


Abstract
We investigated whether the standardized uptake value (SUV) of the primary tumor, the tumor length measured on a PET image, the number of 18F-FDG PET-positive nodes, and the PET stage were independent prognostic predictors over other clinical variables in patients with esophageal squamous cell carcinoma who were undergoing curative surgery. Methods: Sixty-nine patients with newly diagnosed esophageal squamous cell carcinoma who underwent preoperative 18F-FDG PET and curative esophagectomy were included. The events for survival analysis were defined as recurrence or metastasis and cancer-related death. The disease-free and overall survival rates of each variable were estimated by the Kaplan–Meier method. The Cox proportional hazards model was used to evaluate independent prognostic variables for multivariate survival analysis. Results: Using univariate survival analysis, the presence of adjuvant therapy, pathologic stage, number of CT-positive nodes (0, 1, ≥2), tumor length on PET (cutoff: 3 cm, 5 cm), number of PET-positive nodes (0, 1, 2, ≥3), and PET stage (N0 M0, N1 M0, M1) were significant prognostic predictors for disease-free survival. However, only the number of PET-positive nodes was an independent significant prognostic predictor for disease-free survival in multivariate analysis (hazard ratio = 1.87, P < 0.001). In univariate survival analysis, the sex, presence of adjuvant therapy, clinical and pathologic stages, number of CT-positive nodes, maximum SUV of the primary tumor (cutoff: 6.3, 13.7), tumor length on PET, number of PET-positive nodes, and PET stage were significant prognostic predictors for overall survival. In contrast, the clinical stage (hazard ratio = 0.53, P < 0.05), pathologic stage (hazard ratio = 3.14, P < 0.005), tumor length by PET (hazard ratio = 2.74, P = 0.01), and number of PET-positive nodes (hazard ratio = 1.71, P < 0.05) were independent significant prognostic predictors for overall survival in multivariate analysis. Conclusion: In addition to the pathologic stage, 18F-FDG PET provides noninvasively independent prognostic information using the number of positive lymph nodes and the tumor length on the PET image in preoperative esophageal squamous cell carcinoma. A revised TNM classification system for esophageal carcinoma may consider tumor length and the number of positive lymph nodes as important prognostic factors.
Because esophageal cancer is associated with unfavorable prognosis, proper assessment of prognosis is necessary for treatment selection and follow-up planning. The depth of invasion and presence of lymph node metastasis are independent prognostic variables in esophageal cancer (1). Open esophagectomy with comprehensive lymph node dissection is the most accurate method for pathologic staging as well as the most common treatment method for esophageal cancer. However, this operation is frequently associated with significant morbidity, and a mortality rate from experienced institutes is reported in the range of 6%–7% (2). There are several noninvasive staging methods for esophageal cancer. Endoscopic ultrasound (EUS) and 18F-FDG PET have recently shown good results for clinical staging in esophageal cancer (3–9).
Current staging systems for esophageal cancer do not consider the number of metastatic lymph nodes or the tumor length as a prognostic factor (1). However, many studies reported that the number of pathologically proven malignant lymph nodes was one of the significant independent prognostic factors in esophageal cancer (10–14). No previous studies investigated whether the number of positive lymph nodes shown by noninvasive staging methods was a significant prognostic factor in esophageal cancer, except one study by EUS (9). Pathologically measured tumor length was also suggested to be an independent prognostic factor in esophageal cancer (14–17). No previous studies reported the relation between prognosis and tumor length measured by PET. The degree of 18F-FDG uptake in the primary tumor presenting as the standardized uptake value (SUV) was also associated with prognosis in esophageal cancer (8,18,19). However, it was unknown whether the SUV of the primary tumor was an independent prognostic factor in esophageal cancer.
In this study, we investigated whether the SUV of the primary tumor, tumor length measured by PET, number of 18F-FDG PET-positive nodes, and PET stage were independent prognostic predictors over other clinical variables in patients with esophageal cancer who were undergoing curative surgery.
MATERIALS AND METHODS
Subjects
Eighty-nine consecutive patients having newly diagnosed esophageal cancer between February 1997 and May 2000 were initially included in this prospective study. All patients underwent bone scintigraphy, esophagogastroduodenoscopy, bronchoscopy, EUS, abdominal ultrasonography, CT of the chest and upper abdomen, and 18F-FDG PET within 3 wk after diagnosis of esophageal cancer. Abdominal or neck CT and neck ultrasonography were performed when clinically indicated. In this study, all patients without distant organ metastasis or definite evidence of extensive tumor invasion to adjacent organs were routinely subjected to extensive regional lymph node dissection along with esophageal resection. We do not consider the presence of extensive or distant lymph node metastasis as a contraindication to surgical resection, as long as the nodes were included in the primary resection field. The ethics committee of our institution approved the protocol and informed consent was obtained from all subjects.
R0 resection of the primary mass was not accomplished in 1 patient, who was excluded from further analysis. Esophagectomy was not performed in 19 patients. Nine patients had surgically resectable disease but refused surgery. The remaining 10 patients were inoperable; 4 patients demonstrated distant metastatic lesions on preoperative staging tests including 18F-FDG PET, 3 had evidence of direct invasion to adjacent organs (main bronchus, thyroid gland, or epiglottis), 2 had poor medical conditions to overcome surgery, and 1 showed malignant omental seeding on laparotomy. The 19 patients who did not undergo esophageal resection were also excluded from further analysis. Therefore, a final total of 69 patients (64 men, 5 women; age, 41–77 y) with esophageal squamous cell carcinoma were included in the study.
PET
All patients fasted for at least 6 h before the PET study. PET scans were performed using an Advance PET scanner (General Electric Medical Systems). Emission scans were performed from thigh to head for 5 min per frame, 45 min after the intravenous injection of 370 MBq 18F-FDG. Tomographic images were reconstructed without attenuation correction by filtered backprojection with a Hanning filter (cutoff frequency = 8.0 mm) and displayed in a 128 × 128 matrix (pixel size = 4.29 × 4.29 mm with a slice thickness of 4.25 mm). In addition, attenuation-corrected images were acquired in the thorax or upper abdomen level by reconstruction using 10-min postemission transmission or preinjection transmission images with 68Ge rods.
Tomographic images displayed as coronal, sagittal, and transaxial slices were viewed on a Hewlett Packard workstation. Two nuclear physicians who were unaware of the CT and EUS findings and histologic results reviewed together and interpreted the PET images by consensus. The maximum SUV of the primary mass was acquired using the attenuation-corrected images, the amount of injected 18F-FDG, the body weight of each patient, and the cross-calibration factors between PET and the dose calibrator. Tumor length was measured from the number of transaxial slices in which the primary tumor was observed. In other words, the number of transaxial slices with the primary tumor multiplied by the slice thickness corresponded to tumor length. Lymph nodes were considered positive for malignancy if focal prominent 18F-FDG uptake, compared with normal mediastinal activity, was found in ≥2 consecutive transaxial slices. The number of PET-positive nodes and the PET stage (N0 M0, N1 M0, M1) in each patient were recorded (1).
Staging
The conventional preoperative clinical stage of each patient was determined by bone scintigraphy, esophagogastroduodenoscopy, bronchoscopy, EUS, abdominal ultrasonography, and CT. The detailed protocol and interpretation of CT and EUS were described in our previous study (4).
All patients underwent transthoracic esophagectomy with either 2-field (thoracoabdominal; n = 51) or 3-field (thoracoabdominal and cervical; n = 14) lymph node dissection, except 4 patients who underwent transhiatal esophagectomy. A thoracic surgeon dissected all visible or palpable lymph nodes within the surgical field, taking into consideration all of the results from the preoperative studies, including 18F-FDG PET. Each dissected nodal group was labeled according to the modified lymph node mapping system for esophageal cancer (4), and the nodes of each group were examined histopathologically for the presence of malignant cells. The location, depth, length, cell type, and degree of differentiation of the resected primary tumor were also examined histopathologically. Clinical and pathologic stages of each patient were determined according to the TNM system (1).
Clinical Follow-Up
Adjuvant therapy, including radiation therapy and chemotherapy after surgery, was performed according to each patient’s situation and the corresponding physician’s decision. After surgery, all patients were monitored regularly to obtain accurate information regarding recurrence. The follow-up program was every 2–4 mo during the first year, every 4–6 mo during the next 2 y, and every year thereafter. Every follow-up evaluation included a complete physical examination, complete blood count, biochemical screening, and chest x-ray. CT scans of the chest and upper abdomen were performed every 6 mo to 1 y or more frequently if clinically indicated. Other tests, including barium contrast esophagography, esophagogastroduodenoscopy, and ultrasonography or CT of the neck and abdomen, were also performed if clinically indicated.
Recurrence or metastasis was considered when there was an abnormal finding suggesting recurrence or metastasis on serial imaging studies or pathologically confirmed malignancy. The events for survival analysis were defined as recurrence or metastasis and cancer-related death. The disease-free and overall survival durations to the last follow-up were recorded for each patient.
Data Analysis and Statistics
The disease-free and overall survival rates for each variable were estimated by the Kaplan–Meier method (20). Equivalences of the survival curves were tested with log rank statistics. The Cox proportional hazards model with likelihood-ratio statistics based on the conditional parameter estimate was used to evaluate independent prognostic variables for multivariate survival analysis (21).
Clinical variables for univariate survival analysis included age, sex, location of primary site, cell type of tumor, histologic grade of primary tumor, performance of adjuvant therapy, clinical and pathologic stages, number of CT-positive nodes, maximum SUV of primary tumor, tumor length measured on PET, number of PET-positive nodes, and PET stage. Only significant variables after univariate survival analysis (P < 0.1) were included in multivariate survival analysis. Numeric data were expressed as the mean ± SE, if not described.
RESULTS
Demographic Data
The characteristics of patients and tumors are given in Table 1. The mean age at the time of diagnosis was 63 y. More than 90% of patients were male. Most of the tumors were invasive squamous cell carcinoma. The majority of tumors originated from the middle and lower esophagus. All patients with stage IV disease had nonregional lymph node metastasis without distant organ metastasis.
Characteristics of Patients with Esophageal Cancer Included in Study and Results of Univariate Survival Analysis
There were 130 malignant nodal groups of 554 dissected nodal groups in 43 of 69 patients on pathologic examination. Ninety-six positive lymph nodes in 43 patients were evident on 18F-FDG PET. Only 30 lymph nodes were positive in 24 patients on CT. EUS revealed lymph node metastases in 27 patients. EUS could not be completed in 27.5% of patients (19/69) due to esophageal stenosis.
Survival Data
At the time of the last follow-up, 33 patients were alive and had no evidence of disease, 5 were alive with recurrent esophageal cancer, 24 had died of esophageal cancer, and 7 had died due to intercurrent illness (n = 5) or postoperative complications (n = 2).
After univariate survival analysis, the performance of adjuvant therapy, pathologic stage, number of CT-positive nodes, tumor length on PET, number of PET-positive nodes, and PET stage were found to be significant prognostic predictors for disease-free survival (Table 1). After multivariate analysis, the performance of adjuvant therapy and number of PET-positive nodes was shown to be an independent significant prognostic predictor for disease-free survival (Table 2).
Results of Multivariate Survival Analysis for Predicting Disease-Free Survival and Overall Survival
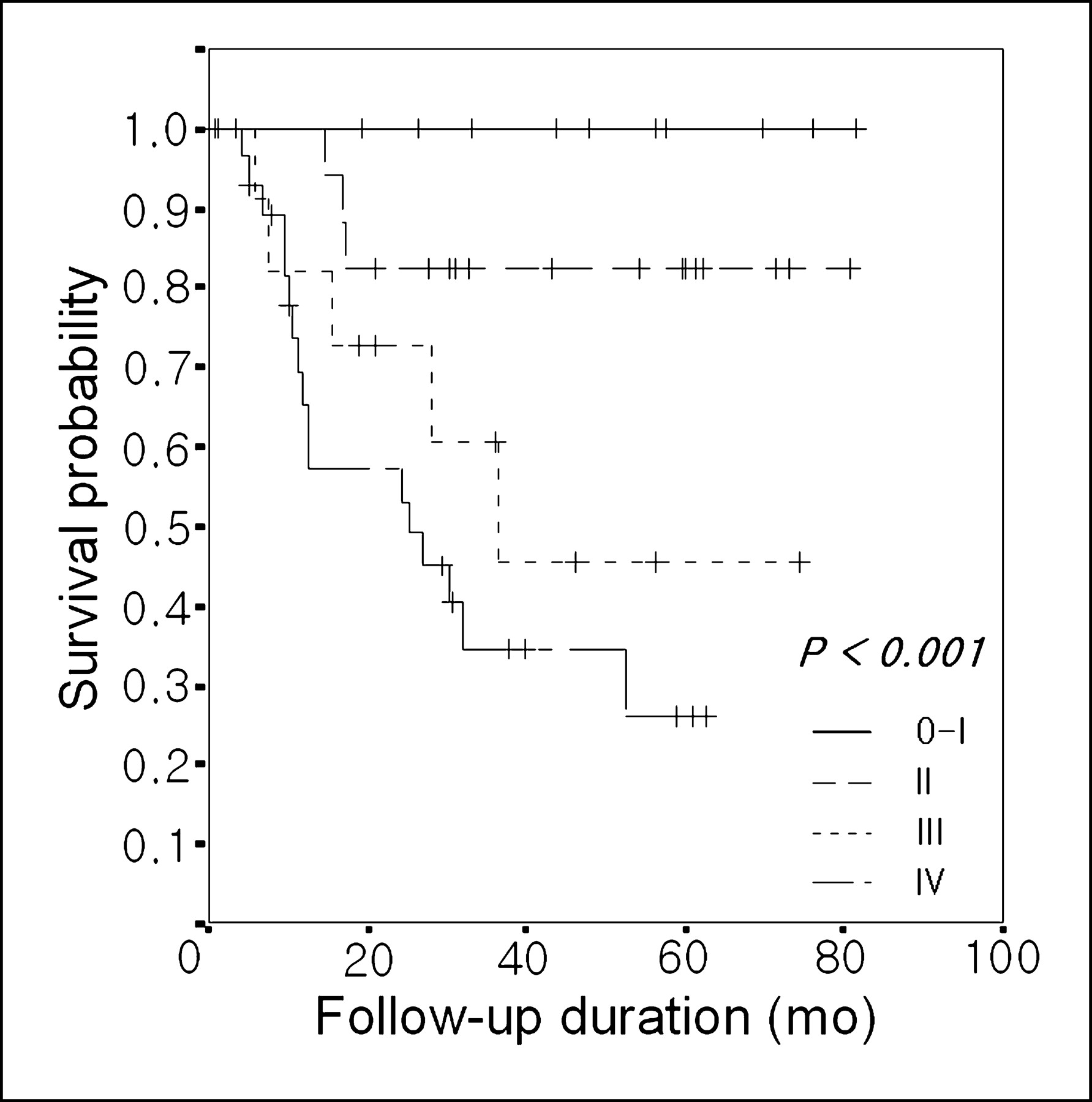
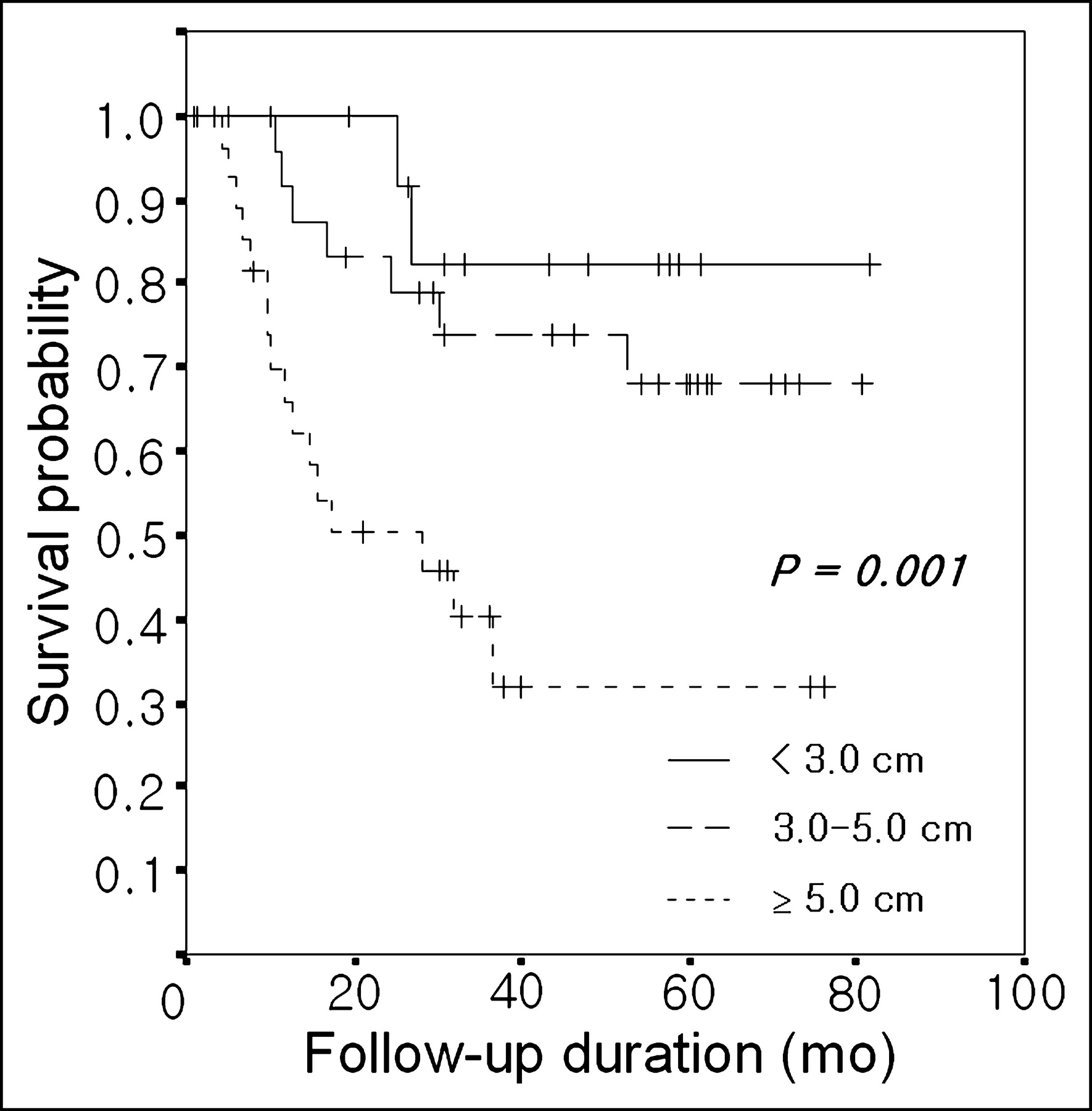
After univariate survival analysis, the sex, performance of adjuvant therapy, clinical and pathologic stages, number of CT-positive nodes, maximum SUV of primary tumor, tumor length on PET, number of PET-positive nodes, and PET stage were significant prognostic predictors for overall survival (Table 1). After multivariate analysis, the clinical stage, pathologic stage, tumor length on PET, and number of PET-positive nodes were independent significant prognostic predictors for overall survival (Table 2; Figs. 1–3).
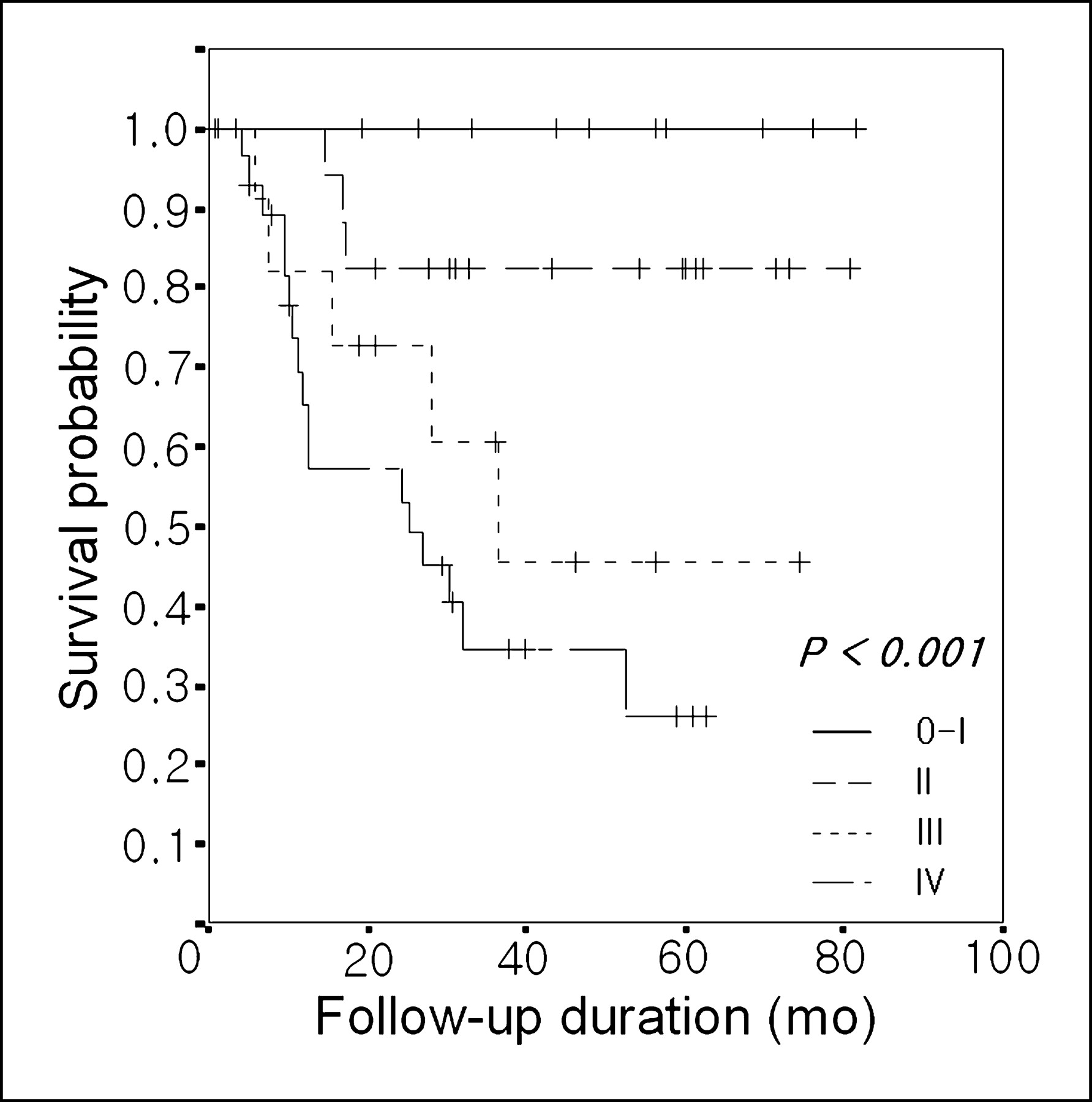
Overall survival curves according to pathologic stage.
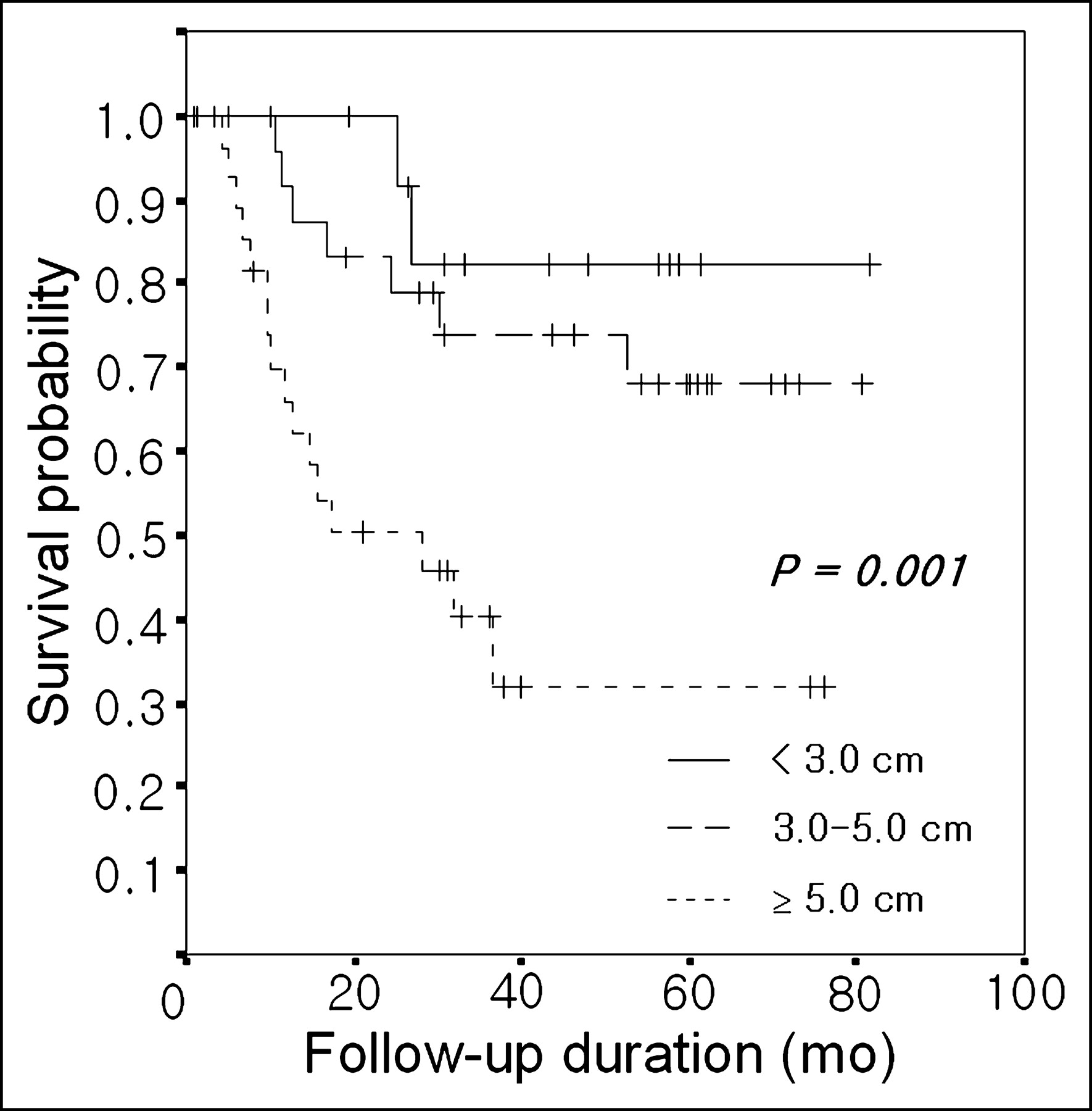
Overall survival curves according to tumor length on PET.
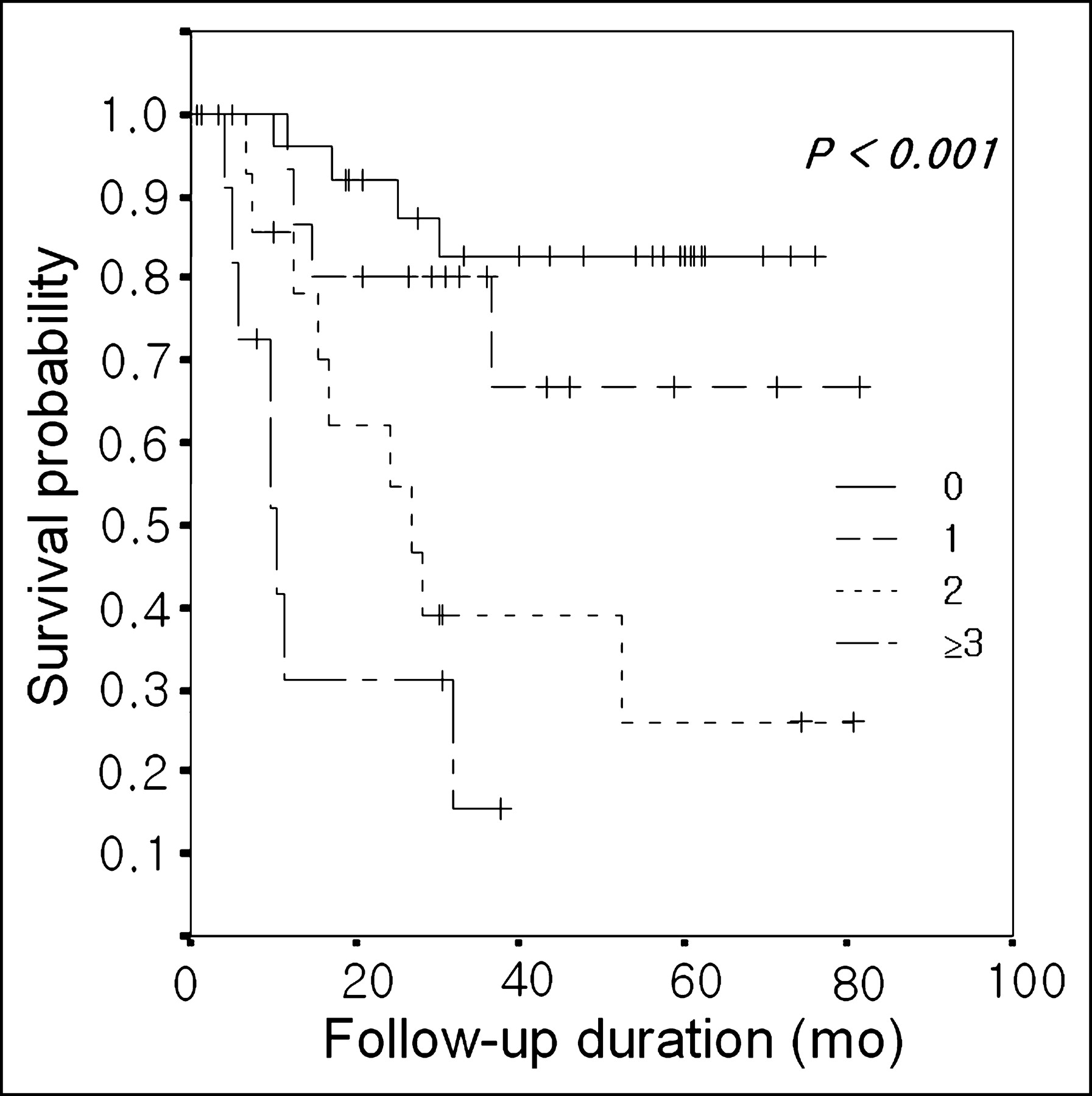
Overall survival curves according to number of PET-positive lymph nodes.
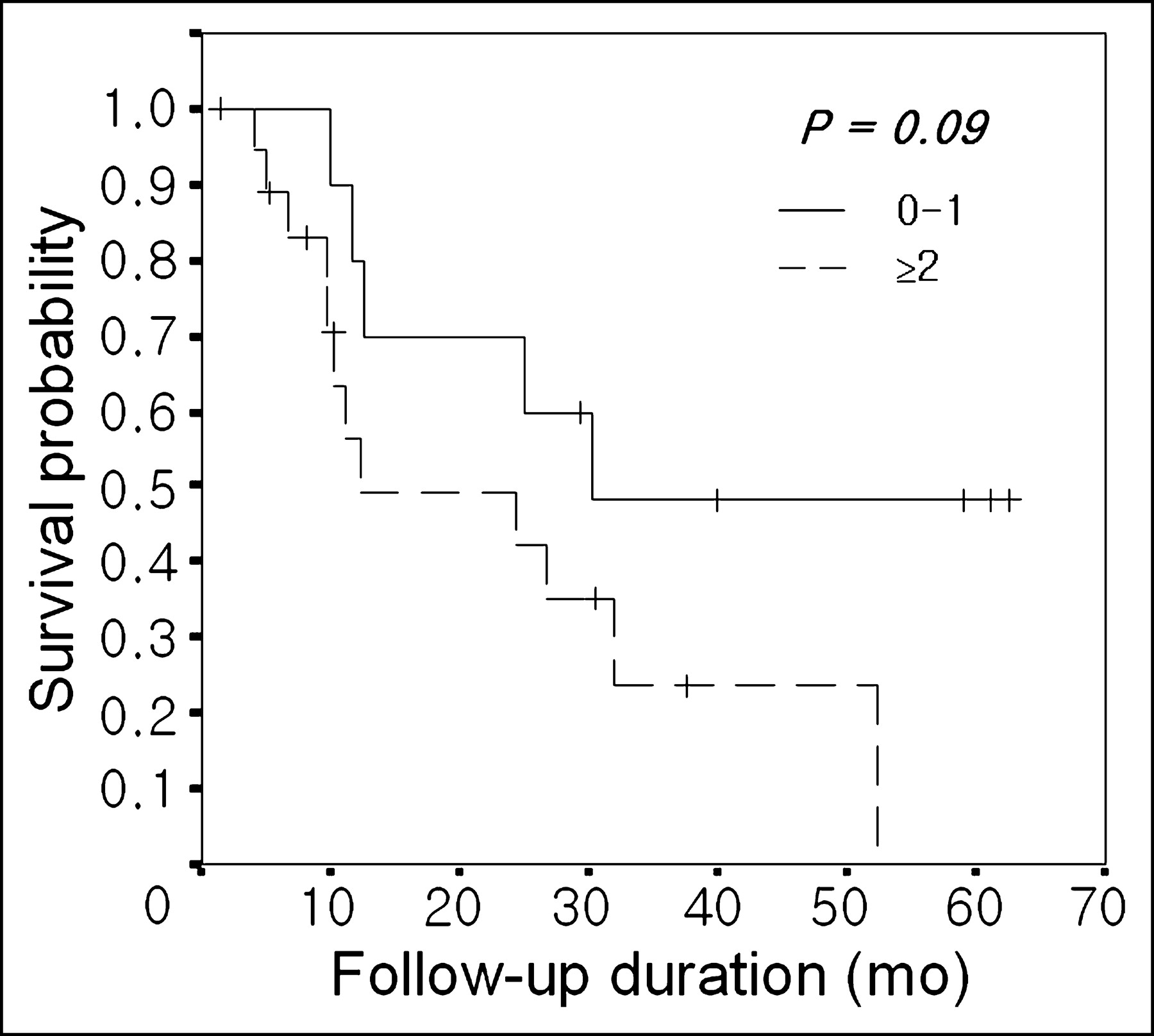
In the subgroup of patients with pathologic stage III disease, overall survival was significantly different according to the number of PET-positive nodes (mean survival: no event [n = 2] vs. 41.4 ± 3.5 mo [n = 4] vs. 31.4 ± 13.0 mo [n = 5] vs. 6.0 ± 0.0 mo [n = 1], P = 0.005; Fig. 4). In the subgroup of patients with pathologic stage IV disease, overall survival appeared to differ according to the number of PET-positive nodes (estimated 5-y survival: 48.0% ± 16.4% [n = 11] vs. 0.0% ± 0.0% [n = 18], P = 0.09; Fig. 5).

Overall survival curves according to number of PET-positive lymph nodes in subgroup of patients with pathologic stage III disease.
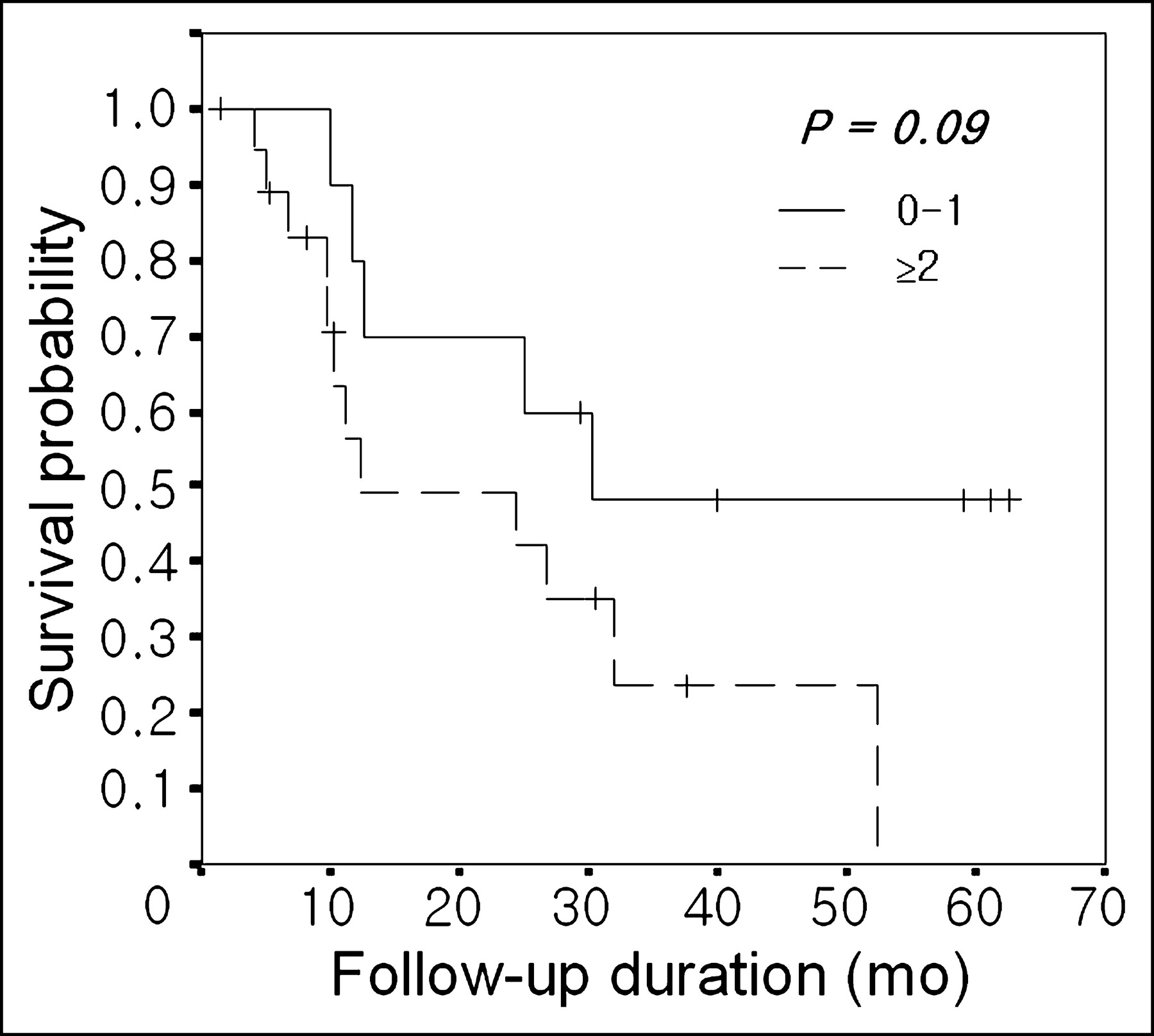
Overall survival curves according to number of PET-positive lymph nodes in subgroup of patients with pathologic stage IV disease.
DISCUSSION
Accurate staging is mandatory in esophageal cancer because it reflects the prognosis, and treatment modalities depend on the stage of disease. The pathologic stage is determined by surgery or thoracoscopic or laparoscopic biopsy, but these procedures require hospitalization, involve high cost, and have a potential procedural risk of mortality and morbidity. Thus, a noninvasive accurate staging method that reflects the prognosis is desirable in esophageal cancer. CT has been widely used for this purpose but is not satisfactory because of its poor sensitivity for detecting nodal metastasis (3–8). 18F-FDG PET has been reported to show better accuracy in detecting lymph node and distant metastasis than CT or EUS in esophageal cancer (3–8). In this study, our results confirm that this improved accuracy for staging by PET leads to better prediction of prognosis in esophageal cancer over other clinical factors. The tumor length measured on the PET image and the number of positive lymph nodes on PET were independent prognostic factors in esophageal cancer. Especially, the number of PET-positive lymph nodes was the single prognostic factor predicting both disease-free and overall survival.
Many studies reported that the number of pathologically positive lymph nodes was an independent prognostic factor in esophageal cancer, although the cutoff points for the node number in grouping subjects was different between the studies (10–14). In this study, patients were divided into 4 subgroups to compare survival according to the number of PET-positive nodes (0, 1, 2, and ≥3), which reflected the patients’ best prognosis. In other studies, the cutoff points of the node number in grouping subjects were somewhat higher than the cutoff points in our study. For example, Korst et al. used a cutoff of 4 pathologic positive nodes (13), and Eloubeidi et al. used a cutoff of 5 (17). This difference may be explained by the sensitivity of 18F-FDG PET in detecting nodal metastasis. Though superior to CT, 18F-FDG PET showed only a moderate sensitivity of 40%–60% for detecting individual metastatic lymph nodes in comparison with pathologic findings (4,5). However, false-negative results for detecting metastatic nodes may have some prognostic implication in this study. In the subgroup of patients with pathologic stage III disease, which means that all subjects had pathologically confirmed nodal metastasis, overall survival was significantly different according to the number of PET-positive nodes (Fig. 4). Furthermore, no events occurred in the subgroup of patients without nodal metastasis on 18F-FDG PET during follow-up. This finding suggests that microscopic nodal metastasis not detected by PET meant a more favorable outcome than gross nodal metastasis detected by PET.
The number of CT-positive nodes was a significant prognostic factor for disease-free and overall survival on univariate analysis, but not an independent predictor after multivariate analysis. This might result from the poor sensitivity of CT for detecting nodal metastasis in esophageal cancer. Natsugoe et al. reported that the number of EUS-positive nodes was a significant prognostic factor for overall survival in esophageal cancer (9). However, they did not show whether it was an independent prognostic factor over alleged predictors. In our series, the probe of EUS failed to pass through the whole esophagus due to severe stenosis induced by the primary tumor in 19 of 69 patients (28%), which was similar to the results of previous studies (22,23). Complete nodal evaluation and exact measurement of tumor length was impossible in those patients. Accordingly, we couldn’t compare 18F-FDG PET with EUS directly for prognosis evaluation. The relative high failure rate to complete EUS examinations may be a serious drawback for initial staging and prognosis evaluation in esophageal cancer. Therefore, 18F-FDG PET may be a single noninvasive diagnostic modality that can provide independent prognostic information in esophageal cancer.
The tumor length measured on the PET image was an independent prognostic factor for overall survival, as several previous studies reported (14–17). Cutoff points of 3 and 5 cm in this study were also used in previous studies (14–17). The maximum SUV of the primary tumor was a significant prognostic factor for overall survival on univariate analysis, but not an independent predictor on multivariate analysis. This suggested that the degree of metabolic change was not associated with the patients’ survival. Flamen et al. reported that the extent of lymph node involvement (N0 M0, N1 M0, M+ly [distant nodal metastasis without organ metastasis]) on prechemoradiation therapy (CRT) PET predicted the pathologic response to CRT and the patients’ survival after CRT and surgery in esophageal cancer (24). But, they did not include the tumor length on PET and the number of positive nodes on PET as variables for analysis. In this study, PET stage (N0 M0, N1 M0, M1) was a significant prognostic factor for disease-free and overall survival after surgery in univariate analysis. However, it was not an independent predictor for survival in multivariate analysis. This supports the suggestion that the number of positive nodes is more important than the location of positive nodes on 18F-FDG PET for the patients’ survival.
The clinical stage using conventional imaging methods was an independent prognostic factor for overall survival in this study. However, there were no significant differences in survival between stage II and stage IV patients (Table 1), and the hazard ratio of the clinical stage was <1 (Table 2). This suggested that the clinical stage using conventional imaging methods was not helpful to evaluate and manage esophageal cancer patients.
Our results showed that only 18F-FDG PET could provide prognostic information in esophageal squamous cell carcinoma over other clinical variables. This may be helpful to determine a treatment plan in patients with esophageal cancer. For example, when there were multiple nodal metastases or an esophageal mass involving long segments on 18F-FDG PET, alternative treatment other than surgery alone might be considered. On the contrary, a single nonregional nodal metastasis on 18F-FDG PET may deserve curative surgery. However, this does not mean that the pathologic stage is obsolete. Multivariate analysis revealed that the pathologic stage was not only an independent prognostic factor but also had the highest hazard ratio. Considering that the accurate pathologic stage was acquired by only extended lymph node dissection, we believe 18F-FDG PET may be more practical to determine a treatment plan and predict prognosis of the individual patient in the initial staging.
The current staging system for esophageal carcinoma by the American Joint Committee on Cancer classifies positive lymph nodes as either regional or metastatic disease (stage IV), according to the location of the lymph node and the location of the primary tumor, and does not consider the length of the primary tumor (1). However, the adequacy of the current staging system has been questioned for several reasons (10–17). First, considering lymph node involvement outside regional nodes as M1 disease, it classifies such tumors as stage IV and categorically unresectable. However, as our results showed, the subgroup of patients with pathologic stage IV disease with 0 or 1 positive node on 18F-FDG PET had a relatively favorable outcome of about 50% 5-y overall survival rate after curative surgery. Second, it does not stratify disease according to the number of metastatic lymph nodes, a factor thought to be important for predicting the survival of patients undergoing resection for esophageal carcinoma. Our results also support the independent prognostic significance of the number of metastatic lymph nodes. Third, it does not consider the length of the primary tumor as a prognostic factor. As in previous studies, our study showed that the length of primary tumor was an independent prognostic factor in esophageal cancer. Recently, Eloubeidi et al. proposed a new TNM classification system for esophageal carcinoma considering the tumor length and the number of positive nodes (17). Our results also support this new staging system. If the staging system were to be revised with considerations of the number of malignant nodes and the length of primary tumor, 18F-FDG PET might become more useful for the noninvasive staging of esophageal cancer, due to its good results for predicting prognosis.
This study has several limitations. The small number of enrolled patients is a major limitation of this study, especially for multivariate analysis. As well, other predictors might be considered independent variables in a larger study population. In addition, due to a limited number of subjects, we were unable to analyze the survival data by dividing stage II into stage IIA and stage IIB, which were proven to have a difference in prognosis. Another potential limitation of this study is that not all subjects underwent neck lymph node dissection. Cervical and supraclavicular node dissection was performed in only 20% of the subjects, most of whom had a primary tumor located in the cervical or upper esophagus. The remaining patients did not undergo neck dissection at surgery, although none had clinical or imaging findings suggesting cervical node involvement. Since the lymphatic spread of esophageal cancer can occur along the whole length of the esophagus, regardless of the primary tumor site, we cannot exclude the possibility of microscopic metastasis in these nodes that was undetected with the imaging studies and may have influenced the prognosis of patients. Finally, there were few subjects with adenocarcinoma of the esophagus in this study. Two patients had adenocarcinoma but were excluded from further analysis because of their refusal of surgery. A very low prevalence of esophageal adenocarcinoma is a typical finding of esophageal cancer in East Asian countries, including Korea. Currently, there was no definite evidence of differences in prognosis between squamous cell carcinoma and adenocarcinoma of esophagus (1,16). Thus, this may not affect our results significantly.
CONCLUSION
The number of 18F-FDG PET-positive lymph nodes and the tumor length on PET are independent prognostic predictors, along with pathologic stage, in patients with esophageal cancer who are undergoing curative surgery. A revised TNM classification system for esophageal carcinoma may consider the tumor length and the number of positive lymph nodes as important prognostic factors. Alternative treatment other than surgery alone may be considered in patients with esophageal cancer who have multiple lymph node metastases or a primary mass involving long segments on 18F-FDG PET before treatment due to poor prognosis.
Acknowledgments
This study was supported by a grant of the Korea Health 21 R&D Project, Ministry of Health and Welfare, Republic of Korea (02-PJ3-PG6-EV06-0002).
Footnotes
Received May 2, 2004; revision accepted Jul. 14, 2004.
For correspondence or reprints contact: Byung-Tae Kim, MD, Department of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 50 Ilwon-dong, Kangnam-ku, Seoul 135-710, Korea.
E-mail: btkim{at}smc.samsung.co.kr





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}