


Abstract
The concentration of 18F-FDG in the gastroesophageal junction (GEJ) and gastric antrum (GA) varies significantly from patient to patient. To document the reference range of uptake in patients, we reviewed the 18F-FDG PET scans of patients with no documented gastroesophageal disease. Methods: The medical records of patients undergoing PET/CT were reviewed. Patients with known gastric, pancreatic, or liver pathology were excluded. The peak standardized uptake value (SUV) for the GEJ and GA were measured in the remaining patients. The clinical record was also reviewed for gastroesophageal reflux disease (GERD) and previous chemotherapy. Results: A total of 763 patients met the inclusion criteria (388 male and 375 female; mean age ± SD, 57.4 ± 17 y; range, 15–95 y). Images were recorded 68.2 ± 11.8 min after injection of 558.7 ± 35.1 MBq of 18F-FDG. PET/CT was performed on a Discovery LS scanner for 373 patients and on a Biograph scanner for 390. The maximum SUV was less than 4 in 94.4% of patients. GEJ SUV measurements on the Discovery LS and on the Biograph did not significantly differ. During the 6 mo before the scan, 515 patients received no antineoplastic chemotherapy. Of the remaining 248, 137 received chemotherapy within 1 mo before the scan; 65, between 1 and 3 mo before the scan; and 46, between 3 and 6 mo before the scan. No significant differences were found between groups. GERD was documented in the records of 75 patients. Only 58 of these patients were treated with an antacid regimen. In 552 patients, GERD was not known to be present nor was antacid treatment used. An additional 136 patients had antacid treatment without specified gastric symptomatology. Patients with a history of GERD had a slightly higher but not statistically significant SUV peak in the stomach and particularly in the GEJ, except when compared with the group without associated antacid treatment (P = 0.049). Conclusion: In patients without a specific history of esophagogastric disease, a gastroesophageal maximum SUV less than 4 is usually not associated with gastroesophageal neoplasia.
PET scans obtained with 18F-FDG demonstrate a wide patient-to-patient variation in the concentration of tracer at the gastroesophageal junction (GEJ), gastric antrum (GA), and myocardium (1–3). Potential causes of this variation at the GEJ are the often-undocumented presence of inflammation due to intermittent gastroesophageal reflux disease (GERD), subclinical infection with Helicobacter pylori, or secondary effects of chemotherapeutic agents (4,5). The variation in uptake in benign disease makes it difficult to identify neoplasms in this region (6). This study was performed to measure the standardized uptake value (SUV) of gastroesophageal 18F-FDG uptake in a series of patients with no documented disease in this area.
MATERIALS AND METHODS
Patient Population
This was a retrospective study of 18F-FDG PET/CT scans obtained during 2 periods of 1 mo each, from November 1 to November 30, 2003, and from February 8 to March 5, 2004, in the Department of Nuclear Medicine of the Memorial Sloan-Kettering Cancer Center. The studies of all patients referred for imaging to determine the presence or extent of a neoplasm were evaluated. Patients with cancer involving the esophagus, stomach, pancreas, or liver were excluded.
PET Imaging Protocol
Patients were imaged on either a Biograph (Siemens/CTI) or a Discovery LS (General Electric Medical Systems) PET/CT scanner. Both systems produce transaxial, coronal, and sagittal reconstructions of CT, PET, and fusion PET/CT data for interpretation. The Biograph scanner combines a dual-detector spiral CT scanner (Somatom Emotion) and a high-resolution PET scanner with 4.5-mm spatial resolution and 3-dimensional image acquisition. A multimodality computer platform (Syngo; Siemens) is used for image review and manipulation. The Discovery LS scanner consists of a 4-detector-row spiral CT scanner (Light Speed) and a PET scanner (Advance) with a 2- or 3-dimensional image-acquisition algorithm. A workstation (Xeleris; Elgems) was used for image display and analysis.
After the patients had fasted for at least 6 h, they received approximately 555 MBq (15 mCi) of 18F-FDG by intravenous injection. Afterward, the patients rested quietly in a comfortable chair for about 60 min. Patients without contraindications received 450 mL of a dilute barium solution (Readi-Cat 2, 2.1% w/v, 2.0% w/w) to demarcate the bowel. At the time of imaging, patients were placed supine on the imaging table. Spiral CT was performed from the level of the middle of the skull to the level of the pelvic floor. On the Biograph, a scout view was recorded with 30 mA and 130 kV(p), followed by a spiral CT scan at 50 mA, 130 kV(p), 5-mm section width, 4-mm collimation, and a 12-mm table feed per rotation. On the Discovery LS, a scout view with 30 mA and 120 kV(p) was followed by a spiral CT scan at 0.8-s rotation time, 80 mA, 140 kV(p), 5-mm section width, and a 4.25-mm interval in high-speed mode. This was followed by acquisition of PET emission images. Each image was acquired for 3–4 min per bed position (11.2-cm increments on the Biograph [3-dimensional mode]; 14.2 cm-increments on the Discovery LS [2-dimensional mode]). The total acquisition time ranged from 25 to 35 min per patient. The CT data were used for attenuation correction of PET emission images and for anatomic localization of emission data.
Image Interpretation
All PET/CT images were read directly from the screen of the computer workstation. A region of interest was drawn on the fused PET/CT image to measure the peak SUV of the GEJ and GA: SUV = (peak kBq/mL in region of interest)/(injected activity/g of body weight).
Clinical Review
The clinical record of each patient was reviewed to identify patients with GERD, patients currently receiving antacid treatment, and patients receiving chemotherapy during the 6 mo before the scan.
The patients were divided into 4 groups: those treated with antineoplastic chemotherapy during the 6 mo before imaging, those with GERD treated with antacid medication, those with GERD not treated with antacid medication, and untreated patients. Data were analyzed with the χ2 test. A P value of ≤0.05 was considered to indicate a statistically significant difference. Data are expressed as mean ± SD.
RESULTS
A total of 763 patients met the inclusion criteria, 388 of whom were male and 375 female. The mean age for the entire study population was 57.4 ± 17 y (range, 15–95 y). The images were acquired 68.2 ± 11.8 min after injection of 558.7 ± 35.1 MBq of 18F-FDG. Blood sugar levels before the scans were 90.5 ± 24.3 mg/dL. PET/CT scans were obtained on the Discovery LS for 373 patients and on the Biograph for 390. Patients were referred for the PET/CT examination for evaluation of several different types of cancer (Table 1). The average of the SUV peak was 2.6 ± 0.8 (range, 0.8–7) for the GEJ and 2.2 ± 0.7 (range, 0.8–6.8) for the GA.
Indications for PET/CT
GEJ SUV measurements on the Discovery LS and on the Biograph PET/CT scanners did not significantly differ: respectively, 2.7 ± 0.8 versus 2.5 ± 0.7 (χ2 = 14.95; P = 0.06). A typical 18F-FDG PET scan of normal gastric uptake is shown in Figure 1 and demonstrates diffuse, mild uptake in the gastric wall, with an SUV peak at 2.8.
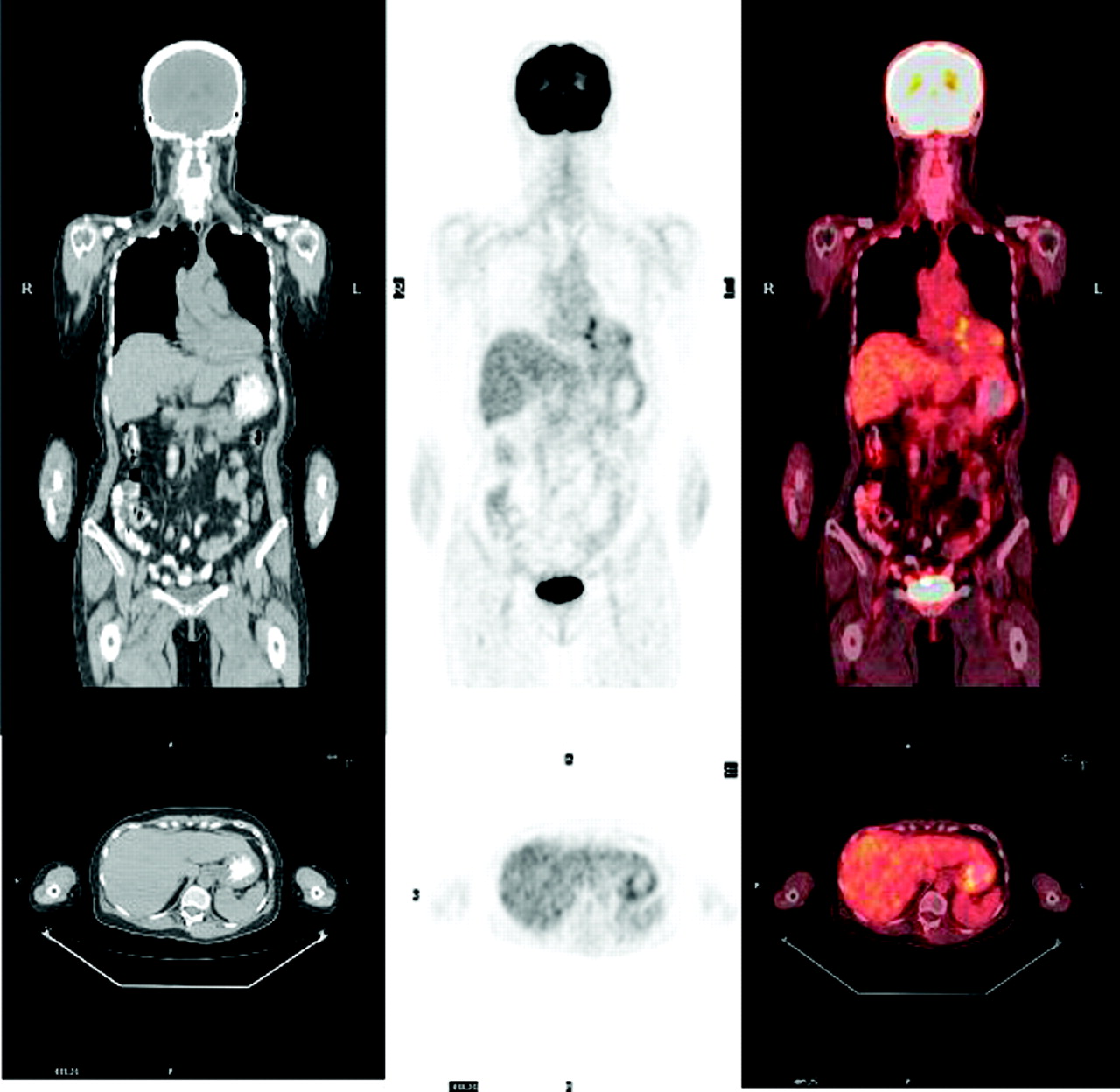
Diffuse uptake (SUV peak, 2.8) in stomach wall. From left to right, images are CT, 18F-FDG PET, and 18F-FDG PET/CT, with sagittal views at top and axial views at bottom.
The number of patients receiving barium to demarcate the bowel was 590, whereas 173 patients received no barium. The SUV peak was 2.6 ± 0.7 for the GEJ and 2.2 ± 0.7 for the GA in both groups of patients (P = not statistically significant).
In the 6 mo before the scan, 515 patients had no antineoplastic chemotherapy; of the remaining 248, 137 received chemotherapy during the month before scan; 65, between 1 and 3 mo before the scan; and 46, between 3 and 6 mo before the scan. The SUV measurements for the GEJ and GA of those patients are summarized in Table 2.
SUVs According to Timing of Chemotherapy
GERD was documented in the records of 75 patients. Only 58 of these patients were treated with an antacid regimen. In 552 patients, GERD was not present nor was antacid treatment used. An additional 136 patients received antacid treatment without specified gastric symptomatology. The SUV measurements for the GEJ and GA of those patients are shown in Table 3. Increased uptake was seen in the GEJ and GA of a patient with GERD (Fig. 2).
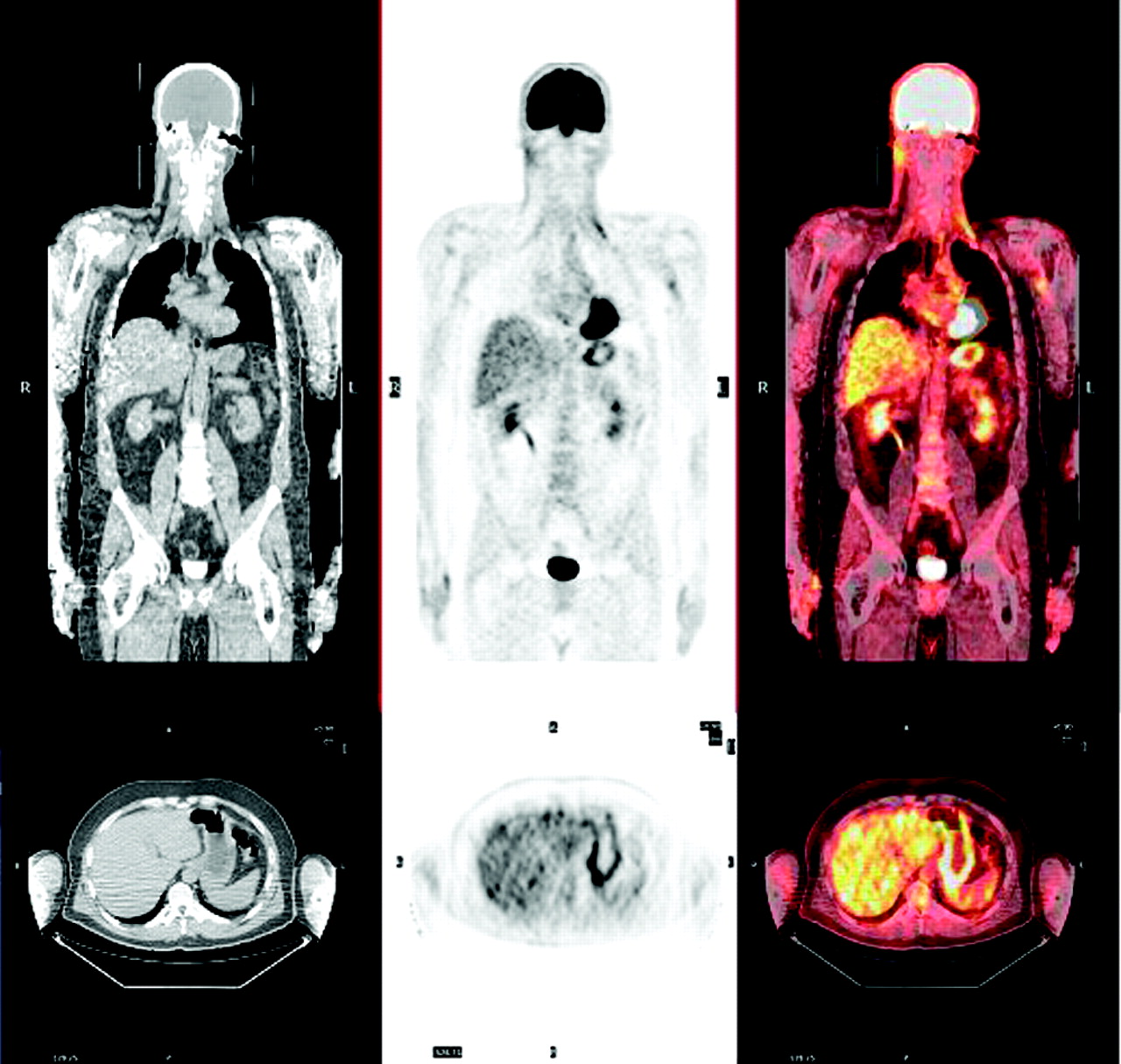
Increased uptake (SUV peak, 3.9) in GA in patient who presented with untreated GERD. From left to right, images are CT, 18F-FDG PET, and 18F-FDG PET/CT, with sagittal views at top and axial views at bottom.
SUVs According to Presence of GERD and Use of Antacids
DISCUSSION
A major application of 18F-FDG PET/CT is the detection and staging of cancer. High target-to-nontarget ratios are obtained for common neoplasms and allow detection of disease in many areas of the body (7). 18F-FDG uptake also occurs in nonmalignant tissue, such as brain, in which glucose is the principal source of energy. However, there are other sites, such as the bowel and stomach, that have variable physiologic 18F-FDG uptake, partly because of smooth muscle activity (8,9) or nonneoplastic inflammation, that may be confused with malignancy. The purpose of this study was to clarify the reference range of 18F-FDG uptake in the region of the GEJ in patients with no known disease of the distal esophagus or stomach.
In general, after qualitatively evaluating the attenuation-corrected PET images, the interpreting physician uses semiquantitative analysis of a region-of-interest radioactivity value normalized to the injected dose and body weight (SUV) to help distinguish neoplasia from nonneoplastic disease (10). In our study, more than 95% of patients had a peak SUV of less than 4 in the GEJ and GA. These data correspond to the results of Gordon et al. (2).
SUV measurements are affected by the methods of both image reconstruction and attenuation correction, and this effect should be considered when serial PET studies are performed on cancer patients (11). Although PET emission images were acquired in 3-dimensional mode on the Biograph and 2-dimensional mode on the Discovery LS, no systematic differences in SUV measurements were found between scans obtained on the 2 instruments.
SUV measurements can also be modified by the use of oral contrast medium (12,13). However, in our study, peak SUV in the GEJ or GA did not differ significantly between the patients who received a dilute barium solution and the patients who did not.
Infectious and inflammatory lesions may show increased 18F-FDG accumulation and mimic tumor. These findings are attributed to an increased metabolic state of inflammatory cells in the lesion (14).
Mucositis is a common cause of morbidity during chemotherapy (4). The incidence of National Cancer Institute grade 3–4 oral and gastrointestinal mucositis derived from clinical trials of standard-dose chemotherapy is estimated at about 15% and exceeds 15% in patients treated with 5-fluorouracil or irinotecan (15). In our study, antineoplastic chemotherapy in the 6 mo before PET/CT did not increase gastric uptake.
Unfortunately, it was difficult to accurately gauge the use of antacid medication, because 37.6% of the patients who had received antineoplastic chemotherapy also received antacid therapy, whereas only 20.4% of patients without antineoplastic chemotherapy received antacid medication. These findings suggest that recent chemotherapy cannot explain increased uptake in the GEJ or GA.
The cardia, located immediately distal to the GEJ, is a frequent site of chronic inflammation (16). Inflammation in this region is termed chronic carditis and is often associated with GERD (5,17). In our study, patients with a history of GERD had a slightly higher but not statistically significant SUV peak in the stomach and particularly in the GEJ, except when compared with the group not receiving associated antacid treatment. This difference was small, with a large overlap between the different groups. The SUV peak 18F-FDG uptake for the GEJ of these patients was 3.0 ± 1.1 (range, 1.7–7; <4 in 94.4% of patients). Accordingly, a known history of GERD cannot explain a major increase in focal 18F-FDG uptake in the stomach.
Each year in the United States more than 25,000 patients are diagnosed with cancer of the stomach, with a death rate of 14,000 per year (18). The sensitivity of 18F-FDG PET for localizing the primary lesion and identifying local spread has made the imaging procedure an integral part of patient evaluation. According to Yeung et al. (6), the primary gastric cancer lesion has a peak SUV of about 8.0 (range, 4.6–17.6). This finding agrees with those of Herrington et al. (19). Yeung et al. (20) also reported on patients with esophageal cancer; 18F-FDG PET detected 99% of primary lesions (66/67), and peak SUV was about 11 (range, 3.6–46). Ott et al. (21) reported a peak SUV of between 5.2 and 50.3 in 52 patients with adenocarcinomas of the esophagogastric junction. Among all patients included in those studies, only 1 had an SUV of less than 4 (3.6). This is in agreement with our data, because 94.4% of our patients without a known medical history of esophagogastric malignancy had a peak SUV of less than 4. Moreover, cases of benign increased 18F-FDG uptake have been published, as described for Ménétrier’s disease, but with an SUV commonly lower than 4 (22).
CONCLUSION
In patients without a specific history of esophagogastric disease, a gastroesophageal maximum SUV of less than 4 is usually not associated with gastroesophageal neoplasia. When the SUV is greater than 4, however, further evaluation, such as endoscopy, may be warranted.
Acknowledgments
This work was supported by the Conseil Régional de Bretagne, France.
Footnotes
Received Jun. 4, 2004; revision accepted Aug. 23, 2004.
For correspondence or reprints contact: Pierre Y. Salaun, MD, Nuclear Medicine Department, CHU Brest, Boulevard Tanguy Prigent, 29609 Brest Cedex, France.
E-mail: Pierre-yves.salaun{at}chu-brest.fr





{kind=link}
{kind=link}