a prognostic factor in a follow-up study. Chart reviews and telephone interviews were conducted. The patients were monitored for at least 6 mo and up to 6 y (mean ± SD, 32 ± 20 mo). Cardiac events were defined as cardiac death, myocardial infarction, and heart failure requiring hospitalization. The patients were divided into 2 groups according to the logistic probability, and the event-free survival rates for the groups were compared.
Statistical Analysis
Receiver-operating-characteristic (ROC) curve analysis was performed to determine the predictive value and the optimal cutoff value of each parameter. Area-under-the-curve (AUC) values were compared; curves were designated as being significantly different when the P value was <0.05. A discriminant analysis was also performed to select significant parameters for the logistic probability.
For the statistical analysis, SPSS (SPSS Inc.) and MedCalc (MedCalc) software were used.
RESULTS
Viability Assessment with Various Parameters
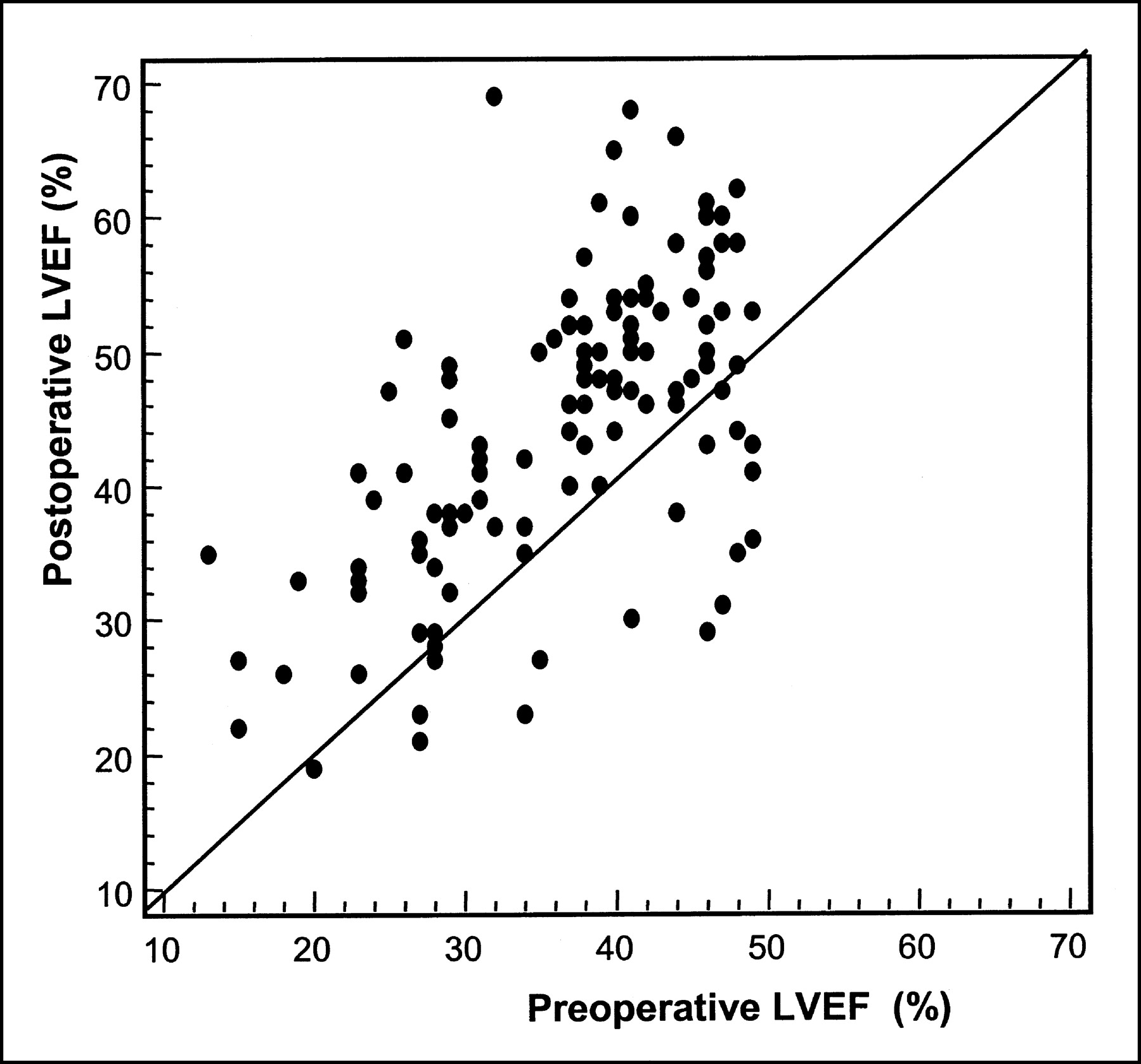
The LVEF was improved after bypass surgery from 36% ± 9% to 44% ± 11% (Fig. 1), and the ESV was decreased from 97 ± 47 mL to 75 ± 44 mL (data are reported as mean ± SD). In 83 patients, the LVEF was improved by >5%, and in another 13 patients, the ESV was decreased by >10 mL without improvement in the LVEF. These 96 patients were classified into the global viable group, and the remaining 27 were classified into the nonviable group.

Scatter plot showing pre- and postoperative LVEF values.
A total of 1,341 dysfunctional segments were evaluated for the 123 patients. An ROC curve analysis was performed with the SPECT parameters. The AUC value for viable segments in rest perfusion was 0.755 (95% confidence interval [CI], 0.669–0.828) (Fig. 2A), and that for the reversibility score was 0.735 (95% CI, 0.648–0.811) (Fig. 2B). The difference in AUC values between rest perfusion and the reversibility score was statistically significant (P < 0.05). The AUC value for preserved systolic wall thickening was 0.682 (95% CI, 0.592–0.763) (Fig. 2C), and that for delayed redistribution was 0.694 (95% CI, 0.547–0.818) (Fig. 2D). The numbers of segments with the best diagnostic values are shown in Table 1. The number of viable segments in rest thallium uptake (≥4) and the number of reversible segments (≥5) were found to be statistically significant by the ROC curve analysis. However, the number of segments with preserved systolic wall thickening (≥6) and the number of viable segments in delayed thallium uptake (≥3) showed no statistical significance.

ROC curve analyses for prediction of postoperative global functional improvement with each SPECT predictor. (A) Analysis by rest thallium uptake. (B) Analysis by reversibility score. (C) Analysis by measurement of preserved systolic wall thickening. (D) Analysis by delayed redistribution thallium uptake.
Results of Discriminant Analysis of Global Functional Improvement with Predictors from Gated SPECT
Single Predictor with Logistic Probability Function
With a logistic probability function, a single predictive parameter (logistic probability) was calculated from the statistically significant variables, that is, the number of viable segments in rest thallium uptake and the number of reversible segments (Table 2).
Coefficient Estimates of Numbers of Viable Segments Determined by Multivariate Logistic Regression to Predict Global Functional Myocardial Viability
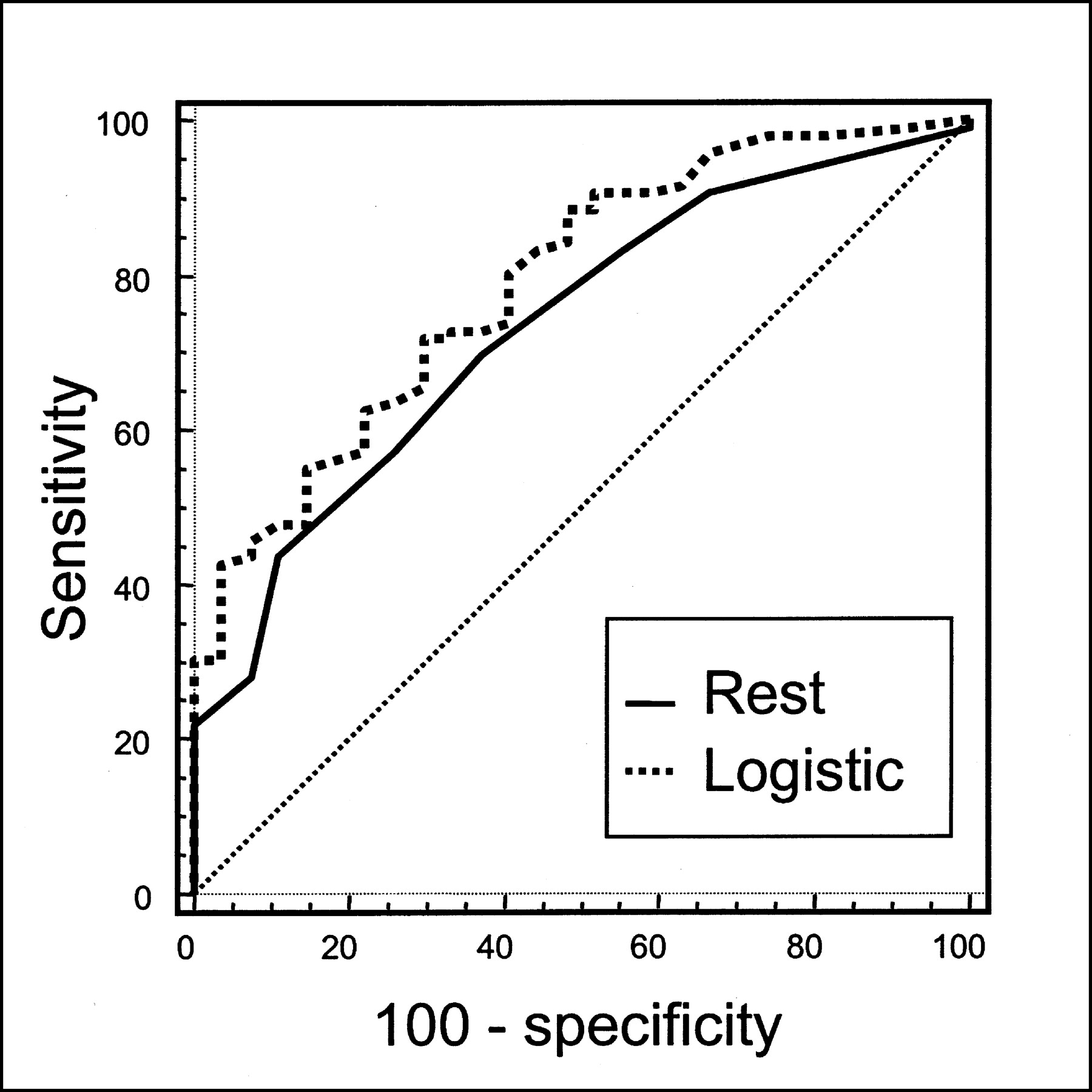
The AUC of the logistic probability function was 0.794 (95% CI, 0.706–0.857). The cutoff value determined from the ROC curve was 0.84; the sensitivity and specificity were 55% and 89%, respectively (Fig. 3). The AUC for the logistic function was larger than that for any single variable from gated SPECT (P < 0.05) (Fig. 4).

ROC curve analysis for prediction of postoperative global functional improvement by logistic function encompassing rest thallium uptake and reversibility.
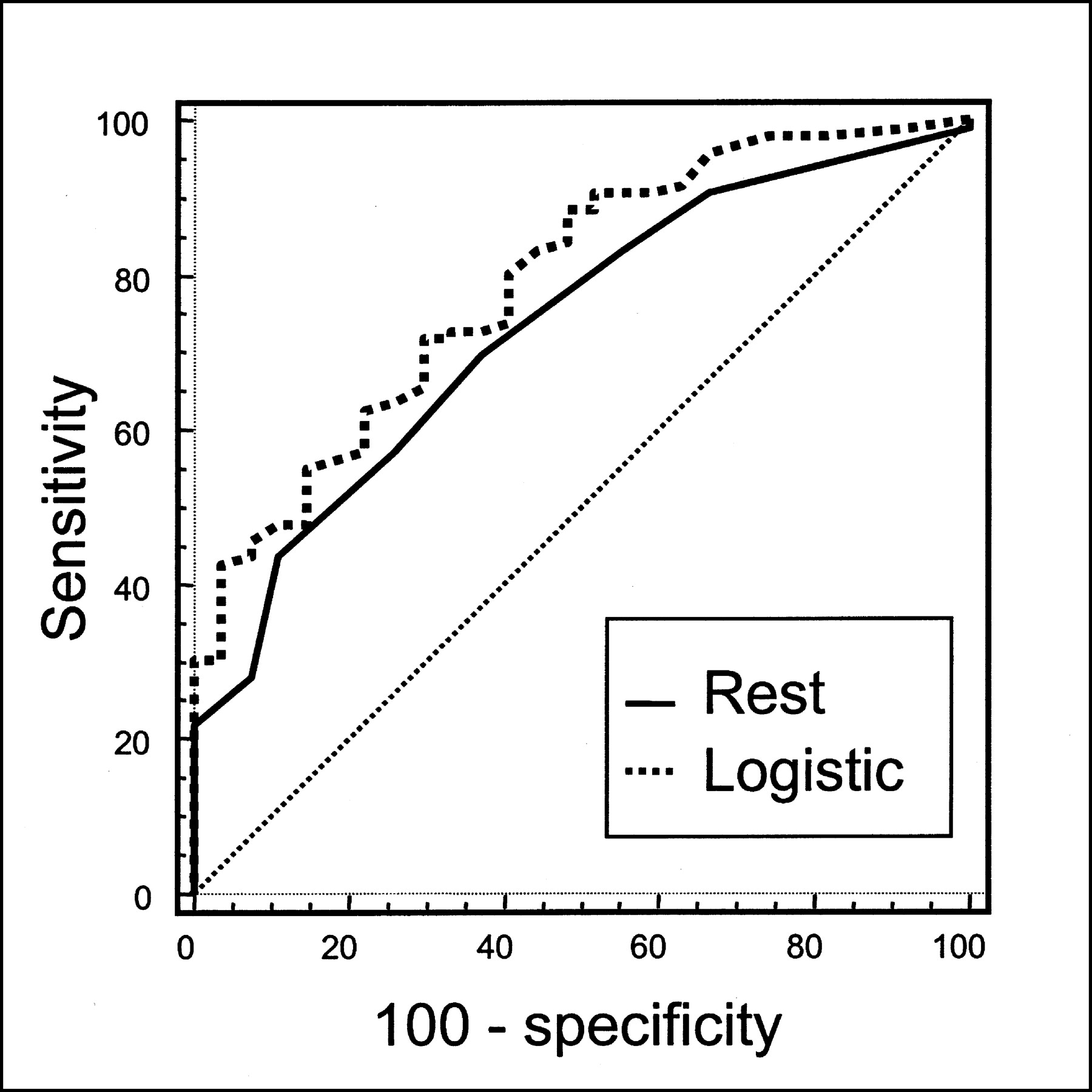
Comparison of ROC curve for logistic function with that for rest thallium uptake.
Event-Free Survival Analysis
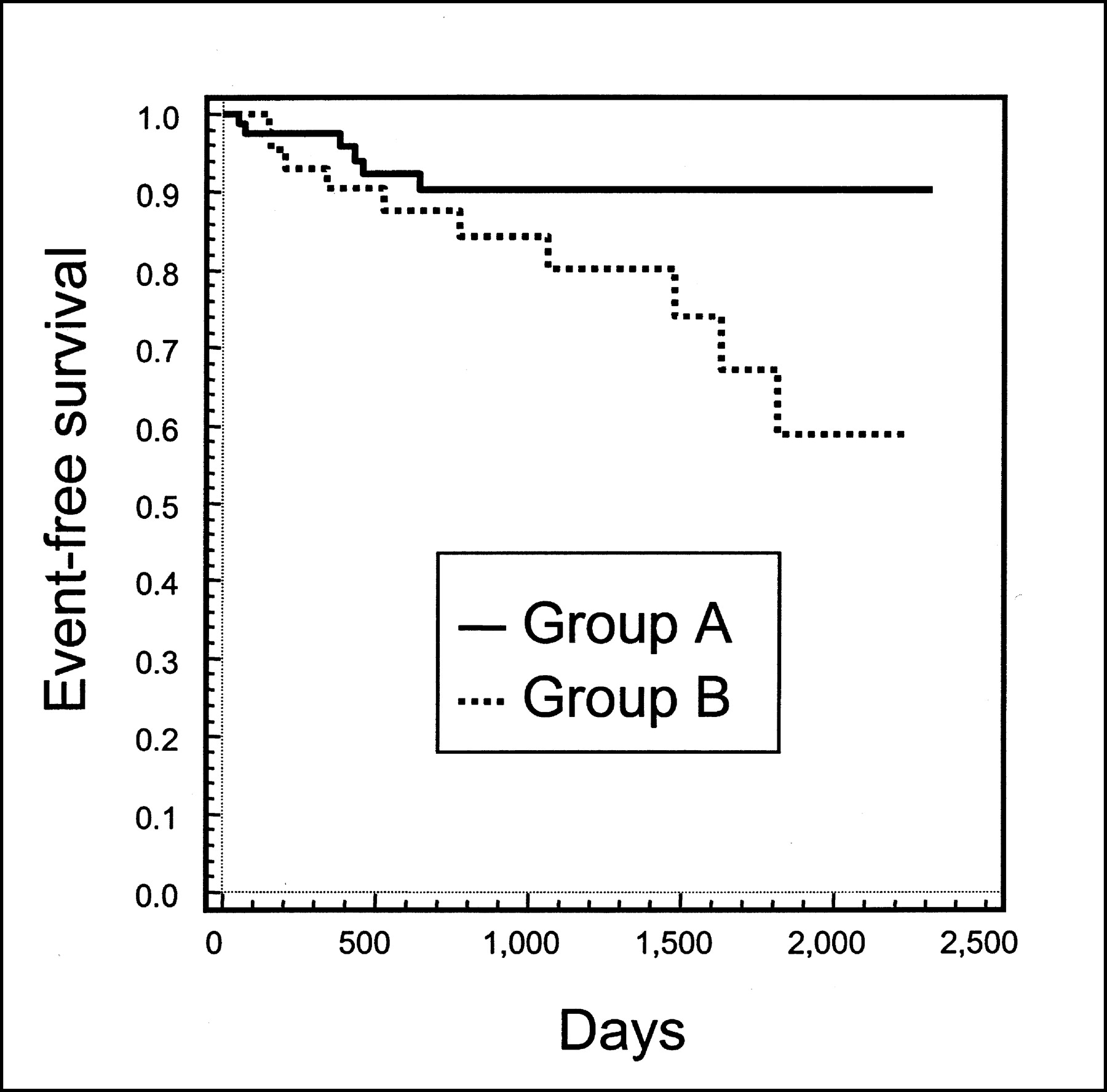
The follow-up period was 32 ± 20 mo, and 17 cardiac events occurred during this period. There were 2 cases of cardiac death, 1 of myocardial infarction, and 14 of heart failure. According to the best diagnostic cutoff value for the logistic function, the patients were divided into 2 groups (group A logistic function, ≥0.84; group B logistic function, <0.84). Fifty-two patients were assigned to group A, with 6 experiencing cardiac events. Seventy-one patients were assigned to group B, with 11 experiencing cardiac events. The rate of cardiac events was significantly higher in group B (log-rank test, P < 0.05) (Fig. 5).
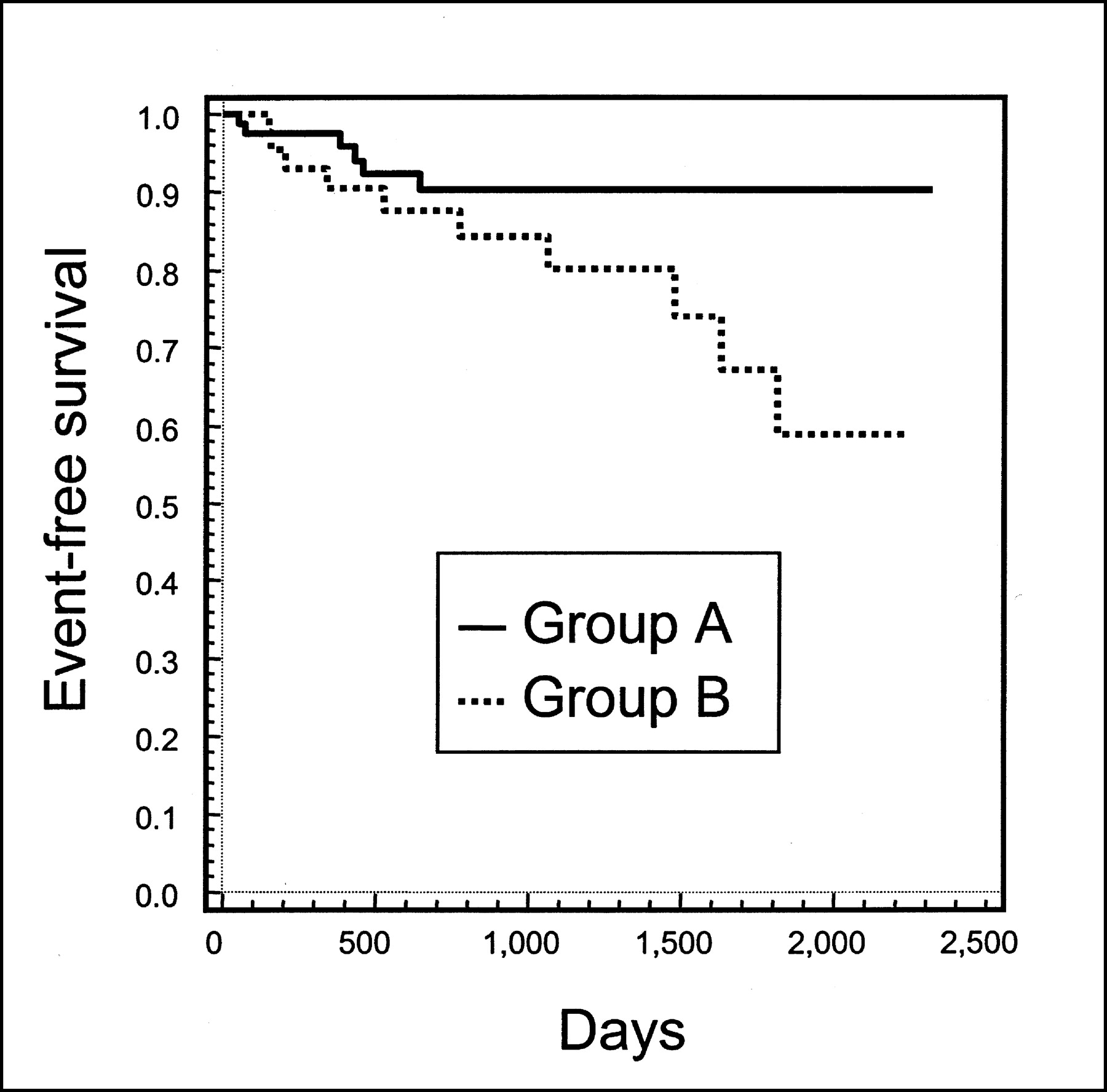
Event-free survival curves for patients in 2 groups. Patients with higher logistic function (≥0.84) were assigned to group A; those with lower logistic function (<0.84) were assigned to group B. Rate of cardiac events was higher in group B (P < 0.05).
DISCUSSION
The assessment of myocardial viability on a segmental basis provides information on whether a certain segment will improve after revascularization. However, myocardial viability should be evaluated in terms of the patient, as is the case for bypass surgery.
The LVEF is a well-known parameter that predicts an improvement in the quality of life. The left ventricular ESV has been linked to event-free survival (22,23). Therefore, global functional improvement represented by an increase in LVEF and a decrease in ESV can be a principal target of revascularization. In this study, we used poststress LVEF or ESV as an alternative to rest LVEF or ESV (16). Although poststress LVEF and ESV values may differ from rest values, it has been reported that poststress global functional improvement can serve as an alternative to an evaluation of the rest function and may offer incremental information beyond the rest function because the poststress period can reflect stunning effects (22). The reproducibility of LVEF and ESV values obtained from gated SPECT with automatic quantitative software has been reported elsewhere (25–27).
In segmental viability analysis, the extent of perfusion is an important marker, but in a patient-based analysis, the extent of diseased myocardium also is important, because the main required end result of this study was an improvement in global function, such as LVEF or ESV. In this study, the numbers of segments necessary to predict functional improvement after surgery were 4 in rest thallium uptake and 5 in terms of reversibility; which numbers represent 20%–25% of the entire myocardium. We could infer that more than 20%–25% viable myocardium is necessary for an improvement in global function after bypass surgery. In previous studies with FDG SPECT and dobutamine stress echocardiography, 31% viable myocardium (4 of 17 segments) was necessary for global functional improvement (21,28).
A patient-based viability study can determine whether a patient should undergo surgery, and the possibility for bypass surgery should be evaluated by consideration of all of the possible variables from rest-stress gated myocardial SPECT. Therefore, we needed to devise a new method to find an appropriate representative parameter containing all of the significant predictors from gated SPECT and its optimal cutoff value for the prediction of postoperative myocardial viability.
To devise a new method containing significant variables, we adopted a multivariate logistic function. With a logistic regression method, the coefficients of the participating predictors from a maximum-likelihood method were acquired. We were able to calculate the logistic function from these coefficients, along with the quantitative scores for the perfusion and function parameters. As rest thallium uptake and reversibility were significant parameters, we created a logistic function from them. The simultaneous assessment of the number of viable segments in rest thallium uptake and the number of reversible segments was useful as a single parameter for the prediction of global functional viability after bypass surgery. The logistic function is expected to be used for variables that should be considered simultaneously.
Samady et al. (29) reported that bypass surgery in patients with viable myocardium might improve survival and quality of life with no change in global function. Therefore, event-free survival should be another endpoint of viability studies. On the basis of the most accurate cutoff values for the logistic function, patients could be classified into high- and low-logistic-function groups. The high-logistic-function group showed better survival after bypass surgery than did the low-logistic-function group. The independent predictive value of viability markers on rest-stress gated myocardial SPECT could have been examined to predict postoperative clinical outcome (event-free survival) for patients whose global function did not improve after bypass surgery.
We used a 20-segment model for the quantification of perfusion and wall function, instead of a 17-segment model, as the quantitative scores could be acquired automatically with our routine protocol. In the 20-segment model, there might be some differences in size according to the location of the segment. In this study, we were not concerned about the location or distribution of viable segments. Further studies on the effects of the location and distribution of viable segments on postsurgical outcomes are needed.
Abnormal septal wall motion caused by anteromedial cardiac translation is a common finding after CABG. Gated myocardial SPECT also has demonstrated the development of septal wall motion abnormalities after CABG (30,31). However, septal wall motion abnormalities have been known not to influence LVEF or ESV. Therefore, we do not think that this phenomenon, commonly known as heart swing, had an effect on our study results.
A limitation of this study was the short follow-up period. Further improvement in global function might be possible after the 3- to 4-mo follow-up period used in this study. Long-term follow-up is necessary to evaluate long-term outcomes.
CONCLUSION
This study demonstrated the overall diagnostic accuracy of rest-stress gated myocardial SPECT in predicting postoperative clinical outcomes in patients with coronary artery disease with left ventricular dysfunction. Using a logistic function, we devised a single predictor that contained statistically significant variables from gated myocardial SPECT and that showed better diagnostic accuracy than any other single variable. The cardiac event rate was higher in the low-logistic-function group.
Footnotes
Received Mar. 5, 2003; revision accepted Jul. 10, 2003.
For correspondence or reprints contact: Dong Soo Lee, MD, Department of Nuclear Medicine, Seoul National University College of Medicine, 28 Yeongeon-dong, Jongno-gu, Seoul 110-744, Korea.
E-mail: dsl{at}plaza.snu.ac.kr




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}