


Abstract
Because of damage to cardiomyocytes and the contractile apparatus, contractile reserve may be observed less frequently in hibernating than in stunned myocardium. The aim of this study was to assess the presence of contractile reserve in response to dobutamine infusion in a large group of patients with stunned and hibernating myocardium. Methods: A total of 198 consecutive patients with ischemic cardiomyopathy (left ventricular ejection fraction ≤ 40%) underwent resting 2-dimensional echocardiography to assess regional contractile dysfunction. On the basis of assessment of perfusion (with 99mTc-tetrofosmin SPECT) and glucose use (with 18F-FDG SPECT), dysfunctional segments were grouped. Dysfunctional segments with normal perfusion were classified as stunned. Dysfunctional segments with a perfusion defect were classified as hibernating when a perfusion-18F-FDG mismatch was present. Dysfunctional segments with a perfusion defect were classified as scar tissue when a perfusion-18F-FDG match was present; these segments were subdivided into nontransmural and transmural scars. Contractile reserve was evaluated by dobutamine stress echocardiography. Results: Dobutamine-induced contractile reserve was more frequently found in stunned than in hibernating myocardium (61% vs. 51%, respectively; P < 0.01). Only 14% of the scarred segments improved in wall motion during dobutamine infusion, significantly less than stunned or hibernating myocardium (P < 0.001). Nontransmural scars exhibited contractile reserve more frequently than did transmural scars. Conclusion: The progressive reduction of contractile reserve in stunned, hibernating, and scarred myocardium supports the hypothesis that stunning, hibernation, and scarring are not circumscript pathophysiologic entities but represent gradual ultrastructural damage on the myocyte level.
In patients with ischemic cardiomyopathy, distinguishing between hibernating, stunned, and scarred myocardium may have important implications for clinical management and outcome. If hibernating or stunned myocardium is present, coronary revascularization may not only reverse regional wall motion abnormalities but also improve global function, heart failure symptoms, and survival (1–3). Hibernating myocardium has been defined as a chronic state of contractile dysfunction with reduced blood flow at rest (4,5). Frequently, however, regional perfusion in chronic dysfunctional myocardium has been normal or nearly normal and has been referred to as stunning or repetitive stunning (6). Instead of 2 different entities, it is likely that stunning and hibernation form a continuum and that a gradual reduction of flow is accompanied by more ultrastructural damage on the myocyte level (7,8). Because of damage to the myocytes and the contractile apparatus, contractile reserve may be observed less frequently in hibernating myocardium than in stunned myocardium. However, the presence or absence of contractile reserve in these different entities has not been studied extensively. Therefore, the aim of this study was to assess the presence or absence of contractile reserve in response to dobutamine infusion in a large group of patients with stunned or hibernating myocardium.
MATERIALS AND METHODS
Study Population
A total of 198 consecutive patients with a clinically stable heart, angiographically proven chronic coronary artery disease, a left ventricular ejection fraction (LVEF) ≤ 40%, and heart failure symptoms were studied at least 6 mo after myocardial infarction. Patients with primary cardiomyopathy, significant valvular heart disease, or an inadequate acoustic window were not included in the study protocol.
The study protocol was as follows. First, LVEF was assessed by radionuclide ventriculography. Next, dysfunctional myocardium was identified by resting 2-dimensional echocardiography; the dysfunctional myocardium was then evaluated for the presence of stunning or hibernation by assessment of perfusion and glucose metabolism using SPECT. Finally, the presence of contractile reserve was evaluated by dobutamine stress echocardiography. All patients gave their informed consent; the local Ethics Committee approved the study protocol.
Radionuclide Ventriculographic Assessment of LVEF
After injection of 99mTc (740 MBq), radionuclide ventriculography was performed at rest with the patient supine. A small-field-of-view gamma camera (Orbiter; Siemens, Erlangen, Germany) was used, oriented in a 45° left anterior oblique position with a 5°–10° caudal tilt. The LVEF was calculated by standard methods (3).
Two-Dimensional Echocardiographic Assessment of Regional Dysfunction and Contractile Reserve
A commercially available imaging system (Sonos 5500; Hewlett Packard, Andover, MA) and a 1.8-MHz transducer using second harmonic imaging to optimize endocardial border visualization were used (9). Two-dimensional imaging was performed with the patient in the left lateral position; standard views were recorded onto an optical disk (cine loops).
For the assessment of contractile reserve in dysfunctional myocardium, dobutamine stress echocardiography was performed as described previously (9). β-Blocker therapy was not routinely discontinued during dobutamine stress echocardiography. Two patients were in atrial fibrillation. After the resting echocardiographic study, dobutamine was administered intravenously, starting at a dose of 5 μg per kilogram of body weight per minute for 5 min, followed by a 10 μg/kg/min dose for 5 min (low dose). Incremental doses of 10 μg/kg/min were given at 3-min intervals up to a dose of 40 μg/kg/min (high dose), and atropine was added if necessary.
Two experienced observers, unaware of the clinical data or the SPECT results, scored the digitized echocardiograms offline. In cases of disagreement, a majority decision was reached by a third observer. The left ventricle was divided into 16 segments according to the method of the American Society of Echocardiography (10). Regional wall motion and systolic wall thickening were scored using a 5-point grading scale: 1 = normal, 2 = mildly hypokinetic, 3 = severely hypokinetic, 4 = akinetic, and 5 = dyskinetic. Segments with hypokinesia, akinesia, or dyskinesia were considered abnormal; segments with mild hypokinesia were considered normal. Contractile reserve was defined as an improvement of segmental wall motion score by ≥1 grade after infusion of low-dose dobutamine. The wall motion score index was determined as the sum of the segmental scores of the 16 segments, divided by 16.
SPECT Assessment of Stunning and Hibernation
All patients underwent dual-isotope simultaneous-acquisition SPECT. Resting 99mTc-tetrofosmin SPECT (600 MBq) was used to assess regional perfusion. Myocardial glucose use was evaluated by 18F-FDG SPECT (185 MBq). To optimize and standardize the metabolic conditions during 18F-FDG SPECT, we administered 500 mg of Acipimox (BYK, Deventer, The Netherlands) orally to all patients (11,12). Patients with diabetes mellitus were instructed to continue antidiabetic medication. Plasma glucose levels were measured immediately before the study. In patients with a plasma glucose level > 8 mmol/L, insulin was administered intravenously to enhance myocardial 18F-FDG uptake. The plasma glucose level was measured again, and additional insulin was given if necessary. With this regimen, the image quality was good in all patients studied. A triple-head gamma camera (Prism 3000XP; Picker, Cleveland, OH) was used. The camera was equipped with commercially available high-energy 511-keV collimators (13). The energies were centered on the 140-keV photon peak of 99mTc-tetrofosmin with a 15% window and on the 511-keV photon peak of 18F-FDG with a 15% window. Data were acquired over 360° (120 sectors of 3°), with the patient supine. Total imaging time was 32 min. Data were stored in a 64 × 64, 16-bit matrix. The image data were reconstructed by filtered backprojection using a Butterworth filter (cutoff frequency, 0.17 cycles per pixel); 6-mm-thick (1 pixel) transaxial slices were obtained. Subsequently, standard short- and long-axis projections perpendicular to the heart axis were reconstructed.
The left ventricle was divided into 16 segments identical to the echocardiographic segmentation (10). Both 99mTc-tetrofosmin and 18F-FDG studies were analyzed quantitatively (segments normalized to maximum tracer uptake). Dysfunctional segments (identified by resting echocardiography) were evaluated for viability (14–16). Dysfunctional segments with normal perfusion (according to a normalized 99mTc-tetrofosmin uptake of >80%) were classified as stunned. Dysfunctional segments with a perfusion defect (normalized 99mTc-tetrofosmin uptake < 80%) were classified as hibernating when a perfusion-18F-FDG mismatch was present (increase in 18F-FDG uptake ≥ 10%, compared with 99mTc-tetrofosmin uptake). Dysfunctional segments with a perfusion defect were classified as scar tissue when a perfusion-18F-FDG match was present (<10% difference in tracer activities); these segments were subdivided into nontransmural and transmural scars. Segments with 99mTc tetrofosmin and 18F-FDG uptake ≥ 50% but without mismatch were classified as nontransmural scars, whereas segments with tracer activities < 50% were classified as transmural scars (14–16).
Statistical Analysis
Values are expressed as mean ± SD, and percentages are rounded when appropriate. Continuous variables were compared using the Student t test for unpaired samples. Differences between proportions were compared using the χ2 test. A value of P < 0.05 was considered statistically significant.
RESULTS
Demographics and Echocardiography
The clinical characteristics of the 198 patients are summarized in Table 1. All patients had heart failure symptoms; New York Heart Association (NYHA) functional class was, on average, 2.5 ± 0.9, and 120 patients (61%) were in NYHA class III or IV. Ventricular function was severely impaired in all patients; the LVEF averaged 30% ± 12%.
Clinical Characteristics of the 198 Study Patients
Echocardiography at rest was performed on 3,168 segments; 1,016 segments (32%) were normal or mildly hypokinetic and not considered for myocardial viability. Of the 2,152 dysfunctional segments, 1,119 were severely hypokinetic, 1,014 were akinetic, and 19 were dyskinetic.
SPECT Tissue Characterization
Dual-isotope SPECT demonstrated that 666 (31%) of the 2,152 dysfunctional segments had normal perfusion and glucose use; these segments were considered stunned. Reduced perfusion and relatively preserved glucose use (hibernating myocardium) were seen in 221 (10%) of the dysfunctional segments. The majority of the dysfunctional segments (1,265, or 59%) had concordantly reduced perfusion and metabolism and were considered scar tissue. There were 248 (20%) nontransmural and 1,017 (80%) transmural scars. The prevalence of stunned myocardium was higher in patients with mild heart failure symptoms (NYHA I/II) than in patients with severe heart failure symptoms (NYHA III/IV): 255 (36%) of 715 segments versus 411 (29%) of 1,437 segments (P = 0.001). Stunned myocardium was more frequently present in patients with angina (450 of 1,349 segments [33%]) than in patients without angina (216 of 803 segments [27%]) (P < 0.005).
Dobutamine Echocardiographic Assessment of Contractile Reserve
The hemodynamic variables at baseline and during low-dose dobutamine infusion (5 and 10 μg/kg/min stages) are shown in Table 2. During low-dose dobutamine infusion, both heart rate and the systolic heart rate-systolic blood pressure product increased significantly. The administration of dobutamine was well tolerated by all patients; the protocol was completed for all patients and no serious side-effects occurred.
Hemodynamic Changes During Dobutamine Infusion
Generally, wall motion score increased significantly in response to low-dose dobutamine (Table 2). Overall, 696 (32%) of the 2,152 dysfunctional segments exhibited contractile reserve during low-dose dobutamine stimulation. The prevalence of contractile reserve was higher in patients with mild heart failure symptoms (NYHA I/II) than in patients with severe heart failure symptoms (NYHA III/IV): 269 (38%) of 715 segments versus 427 (30%) of 1,437 segments, respectively (P < 0.001). In patients with and without angina, contractile reserve was present in 469 (35%) of 1,349 segments and in 227 (28%) of 803 segments, respectively (P < 0.005).
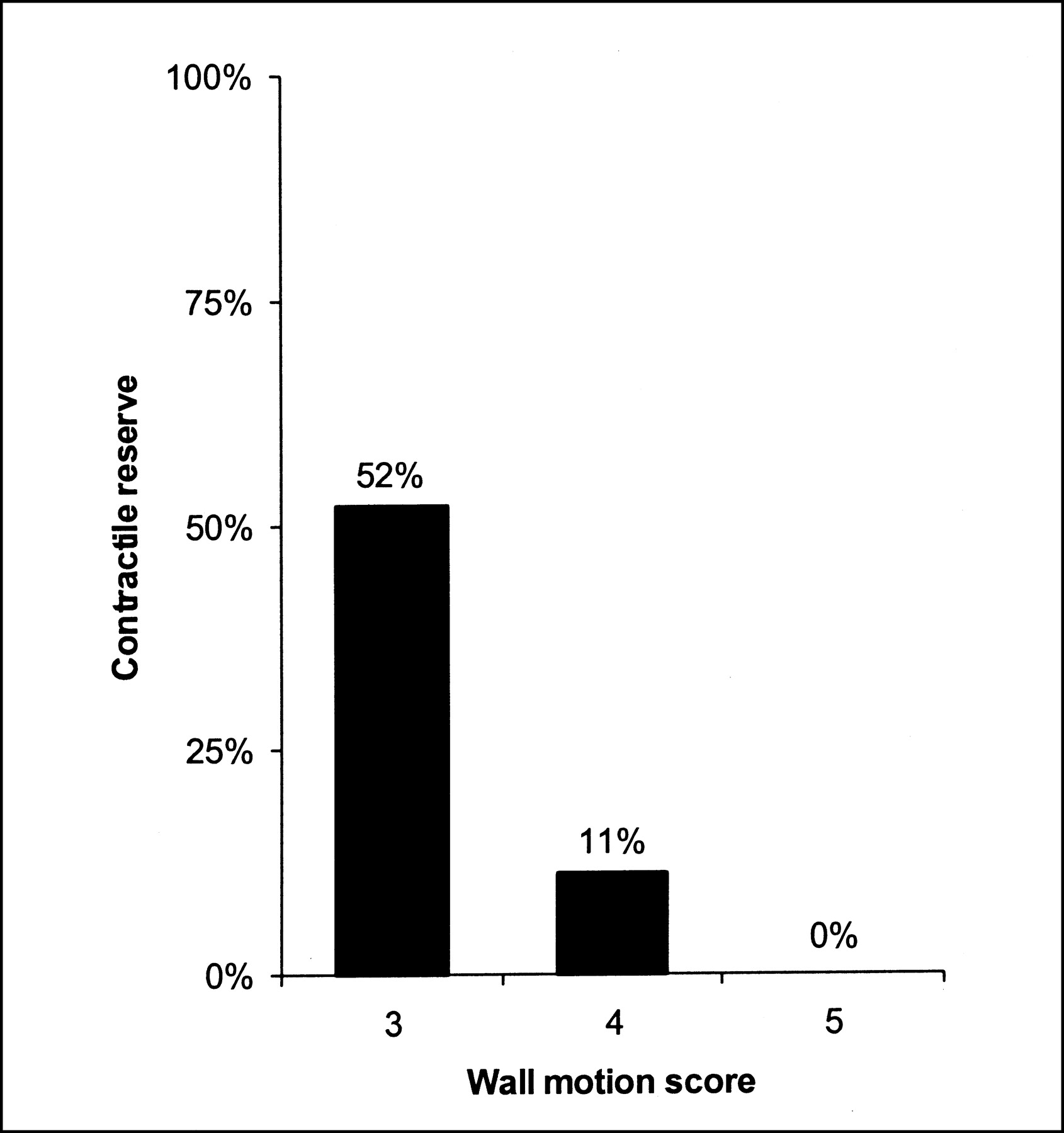
Contractile reserve in relation to severity of wall motion abnormalities is demonstrated in Figure 1. Severely hypokinetic segments more often exhibited contractile reserve than did akinetic segments (582 of 1,119 [52%] vs. 114 of 1,014 [11%], respectively; P < 0.001). In contrast, dobutamine-induced contractile reserve was absent from all 19 segments that were dyskinetic at baseline echocardiography.

Contractile reserve according to baseline wall motion (3 = severely hypokinetic, 4 = akinetic, 5 = dyskinetic) in all dysfunctional segments.
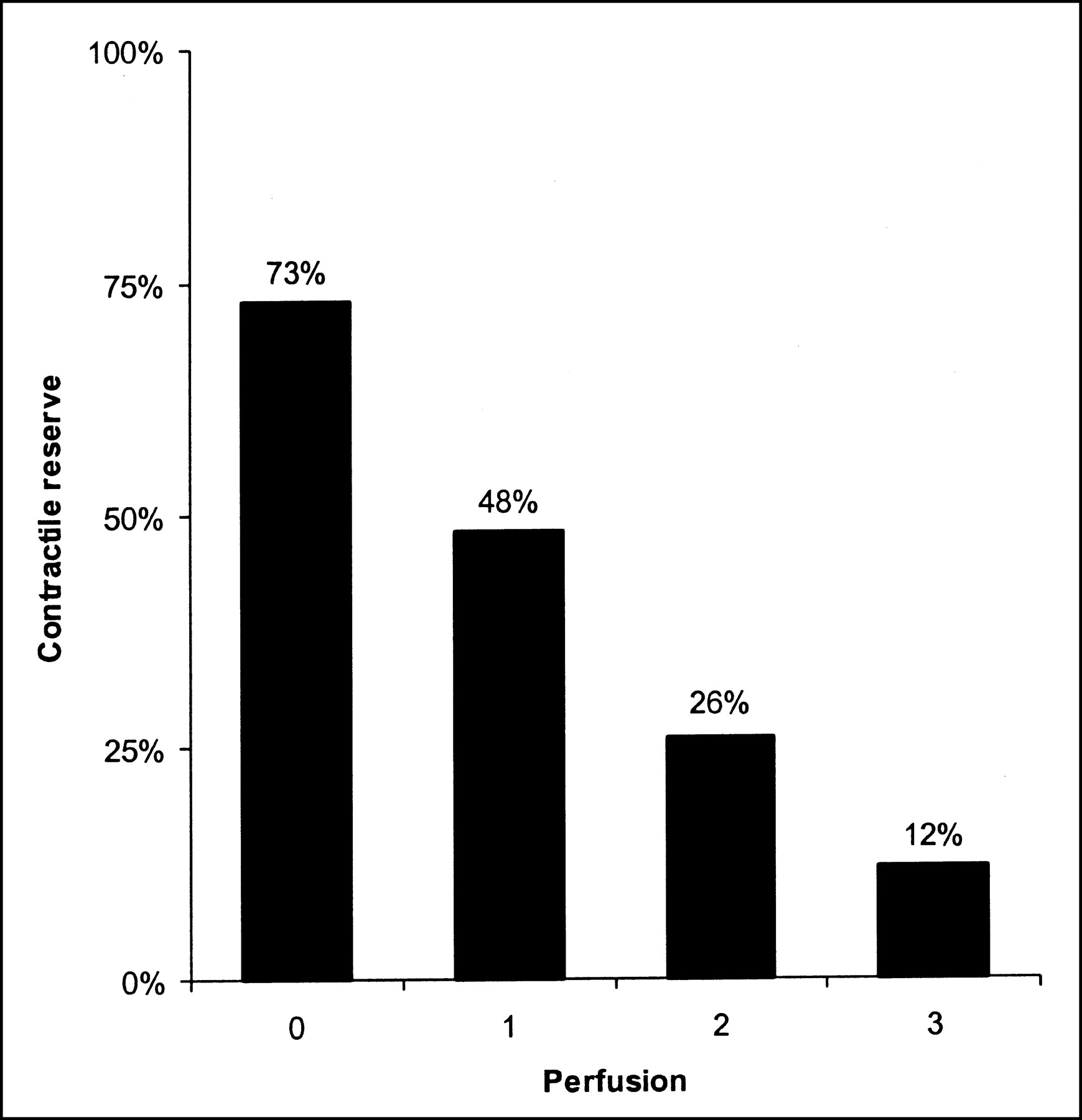
Figure 2 demonstrates the relationship between myocardial perfusion as measured by 99mTc-tetrofosmin and the presence of contractile reserve. Contractile reserve was present in most (73%) of the segments with normal perfusion but was virtually absent from segments with severely reduced or absent perfusion.

Presence of contractile reserve according to resting 99mTc-tetrofosmin perfusion (0 = normal [100% ≥ uptake > 80%], 1 = mildly reduced [80% ≥ uptake > 50%], 2 = moderately reduced [50% ≥ uptake > 25%], 3 = severely reduced or absent [25% ≥ uptake ≥ 0%]).
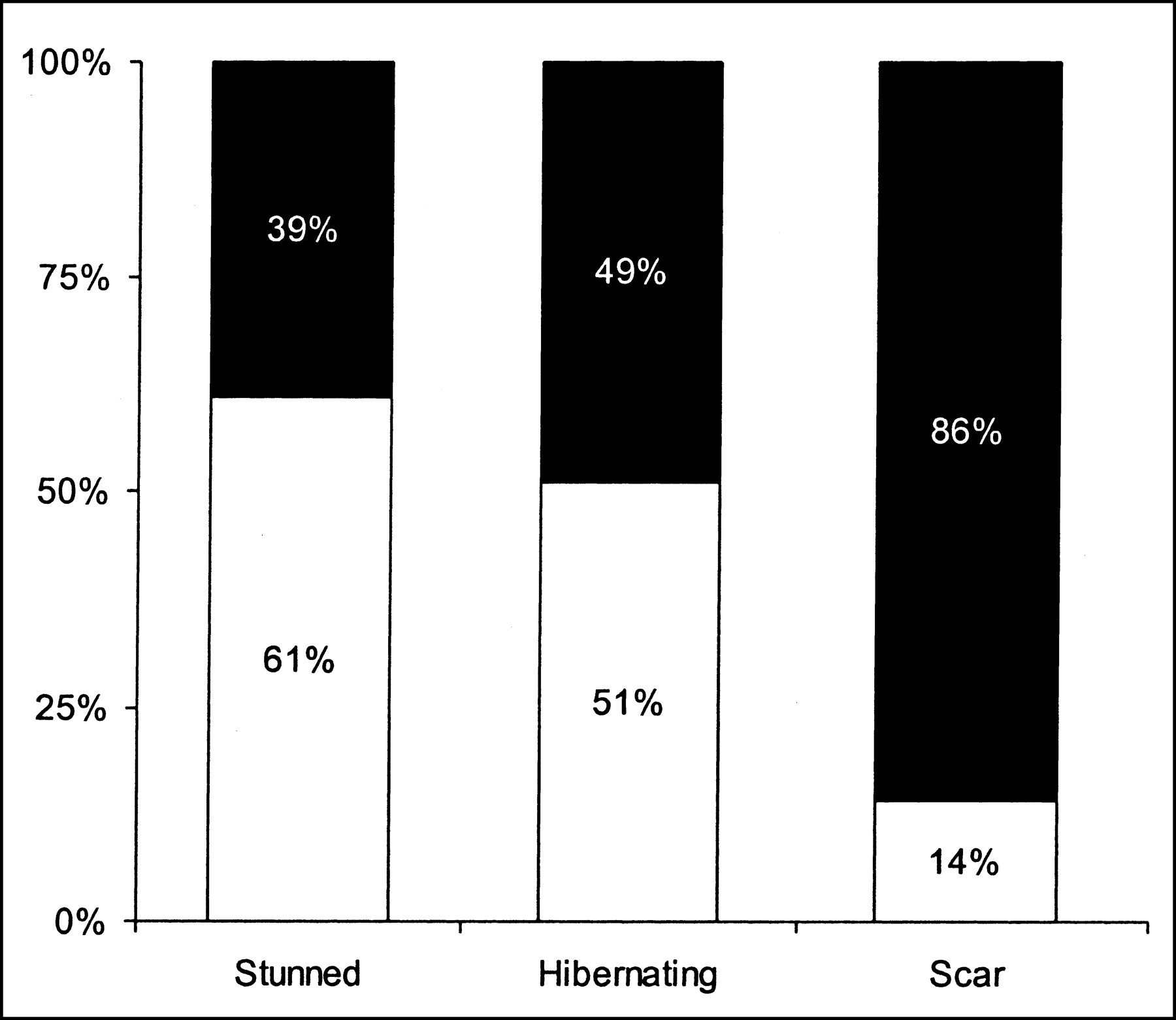
Dobutamine-induced contractile reserve was observed in 519 (59%) of 887 of the dysfunctional segments that were viable (either stunned or hibernating) according to 18F-FDG metabolic imaging. However, contractile reserve was more frequently found in stunned than in hibernating myocardium (407 of 666 [61%] vs. 112 of 221 [51%], respectively; P < 0.01). Only 177 (14%) of the 1,265 scarred segments improved in wall motion during dobutamine infusion; this percentage was considerably less than the percentage of contractile reserve seen in stunned or hibernating myocardium (P < 0.001; Fig. 3). Residual contractile reserve was related to the extent of scar tissue. Figure 4 shows that a contractile response to dobutamine was more frequently observed in nontransmural than in transmural scar tissue.

Segments with (white portions) and without (black portions) contractile reserve in response to dobutamine infusion in stunned, hibernating, and scarred myocardium. Contractile reserve was more frequently found in stunned than in hibernating myocardium (407 of 666 [61%] vs. 112 of 221 [51%], respectively; P < 0.01). Only 177 (14%) of 1,265 scarred segments exhibited contractile reserve; this percentage was considerably less than in stunned or hibernating myocardium (P < 0.001).
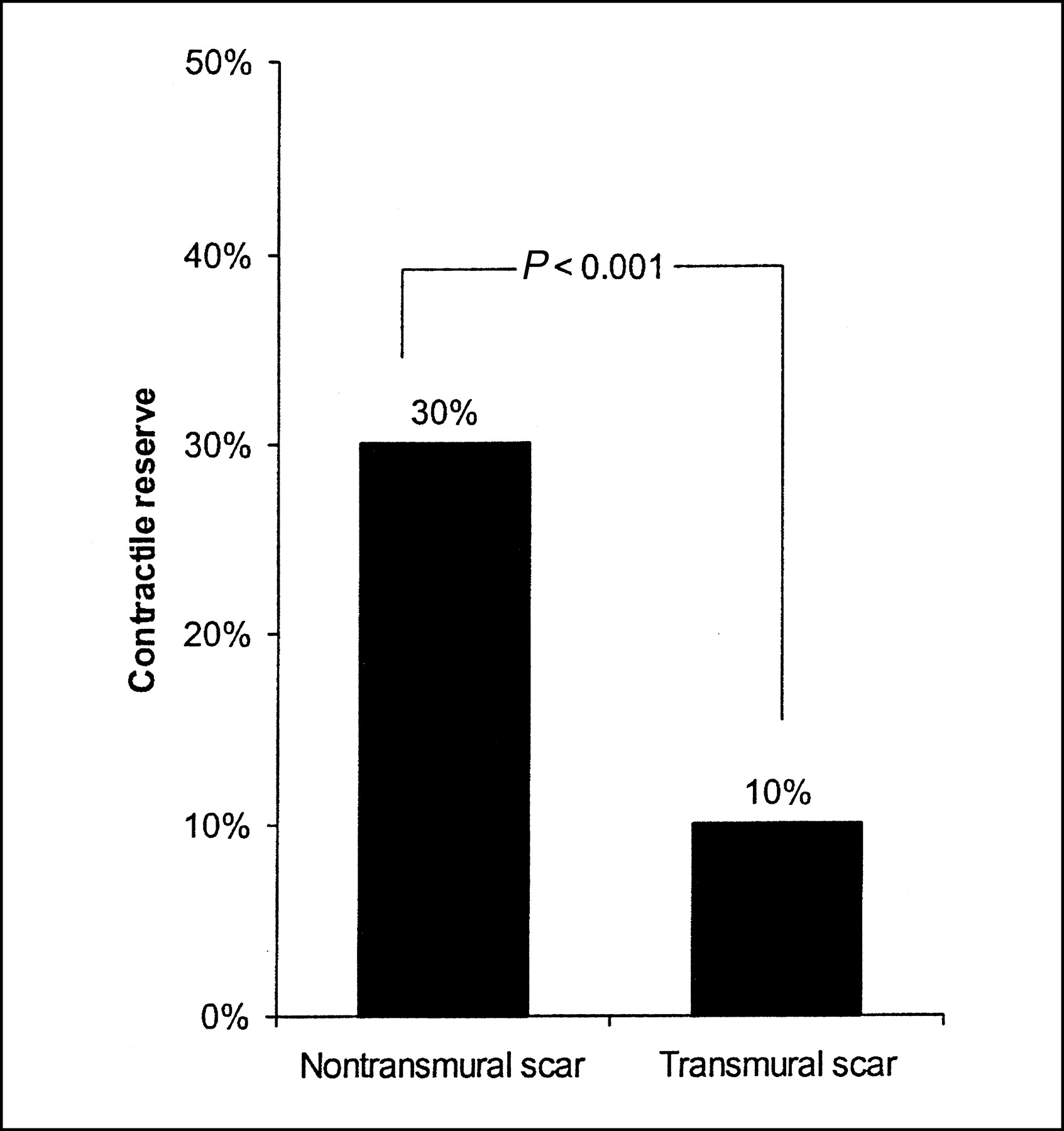
Contractile reserve in nontransmural and transmural scar tissue. Contractile reserve was more frequently observed in nontransmural than in transmural scars (P < 0.001).
Dobutamine Echocardiographic Assessment of Ischemia
During low-dose/high-dose dobutamine echocardiography, 345 segments (16%) showed sustained improvement, 351 (16%) showed a biphasic response, 131 (6%) showed worsening, and 345 (16%) showed no change of wall motion pattern. Hence, myocardial ischemia was present in 482 (22%) of the 2,152 dysfunctional segments. Table 3 demonstrates the patterns of functional response to low-dose/high-dose dobutamine infusion in stunned and hibernating myocardium. The prevalence of the biphasic response and worsening (patterns indicating myocardial ischemia) was similar in stunned and hibernating segments. A sustained improvement of wall motion during dobutamine echocardiography was more frequently observed in stunned than in hibernating myocardium: 217 segments (33%) versus 52 segments (24%) (P < 0.005). Hibernating segments more often showed no change during dobutamine infusion than did stunned segments: 94 segments (43%) versus 206 segments (31%) (P < 0.05).
Functional Response During Low-Dose/High-Dose Dobutamine Infusion
DISCUSSION
In the present study on 198 patients with ischemic cardiomyopathy, dobutamine-induced contractile reserve was observed in 32% of all dysfunctional segments. It was more frequently observed in stunned myocardium than in hibernating myocardium (61% vs. 51%, P < 0.01). Moreover, patients with more severe heart failure less frequently showed contractile reserve than did patients with mild heart failure. Contractile reserve was absent from most scar segments; only 14% of scar segments exhibited contractile reserve. Moreover, residual contractile reserve was also related to the extent of scar tissue; nontransmural scar tissue more often exhibited a dobutamine-induced contractile response than did transmural scar tissue.
In our study, 32% of all dysfunctional segments exhibited contractile reserve. This percentage is in line with previous studies: In a recent meta-analysis (17) of 16 studies involving 448 patients with chronic ischemic left ventricular dysfunction, 1,128 (50%) of 2,268 dysfunctional segments had contractile reserve. The presence or absence of contractile reserve was related to baseline wall motion abnormalities: Contractile reserve occurred more frequently in severely hypokinetic segments than in akinetic segments and was never observed in dyskinetic segments (Fig. 1). Thus, the more severe the wall motion abnormalities, the lower the incidence of contractile reserve. The presence or absence of contractile reserve was also related to resting perfusion: Most segments with normal perfusion exhibited contractile reserve, whereas the incidence of contractile reserve was inversely related to the severity of the reduction in resting perfusion (Fig. 2). Similar findings were reported by Panza et al., who found less contractile reserve in segments with more severely reduced perfusion, as evaluated by PET (18). These observations suggest that more damaged segments (with more severe wall motion abnormalities and lower levels of perfusion) less frequently exhibit contractile reserve.
In this study, segments were divided into stunned and hibernating types on the basis of combined assessment of perfusion and glucose use (3,5–8). Stunned myocardium is thought to have normal resting perfusion, whereas hibernating myocardium may have reduced resting perfusion (5–8). Therefore, in the current study and in other studies (3,5–8), chronic dysfunctional myocardium with normal resting perfusion was considered stunned, whereas segments with a reduced resting perfusion (but with preserved 18F-FDG uptake) were considered hibernating. Using a pig model of chronic hibernation, Fallavolita and Canty (7,8) showed that in dysfunctional myocardium, blood flow was normal at 1–2 mo (indicative of chronic stunning) but was reduced at 3–4 mo (hibernation). These observations suggest a temporal progression from chronic stunning (characterized by normal flow) to hibernation (with a reduced resting flow). It is conceivable that a longer duration of myocardial dysfunction in combination with more severe reductions in myocardial blood flow lead to more extensive myocyte damage. Studies on patients with ischemic cardiomyopathy have shown structural dedifferentiation of cardiac myocytes in biopsy samples obtained at the time of coronary revascularization (6,19,20). Hibernating myocardium showed a loss of contractile filaments (sarcomeres), an accumulation of glycogen in the spaces previously occupied by the myofilaments, nuclei with uniformly distributed chromatin, small mitochondria, and a nearly absent sarcoplasmic reticulum (6,19,20). For these reasons, it is anticipated that contractile reserve may be less frequently present in hibernating myocardium than in stunned myocardium. Indeed, studies on small groups of patients have indicated that contractile reserve was less frequently preserved in hibernating myocardium than in stunned myocardium (21,22). In the current study on a large group of patients, contractile reserve was present in 61% of stunned segments, compared with 51% of hibernating segments. Moreover, patients with severe heart failure less frequently exhibited contractile reserve than did patients with mild heart failure. These observations provide further evidence that more severe damage results in loss of contractile reserve. In these segments, viability may still be maintained (as evidenced by the preserved glucose use in some of these segments).
From a clinical point of view, the most important question is the potential for improvement of contractile function in segments with hibernation but without contractile reserve (the segments that are thought to be more severely damaged). These segments are indeed damaged more severely, as was demonstrated by Pagano et al. (23). Those authors studied 22 ischemic cardiomyopathy patients with 18F-FDG PET and low-dose dobutamine echocardiography. Transmural biopsies were obtained during bypass surgery, and the relationship between the histologic findings and the 18F-FDG PET and dobutamine echocardiographic data was evaluated. Segments with preserved 18F-FDG uptake but without contractile reserve appeared more damaged (higher extent of myofibrillar loss) than did segments with preserved 18F-FDG uptake and contractile reserve. Segments with hibernation but without contractile reserve are frequently observed in patients with ischemic cardiomyopathy (up to 30%–40%) (24,25). Currently, no data are available on recovery of function in these segments. However, we recently demonstrated that recovery of function may take longer for hibernating myocardium than for stunned myocardium (26). Thus, recovery of more severely damaged myocardium is likely to take longer. Whether there is a point of no return (when damage is too much) needs further study. More severely damaged myocardium less frequently exhibits contractile reserve, but recovery of function should not be excluded; therefore, these patients may still be candidates for revascularization. However, the use of definitions (stunning, hibernation, nontransmural scar, transmural scar) is to some extent artificial. These pathophysiologic states represent a continuum of disease, and grouping is difficult. Still, for a clinically meaningful interpretation and comparison with the existing literature, the definitions were used.
In the current study, the presence of contractile reserve was also evaluated in scar tissue. Of all segments with scar tissue (as established by combined perfusion–18F-FDG imaging), only 14% had contractile reserve. In segments with transmural scars, it was virtually never observed, whereas a substantial percentage of segments with nontransmural scars did exhibit contractile reserve. This finding is not surprising, since segments with nontransmural scars contain a substantial amount of normal, viable tissue (located epicardially). This tissue responds well to dobutamine infusion and explains the observed improved contraction. The resolution of echocardiography does not allow discrimination of these endocardial and epicardial layers, but recent studies with MRI have demonstrated the superior resolution of this technique (27), enabling the detection of “epicardial” contractile reserve in subendocardial scars (28). Although these segments are not likely to improve in contractile function after revascularization, they may be important in the prevention of remodeling and, thus, long-term prognosis.
CONCLUSION
Left ventricular dysfunction in patients with ischemic cardiomyopathy is often caused by myocardial stunning, hibernation, and scar tissue. The results of this study show that dobutamine-induced contractile reserve was more often found in stunned than in hibernating myocardium. In contrast, contractile reserve was virtually absent from scarred myocardium. Nontransmural scar tissue more often exhibited contractile reserve than did transmural scar tissue. This progressive reduction of contractile reserve in stunned, hibernating nontransmural and transmural scar tissue supports the hypothesis that stunning, hibernation, and scarring are not circumscript pathophysiologic entities but represent gradual ultrastructural damage on the myocyte level. Further studies are needed to determine the clinical relevance (in terms of the effect on long-term prognosis) of these different segments.
Footnotes
Received May 2, 2002; revision accepted Sep. 17, 2002.
For correspondence or reprints contact: Don Poldermans, MD, PhD, Department of Cardiology, Erasmus Medical Center, Thoraxcenter Room Ba 300, Dr. Molewaterplein 40, 3015 GD Rotterdam, The Netherlands.
E-mail: poldermans{at}hlkd.azr.nl




{kind=link}
{kind=link}
{kind=link}
{kind=link}