


Abstract
Noninvasive cardiac imaging is now central to the diagnosis and management of patients with known or suspected chronic coronary artery disease (CAD). Although rest echocardiography has become the most common of the techniques, nuclear cardiology and more recently cardiac computed tomography (CCT) and cardiac magnetic resonance (CMR) play important roles in this regard. This review examines the current applications and interactions of noninvasive cardiac imaging approaches for the assessment of patients with suspected CAD. In addition to considering the strengths and weaknesses of each technique, this review attempts to provide a guide to the selection of a test (or tests) that is based on the question being asked and the ability of each test to answer this question. In patients with suspected CAD, the pretest likelihood of disease, a clinical assessment, becomes the most important determinant of the initial test. If the likelihood is very low, no testing is needed. However, if the likelihood is low, recent data suggest that assessment of early atherosclerosis is likely to be the most useful and cost-effective test. In patients who have an intermediate likelihood of CAD, nuclear cardiology with myocardial perfusion SPECT (MPS) becomes highly valuable; however, coronary CT angiography (CTA), with fast 16-slice or greater scanners, may emerge as the initial test of choice. MPS would then be used if the CTA is inconclusive or if there is a need to assess the functional significance of a stenosis defined by CTA. Coronary CTA, however, is not yet widely available and is limited in patients with dense coronary calcification. In older patients with a high likelihood of CAD, MPS may be the initial test of choice, since a high proportion of these patients have too much coronary calcium to allow accurate assessment of the presence of coronary stenoses. PET/CT or SPECT/CT could emerge as important modalities combining the advantages of each modality. While CMR has great promise as a radiation-free and contrast-free “one-stop” shop, it currently lags behind CTA for noninvasive coronary angiography. Nonetheless, CMR clearly has the potential for this application and has already emerged as a highly effective method for assessing ventricular function, myocardial mass, and myocardial viability, and there is increasing use of this approach for clinical rest and stress perfusion measurements. CMR is particularly valuable in distinguishing ischemic from nonischemic cardiomyopathy. While CT and CMR are likely to grow considerably in diagnostic evaluation over the next several years, MPS and PET will continue to be very valuable techniques for this purpose.
- cardiac computed tomography
- cardiac magnetic resonance
- coronary artery disease
- myocardial perfusion SPECT
Noninvasive cardiac imaging is now central to the diagnosis and management of patients with known or suspected chronic coronary artery disease (CAD). Although rest echocardiography has become the most common of the techniques, nuclear cardiology and more recently cardiac computed tomography (CCT) and cardiac magnetic resonance (CMR) play important roles in this regard. This review examines the current applications and interactions of noninvasive cardiac imaging approaches.
Which of these methods is most appropriate as the initial test depends on the clinical question being asked. Among asymptomatic patients or those with nonanginal symptoms with a relatively low likelihood of CAD, the clinical question frequently revolves around the presence of subclinical coronary atherosclerosis for delineation of long-term risk for developing clinical CAD. The answer to this question will help determine who needs aggressive medical management. But as a priori risk for cardiac disease increases, a second question becomes increasingly important: “What is the shorter-term risk of myocardial infarction (MI) or cardiac death?”—a question that appears to be best answered by determining the extent and severity of inducible ischemia. In all stages of atherosclerosis, it would be desirable to be able to evaluate the effects of therapy noninvasively. Then, as the stage of disease progresses and extensive ventricular dysfunction develops, the question frequently becomes: “Is improvement in ventricular function, survival, or symptoms likely with surgical intervention or should surgical reshaping of the left ventricle be performed?” Here the answer may depend on the extent of viable and nonviable myocardium.
ASSESSMENT OF SUBCLINICAL ATHEROSCLEROSIS BY CORONARY CALCIUM SCANNING
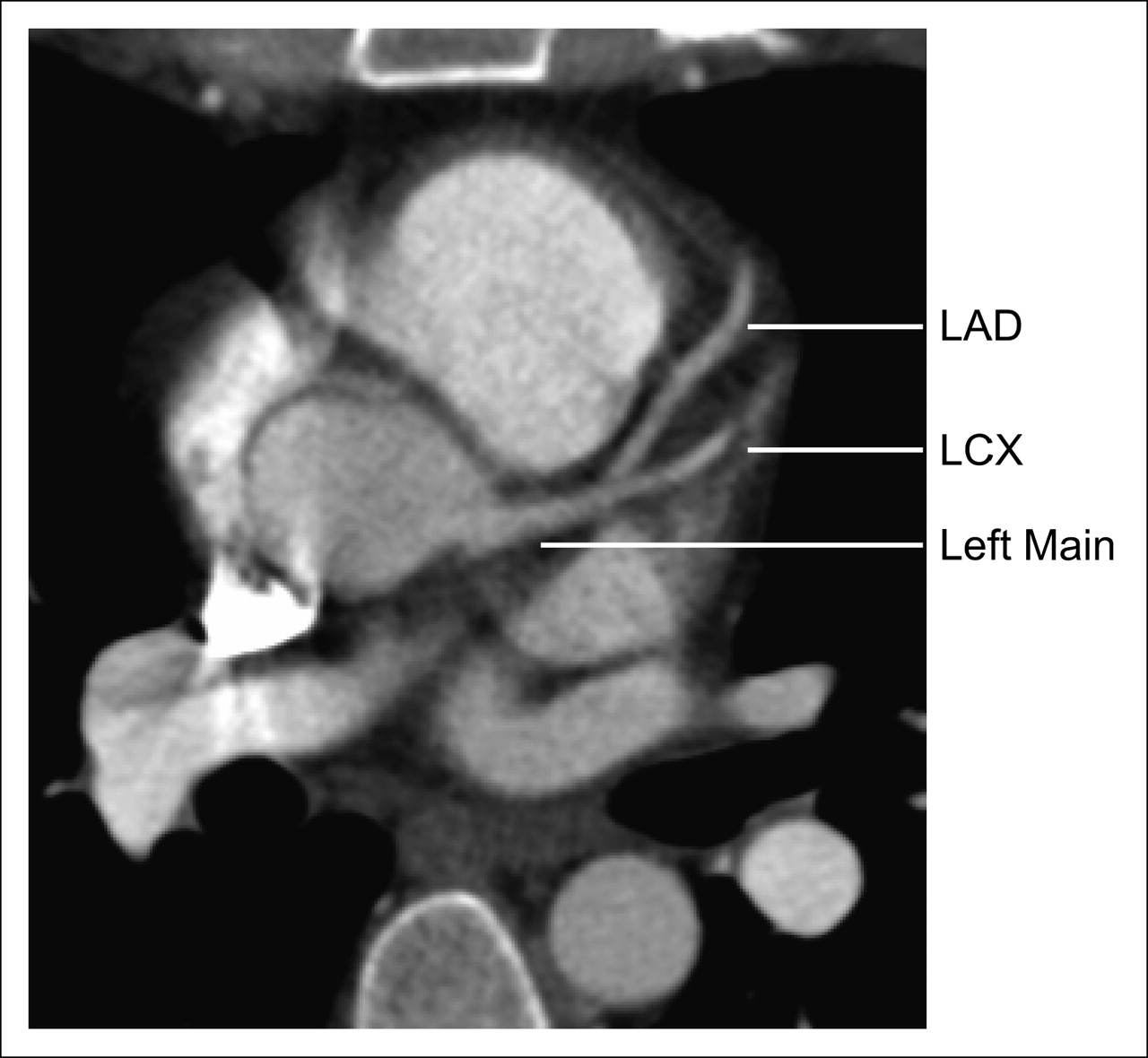
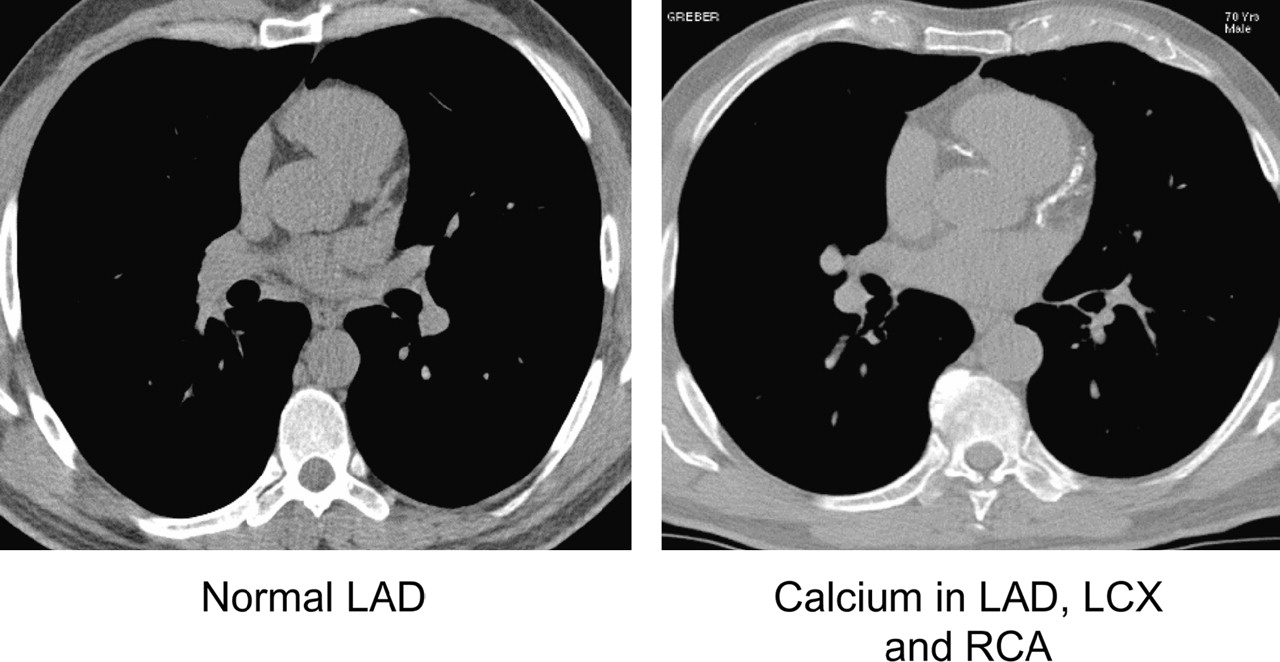
Vascular calcification has been associated with atherosclerosis since the 1920s (1). In 1959, Blankenhorn and Stern described the importance of coronary artery calcium (CAC) as a marker of coronary atherosclerosis (2). For many years, the assessment of CAC using fluoroscopy was recognized as providing clinically useful information. In fact, Diamond et al. incorporated a subjective fluoroscopic assessment of CAC into their original algorithm for assessing the likelihood of angiographically significant CAD by Bayesian analysis (3). The advent of CT provided a technique that was potentially quantifiable, avoiding the subjectivity of fluoroscopy. Though CAC measurements were first described using electron beam CT (EBT), investigators are increasingly recognizing that recent-generation multislice CT (MSCT) and EBT provide comparable measurements for practical clinical purposes (4,5). In standard practice, the presence and extent of coronary calcium is expressed by the Agatston coronary calcium score (CCS), related to the extent and the density of calcification in the coronary tree. Examples of coronary calcium scans obtained with EBT are shown in Figure 1.

Examples of normal and abnormal coronary calcium scans obtained by electron beam tomography. LAD = left anterior descending coronary artery; LCX = left circumflex artery; RCA = right coronary artery.
When measuring coronary calcium by CT, the scoring of these scans typically involves a reproducible semiautomatic computer method. The CCS is defined for each focus of calcium in the coronary tree, with areas containing calcium being defined by having Hounsfield units (HU) >130. The software calculates lesion-specific scores as the product of the area of each calcified focus and peak CT number (scored as 1 for 131–199 HU, 2 for 200–299 HU, 3 for 300–399 HU, and 4 for ≥400 HU) according to the method of Agatston et al. (6). These are summed across all lesions identified in the coronary arteries to provide the total CCS.
In common practice, this score is often also expressed as a coronary calcium percentile score based on age and sex using one of many available databases (7–9). Though initially developed for EBT, methods for approximating the density-weighted Agatston score using MSCT have been developed. Most of the available software programs also often provide a calcified volume score developed by Callister et al. (10), which has been reported as more useful for following the progression (or regression) of the calcification over time (11). With the use of calcium phantoms as standards, the mass of calcium in the coronary tree can also be accurately measured by EBT or MSCT. Given the large number of publications using the Agatston score, it is not likely that this score will be replaced by volume or mass scores any time soon.
EARLY DETECTION AND QUANTIFICATION OF CORONARY ATHEROSCLEROSIS
Role of Coronary Calcium Scanning
Assessment of the presence of subclinical coronary atherosclerosis provides an opportunity to identify asymptomatic patients who are at risk for developing clinical coronary heart disease (CHD) over the long term. While consideration of conventional risk factors for atherosclerosis—such as increased serum cholesterol levels, hypertension, smoking, and so forth—play a role in the overall assessment, this approach does not provide an actual marker of the pathologic disease state. Conventionally, these risk factors are aggregated into a global score of risk such as the Framingham Risk Score (FRS), which is expressed as a number reflecting the likelihood of CHD death or nonfatal MI over a 10-y period (12). The FRS has been proposed as a guide to risk assessment and the need for aggressive antiatherosclerotic treatment among asymptomatic patients, but this algorithm, developed in healthy epidemiologic cohorts, has not been widely tested as a screening algorithm among patients typically eligible for cardiac stress testing. Moreover, the FRS does not take into account family history of early heart disease, of known importance but not accurately recorded in the initial FRS database, as well as other factors (such as visceral obesity), which might be of importance for certain patients. It frequently underestimates long-term risk in women (13,14). As an alternative, coronary calcium scanning or carotid intima–media thickness (IMT) measurements using ultrasound (15,16) have become increasingly used to screen for atherosclerosis among patients with a relatively low likelihood of hemodynamically significant CAD.
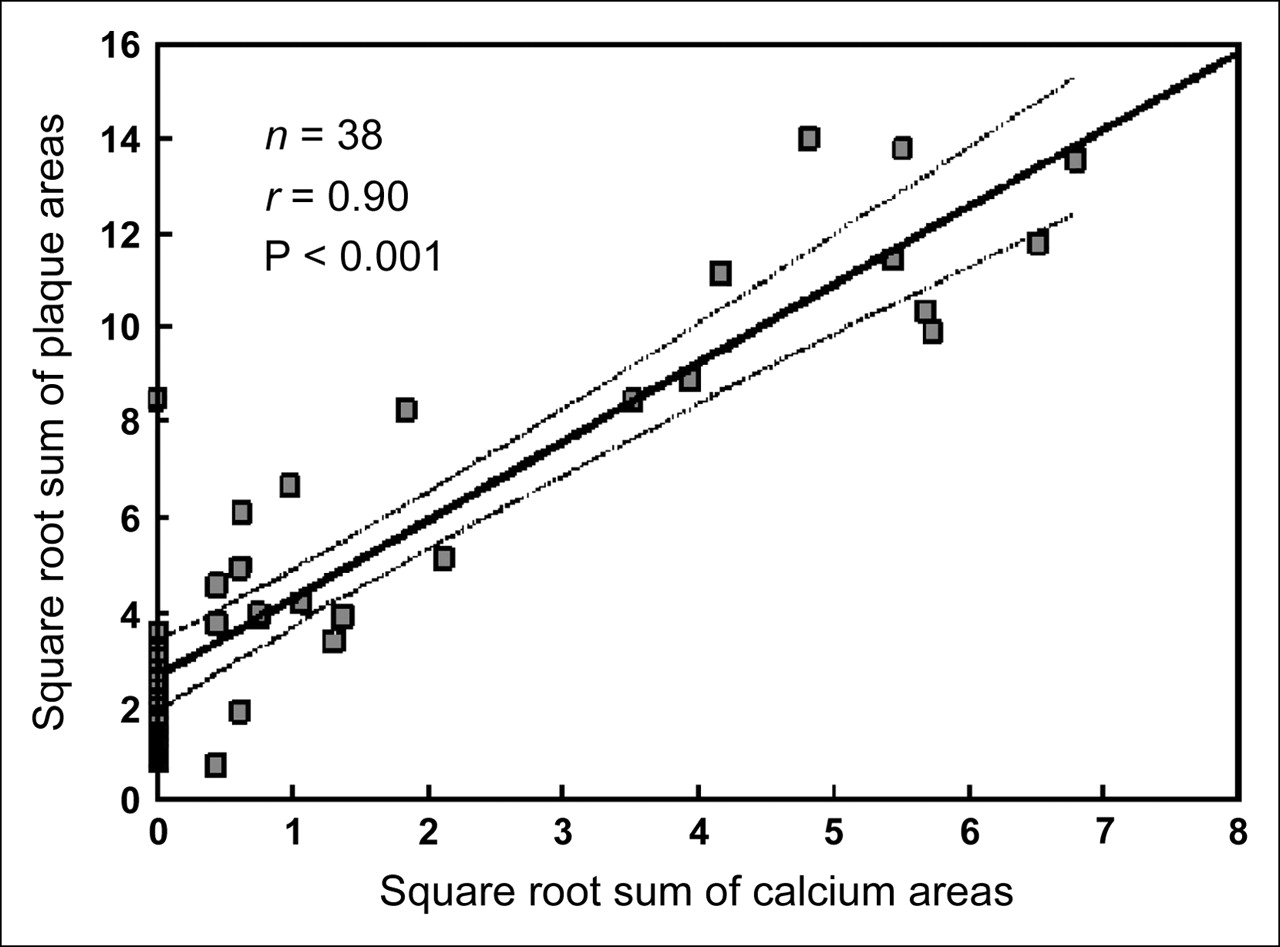
From the currently available information, in a Bethesda conference on imaging of coronary atherosclerosis (17), it was concluded that CT CAC provides the most accurate method currently available for the early detection of coronary atherosclerosis. The amount of coronary calcium correlates strongly with the overall amount of coronary plaque (calcified and noncalcified) as determined at postmortem examination (18) (Fig. 2). This correlation implies that approximately 80% of plaque is noncalcified and 20% is calcified in the untreated patient. While microscopic calcification of coronary plaque appears very early in the atherosclerotic process, macroscopic calcification (the amount required for detection by the EBT/MSCT) occurs after a period of cholesterol and inflammatory cell accumulation, apparently representing “bone” formation to wall off the inflammatory process (19). Nonetheless, it is very uncommon for extensive atherosclerosis to be present without any evidence of calcification on the coronary CT scan. Of note, in preliminary work, only 1 of 276 patients scanned before admission with a suspected acute coronary syndrome was then found to have an acute syndrome in the absence of coronary calcium by EBT (20).
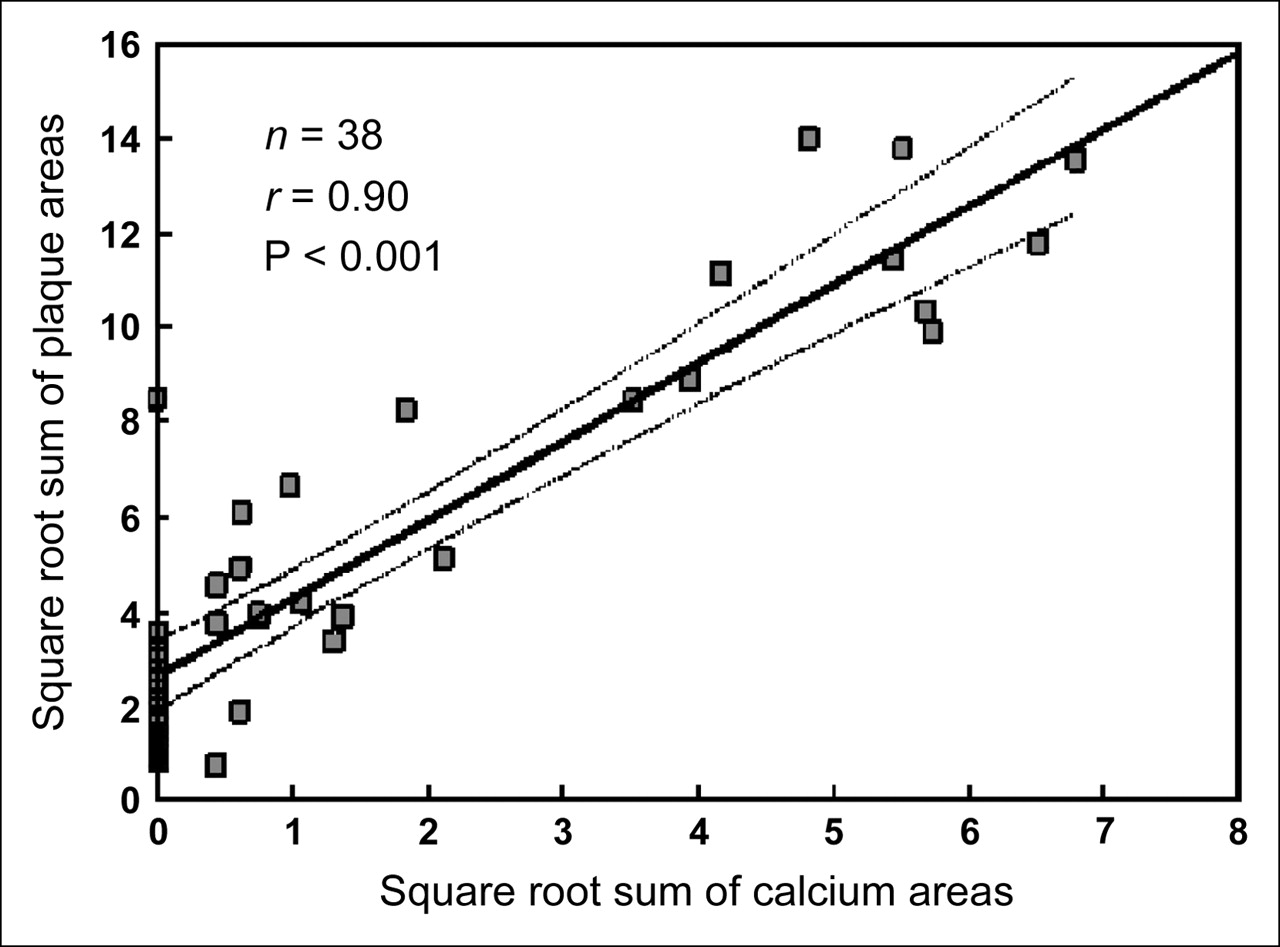
Relationship between coronary calcium areas (mm) by electron beam tomography and atherosclerotic plaque areas by postmortem examination for each individual coronary artery in patients who died of noncardiac cause. (Adapted with permission from (18).)
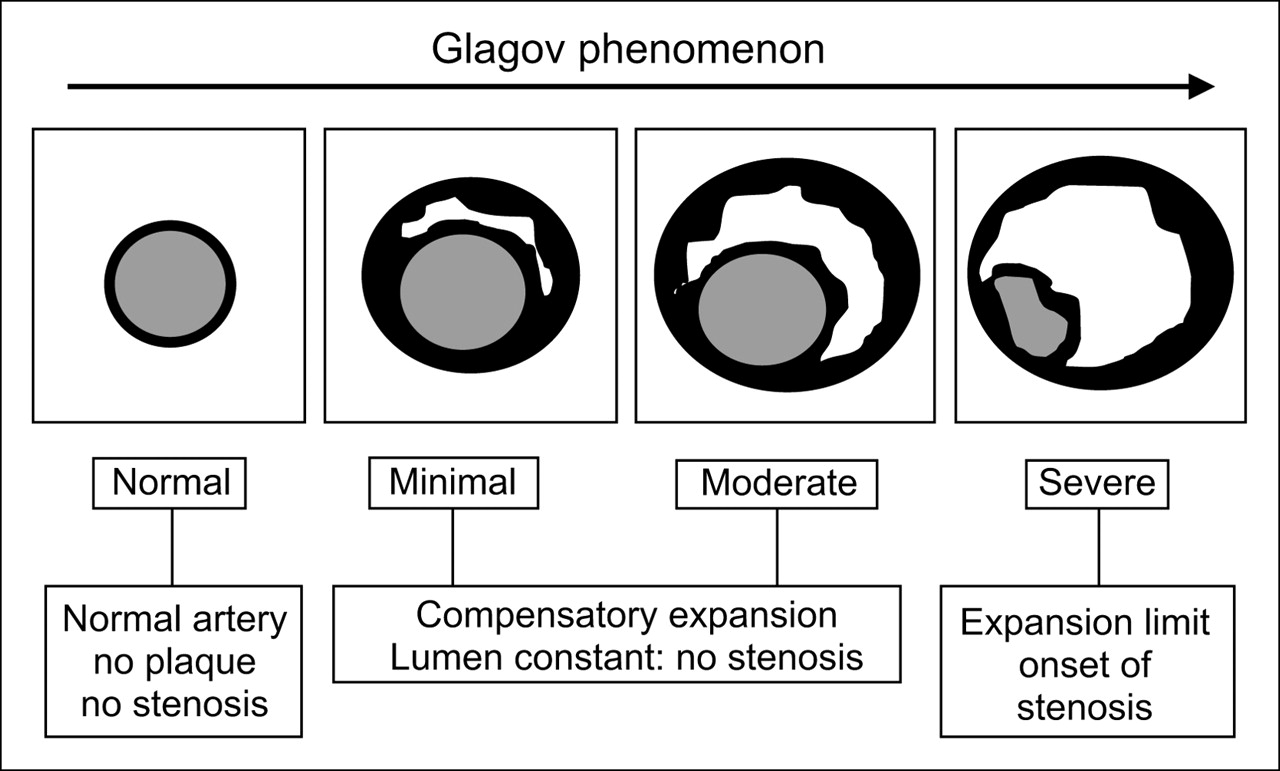
It became clear from the early coronary calcium scanning experience that, although CAC was almost always present in the presence of angiographically significant CAD (≥50% stenosis), CAC had low specificity—that is, calcification implies atherosclerosis but not necessarily the presence of a stenosis. This phenomenon is explained by a process referred to as the Glagov phenomenon (21) (Fig. 3). Characteristically, in the early stages of coronary atherosclerosis, and often in the more advanced stages, plaque accumulation produces an outward remodeling (expansion) of the external elastic membrane. During this phase, there is little or no encroachment of the plaque on the vascular lumen. In simplistic terms, in most circumstances, only after maximal outward remodeling does a narrowing of the lumen develop. Because of this process, there is only a weak relationship between plaque burden and the percentage of the coronary artery tree supplied by vessels with >50% stenosis. However, if more mild luminal narrowing is considered—for example, the number of segments demonstrating ≥20% stenosis by coronary angiography—the total CCS, as determined from EBT, has been shown to correlate strongly with the angiographic extent of atherosclerosis (r = 0.77) (22). Thus, assessment of coronary calcium allows detection of atherosclerotic lesions often long before they become hemodynamically significant.

Diagrammatic representation of progression of atherosclerosis as described by Glagov et al. (21). White area indicates presence of plaque, without consideration of distinction between calcified and noncalcified plaque. Positive remodeling during minimal and moderate phases of plaque buildup can occur without compromise of lumen. However, as plaque volume becomes large, the artery no longer enlarges at a rate sufficient to prevent narrowing of the lumen. Although this is a highly simplified illustration of a complex and variable process, this phenomenon is the likely explanation for the observation that the vast majority of calcified coronary plaques are not associated with coronary stenosis (Adapted with permission from (21).)
In contrast, stress nuclear cardiology techniques (as with all stress imaging methods) require the presence of a hemodynamically significant lesion, either fixed or dynamic, before an abnormality becomes evident. In the above study (22), without the CCS, stress myocardial perfusion SPECT (MPS) provided significant information for the prediction of the number of segments with ≥20% maximal coronary stenosis at angiography, along with age, male sex, and cholesterol measurements in a multivariate model. However, once the CCS was known, the radionuclide perfusion score and conventional risk factors were no longer a significant predictor. Although this study represents only one of several studies that have shown that the CCS provides independent and incremental information over risk factors for predicting the extent of angiographic CAD, it gives insight into the perceived discordance between angiographic and CAC results and is illustrative of the concept that the presence of CAC is expected to be more sensitive than MPS or even the angiographic gold standard in the detection of early coronary atherosclerosis. Table 1 summarizes the implications of coronary calcium measurements by EBT/MSCT for early detection and quantification of coronary atherosclerosis.
Early Detection and Quantification of Atherosclerosis
Role of MPS
The diagnostic applications of noninvasive stress testing (i.e., their use to detect the presence of CAD) are based on the ability to detect a hemodynamically significant anatomic endpoint: a flow-limiting coronary stenosis, either fixed or dynamic, generally defined as ≥50% diameter stenosis (translating to a 75% cross-sectional area reduction). This criterion is operationally important to invasive cardiologists as it is considered to represent a minimal criterion for the consideration of revascularization with either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG).
By current guidelines (23), the consideration of using a stress imaging study is preceded by assessment of the pretest likelihood of CAD. Specifically, before stress testing, the likelihood of CAD can be assessed by Bayesian analyses of patient age, sex, risk factors, and symptoms, as initially developed by Diamond and colleagues (3,24). Patients with an intermediate likelihood of CAD after the analyses of the above factors have been considered the best candidates for stress testing (with or without imaging). Patients reclassified as low-likelihood patients after stress testing will still require modifications of coronary risk factors, which may follow along either primary or secondary prevention guidelines. Patients who are reclassified as having a high likelihood of CAD after stress testing may become appropriate referrals for cardiac catheterization depending on the magnitude of inducible ischemia on stress testing. There is no consensus as to the exact range for this intermediate likelihood, with various recommendations ranging from 10%–90% to 30%–70%. This diagnostic application has resulted in class I indications in the recent American College of Cardiology/American Heart Association/American Society of Nuclear Cardiology (ACC/AHA/ASNC) guidelines (25). Patients with an initially high likelihood of CAD before stress testing are unique in that the question regarding them is not diagnostic but rather prognostic: Are they of sufficient risk to merit aggressive intervention? As a consequence, such high-likelihood patients also commonly benefit from MPS as the next step in their clinical evaluation, because a normal MPS study identifies them as low-risk patients relative to cardiac events (26,27). Conversely, the more abnormal the MPS study is, the greater the likelihood is that a patient would benefit from revascularization (e.g., PCI, CABG) (28).
This approach is embodied in multiple ACC/AHA guidelines in which stress testing, with or without stress imaging, is considered a class I indication in many patients with an intermediate likelihood of CAD, but a class IIb indication (usefulness or efficacy is less well established by evidence or opinion) for diagnostic testing in patients with either high or low pretest probability of CAD (23,25,29,30).
Role of CCS
The coronary calcium scan can also be considered with regard to its ability to detect angiographically significant CAD—not only the ability to detect early atherosclerosis. In this regard, the presence of any coronary calcification has been shown to have a sensitivity of 95% after correction for verification bias, based on a CAC score >0 (31). In the largest single study to date, the sensitivity has been reported to be 99%, with equally high sensitivity in both sexes in a study of 1,764 consecutive patients being referred for coronary angiography because of clinical reasons (32). This implies that many patients with a CAC score of 0 might be spared from unnecessary coronary angiography if there are no symptoms or signs of the presence of disease. An approach that incorporates age, sex, and CCS in prediction of the likelihood of angiographically significant CAD has been described (31), and the approach could be further refined by incorporation of the presence or absence of chest discomfort and its type as well as the results of stress testing. In general, if the pretest likelihood of CAD is <50%, a CAC score of 0 provides very strong evidence against the presence of CAD and can be used confidently for clinical decision making.
Unlike an abnormal MPS, however, the presence of coronary calcium alone is not an accurate prediction of angiographically significant stenosis because the specificity of CCS for defining obstructive CAD (i.e., 50% stenosis) is low. Extensive atherosclerosis is known to occur before there is any luminal encroachment by the plaque as explained by the Glagov phenomenon (21). Although the higher the CCS is, the greater the likelihood is of angiographically significant CAD (32), and though the incorporation of age and sex can improve the angiographic predictions, asymptomatic patients even with a very high CCS (i.e., >1,000) are generally referred for stress imaging rather than for catheterization in the absence of other evidence of ischemia.
Role of CT Coronary Angiography
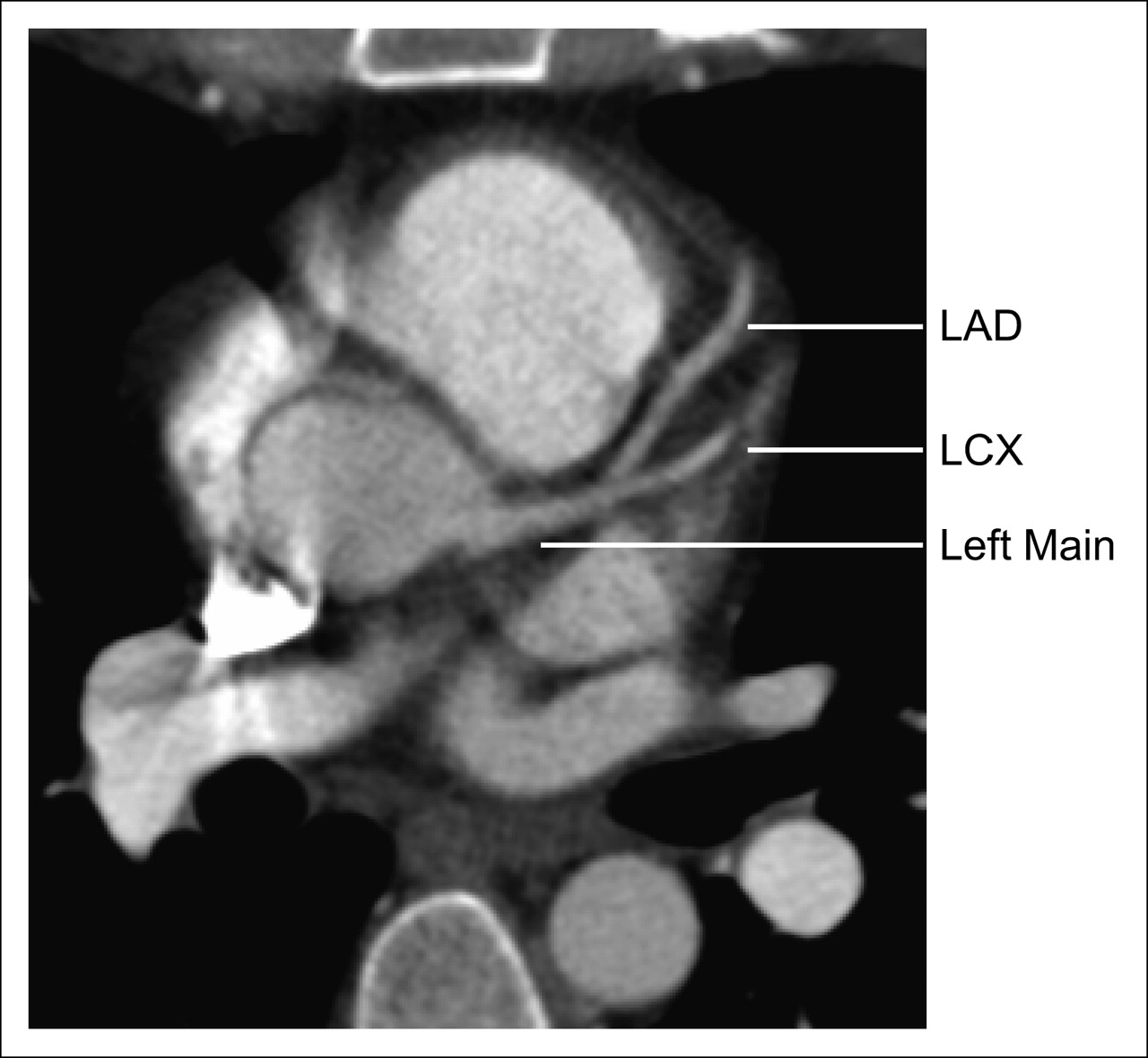
Beyond its use in assessment of coronary calcium, cardiac CT is increasingly being used for noninvasive CT coronary angiography (CTA), which has a high sensitivity and specificity for detecting coronary stenosis (33–35). Though virtually all EBT scanners and most recent-generation MSCT scanners are capable of the CCS measurements, coronary CTA is more technically demanding. At the present time, it appears that further development of the EBT scanners will not be pursued by industry in the near future. Current EBT scanners are limited in their z-axis resolution (1.5 mm), diminishing their value for coronary CTA. On the other hand, with 16-slice or greater MSCT scanners operating with rotation times of ≤420 ms, clinically useful results have been reported with coronary CTA. Because tomography with CT requires approximately 210° acquisition (slightly more than SPECT), the fastest of the currently available scanners operating at a 330-ms rotation time has a single-beat acquisition time of approximately 180 ms. With heart rates of <65 beats/minute (usually through the use of β-blockers) and regular rhythm, this speed is associated with minimal coronary artery motion. The 16-slice or greater scanners produce images with isotropic voxels. Investigations showing approximately 90% sensitivity and 90% specificity for >50% coronary stenosis have been consistently reported with 16-slice scanners (36–39), in selected patient groups (see limitations below). In 2004, 64-slice MSCT was introduced for routine clinical use, and in 2005 the 4 major manufacturers had commercially available 64-slice scanners with spatial resolution of 0.4 mm. Several abstracts and manuscripts have documented that the 64-slice approach also results in very high sensitivity and specificity for CAD and it appears to be associated with a smaller number of uninterpretable segments due to motion or the presence of coronary calcium (40–42). With the 64-slice scanners, covering between 20 and 40 mm with each rotation, fewer heart beats are required for acquisition, and contrast volumes of <100 mL are routine. The low-contrast dose reduces problems associated with higher contrast loads in terms of potential nephrotoxicity—of particular concern if the CT findings result in diagnosis of a condition that requires urgent contrast coronary angiography and the need for more contrast. The entire coronary CTA procedure can be performed in approximately 10 min, and rapid reconstruction possible with new computer systems makes the study immediately available for final interpretation. Of additional note, coronary CTA can visualize not only the vessel lumen but also the wall, allowing the noninvasive assessment of the presence and, potentially, the size of noncalcified coronary plaque (43). Also, the assessments possible from a single first-pass acquisition of the chest CT data can be expanded to include assessment of ventricular function. Potentially, this approach can also become of value in the emergency department setting and has the potential to provide assessments of pulmonary embolism, acute coronary syndrome, and aortic dissection in a single study (i.e., “triple rule-out”). Figure 4 shows an example of normal 16-slice coronary CTA from our laboratory, and Figure 5 illustrates a published 16-slice example of coronary stenosis (38).
Example from our laboratory of normal coronary CTA using 16-slice MSCT scanner (Philips). LAD = left anterior descending coronary artery; LCX = left circumflex artery.
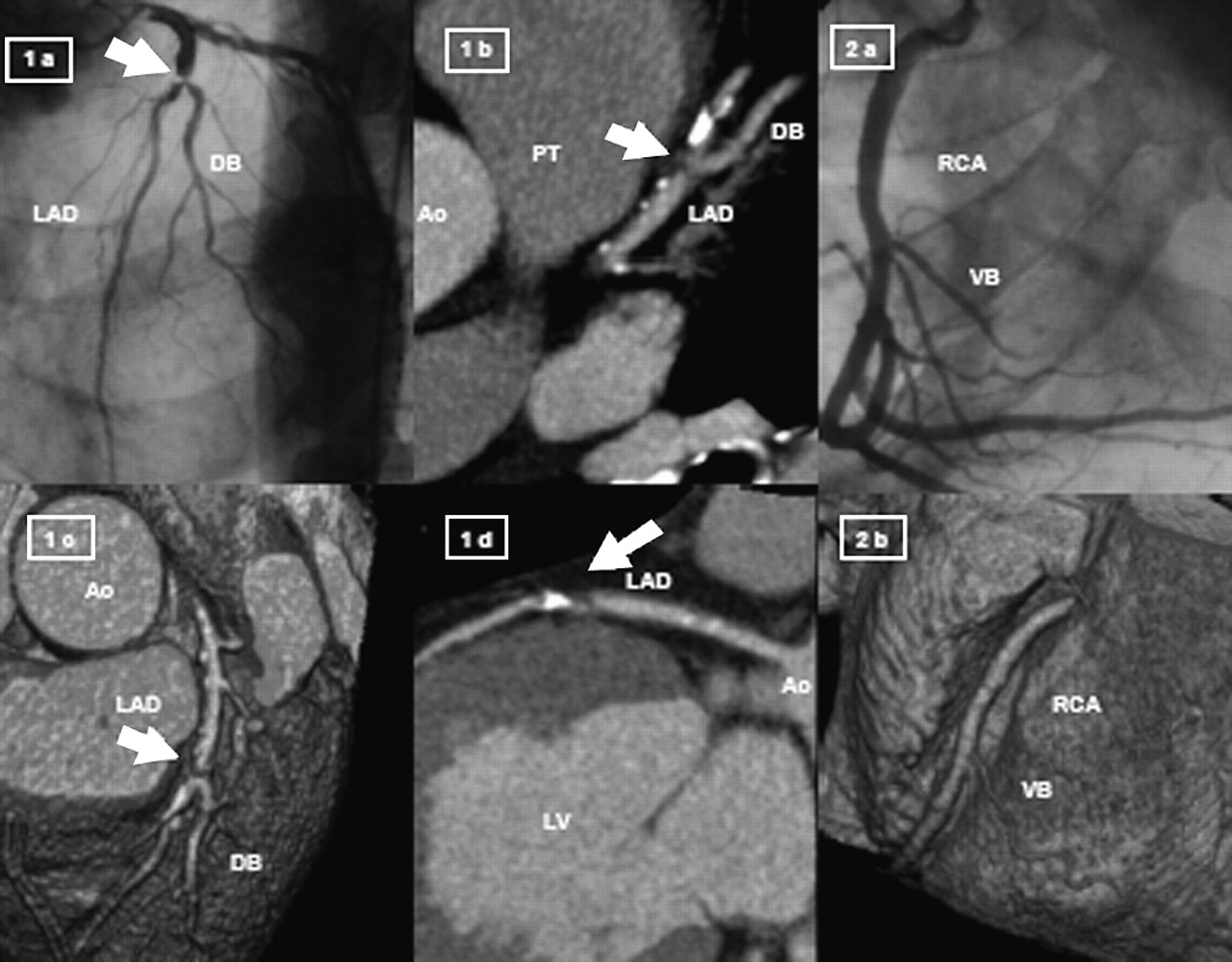
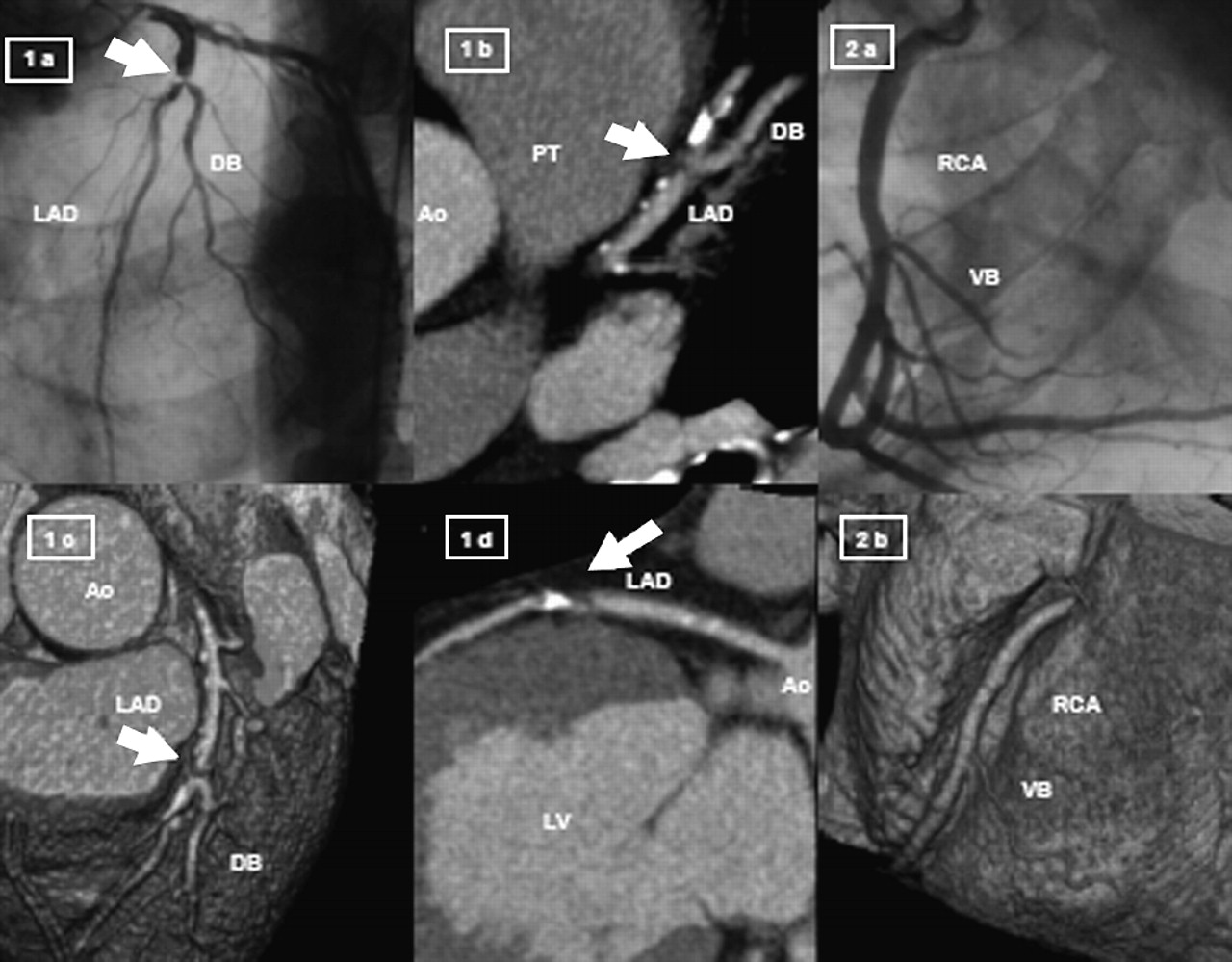
Published example of 16-slice CTA (Siemens) in 49-y-old male with chest pain and ischemic exercise electrocardiography. CTA revealed left anterior descending artery (LAD) stenosis and normal right coronary artery (RCA). (1a) Coronary angiography showing severe lesion in LAD. (1b) A volume-rendering technique of RCA (MDCT) axial slice visualizing high-grade lesion. (1c) MDCT 3-dimensional volume-rendering technique. (1d) MDCT curved multiplanar reconstruction. (2a) Coronary angiography of RCA. (2b) MDCT volume-rendering technique of RCA. Ao = aorta; DB = diagonal branch; LV = left ventricle; PT = pulmonary trunk; VB = ventricular branch. (Adapted with permission from (38).)
Although the relationship between CCS and MPS is fairly well understood, the relative roles of MPS and CTA have not yet been defined. Given what appears to be a higher sensitivity and specificity of coronary CTA than of MPS, it may be that coronary CTA will produce dramatic changes in the approach to diagnosis in the patient with an intermediate likelihood of CAD. Coronary CTA may well become the preferred initial test in these patients, with MPS serving more of a secondary test role. Conceptually, if a patient with an intermediate pretest likelihood of CAD has an entirely normal coronary CTA, without significant coronary calcification, no further testing would be required. Similarly, if critical coronary stenoses in the proximal portions of the coronary arteries are found, catheter-based coronary angiography would be indicated for possible PCI or CABG. In many patients, however, stenoses defined by coronary CTA will be of uncertain significance, and MPS would then be appropriate for further diagnostic assessment. MPS would remain, however, the initial test in patients with known disease, where it is used for purposes of risk-stratification and guiding patient management. One problem of MPS or even myocardial perfusion PET is the occasional finding of a normal study in a patient with severe CAD and balanced reduction in blood flow. In contrast, it is highly unlikely that coronary CTA would be completely normal in such patients.
Limitations of Coronary CTA.
The principal limitation of coronary CTA, with even the most recent-generation scanners, is the presence of dense calcification of the coronary arteries. Though mild amounts of calcification do not pose a problem for these scanners, with dense calcification it is not possible to assess the degree of luminal obstruction within the calcified zone. Other limitations include the need for a regular heart rhythm and a relatively low heart rate (usually considered <70), the latter usually resulting in the routine requirement for the administration of β-blockers at the time of scanning. To date, it is not possible to perform CTA, for example, in patients with atrial fibrillation, unless it is highly regular. Additionally, a tendency of the coronary CTA to overestimate the degree of stenosis has been described, resulting in a frequent need for a confirmatory functional test such as MPS after the anatomic CTA. Of course, coronary CTA also results in radiation to the patient. However, when using methods with maximal x-ray exposure only during needed portions of the cardiac cycle, the amount of radiation associated with these procedures becomes comparable to that received with the standard nuclear cardiology procedures.
Applications of Coronary CTA.
With the wider availability of fast 16-slice or greater CT scanners, noninvasive MSCT coronary angiography is becoming commonly used for clinical purposes. This application is likely to be furthered by the formation and activities of the Society of Cardiovascular CT. It is also likely that new procedure codes will become accepted for coronary CTA. As CTA becomes more widely available, it is likely that this technology will compete with stress imaging methods (MPS or stress endocardiography) in patients with an intermediate likelihood of CAD. For purposes of risk assessment, for patients with known disease or for those known or likely to have extensive coronary calcium, MPS is likely to remain as the dominant approach. If MPS has been performed as the initial test, some patients might benefit from the further assessment by CTA. These include those with a strong clinical suggestion of CAD after a normal or equivocal MPS or patients with marked discordance between nuclear and clinical or electrocardiography (ECG) responses to stress. CTA may be of particular value also in any patient in whom the combined MPS and stress ECG responses raise the possibility of left main or triple-vessel CAD (e.g., transient ischemic dilation, exercise hypotension with normal MPS). Because MPS has the rare, but important, limitation of at times missing the balanced reduction of coronary flow, such as might be observed in patients with left main CAD (Figs. 6 and 7), assessment by coronary CTA may be useful in identifying these patients. Coronary CTA can also be of use in patients with suspected nonischemic cardiomyopathy, patients with coronary anomalies, and young patients undergoing valvular surgery.

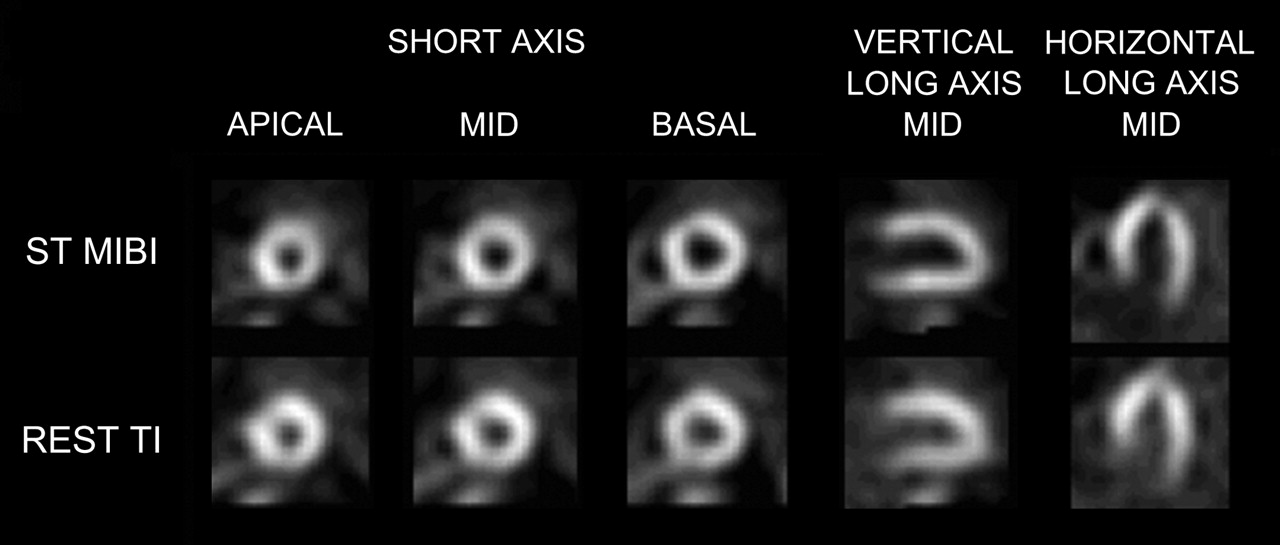
Exercise MPS in asymptomatic 70-y-old male diabetic shows mild decreased uptake in anterior and lateral walls. Overall the MPS study, including ventricular, was considered equivocal. ST = stress; TI = thallium.

EBT study at level of left main coronary artery of patient in Figure 6. There is severe calcification in the left main and LAD coronary arteries. CCS was 1,295 (87th percentile). On the basis of combined MPS and CCS information, patient underwent coronary angiography, which revealed 75% stenosis in left main artery and 60% stenosis in mid of LAD. Patient underwent successful CABG.
The availability of PET/CT and SPECT/CT will add further complexity to the concepts regarding appropriate selection of tests, with their ability to provide both detection of coronary stenosis and assessment of functional significance (44). With the development of cardiac dedicated PET/CT and CT/SPECT systems, it may be that a large body of data will be available in the future, providing information with regard to coronary calcium, coronary stenoses, and stress-induced ischemia. Such databases would be a source of evidence with regard to which test or combination of tests is most appropriate in a given setting. Because rest/stress PET or SPECT studies could be performed as a routine in conjunction with coronary CTA, the possibility of taking “all comers” regardless of the amount of coronary calcium that they have would enhance the usefulness of the noninvasive coronary angiography.
Role of CMR in Detection of CAD
CMR provides a very effective method for comprehensive cardiac assessment. In addition to the assessment of myocardial viability, which is probably the single most important use of CMR in CAD at the present time, the approach provides the most accurate assessment of cardiac chamber volumes and function as well as myocardial mass and has become used as the gold standard for these measurements. Additionally, CMR is useful for visualizing and characterizing cardiac masses and thrombi, for assessing valvular function, and for demonstrating with high resolution complex congenital and acquired cardiac and vascular disease processes. Late enhancement with gadolinium has emerged as a highly sensitive and specific method for detecting myocardial necrosis or fibrosis (45), resulting in high accuracy for detecting MI, both acute and chronic. MI is usually easily distinguished from a variety of other myocardial disease processes by the pattern of involvement of the subendocardium. With regard to detection of CAD, the presence and pattern of delayed hyperenhancement by CMR is perhaps of greatest use in establishing whether a patient presenting with ventricular dysfunction has ischemic or nonischemic cardiomyopathy (46).
Promising work has been done with rest and pharmacologic stress myocardial perfusion with CMR, an example of which is shown in Figure 8. In comparison to MPS, a key advantage of CMR is the lack of dependence on regional hypoperfusion. Because the high resolution of CMR allows the discrimination of subendocardial and subepicardial flow, the limitation of balanced reduction of flow is unlikely to apply to CMR—that is, diffuse subendocardial ischemia would be detected in these patients. The method may be well suited to women with syndrome X, who may have diffuse subendocardial ischemia (47). At the present time, CMR for rest/stress perfusion is limited principally by the dependence on a first-pass technique and the lack of conspicuity of perfusion defects.
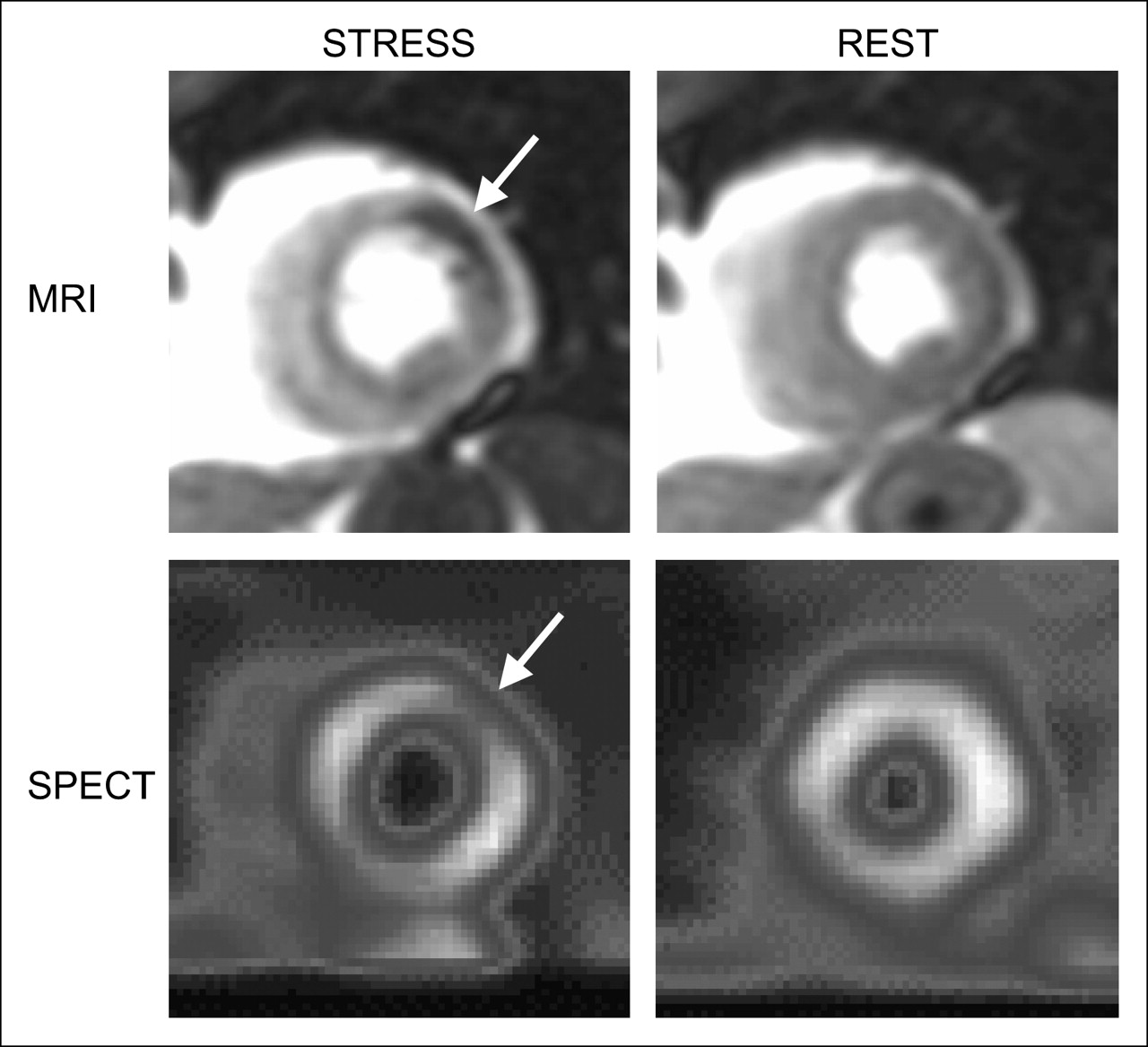
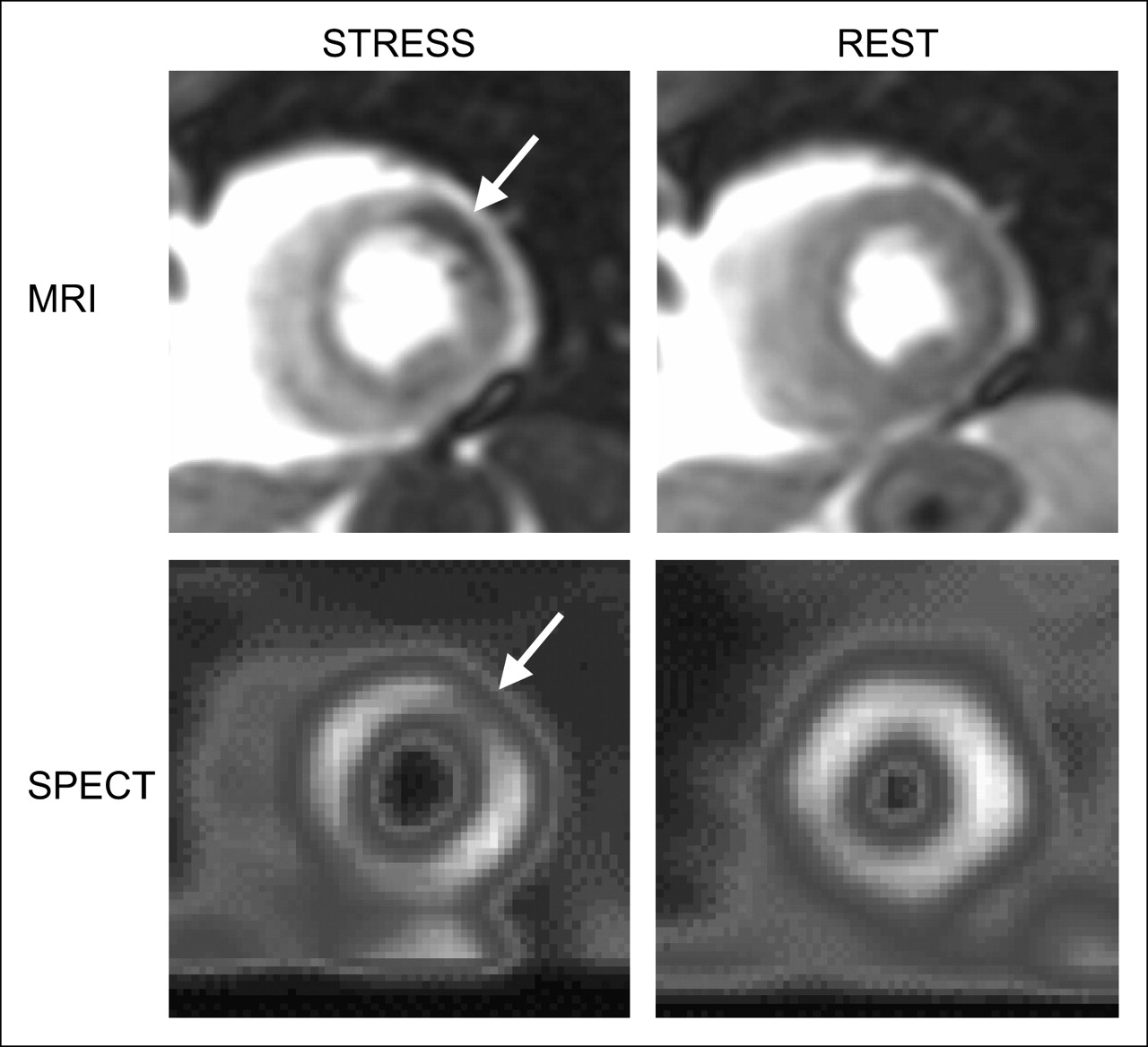
Case example from our laboratory shows concordant left circumflex territory perfusion defects on CMR and MPS. Short-axis perfusion images acquired during adenosine (left) and at rest (right) using first-pass CMR (top) and dual-isotope MPS (bottom) are shown. CMR images acquired during pharmacologic vasodilation revealed reduced image intensity in anterolateral wall (arrow) that was not present on rest CMR. Similarly, MPS tomograms at same short-axis level, obtained after sestamibi injection during the same adenosine stress as used for CMR, also revealed a reversible perfusion defect in anterolateral wall (arrow).
In general, the comprehensive, high-resolution assessments provided by CMR are similar in many ways to echocardiography, with the difference being that with CMR there is no dependence on the patient's acoustic window and any portion of the myocardium can be examined. However, the technique is complex and currently highly dependent on the expertise of the operator. Advantages of this method are the excellent soft-tissue contrast provided and the ability to characterize tissue with a variety of pulse sequences. In addition, there is no radiation and no need for potentially nephrotoxic contrast administration. While the routine “one-stop shop” application of CMR for comprehensive cardiac assessment remains possible, its full realization would appear to depend on developments that make at least the myocardial perfusion assessments and possibly the coronary angiographic assessments more of a practical, clinical routine that would “travel well” from laboratory to laboratory.
On a research basis, great strides have been made in CMR for purposes of noninvasive coronary angiography. A variety of technical approaches are available for this purpose. However, there are several obstacles impeding the routine use of CMR for noninvasive coronary angiography. Although true 3-dimensional “whole-heart” acquisition (48) has recently been reported, this approach is not yet practical, and there is the need for separate prescription of the 2-dimensional planes for imaging, a step that extends the study time and takes considerable expertise. The acquisitions are obtained over several heart beats, increasing the possibility of misregistration. Intrinsically, CMR does not achieve as high spatial resolution as CT. Although, over time, CMR coronary angiography could become more common, at present, it is widely accepted that CT has at least a multiple-year lead in this application. Supporting this is a meta-analysis of 48 studies in which MSCT has been shown to have higher sensitivity and specificity than CMR for noninvasive coronary angiography (49).
CONCLUSION
Nuclear cardiology, coronary calcium scanning, CTA, and CMR imaging techniques have specific roles in the assessment of patients with suspected coronary disease. Although CT and CMR techniques are currently undergoing rapid technological development and growth, nuclear cardiology techniques will continue to be of great practical value and will often be used in combination with the CCT or CMR modalities.
Acknowledgments
This research was funded in part by a grant from The Eisner Foundation.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH JANUARY 2007.
References
- Received for publication September 21, 2005.
- Accepted for publication October 5, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Plagiarism, Copyright Issues, and How to Format and Cite References Using AMA Style
- IQ SPECT Allows a Significant Reduction in Administered Dose and Acquisition Time for Myocardial Perfusion Imaging: Evidence from a Phantom Study
- Physician-Preferred Versus Policy-Based Testing: Where Do Appropriate Use Criteria Fit In?
- Leaving Relativity Behind: Quantitative Clinical Perfusion Imaging
- Myocardial Perfusion Imaging Versus CT Coronary Angiography: When to Use Which?
- Patterns of Cardiac Stress Testing After Revascularization in Community Practice
- The evolving role of molecular imaging for coronary artery disease: where do we stand today?
- Perfusion Cardiovascular Magnetic Resonance in the Clinical Scenario of Patients With Coronary Artery Disease
- Quantitative Analysis of Myocardial Perfusion SPECT Anatomically Guided by Coregistered 64-Slice Coronary CT Angiography
- Anatomic and Functional Assessment of Coronary Artery Disease: Convergence of 2 Aims in a Single Setting
- SPECT/CT
- Stunning, Hibernation, and Assessment of Myocardial Viability
- Comparison of Imaging Techniques for Tracking Cardiac Stem Cell Therapy
- A comparative study of thoracic radiation doses from 64-slice cardiac CT
- Roles of Nuclear Cardiology, Cardiac Computed Tomography, and Cardiac Magnetic Resonance: Noninvasive Risk Stratification and a Conceptual Framework for the Selection of Noninvasive Imaging Tests in Patients with Known or Suspected Coronary Artery Disease