


Abstract
The usefulness of 18F-FDG PET in gastric cancer recurrence is limited by low sensitivity. Given that detectability by PET is dependent on the tumor’s metabolic characteristics, we tested whether the performance of PET for gastric cancer recurrence is enhanced in patients with 18F-FDG–avid primary tumors. Methods: Three hundred sixty-eight patients with advanced gastric cancer underwent 18F-FDG PET/CT for initial staging and for recurrence surveillance after curative surgery. On initial PET/CT, primary tumors were 18F-FDG–avid if they displayed focal uptake with an SUVmax 4 or more. Follow-up 18F-FDG PET/CT was evaluated for recurrent disease. Results: On initial PET/CT, the primary tumor was 18F-FDG–avid in 236 of 368 (64.1%) and nonavid in 132 patients (35.9%). During follow-up for 18.9 ± 13.3 mo, 72 patients (19.6%) had recurrence. Of the 63 PET scans with recurrence, 42 (66.7%) and 21 (33.3%) were scans of patients with 18F-FDG–avid and nonavid primary tumors, respectively. PET sensitivity was higher in scans of patients with 18F-FDG–avid than nonavid tumors for all recurrences (81.0% vs. 52.4%; P = 0.018) and nonanastomosis site recurrences (82.1% vs. 47.4%; P = 0.006). The sensitivity for detecting peritoneal recurrence was also higher for the avid tumor group. PET specificity was similarly high (97.1% and 97.5%) for both groups. Adding cell type and Lauren classification to tumor 18F-FDG avidity further enhanced PET sensitivity. Conclusion: Surveillance 18F-FDG PET/CT after resection of gastric cancer has significantly higher sensitivity in patients with 18F-FDG–avid primary tumors and may have greater value in this group.
Gastric cancer is the fifth most common cancer and a third leading cause of cancer death worldwide (1). Surgery is the standard treatment for patients with resectable disease, but the prognosis remains grave with a 5-y survival of only 26% (2). Because most deaths after gastric cancer resection occur from distant recurrence (3), surveillance for recurrent disease is an important part of the postsurgical management of patients. 18F-FDG PET/CT is a valuable imaging tool for the detection and staging of various malignancies including gastric cancer (4). The current guidelines of the National Comprehensive Cancer Network state that 18F-FDG PET/CT is useful for the evaluation of recurrent gastric cancer (5). However, studies to date have shown inconsistent results regarding the performance of 18F-FDG PET/CT for this purpose (6–8), and there are concerns that low diagnostic sensitivity may limit its usefulness (9). As such, it would be clinically useful to identify subpopulations of gastric cancer patients who are most likely to benefit from surveillance with 18F-FDG PET/CT after curative gastrectomy (10,11).
Gastric adenocarcinomas display extreme genetic complexity and biologic heterogeneity, and 18F-FDG avidity is clearly dependent on the biologic and clinical–pathologic characteristics of the tumors (12–14). For instance, high 18F-FDG uptake of primary gastric cancers has been shown to be associated with greater aggressiveness and poor patient survival (15,16). The histologic type of the primary tumor may also influence the sensitivity of 18F-FDG PET for detecting recurrent gastric cancer. In addition, 18F-FDG avidity of primary gastric cancers observed on initial PET/CT has been shown to correlate with the magnitude of 18F-FDG uptake by distant metastatic lesions and lymph nodes (17,18).
Taken together, these findings suggest that 18F-FDG avidity of the primary gastric cancer on initial PET/CT could be a major factor in the capacity of follow-up PET/CT to detect recurrent disease, but this has not been previously explored. In this study, we thus investigated the relation between primary gastric cancer 18F-FDG avidity and the performance of surveillance PET/CT for detecting recurrent disease after curative gastrectomy.
MATERIALS AND METHODS
Study Subjects
Study subjects were selected from 919 patients with stomach cancer who underwent preoperative 18F-FDG PET/CT between 2008 and 2013, had surgical resection with curative intention, and underwent follow-up 18F-FDG PET/CT to screen for possible recurrence. Among these, 202 patients who had history of another malignancy or coexisting malignancy were excluded, as were 15 patients who were treated for recurrence before follow-up PET/CT. In addition, 324 patients who had early gastric cancer and 6 patients who had no residual malignancy remaining after biopsy were also excluded. Finally, 4 patients were excluded for indeterminate clinical diagnosis, and a total of 368 subjects with advanced gastric cancer were included in the study. This resulted in a total of 368 preoperative PET/CT scans and 577 follow-up PET/CT scans for analysis. The mean number of follow-up PET/CT scans per patient was 1.6 (range, 1–5).
This retrospective observational study was approved by our institutional review board with exemption for written consent of study subjects.
18F-FDG PET/CT Imaging
Patients fasted for at least 6 h, and blood glucose level was less than 200 mg/dL at the time of 18F-FDG injection in all cases. At 60 min after injection of 18F-FDG (5 MBq/kg), imaging was performed on a Discovery LS (GE Healthcare; n = 224 scans) or an STe PET/CT scanner (GE Healthcare; n = 721 scans) without intravenous or oral contrast. Whole-body CT was performed using a continuous spiral technique with an 8-slice helical CT (140 keV; 40–120 mA; section width, 5 mm; Discovery LS) or a continuous spiral technique with 16-slice helical CT (140 keV; 30–170 mA; section width, 3.75 mm; STe).
After CT, an emission PET scan was obtained from head to thigh. This was 4 min per frame in 2-dimensional mode with attenuation-corrected images (4.3 × 4.3 × 3.9 mm) reconstructed using an ordered-subset expectation maximization algorithm (28 subsets, 2 iterations; Discovery LS) or 2.5 min per frame in 3-dimensional mode with attenuation-corrected images (3.9 × 3.9 × 3.3 mm) reconstructed using a 3-dimensional ordered-subset expectation maximization algorithm (20 subsets, 2 iterations; Discovery STe).
Medical Record Review
Histopathology of the surgical specimen was based on the Japan Gastric Cancer Association system and the Lauren classification. Medical records showed that patients underwent postoperative clinical follow-up for a mean duration of 38.1 ± 16.1 mo (range, 1–72 mo). All patients without recurrence had a follow-up period of at least 12 mo. Appropriate imaging studies or histologic tests were performed whenever recurrence was suspected. The presence or absence of recurrent disease was determined by clinical decision based on all available information. For recurrent disease, this included histopathology results (n = 22), characteristic radiologic findings (n = 48), rise of serum CA 19-9 that decreased by chemotherapy (n = 1), and development of intractable ascites (n = 1).
Analyses of Preoperative PET/CT
Preoperative PET/CT images were evaluated for 18F-FDG avidity of primary gastric tumors according to criteria set at the stage of study design. Tumor sites were assessed on the basis of tumor locations described on endoscopy reports. Tumors were classified as 18F-FDG–avid if there was focal uptake on the known tumor site that was visually discernable from the remaining stomach and the measured SUVmax was 4.0 or greater. Tumors were 18F-FDG–nonavid if they were not visually discernable from the remaining stomach or if tumor SUVmax was less than 4. Diffuse gastric 18F-FDG uptake that could not be differentiated from physiologic activity was not considered specific tumor uptake. SUVmax was measured by manually placing a circular region of interest on visually discernable primary tumors.
Analyses of Follow-up PET/CT
Follow-up 18F-FDG PET/CT was performed as part of a routine surveillance protocol without specific symptoms in most (n = 494) scans. In the remaining scans, it was performed for abnormal radiologic findings (n = 73), abdominal pain (n = 3), ascites (n = 3), elevated CA 19-9 level (n = 1), or complaint of nonspecific symptoms (n = 3).
PET sensitivity and specificity for diagnosing recurrence were analyzed using scan-based rather than patient-based data, using 352 scans of patients with 18F-FDG–avid primary tumors and 225 scans in patients with nonavid tumors. PET sensitivity for recurrence was assessed with PET/CT scans obtained within 3 mo of clinical decision on recurrence. Follow-up PET scans were categorized as positive if the formal report by experienced nuclear medicine physicians concluded high probability for recurrence. Scans with formal reports concluding low or intermediate probability for recurrence were reevaluated, and only scans with lesions with focal 18F-FDG uptake clearly discernible from surrounding activity that could be differentiated from physiologic activity were categorized as positive, whereas the remaining scans were categorized as negative for recurrence. The SUVmax of suspected recurrent lesions was measured with circular regions of interest. PET interpretation was combined with the final clinical diagnosis to yield false- or true-positive and -negative PET results.
Statistical Analysis
Comparison of clinical characteristics between patients with 18F-FDG–avid and –nonavid primary tumors was performed with Student t tests, Pearson χ2 tests, or Fisher exact tests. The relation between SUVmax of primary tumors and recurrent lesions was analyzed by Pearson correlation tests. SPSS software for Windows (SPSS) was used for statistical analysis, and P values of less than 0.05 were considered significant.
RESULTS
Clinical Characteristics According to Primary Tumor 18F-FDG Avidity
The clinical characteristics of the 368 study subjects are summarized in Table 1. The total population had a mean age of 57.8 ± 11.6 y, and there were 250 men and 118 women. On preoperative PET/CT, the primary tumor was 18F-FDG–avid in 236 cases (60.2 ± 10.9 y; 171 men) and 18F-FDG–nonavid in 132 cases (53.5 ± 11.6 y; 79 men). Patients with 18F-FDG–avid primary tumors had a significantly greater incidence of intestinal-type histology according to the Lauren classification (49.2%) than those with nonavid tumors (22.7%). In contrast, patients with 18F-FDG–nonavid primary tumors had a significantly greater incidence of diffuse-type histology than those with avid tumors (59.1% vs. 35.6%). Patients with 18F-FDG–nonavid primary tumors also more frequently had signet ring cell carcinomas than their counterpart (24.2% vs. 8.1%). Surgical tumor size was not significantly different between the 2 groups. Pathologic staging according to the seventh edition of the American Joint Committee on Cancer staging manual (19) showed that T2 disease (58.3% vs. 44.1%) and N0 disease (50.8% vs. 28.8%) were more frequent in patients with 18F-FDG–nonavid than avid primary tumors.
Clinical Characteristics of 368 Study Subjects with Advanced Gastric Cancer
Clinical Follow-up and Disease Recurrence
All study subjects underwent subtotal or total gastrectomy with regional lymph node dissection under curative intention. In a total of 72 patients (19.6%), recurrent disease occurred during follow-up (Table 2). This occurred at a mean interval of 18.9 ± 13.3 mo after surgery. The remaining 296 patients showed no evidence to suggest recurrence during follow-up. The mean follow-up period of patients without recurrence was 42.8 ± 13.0 mo (range, 11–72 mo). Comparison of patients with 18F-FDG–avid and –nonavid primary tumors (Table 2) showed no difference in recurrence rate (19.5% vs. 19.7%) or time to recurrence (17.3 ± 13.3 vs. 21.8 ± 12.9 mo).
Gastric Cancer Recurrence and Diagnostic Performance of 18F-FDG PET
Postoperative Surveillance 18F-FDG PET/CT
We next investigated the sensitivity of follow-up 18F-FDG PET for detecting recurrence using a total of 63 PET scans obtained within 3 mo of clinical decision of recurrence. Although an interval of 3 mo was used, the actual interval in most patients with recurrence was much shorter. Hence, the mean interval was 11.3 ± 1.6 d, and 75% of the patients had an interval of less than 2 wk. The results showed that follow-up 18F-FDG PET/CT had an overall sensitivity of 71.4% for the detection of recurrent disease, which was not significantly affected (70.7%) by excluding recurrences in remnant stomach or anastomosis from analysis (Table 2). Comparison of groups revealed that the sensitivity of PET/CT for detecting recurrence was superior in scans of patients with 18F-FDG–avid compared with 18F-FDG–nonavid primary tumors (81.0% vs. 52.4%). Furthermore, the superior sensitivity for 18F-FDG–avid primary tumor persisted when recurrences at remnant stomach or anastomosis site were excluded (82.1% vs. 47.4%; Table 2).
PET specificity determined using 514 follow-up PET/CT scans without recurrent disease was 97.3%. This high specificity was obtained by interpreting mild activity on remnant stomach and anastomosis sites as nonspecific. The specificity for recurrence was similarly high for both primary tumor 18F-FDG–avid and –nonavid groups (97.1% vs. 97.5%; Table 2). A representative true-positive case with an 18F-FDG–avid primary tumor and a false-negative case with an 18F-FDG– nonavid primary tumor are illustrated in Figures 1 and 2, respectively.
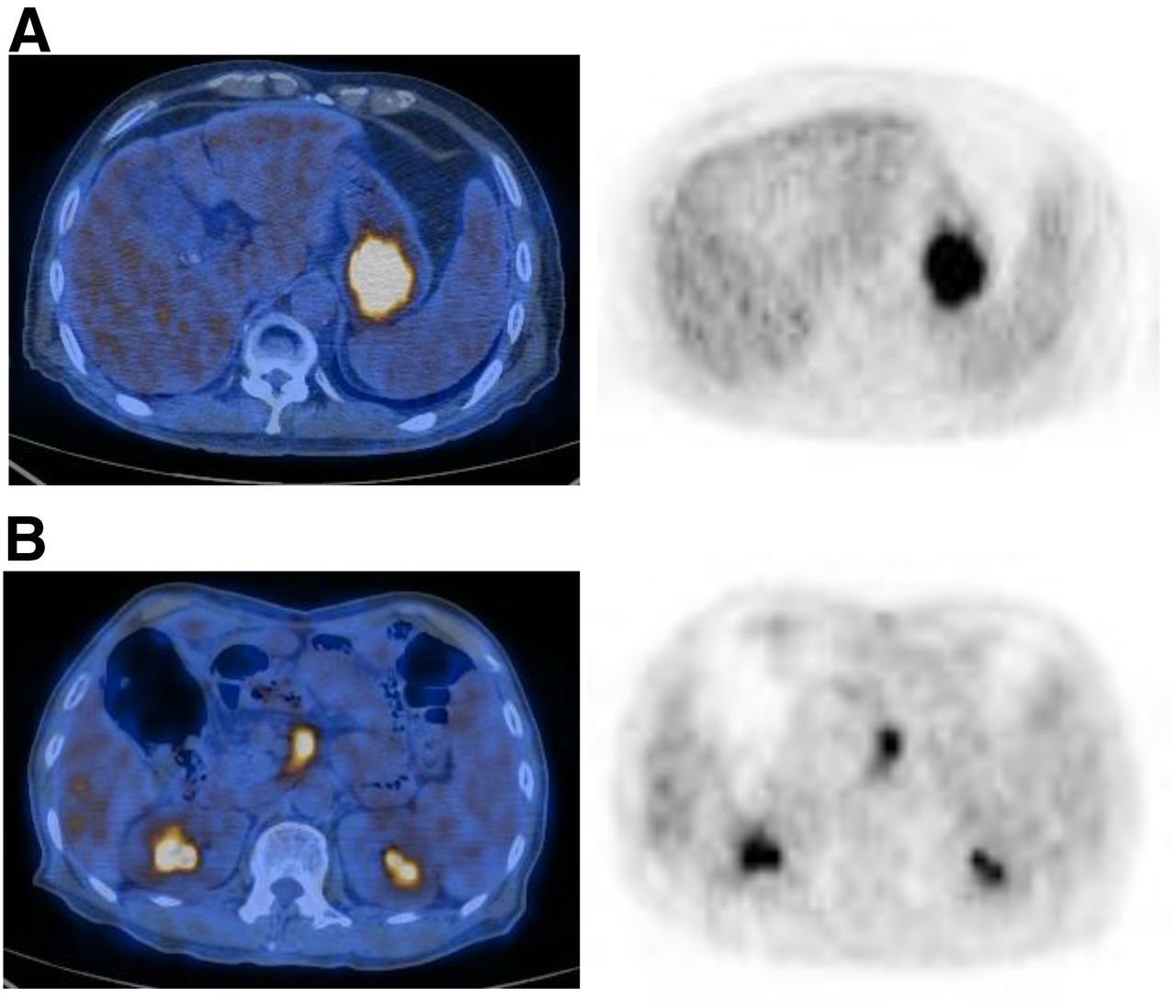
Representative case of 18F-FDG–avid primary tumor. (A) Preoperative PET/CT and PET images of 75-y-old patient show a gastric cancer with high 18F-FDG uptake (SUVmax, 11.9). Primary tumor was moderately differentiated tubular adenocarcinoma (4.5 × 4 × 0.6 cm) located in center of high body and posterior wall. (B) Follow-up PET/CT and PET images 27 mo later demonstrated increased 18F-FDG uptake in mesenteric lymph node (SUVmax 7.5) that was confirmed to be recurrent disease by radiologic studies.

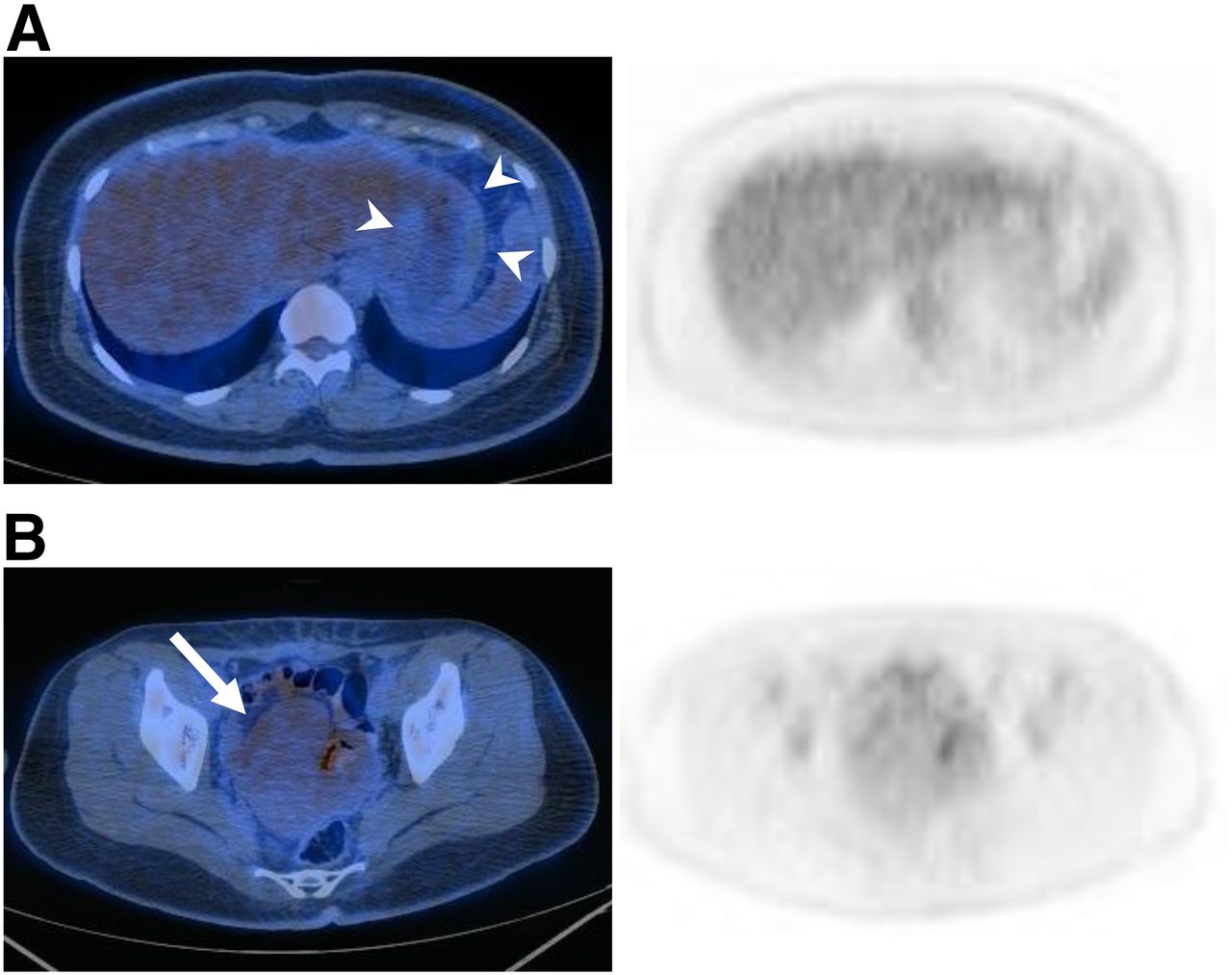
Representative case of 18F-FDG–nonavid primary tumor. (A) Preoperative PET/CT and PET images of 38-y-old patient showed gastric cancer without visually discernable 18F-FDG uptake. CT findings show diffuse thickening involving most of the stomach wall (arrowheads). Primary tumor was poorly differentiated tubular adenocarcinoma (14 × 13 cm) located in body and anterior wall. (B) Follow-up PET/CT and PET images 10 mo later failed to detect any suggestive 18F-FDG uptake, but recurrence in right ovary (arrow) was pathologically confirmed.
Among the 63 PET scans obtained within 3 mo of clinical decision of recurrence, 30 and 25 scans were from patients who received postsurgery adjuvant chemotherapy and chemoradiotherapy, respectively. PET sensitivity for recurrence was 73.3% in scans of patients with adjuvant chemotherapy and 72.0% in those with chemoradiotherapy, compared with 62.5% in those without adjuvant treatment. In all 3 groups, PET sensitivity for recurrence tended to be greater for those with 18F-FDG–avid than –nonavid primary tumors (82.6% vs. 42.9% for those with adjuvant chemotherapy; 78.6% vs. 63.6% for those with chemoradiotherapy; and 80.0% vs. 33.3% for those without adjuvant treatment).
We additionally evaluated the performance of PET scans for recurrent disease in subjects who underwent PET/CT as surveillance tests (85.6%) or for suggestive signs or symptoms (14.4%). As a result, PET sensitivity for detecting recurrence was 66.7% in the 15 scans obtained for surveillance and 72.9% in the 48 scans obtained for suspicion of recurrence (P = 0.746). In the former group, PET sensitivity was 100% (10/10) in scans of patients with 18F-FDG–avid primary tumor and 0% (0/5) in those with 18F-FDG–nonavid tumor. In the latter group, PET sensitivity was 75.0% (24/32) in those with 18F-FDG–avid tumor and 68.8% (11/16) in those with 18F-FDG–nonavid tumor, both of which had higher sensitivity than cases with nonavid tumors when performed for surveillance (P = 0.003 and 0.012, respectively). PET specificity for detecting recurrence was 97.5% in the 479 scans acquired for surveillance and 94.3% in the 35 scans acquired for suspicion of recurrence (P = 0.246). In the former group, PET specificity was 97.3% (285/293) in scans of patients with 18F-FDG–avid primary tumor and 97.8% (182/186) in those with 18F-FDG–nonavid tumor. In the latter group, PET specificity was 94.1% (16/17) in those with 18F-FDG–avid tumor and 94.4% (17/18) in those with 18F-FDG–nonavid tumor.
We also analyzed PET performance for recurrence based on visual interpretation only. As a result, PET sensitivity for recurrence was 76.1% in scans of patients with visually discernible primary tumor 18F-FDG uptake and 58.8% in those without discernible primary tumor 18F-FDG uptake. Specificity was 97.3% and 97.2%, respectively.
Distribution of Recurrence Site and Detection by 18F-FDG PET
The distribution of recurrence sites and number of lesions detected by 18F-FDG uptake in the 63 patients with recurrent disease (and PET/CT within 3 mo) are summarized in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). In 53 of these patients, recurrence occurred in a single organ (53 sites), whereas the remaining 10 patients had recurrence in multiple sites (28 sites). The most common site of recurrence was the peritoneum (n = 19). Notably, recurrent lesions in the peritoneum were detected with substantially greater sensitivity in the primary tumor 18F-FDG–avid group (10/13) compared with the non-18F-FDG–avid group (1/6; P = 0.041). PET/CT in patients with 18F-FDG–avid primary tumor also detected recurrence in other sites with high sensitivity, including liver and lymph nodes.
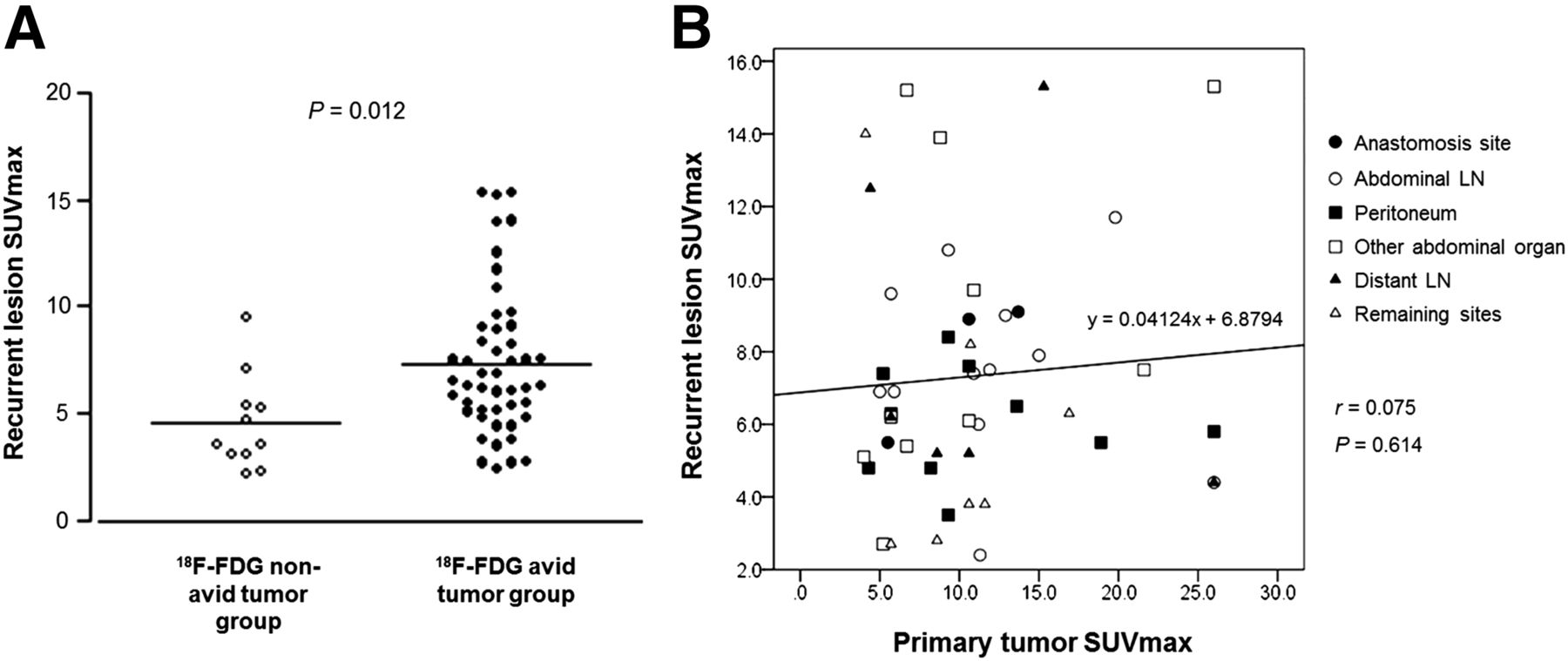
When we compared 18F-FDG uptake levels, patients with 18F-FDG–avid primary tumors showed significantly greater recurrent lesion SUVmax than those with 18F-FDG–nonavid primary tumors (7.3 ± 3.4 vs. 4.5 ± 2.2; Fig. 3A). However, linear regression was unable to show a significant correlation between primary tumor and recurrent lesion SUVmax (r = 0.075, Fig. 3B).

Relation between primary tumor and recurrent lesion 18F-FDG avidity. (A) Scatterplot comparing distribution of recurrent lesion SUVmax between patients with 18F-FDG–avid and –nonavid primary tumors. (B) Correlation analysis between recurrent lesion SUVmax and primary gastric tumor. LN = lymph node.
Other Variables That May Enhance Recurrence Detection
We additionally evaluated whether other tumor characteristics that are potentially linked with glucose metabolism may also provide stratification of patients with enhanced PET performance for detecting recurrence. Categorization into patients with (n = 11) and without signet ring cell carcinoma (n = 52) did not lead to significant difference in PET sensitivity for recurrence (63.6% vs. 73.1%). These groups also showed no difference in PET sensitivity when patients with anastomosis site recurrence were excluded (66.7% vs. 71.4%).
Patients with intestinal-type cancers (n = 23) had a significantly higher PET sensitivity for recurrence than those with diffuse-type cancers (n = 33; 91.3% vs. 54.5%; P = 0.003), and this remained true when patients with anastomosis site recurrence were excluded (90.1% vs. 51.7%; P = 0.003). Comparison of patients with intestinal-type cancer to those with all other cancer types (n = 40) also showed similar results when including (91.3% vs. 60%; P = 0.008) and excluding anastomosis site recurrence (90.1% vs. 58.3%; P = 0.011). However, the number of patients with intestinal-type cancers was only 54.8% (23/42) of that with 18F-FDG–avid primary tumor, limiting its usefulness. We therefore attempted to evaluate whether combining information of primary tumor 18F-FDG avidity and Lauren classification type can offer further benefit. However, all but 1 of the 23 patients with intestinal-type cancers and recurrent disease had 18F-FDG–avid primary tumors. As such, the addition of information on cell type or Lauren classification to that of primary tumor 18F-FDG avidity did not offer incremental benefit in augmenting sensitivity for recurrence.
There were 2 patients, among a total of 63 patients with recurrence, who did not have measurable disease by imaging studies including PET and contrast-enhanced CT. One patient had an 18F-FDG–nonavid primary tumor, and recurrence was diagnosed on the basis of a 3-fold rise of serum CA 19-9 that decreased by chemotherapy. The second patient had an 18F-FDG–avid primary tumor, and recurrence was diagnosed on the basis of development of intractable ascites.
Another 25 patients had recurrent lesions that were small. These were soft-tissue or hepatic lesions less than 2 cm, lymph nodes without enlargement, peritoneal enhancement or bowel wall thickenings without nodule formation, and anastomosis site lesions not seen on enhanced CT. PET had lower sensitivity for detecting these small lesions than larger recurrent lesions (56% vs. 86.1%; P = 0.009). In patients with small recurrent lesions, the primary tumors were 18F-FDG–avid in 14 cases and –nonavid in 11 cases, and PET sensitivity was 64.3% in the former group and 45.5% the latter group (P = 0.435).
DISCUSSION
This study demonstrates that the sensitivity of surveillance 18F-FDG PET/CT for detecting recurrent disease after curative resection of advanced gastric cancer is significantly enhanced by the 18F-FDG avidity of the resected primary tumor.
On initial staging PET/CT, 64.1% of the locally advanced primary gastric cancers in our study were 18F-FDG–avid. This rate of visible tumor 18F-FDG uptake is well within the 34%–94% range of sensitivity reported for PET/CT in detecting advanced gastric cancer (20). The wide range of reported sensitivity indicates that multiple factors influence the magnitude of gastric tumor 18F-FDG uptake. Gastric adenocarcinomas actually comprise a heterogeneous group of tumors with dissimilar biologic characteristics, which in turn can lead to divergent metabolic and bioenergetic properties. In our study, 18F-FDG–avid and –nonavid gastric cancers showed different histopathologic makeups. Although nonsignet ring cell type was more common in both groups, signet ring cell type was 3-fold more frequent in nonavid compared with avid tumors. This finding is consistent with previous observations that signet ring cell and mucinous type gastric cancers tend to have lower 18F-FDG uptake (11–13), a feature that has been attributed to lower glucose transporter-1 expression (12).
Lauren described 2 major gastric cancer types with distinct molecular pathogenesis and clinical–pathologic profiles. Intestinal-type gastric carcinomas occur more frequently in older subjects and are thought to arise from chronic gastritis that progress to intestinal metaplasia and dysplasia. Diffuse-type gastric carcinomas are more common in younger individuals and roughly correspond to poorly cohesive carcinomas of the World Health Organization classification. In our study, intestinal-type tumors occurred more frequently in 18F-FDG–avid than –nonavid tumors, whereas the reverse was true for diffuse-type tumors. Several previous studies showed higher 18F-FDG uptake intestinal-type than diffuse-type gastric cancers (4,11,21,22). Although the mechanism has not been clearly elucidated, greater mucin content in diffuse-type cancers has been proposed as an explanation for this phenomenon (21).
Patients with 18F-FDG–avid primary tumors in our study were also slightly less likely to have lower T stage (T2) and N stage (N0) disease at presentation. These findings are in line with previously described associations between degree of 18F-FDG uptake and tumor invasion depth or nodal involvement (14,21,22) and may be explained by aggressiveness of tumors that have high glycolytic activity. Small tumors can cause underestimation of 18F-FDG measurements by partial-volume effects, but primary tumor size between 18F-FDG avidity groups was not different in our study.
During a mean clinical follow-up of 38.1 mo, recurrent disease was diagnosed in 19.6% of our study subjects. However, despite the slightly higher T and N stage of patients with 18F-FDG–avid primary tumors, the recurrence rate and duration to recurrence were not different between tumor 18F-FDG avidity groups. Tumor 18F-FDG uptake levels have been shown to have significant prognostic associations in various types of malignancies. However, there have been limited data regarding the relation between tumor 18F-FDG uptake level and outcome of patients with gastric cancer. Indeed, previous reports have shown inconsistent results, possibly from differences in proportion of histopathologic subtypes among study populations (15,16,23). For instance, signet ring cell carcinomas and other poorly differentiated tumors with attenuated cell densities generally have low 18F-FDG uptake even though they carry adverse prognosis.
Compared with advanced gastric cancer, early gastric cancers are known to have low 18F-FDG uptake (22) and are associated with a low rate of recurrence. Our database showed 324 early gastric cancer patients who underwent follow-up PET/CT during the same time period of our study population, but only 1 of these patients developed recurrent disease. This is consistent with the report by Sano et al., in which early gastric cancer was estimated to have a recurrence rate of only 1.9% (24). This is the reason patients with early gastric cancers were excluded in our study.
When we investigated the performance of PET for detecting recurrent disease in the entire study population, a diagnostic sensitivity of 71.4% was obtained, which is similar to the 78% recently reported by a meta-analysis study (7). PET sensitivity in our study was similar regardless of whether or not cases with locoregional recurrence were included. The specificity reported in the meta-analysis by Wu et al. was 82% (7). A significant number of false-positive results arise from nonspecific physiologic radioactivity in the anastomosis site or remnant stomach, but these recurrences can be readily excluded by endoscopic surveillance. Furthermore, distant, rather than locoregional, recurrence is responsible for most patient deaths (3). Therefore, when analyzing PET specificity, we considered mild activity on remnant stomach and anastomosis sites as nonspecific findings. As a result, we obtained a high overall PET specificity of 97.3% for detecting recurrent disease.
Using an SUVmax threshold of 4.0, we compared the performance of PET for detecting recurrent disease in 18F-FDG–avid and –nonavid primary tumor groups. The results revealed that patients with 18F-FDG–avid primary tumors had a significantly greater diagnostic sensitivity than those with 18F-FDG–nonavid tumors, whether or not cases with local recurrence were excluded from the analysis. Hence, the former group had a moderate sensitivity of 81.0% (82.1% when excluding local recurrence) for 18F-FDG PET/CT in detecting recurrent disease. The diagnostic specificity was similarly high for both groups. Taken together, these results indicate that 18F-FDG avidity of the primary gastric cancer on initial PET may help select patients likely to benefit from follow-up PET studies. When PET was performed for suspicion of recurrence, cases with 18F-FDG–avid and –nonavid primary tumors both had higher sensitivity than cases with 18F-FDG–nonavid tumors undergoing PET for surveillance. This indicates that whereas routine follow-up PET/CT may be efficient only for 18F-FDG–avid primary tumors, it may benefit patients with both 18F-FDG–avid and 18F-FDG–nonavid tumors when recurrence is suspected.
We performed receiver-operating-characteristic curve analysis to evaluate how different SUVmax thresholds would influence performance of scans in patients with 18F-FDG–avid primary tumors. As a result, PET sensitivity and specificity were 76.1% and 97.3% for SUVmax 3.0, 77.8% and 97.2% for SUVmax 3.5, 81.0% and 97.1% for SUVmax 4.0, and 78.9% and 97.1% for SUVmax 4.5. These findings show that the results are not remarkably affected by the choice of SUVmax threshold. A value of 4.0 also coincides with the observation by Salaun et al. that 18F-FDG uptake in the stomach with a lower SUVmax is usually associated with benign rather than malignant disease (25). Although all primary tumors with discernable 18F-FDG uptake in our study had an SUVmax of more than 3.0, a value of 4.0 corresponded to the 5 percentile SUVmax among such tumors. As such, 17 patients with discernable primary tumor 18F-FDG uptake had an SUVmax between 3.0 and 4.0 and were categorized as 18F-FDG–nonavid tumors.
The compositions of cell types and Lauren classification were found to be different between 18F-FDG–avid and –nonavid primary tumor groups. Given that these differences may themselves influence tumor metabolic profile, we investigated whether histopathologic findings can also help select subjects with improved PET sensitivity for recurrence. The results showed that classification of patients according to signet ring cell types does not affect PET sensitivity. On the other hand, classification according to intestinal-type cancers significantly increased PET sensitivity. However, a substantially smaller portion of patients had this characteristic than tumor 18F-FDG avidity. Furthermore, as it turns out, all but 1 recurrence patient with intestinal-type cancer showed 18F-FDG–avid tumors on initial PET/CT (22/23), whereas only 52.4% (22/42) of those with an 18F-FDG–avid tumor had intestinal-type cancer. These findings support that 18F-FDG avidity of primary tumors is a significantly more robust method to select patients with higher PET/CT sensitivity for recurrence.
Detection performance for recurrent gastric cancer may differ according to involved site. In particular, peritoneal involvement is notoriously difficult to detect by 18F-FDG PET (8,26). We also found a low overall PET sensitivity of 57.9% for detecting peritoneal recurrence. Among scans of patients with 18F-FDG–avid primary tumors, however, PET sensitivity for peritoneal recurrence was increased to 76.9%. In contrast, the sensitivity was reduced to 16.7% for scans of patients with nonavid primary tumors. Other sites of recurrence also showed a trend for higher sensitivity in the 18F-FDG–avid than the –nonavid group. Therefore, PET appeared to detect recurrent disease better in all sites including the peritoneum in patients who had 18F-FDG–avid primary tumors.
The mechanism for the greater PET sensitivity for recurrence evidently lies in the similarity of biologic characteristics between primary and recurrent malignant lesions. This is supported by the significantly greater level of 18F-FDG uptake in recurrent lesions for scans of patients whose primary tumors had higher uptake. Although the positive relation between the level of 18F-FDG uptake by primary and recurrent lesions did not reach statistical significance, this is to be expected given the different sizes and divergent environment of the recurrent compared with the primary tumor.
This study is limited by its retrospective design with a nonsystematic and nonstandardized follow-up imaging schedule. As such, further investigations will be required to help establish an 18F-FDG PET/CT follow-up algorithm for gastric cancer patients after curative resection.
CONCLUSION
The sensitivity of PET for detecting recurrent disease after curative resection is significantly enhanced in patients with 18F-FDG–avid primary gastric cancers. Hence, follow-up PET for surveillance of possible recurrence may be better suited for cases that have high 18F-FDG uptake of the primary tumor on initial PET studies.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported by a grant of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 17, 2015.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 8, 2015.
- Accepted for publication November 20, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.