


Visual Abstract

Abstract
Gastrin-releasing peptide receptors (GRPRs) are potential molecular imaging targets in a variety of tumors. Recently, a 68Ga-labeled antagonist to GRPRs, NeoBOMB1, was developed for PET. We report on the outcome of a phase I/IIa clinical trial (EudraCT 2016-002053-38) within the EU-FP7 project Closed-loop Molecular Environment for Minimally Invasive Treatment of Patients with Metastatic Gastrointestinal Stromal Tumors (‘MITIGATE’) (grant agreement no. 602306) in patients with oligometastatic gastrointestinal stromal tumors (GIST). Methods: The main objectives were evaluation of safety, biodistribution, dosimetry, and preliminary tumor targeting of 68Ga-NeoBOMB1 in patients with advanced tyrosine-kinase inhibitors–treated GIST using PET/CT. Six patients with histologically confirmed GIST and unresectable primary lesion or metastases undergoing an extended protocol for detailed pharmacokinetic analysis were included. 68Ga-NeoBOMB1 was prepared using a kit procedure with a licensed 68Ge/68Ga generator. 68Ga-NeoBOMB1 (3 MBq/kg of body weight) was injected intravenously, and safety parameters were assessed. PET/CT included dynamic imaging at 5, 11, and 19 min as well as static imaging at 1, 2, and 3–4 h after injection for dosimetry calculations. Venous blood samples and urine were collected for pharmacokinetic analysis. Tumor targeting was assessed on a per-lesion and per-patient basis. Results: 68Ga-NeoBOMB1 (50 μg) was prepared with high radiochemical purity (yield > 97%). Patients received 174 ± 28 MBq of the radiotracer, which was well tolerated in all patients over a follow-up period of 4 wk. Dosimetry calculations revealed a mean effective dose of 0.029 ± 0.06 mSv/MBq, with the highest organ dose to the pancreas (0.274 ± 0.099 mSv/MBq). Mean plasma half-life was 27.3 min with primarily renal clearance (mean 25.7% ± 5.4% of injected dose 4 h after injection). Plasma metabolite analyses revealed high stability; metabolites were detected only in the urine. In 3 patients, a significant uptake with increasing maximum SUVs (SUVmax at 2 h after injection: 4.3–25.9) over time was found in tumor lesions. Conclusion: This phase I/IIa study provides safety data for 68Ga-NeoBOMB1, a promising radiopharmaceutical for targeting GRPR-expressing tumors. Safety profiles and pharmacokinetics are suitable for PET imaging, and absorbed dose estimates are comparable to those of other 68Ga-labeled radiopharmaceuticals used in clinical routine.
Radiolabeled peptides for diagnosis and therapy of various malignancies have been a cornerstone of radiopharmaceutical development over the past decades with 68Ga as the mainstay of modern PET-based tumor imaging. The clinical utility of the “thera(g)nostic” approach has peaked in the products recently obtaining marketing authorization for diagnosis (68Ga-DOTATOC as SOMAKit TOC in Europe and 68Ga-DOTATATE as NETSPOT in the United States; Advanced Accelerator Applications) and therapy (177Lu-DOTATATE as Lutathera; Advanced Accelerator Applications), stimulating research on regulatory peptides binding to other receptors (1). One of main targets in this area are gastrin- releasing peptide receptors (GRPRs), which are overexpressed in a variety of cancers including prostate (2–6) and breast cancer (7) as well as glioma (8,9).
A variety of radiolabeled peptides binding to GRPRs, derived from the natural ligand bombesin, have been developed (10). However, early bombesin analogs with agonistic properties led to a high rate of unwanted side effects (11), thus shifting focus toward antagonistic bombesin analogs, avoiding side effects and possibly leading to higher targeting efficiency and metabolic stability.
NeoBOMB1 is a novel DOTA-coupled GRPR-antagonist generated by modification of the C-terminal Leu13-Met14-NH2 of native bombesin. It can be labeled with 68Ga, resulting in high GRPR affinity, metabolic stability, and excellent tumor targeting in various animal models (12,13).
Gastrointestinal stromal tumors (GIST), a rare sarcoma subtype with an incidence of 4.3–22 per million (14,15), express high levels of GRPR (16). Eighty to eighty-five percent of patients with GISTs present localized disease at first diagnosis, but metastases are a frequent phenomenon during the course of the disease in up to 85% of patients (17). Tyrosine kinase inhibitors (TKIs) such as imatinib, sunitinib, or regorafenib have dramatically improved overall survival (18), yet up to 80% of patients develop resistance during therapy (19). A study within the EU-FP7 project Closed-loop Molecular Environment for Minimally Invasive Treatment of Patients with Metastatic Gastrointestinal Stromal Tumors (‘MITIGATE’, grant agreement no. 602306) investigating several radiolabeled peptides on tumor cell lines revealed 68Ga-NeoBOMB1 to be a promising candidate for targeting GIST (16). Recently, the development of a new kit formulation for the preparation of 68Ga-NeoBOMB1 (Advanced Accelerator Applications; Colleretto Giacosa TO, Italy) has allowed radiolabeling without complex synthesis and purification procedures.
Here we report on safety, tolerability, pharmacokinetics, and preliminary targeting properties of 68Ga-NeoBOMB1. These data originated from the first part of a prospective clinical phase I/IIa in patients with advanced GIST under current or previous TKI treatment (“A Phase I/IIa study to evaluate safety, biodistribution, dosimetry and preliminary diagnostic performance of 68Ga-NeoBOMB1 in patients with advanced TKI-treated GIST using positron-emission tomography/computer tomography (PET/CT)”, EudraCT no. 2016-002053-38).
MATERIALS AND METHODS
Study Approval and Registration
Study approval was granted on July 25, 2016, by the local Ethical Review Board (Ethics Committee Medical University Innsbruck), and on November 28, 2016, by the Austrian Competent Authority (Bundesamt für Sicherheit im Gesundheitswesen). All participants signed a written informed consent form. Monitoring was provided by the local Clinical Trial Centre (KKS, MUI). The study was registered both within EudraCT (2016-002053-38) and ClinicalTrials.gov (NCT02931929) and was officially initiated in December 2016.
Subjects, Study Plan, and Safety Assessment
Overall, 6 patients with advanced GIST—defined as metastatic disease without a curative surgical option—were enlisted for full pharmacokinetic analysis, representing a subset of a total of 9 patients enrolled in the study. At least 50% of patients were required to have a first-, second-, or third-line TKI resistance defined by disease progress under treatment. Disease progress was classified by imaging (usually by Choi criteria (20)). To minimize a bias of patients with a greater disease burden, 2 patients with a stable disease were also included. Details on disease status and treatment are provided in Table 1.
Patient Characteristics, Injected Doses, and 68Ga-NeoBOMB1 Lesion Uptake
Detailed inclusion and exclusion criteria are provided in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). Oral and written informed consent was obtained from all participants.
The occurrence of adverse events and severe adverse events were documented and graded in regard to severity and causal correlation to the administration of 68Ga-NeoBOMB1 following the Common Terminology Criteria for Adverse Events (version 5.0; National Institutes of Health).
Participants were screened and enrolled at least 24 h before the tracer administration (visit 0) after review of inclusion and exclusion criteria, medical history, and physical status. A pregnancy test was performed in female participants via a urine dipstick test.
Before the tracer administration (visit 1), inclusion and exclusion criteria, medical history, and physical status were reviewed again. Serial venous blood samples were taken at 0, 2, 5, 10, 30, and 45 min and 1, 2, and 3–4 h after tracer administration. Furthermore, 1 urine sample was taken before and at least 1 urine sample after administration. Patients were hospitalized for observation until the next morning, reexamined (visit 2), and discharged if no adverse events were observed.
The follow-up examinations (visit 3) took place 5–8 d after tracer administration and included physical examination, history, and blood analysis. A final telephone interview (visit 4) was conducted 12–20 d after the tracer administration. Patients were advised to readily report any abnormalities to the investigators at any time for the study duration and beyond. A flow chart of the study plan is provided in Supplemental Figure 1.
Preparation, Quality Control, Pharmacokinetics, and Metabolite Analysis of 68Ga-NeoBOMB1
A kit-based preparation was used for 68Ga-NeoBOMB1 (technical details on preparation, quality control, pharmacokinetic, and metabolite analysis are provided in Supplemental Appendix 1) (21).
PET Imaging
Patients were intravenously injected with 127–214 MBq of 68Ga-NeoBOMB1 (on average 174 ± 28 MBq), corresponding to the total content of the kit. A 5 × 60 s dynamic PET/CT scan of the upper abdomen (1 bed position with an axial field of view of 15.6 cm) was started immediately after tracer injection, followed by 3 sequential static PET/CT scans covering the whole abdomen and pelvis (3 bed positions with 2 min per bed position) at 5, 12, and 19 min after injection and 3 late PET/CT scans from the skull vertex to the mid thigh (7 bed positions, 2 min per bed position) at 1, 2, and 3 h after injection. In total, 5 low-dose CT scans were obtained for attenuation correction of the PET emission data (one for the dynamic PET/CT, one for the time points from 5 to 19 min, and one for each of the later time points; low-dose CT scan parameters using BGE smart mA dose modulation: 100 kVp, 15–150 mA, noise index 60, tube rotation 0.8 s, slice thickness 3.75 mm, and pitch 1.375).
All scans were acquired using a Discovery PET/CT 690 VCT scanner (GE Healthcare). PET images were reconstructed using an ordered-subset expectation maximization algorithm with 2 iterations and 24 subsets for static images and 32 subsets for dynamic images. The PET images were normalized to units of Bq/mL by applying corrections for sensitivity, attenuation, scatter, dead-time, and random coincidences and for decay to image acquisition onset.
Positron emission data were reconstructed using an ordered-subset expectation maximization algorithm (2 iterations, 24 subsets). The images were corrected for attenuation using CT data collected over the same regions as for emission imaging.
CT Imaging
If no recent CT of the thorax and abdomen was available, a diagnostic whole-body CT was acquired after the third whole-body PET procedure 3 h after injection, following body weight–adjusted intravenous administration (1.5 mL/kg of body weight) of iopromid (Ultravist 370; Bayer AG). BGE smart mA dose modulation was used (100–120 kVp, 80– 450 mA, noise index 24, tube rotation 0.8 s, slice thickness 3.75 mm, and pitch 0.984).
Image Analysis
For image analysis, Hermes software (version P5 gold 4.4-B; Hermes Medical Solutions AB) was used. To determine the temporal enhancement, representative organ regions of interest were used to measure SUVs then converted into percentage injected dose per volume (%ID/L). To determine ideal imaging time windows, tumor-to-organ ratios for the liver, kidney, and pancreas were calculated in patients with discernible tumor uptake (presented as imaging indices). Lesion tracer uptake was visually assessed using Hermes software on a per-patient and per-lesion-basis, qualitative results and percentage of positive lesions were grouped by primary/local recurrence, and metastases are presented in tabular format.
Dosimetry Calculations
Dosimetry calculations were performed using OLINDA/EXM, covering organ and tumor regions of interest to determine time–activity curves (details are described in Supplemental Appendix 1) (22–25).
Statistics and Visual Presentation
All data were collected and stored in Microsoft Excel (Microsoft Corp.). Statistical analysis was performed in GraphPad Prism 8.1.1 (GraphPad Software Inc.).
Continuous data are presented as dot-plots, including mean and SD. Alternatively, data are presented as bars with whiskers denoting the SD.
PET/CT images are presented according to the AQARA principle (26).
RESULTS
Preparation of 68Ga-NeoBOMB1
68Ga-NeoBOMB1 was prepared with a radiochemical purity of greater than 97%. Radiolabeling timing was performed so that all patients received the total kit content, corresponding to an amount of approximately 50 μg of NeoBOMB1 peptide. Injected activity was between 127 and 214 MBq, dependent on body weight.
Participants, Tolerability, and Adverse Effects
The average age was 68.7 ± 11.5 y, and 4 of 6 participants were female (66.7%). Details on demographics and disease state are summarized in Table 1.
Intravenous administration of 68Ga-NeoBOMB1 was well tolerated in all participants. No serious adverse events were observed; minor adverse events after the administration of 68Ga-NeoBOMB1 were observed in 1 participant (16.7%), yet without a causal relation to the tracer administration (details on preexisting conditions can be found in the Supplemental Table 2). All adverse events had resolved on the last study visit. Details are summarized in Supplemental Table 3.
Blood, Urine, and Metabolite Analysis
Results from analysis of 68Ga-NeoBOMB1 in venous blood, plasma, and urine samples of the 6 patients are summarized in Figure 1. 68Ga-NeoBOMB1 was rapidly eliminated from blood with less than 10% of the total injected activity measured after 3 h. Mean half-life in blood was 35 min with plasma activity levels practically identical, indicating no cellular bound radioactivity. The excreted injected activity in early and late urine samples was 10.6% and 17.2%, respectively, totaling 25.7% after 3 h (mean of n = 6). High-performance liquid chromatography analysis revealed mostly intact peptide in plasma samples with some hydrophilic metabolites detectable at 30 min and 1 h, whereas in urine only hydrophilic metabolites could be found in samples taken both at early and late time points. Retention times of metabolites in urine matched those of metabolites detected in blood, indicating high metabolic stability of 68Ga-NeoBOMB1 and rapid renal excretion.

Summary of pharmacokinetic analyses of 68Ga-NeoBOMB1 in blood and urine. (A) Time–activity curve in plasma and serum, mean values of 6 patients. (B) Mean urinary excretion (n = 6) at early and late time points as well as total after 3 h. (C) Typical radiochromatograms of 68Ga-NeoBOMB1: Reference (I); plasma, 5 min (II); plasma, 30 min, (III); plasma, 60 min (IV); urine, 40 min and 3 h, respectively (V and VI).
Pharmacokinetics and Tumor Accumulation
Liver uptake was immediate at 13.4 %ID/L on average, with a continuous decline over time (Fig. 2A). The highest 68Ga-NeoBOMB1 uptake was found in the pancreas, with a time-dependent increase in activity especially in the head and corpus and highest dose values at the end of the examination up to 45.6 %ID/L, suggesting specific binding (Fig. 2B). Excretion was mainly renal, with immediate significant renal uptake plateauing around 20 %ID/L and concomitant activity accumulation along the ureters and bladder (Fig. 2F). Nonetheless, a continuous increase in gallbladder activity was found over time up to 12.2 %ID/L on average at 3 h (Fig. 2A), hinting at a partial hepatobiliary clearance of 68Ga-NeoBOMB1. The esophagus, colon, and rectum all displayed visible accumulation, with low uptake ranging from 3 to 7 %ID/L with a time-dependent increase in activity in all participants. Spleen and blood-pool activity decreased rapidly, correlating well with in vitro measurements (Fig. 2F; please also refer to Fig. 1) and simultaneous increase in bladder activity.
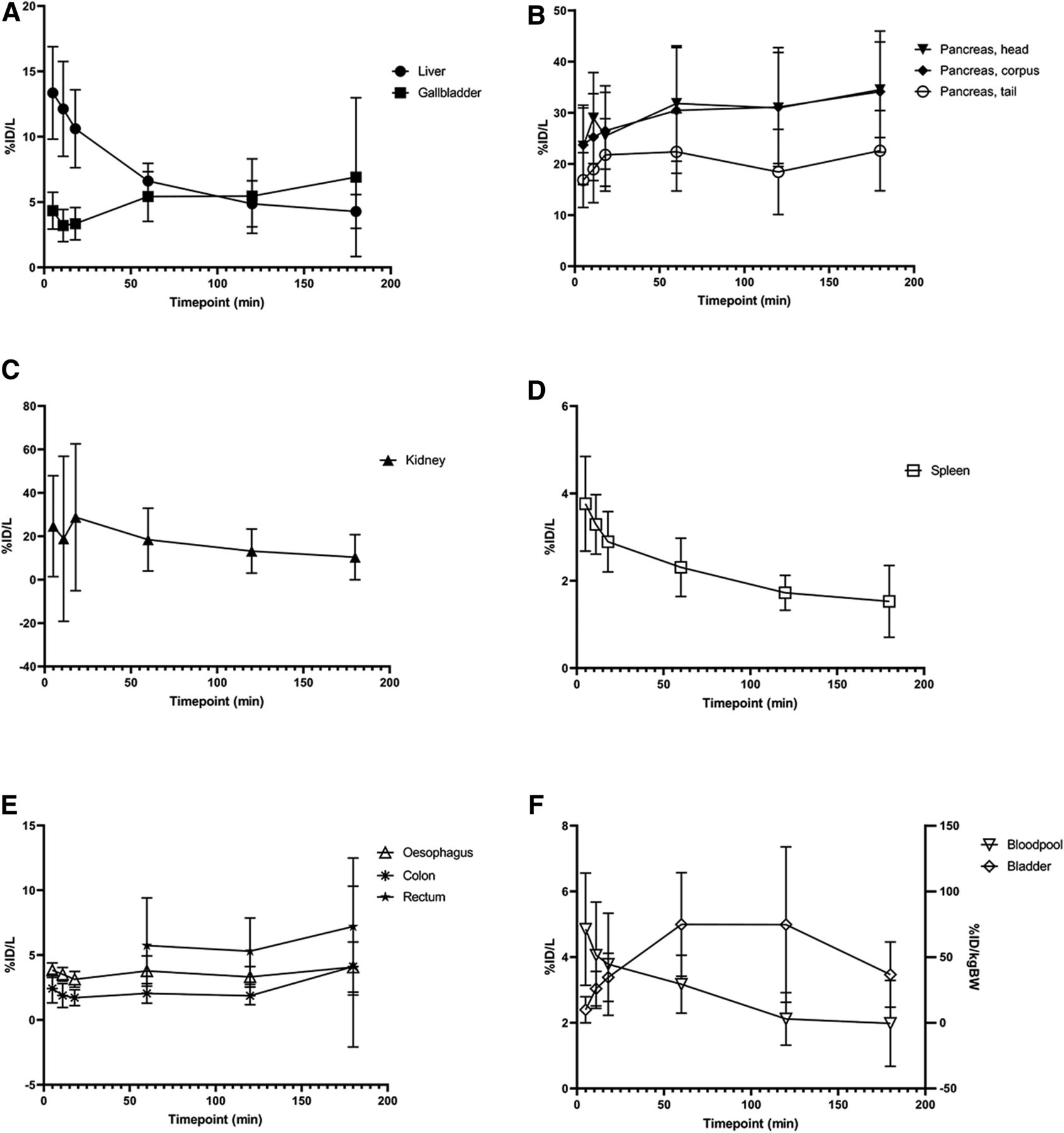
Organ-based pharmacokinetic data for liver and gallbladder (A); pancreatic head, corpus, and tail (B); kidneys (C); spleen (D); esophagus, colon, and rectum (E); as well as blood-pool (left y-axis) and bladder (right y-axis) (F). Note missing rectum values due to small field of view for early time points.
In 3 of 6 patients, a strong tumor uptake was found with a significant uptake starting 1 h after injection increasing over time, leading to an improved tumor-to-tissue contrast ratio. Two participants showed mixed lesion uptake, with a subset of lesions showing virtually no uptake; 1 patient exhibited no lesion uptake at all (additional details are provided in Table 1). Depending on the individual lesions, a ratio of up to 6.9 could be achieved at 2 h after injection (Supplemental Fig. 2). Noise levels were highest at 3 h after injection due to decay of 68Ga, indicating an optimal PET imaging time window between 1.5 and 2.5 h after injection. SUVmax reached 32.1 in 1 case. Figure 3 provides an exemplary illustration of tumor uptake over time (another case is presented in Supplemental Fig. 3).

68Ga-NeoBOMB1 PET/CT of participant 6 with GIST of ileum and histologically verified liver metastases. Maximum-intensity projections (left) and fused PET/CT images (right) at 5 min (A), 60 min (B), and 180 min (C) after injection (p.i.).
Dosimetry Calculations
Individual dose estimates (i.e., doses) after administration of 68Ga-NeoBOMB1 as well as the mean 68Ga-NeoBOMB1 doses and the SD of the 68Ga-NeoBOMB1 doses are presented in Supplemental Table 4. For these dose calculations, a bladder model with voiding every 2 h was considered. In this same table, doses for a well-established diagnostic radiopharmaceutical, 68Ga-DOTATATE, are also presented for comparison (no bladder voiding considered) (25).
As shown in Supplemental Table 3, the pancreas is by a large margin the organ receiving the highest dose after administration of 68Ga-NeoBOMB1 (mean 0.274 ± 0.099 mSv/MBq). Effective doses for 68Ga-NeoBOMB1 ranged from 0.022 to 0.040 mSv/MBq (mean 0.029 ± 0.06 mSv/MBq), which is in line with the reported effective dose for 68Ga-DOTATATE (0.026 mSv/MBq) (25). When compared with 68Ga-DOTATATE, 68Ga-NeoBOMB1 presented a much higher mean dose for the pancreas (by a factor of ∼15) and lower mean doses for the spleen and the kidneys (by factors of ∼0.05 and 0.5, respectively). The rest of the organs presented similar dose values between these two tracers. Higher doses for 68Ga-NeoBOMB1 in the pancreas are due to the high expression of GRPRs in this organ, which is the targeted receptor for NeoBOMB1 (27,28).
DISCUSSION
In this study, safety, tolerability and dosimetry of 68Ga-NeoBOMB1, a novel PET radiopharmaceutical targeting GRPRs were evaluated in 6 patients with metastasized GIST, representing the phase I of the MITIGATE-NeoBOMB1 trial (EudraCT no. 2016-002053-38). Details from phase IIa regarding GIST-targeting properties in all patients will be reported separately.
In contrast to other bombesin derivates, which mainly have agonistic effects, NeoBOMB1 constitutes a GRPR antagonist, potentially reducing the incidence of side effects. Bombesin antagonists have demonstrated properties superior to their agonist counterparts, leading to improved tumor uptake and lower accumulation in physiologic GRPR-expressing nontarget tissues (29,30). Furthermore, side effects are lower compared with agonistic bombesin derivates because of lower internalization rates and consequent physiologic activity (11). NeoBOMB1 is a part of a family of recently described GRPR antagonists for clinical application, mainly labeled with 68Ga (5) or 18F (3).
Metabolic stability was very high, with no detectable peptide fractions in full blood samples, in contrast to other agents such as SB3, probably because of C terminus stabilization (28). Human pharmacokinetics have been reported only for BAY 86-7548, which appeared less stable with only 19% of peptide intact in plasma 1 h after administration (5).
No causally related adverse events were observed, as only transient mild neutrophilia and hypophosphatemia with a Common Terminology Criteria for Adverse Events grade of 1 were encountered in 1 participant, most likely caused by the participant’s advanced disease stage or intake of sunitinib. No serious adverse events were observed.
After intravenous administration, rapid renal clearance was observed, with an increase in gallbladder activity over time, hinting at a relatively minor hepatic clearance, in line with the small and hydrophilic nature of the peptide. The highest organ accumulation was observed in the pancreas—increasing over time, suggesting specific binding to pancreatic GRPRs as described in rats (31). Further apparent physiologic accumulation was found in the gastrointestinal system, notably esophagus, colon, and rectum.
Radiation doses were found comparable to other 68Ga radiopharmaceuticals, supporting the suitable safety profile of 68Ga-NeoBOMB1 (5,25,32,33). As expected, the pancreas with its high physiologic expression of GRPR represents the organ receiving the highest radiation dose. Even though not within the primary scope of the study, tumor uptake was also examined. Reubi et al. have already demonstrated a high rate of bombesin-subtype 2 receptor expression in GIST lesions (34), regardless of primary or metastatic lesion nature. In our study population, tumor accumulation was observed, with the highest tumor-to-organ ratio at 2 to 3 h after administration. Even if negative in 1 participant and mixed in 2 participants (exemplary Fig. 4), tumor uptake was intense in the rest of participants (n = 3), suggesting viability for diagnosis and potentially treatment in a subset of patients with high levels of GRPR expression. This heterogeneity in tumor uptake is unclear, yet may represent changes in tumor biology after prolonged disease duration and under treatment pressure from TKIs, as most patients examined in this study had been diagnosed several years before the study participation. Probably because of the restricted number of participants, no clear correlation between disease duration, current treatment, mutational status, patient sex or age, and 68Ga-NeoBOMB1 uptake could be observed. Interestingly, in another study by Reubi et al. no correlation between receptor status and size, mitotic index, or presence of tumor necrosis could be found by even after therapy with imatinib or chemoembolization (34).
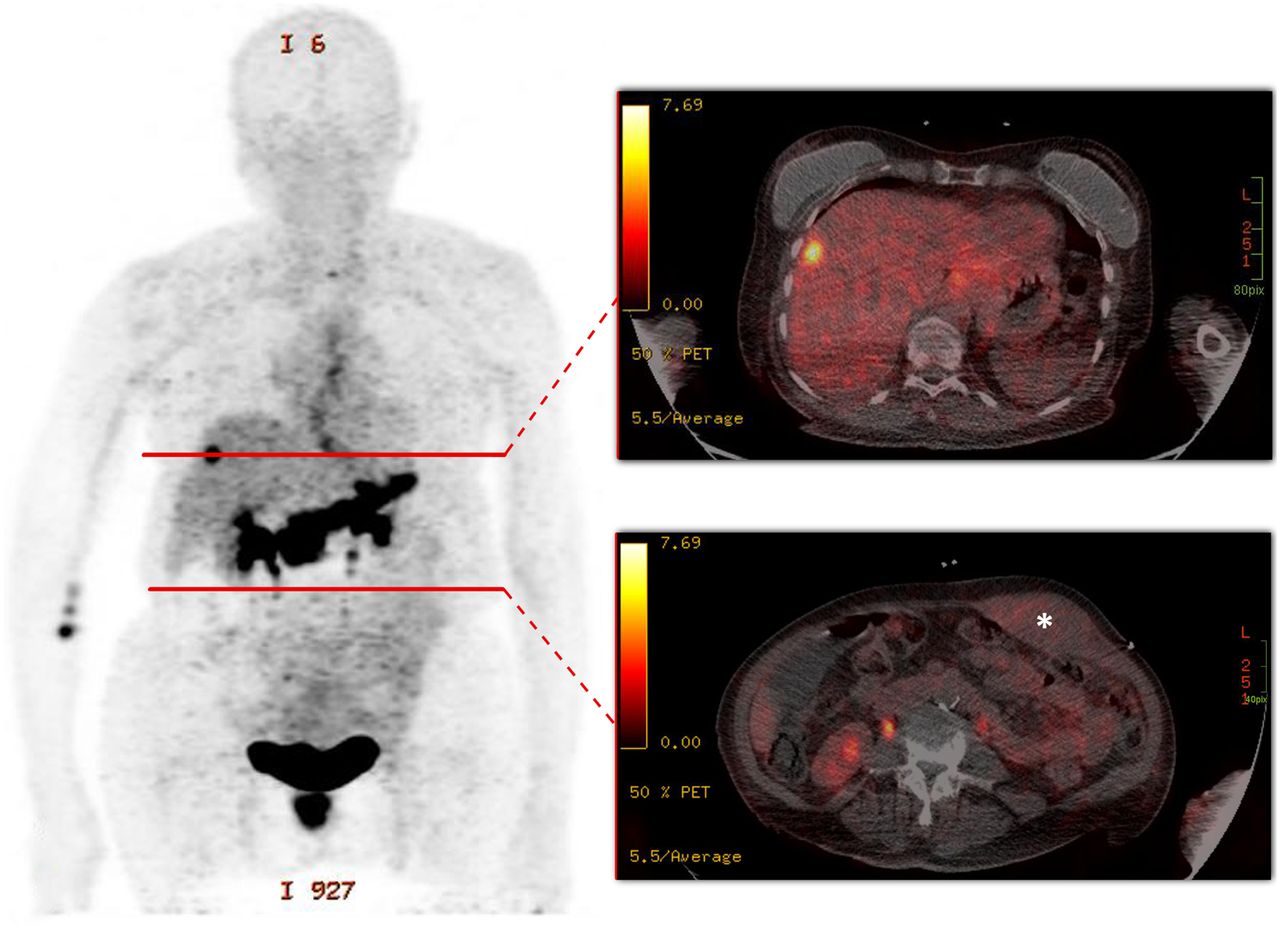
68Ga-NeoBOMB1 PET/CT of participant 1 with duodenal GIST and mixed tracer uptake illustrated by a maximum-intensity projection (left) and fused PET/CT images (right) at 1 h after administration. Strong tracer uptake was observed in a hepatic metastasis, and absent uptake was seen in a tumor formation invading abdominal wall (*). Red lines (left) denote the according section planes for axial PET/CT slices.
A major challenge in GIST-related studies is the low incidence rate. Further details on the diagnostic properties 68Ga-NeoBOMB1 in more patients will be presented separately. GRPR targeting, however, offers diagnosis of other tumor entities, which were also in the focus of studies with other bombesin analogs (2–12). PET imaging of other tumor entities expressing GRPR, such as breast, prostate, or lung cancers, with 68Ga-NeoBOMB1 is currently under investigation in a continuing phase II study, possibly also leading to a theragnostic pathway with the corresponding 177Lu counterpart.
CONCLUSION
68Ga-NeoBOMB1 is a novel, kit-based GRPR-targeting radiopharmaceutical. Our results show an excellent safety profile, low radiation dose, and apparent suitability for diagnostics of GRPR expression. 68Ga-NeoBOMB1 therefore is a promising radiotracer suitable for PET imaging of GRPR expression in oncologic patients and may open a pathway for therapeutic applications.
DISCLOSURE
This study was supported by the EU FP7 project Closed-loop Molecular Environment for Minimally Invasive Treatment of Patients with Metastatic Gastrointestinal Stromal Tumours ‘MITIGATE’ (grant agreement no. 602306). Advanced Accelerator Applications was one of the industrial partners in the ‘MITIGATE’ project. Francesca Orlandi and Maurizio Mariani were employees of Advanced Accelerator Applications at the time of the study. GiPharma is fully owned by Advanced Accelerator Applications. Irene Virgolini was principal investigator of the study EudraCT (2016-002053-38). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is the application of 68Ga-NeoBOMB1 safe for PET imaging applications, and what are the pharmacokinetics, radiation dose, and imaging properties of this novel radiopharmaceutical?
PERTINENT FINDINGS: This study was designed as a phase I/IIa clinical trial, and the outcome of the first 6 patients is reported. 68Ga-NeoBOMB1 showed an excellent safety profile, suitable pharmacokinetics, low radiation dose, and promising targeting properties in GIST tumors.
IMPLICATIONS FOR PATIENT CARE: 68Ga-NeoBOMB1 is a promising radiotracer suitable for PET imaging of GRPR expression in oncologic patients and opens a pathway for translation into a therapeutic approach
Acknowledgments
This article does not contain any studies with animals performed by any of the authors. All procedures performed in this study involving human participants were approved by the ethics committee of the Medical University of Innsbruck and the Austrian Competent Authority (BASG, EudraCT No. 2016-002053-38) and were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All participants signed a written informed consent form.
Footnotes
Published online Apr. 24, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 6, 2019.
- Accepted for publication March 28, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Safety, Biodistribution, and Radiation Dosimetry of the 68Ga-Labeled Minigastrin Analog DOTA-MGS5 in Patients with Advanced Medullary Thyroid Cancer and Other Neuroendocrine Tumors
- Head-to-Head Comparison of [68Ga]Ga-NOTA-RM26 and [18F]FDG PET/CT in Patients with Gastrointestinal Stromal Tumors: A Prospective Study
- Prospective Comparison of 68Ga-NeoB and 68Ga-PSMA-R2 PET/MRI in Patients with Biochemically Recurrent Prostate Cancer