


Abstract
PET with 18F-FDG has shown its potential in cervical cancer. For maximizing the benefits of this new imaging technology, we aimed to define the prognostic features of recurrent cervical cancer patients for selecting appropriate candidates using 18F-FDG PET. Methods: Patients enrolled were from 2 independent prospective studies investigating the role of 18F-FDG PET in cervical cancer patients after definitive treatment with documented failure (CTRP-018) or unexplained elevated tumor marker serum levels (CTRP-016) and proven relapse after PET. A total of 55 eligible patients received PET and CT or MRI. Lesion status was determined from pathologic results or clinical follow-up. The benefits calculated were based on treatment that was modified because of the PET findings. The Cox proportional hazards ratio (HR) was used to select independent prognostic covariates. Results: Thirty-six (65.5%) patients had treatment that was modified due to PET. Primary radiation (HR = 14.62; 95% confidence interval [CI] = 2.74–77.92), squamous cell carcinoma antigen (SCC-Ag) ≥ 4 ng/mL (HR = 5.82; 95% CI = 1.53–22.04), and presence of symptoms (HR = 6.24; 95% CI = 1.99–19.61) at recurrence were significant factors associated with poor survival. A scoring system using these covariates defined 3 distinct prognostic groups: score ≤ 1 (HR = 1.00); score = 2 (HR = 6.91; 95% CI = 1.49–32.14); and score = 3 (HR = 60.46; 95% CI = 9.68–378.09) (P < 0.0001). Conclusion: Using this risk score, 18F-FDG PET may offer maximal benefits by selecting appropriate recurrent cervical cancer patients for salvage therapy with precise restaging information.
Cytologic screening for cervical cancer has been available for >50 y (1,2). The effectiveness of cytology-based screening programs has decreased the incidence and mortality of invasive cervical cancer in many developed countries but not in developing countries because <5% of women in the developing world have ever been screened. Therefore, cervical cancer remains one of the leading causes of cancer-related death among women globally (3,4). The cure rate of cervical cancer is quite high if detected early, but approximately 30% of International Federation of Gynecology and Obstetrics (FIGO) stage IB2 to stage IV disease will ultimately recur with modern multimodality treatment (5,6). Once the primary treatment has failed, the opportunity of secondary cure is slim. Morbidity of salvage therapy is usually high and 5-y survival rates after recurrence are low (6–10). Early detection of recurrence may impact survival. Moreover, detection of asymptomatic recurrences is associated with prolonged overall survival and survival from the time of initial detection of recurrence (11). Therefore, attempts to improve surveillance after treatment might lead to earlier detection of relapse, and precise assessment of recurrent status could improve outcome. Serum tumor markers, such as squamous cell carcinoma antigen (SCC-Ag) and carcinoembryonic antigen (CEA), can accurately reflect the active tumor status of patients with cervical cancer. By far, the most important role for SCC-Ag and CEA in the management of cervical cancer is its potential for monitoring the course of disease and response to treatment, though some controversial results in improving the management of recurrent cervical cancer have been found (12–17).
18F-FDG PET is rapidly expanding worldwide. The clinical application of 18F-FDG PET in cervical cancer has shown great potential and demonstrates the prognostic value related to the presence and the level of 18F-FDG uptake (18–22). However, because of its high cost and limited availability, it is premature to consider PET as a routine clinical practice. The magnitude of impacts on clinical outcome with PET will be determined by the sensitivity of detecting subclinical cancer cell aggregates and whether treatment of such lesions is feasible. For maximizing the benefits of this new imaging technology, we aimed to define the prognostic features of recurrent cervical cancer patients for selecting appropriate candidates for use of 18F-FDG PET. In this study, patients enrolled were from 2 independent prospective studies investigating the role of 18F-FDG PET in cervical cancer patients after definitive treatment with documented failure or unexplained elevated tumor marker serum levels and proven relapse after PET. The benefits calculated were based on treatment that was modified as a result of the PET findings. The Cox proportional hazard ratio (HR) was used to select independent prognostic covariates. A scoring system using these covariates might then define the priority groups for using PET in recurrent cervical cancer.
METHODS AND MATERIALS
Patients
Patients enrolled were from 2 independent prospective studies investigating the role of 18F-FDG PET in cervical cancer patients with documented failure after definitive treatment (CTRP-018) or unexplained elevated tumor marker squamous cell carcinoma antigen (SCC-Ag) or carcinoembryonic antigen (CEA) serum levels (CTRP-016) and proven relapse after PET. These 2 trials were approved by our institutional review board. Informed written consent was obtained from each patient before entry in the CTRP-016 or CTRP-018 study. The common eligibility criteria were (a) completion of definitive radiotherapy (RT) or surgery; (b) without contraindications to and willing to undergo contrast-enhanced CT/MRI and PET scans; (c) willing to receive an image-guided biopsy or surgical exploration if indicated; and (d) potentially curable and willing to receive curative salvage therapy if restaging confirmed the feasibility. Biopsy-documented recurrent or persistent cervical carcinoma was required to enter the CTRP-018 study. For the CTRP-016 study, an additional criterion was either a serum level of SCC-Ag > 2 ng/mL or CEA > 10 ng/mL on 2 successive tests 1 mo apart, but no definite recurrence was identified by conventional imaging studies (including CT/MRI). Patients in the CTRP-016 study were enrolled after proven relapse. Though elevated serum CEA was removed from the inclusion criteria in the amendment of the CTRP-016 project to homogenize the patient characteristics of that trial, we did not exclude those subjects in this analysis.
The common ineligibility criteria were if (a) the patient had received salvage therapy for previous recurrence, (b) the patient was medically or psychologically unfit to receive curative salvage therapy, and (c) the patient had a history of another malignancy excluding basal cell carcinoma of the skin. For CTRP-018, additional exclusion criteria were (a) only a superficial lesion on the cervix or vaginal cuff, (b) disseminated abdominal or pleural lesions with positive fluid cytology, (c) >2 regions involved or a previously irradiated recurrent or persistent pelvic tumor with extrapelvic metastasis.
“Potentially curable” were defined as (a) the proven recurrent disease was confined to the pelvis without previous primary or adjuvant RT; (b) if RT had been given before relapse, the relapse should be limited to the central pelvis without pelvic side wall or extrapelvic involvement; (c) distant recurrences at a sole site that could be completely resected or encompassed by a curative RT procedure, such as paraaortic, supraclavicular, or inguinal lymph nodes (LNs); or pulmonary metastasis without spread to mediastinal LNs, solitary or multiple (≤4 nodules) but confined to 1 lobe (7,23). Every effort was made to differentiate recurrent cervical cancer from new primary malignancy.
CT and MRI
All CT and MR images were obtained with a spiral CT scanner (Hi-Speed; General Electric Medical Systems) or a multislice CT scanner (Somatom Plus 4, Volume Zoom, Version A40; Siemens AG Medical) and a 1.5-T scanner (either a Magnetom Vision or Magnetom Expert; Siemens Medical Systems) with the method described in our previous study (21).
PET
The FDG used in the PET scans was produced by the Institute of Nuclear Energy Research of Taiwan and the images were obtained with an ECAT EXACT HR+ PET camera (CTI), using a full width at half maximum of 4.5 mm and 15-cm transaxial field of view. The preparation of each patient and data acquisition were according to our previous study (21). Transmission scans were obtained with 68Ge rod sources. Reconstruction of both transmission and emission scans used accelerated maximum-likelihood reconstruction and ordered-subset expectation maximization, which reduce image noise and avoid reconstruction artifacts, resulting from filtered backprojection reconstruction of data with low count densities.
Image Analysis
Three experienced nuclear physicians interpreted the PET data with consensus between at least 2. Any foci of abnormally increased 18F-FDG uptake were evaluated using transaxial, sagittal, and coronal displays and compared between early and delayed scans. 18F-FDG accumulation was classified on the basis of visual scores using 5 grades: 0 = normal, 1 = probably normal, 2 = equivocal, 3 = probably abnormal, and 4 = definitely abnormal. The official PET report was primarily interpreted on the basis of visual analysis. The standardized uptake value was used as an additional criterion (21). Images of CT/MRI scans were analyzed by an experienced radiologist 3 times with consensus at least twice. The 5-grade scoring criteria were also used for interpretation of the CT/MR image results: grade 0, a completely normal finding; grade 1, visible nodes with size < 0.5 cm and considered as reactive; grade 2, any single visible node was between 0.5 and 1 cm in length and considered as equivocal for malignancy; grade 3, any LNs > 1 cm in its short axis or clustered nodes (n ≥ 3) with sizes between 0.5 and 1 cm; and grade 4, confluent nodes with central necrosis or an irregular contour (21). Image readings were designated positive with grades 3 and 4, and negative with grades 0, 1, and 2. Disease status was determined from pathologic findings or clinical follow-up.
Study Procedures and Determination of Lesion Status
Abdominal and pelvic CT/MRI were performed on all patients before enrollment. PET and CT/MRI were performed within a period of 2 wk. For CTRP-016, a neck and chest CT scan was done in those patients with suspected lung metastases or supraclavicular node metastases clinically or after PET. For CTRP-018, all patients had neck and chest CT scans. Image fusion of CT/MRI and PET with a commercially available software program (Hermes; Nuclear Diagnostics AB) was applied in an abnormally elevated region of 18F-FDG uptake or discrepant results (24). We examined the suspicious (grade ≥ 3) lesions by a CT- or ultrasound-guided biopsy to confirm lesions demonstrated by coregistered images, if feasible. If a distal site LN metastasis was confirmed histologically, we considered all proximal adenopathy with abnormal uptake (grade ≥ 3) as positive based on the fact that LN metastasis usually follows in a sequential fashion. A biopsy was attempted whenever discrepant findings existed between the CT/MRI and PET scans. If biopsy of the lesion of interest was not feasible, or yielded a negative result, follow-up with CT/MRI or PET was performed 3–6 mo later to assess the interval status of the lesion and to avoid a false-negative (FN) biopsy result.
Statistical Analysis
We prospectively recorded the following data: birth date, date of initial diagnosis and recurrence, initial FIGO staging, initial tumor grade, initial tumor-node-metastasis status, number and type of prior treatment(s) (surgery, radiation, and chemotherapy), serum tumor marker levels (SCC-Ag and CEA), patient’s symptoms and signs at the time of enrollment, results of all biopsies performed, the presence of concurrent infection or inflammation at the time of the PET scan, the official CT/MRI and PET reports, the highest standardized uptake values (SUVs) reported from PET scans for each positive site (local, regional, or distant), evidence (histologic, radiographic, or clinical) of recurrent disease after salvage therapy, site and date of recurrent disease (local, regional, or distant), date of recurrence, subsequent treatment (palliative or curative, modality and field of RT) after recurrence, and status (alive or dead, relapsed or relapse-free) at last follow-up.
Sensitivity, specificity, and accuracy were calculated for PET and CT/MRI results. The area under the receiver-operating characteristic (ROC) curve was calculated for evaluating diagnostic efficacy. The area under the curve (AUC) comparison between PET and CT/MRI was made using the method of Metz (25). Kaplan–Meier estimates and log-rank tests were used to examine how overall survival (OS) varied with prognostic variables at initial diagnosis and recurrence by univariate analysis (26). A Cox proportional hazards model with forward selection was made to identify independent risk factors and to estimate the adjusted hazard ratio (HR) of death (26). A scoring system using these significant covariates was formulated to define distinct prognostic groups. All P values were 2-sided and the significance level was 0.05.
RESULTS
Initial and Recurrent Characteristics
Between February 1, 2001, and January 31, 2003, 55 patients were eligible. Forty patients from CTRP-018 were deemed eligible. Twenty-seven patients from CTRP-016 were assessed, in which 15 had documented relapse after PET and were enrolled for this study. Of these 15 enrolled CTRP-016 patients, 12 had unexplained serum elevation of SCC-Ag and 3 had elevated CEA. The other 12 CTRP-016 patients were excluded due to lack of evidence of lesion presence after tissue studies, image examination, and clinical follow-up. The median age at first recurrence in these 55 patients was 51 y (range, 25–86 y). They were monitored to July 31, 2003. The median follow-up from recurrence was 16 mo (range, 8–28 mo). The interval between the initial diagnosis of cervical cancer and the first documented recurrence was 4–276 mo (mean ± SD, 33 ± 50 mo). Their initial FIGO stages were IB or IIA in 26 patients and IIB to IVA in 29 patients. Twenty had primary radical surgery and 35 received primary RT. Histologic examination revealed squamous cell carcinoma in 44 patients and adenocarcinoma or adenosquamous carcinoma in 11 patients.
Diagnostic Efficacy of PET
Ten sites, including peritoneum, bone, liver/spleen, lung, mediastinal LN, supraclavicular LN, paraaortic LN, pelvic LN, inguinal LN, and central or parametrial persistent or recurrent tumors were evaluated for each patient. Therefore, a total of 550 regions of interest (ROIs) from PET and CT/MRI were studied in the 55 patients (Figs. 1 and 2). Either PET or CT/MRI recognized 104 ROIs as positive (grade ≥ 3), and their final diagnoses were 89 malignant and 15 benign. Of the 550 ROIs, 441 were considered as true-negative (TN). Of these 441 TN ROIs, 9 were proven by biopsy, whereas the remaining 432 ROIs were considered to be TN without biopsy because both PET and CT/MRI scans were negative and the patients remained free of disease for at least 6 mo after clinical and imaging follow-up. Five FN results (proven by positive CT-guided biopsy or clinical imaging follow-up) were found in both CT/MRI and PET. Table 1 shows comparisons of the 550 ROIs of 18F-FDG PET scans and MRI/CT in all patients studied. In all, sensitivity (TP = true-positive) was significantly higher with PET than with CT/MRI for metastatic lesion detection (89.2% vs. 39.2%; P < 0.0001), but there was no significance for local lesion detection (90.0% vs. 80.0%; P = 0.472). The ROC curve indicated that PET was superior to CT/MRI for all lesions (AUC: 0.968 vs. 0.702; P < 0.0001) and metastatic lesions (other than local recurrence or persistent tumor) (AUC: 0.971 vs. 0.684; P < 0.0001), though a marginal effect was observed in local recurrence or persistent tumor (AUC: 0.956 vs. 0.922; P = 0.053).

A 25-y-old woman with poorly differentiated squamous cell carcinoma of uterine cervix, FIGO stage IIIb, underwent concurrent chemoradiation therapy. Three months later, a left neck mass was palpated. Abdominopelvic MRI and chest CT showed no definite abnormal findings except an enlarged supraclavicular LN. Balancing between salvage RT and palliation treatment, PET was performed and suggested nodal metastases at the left supraclavicular, the bilateral upper and lower paraaortic, and the bilateral pelvic regions. After the left supraclavicular and paraaortic nodal metastases were confirmed histopathologically, she received palliation treatment.

A 52-y-old woman with poorly differentiated squamous cell carcinoma of uterine cervix, FIGO stage IIa, underwent concurrent chemoradiation therapy. Four months after complement of treatment, an elevated serum SCC-Ag of 2.23 ng/mL was noted. Abdominopelvic MRI and chest RT showed negative findings. Two months later, her serum SCC-Ag level was 7.36 ng/mL. Conventional images still showed negative findings. A PET scan was then obtained and disclosed a metastatic lesion in the right lower lung. She subsequently received pneumonectomy and was well for 1 y.
Results of 18F-FDG PET (40 Minutes and 3 Hours) and MRI in Recurrent Cervical Cancer Patients (n = 55) and Lesions (n = 550)
Modification of Treatment Due to PET, OS, and Prognostic Factors
Of the 55 study patients who were considered potentially curable for salvage therapy at enrollment, 36 (65.5%) patients had treatment plan modification, and the remaining 19 patients were treated according to the initial plan. Among the 36 patients, 25.0% (n = 9) had treatment remaining curative in intent, yet the modality or field of radiation changed and 75.0% (n = 27) received palliative therapy. Three of the 9 patients (33%) had their treatment modified but still with a curative intent were down staged (CT/MRI grade 3 or 4, with biopsy negative or unfeasible and follow-up disease free).
Up to July 31, 2003, 18 patients had died with disease, 22 were alive with disease, and 15 patients were alive and free of disease. The median survival of the study patients (n = 55) was 19.4 mo. The 6-mo, 1-y, and 2-y OS rates were 92%, 70%, and 29%, respectively. SCC-Ag levels at recurrence were categorized into 2 groups: ≤4 and >4 ng/mL. The serum SCC-Ag cutoff of 4 ng/mL was determined according to the log-rank test with the lowest P value. Univariate analyses showed covariates such as SCC-Ag ≥ 4 ng/mL at recurrence (P = 0.0041) and primary treatment (P = 0.0081) were significantly associated with survival. The presence of symptoms at recurrence (P = 0.0536), pelvic node metastasis before primary treatment (P = 0.0585), and the type of salvage treatment (P = 0.0642) was marginally significant. There has been no death (0/9) among those who remained with a curative intent yet had modified treatment compared with those with a curative intent and no change (6/19); however, the difference was not significant. Other covariates such as initial FIGO stage, histology type, grade of differentiation, or pattern of recurrence did not significantly influence OS by the log-rank test (Table 2). The Cox proportional hazard model using multivariate analysis for forward selection identified SCC-Ag serum levels at recurrence (HR = 5.82; 95% confidence interval [CI] = 1.53–22.04; P = 0.010), primary treatment (HR = 14.62; 95% CI = 2.74–77.92; P = 0.002), and the presence of symptoms (HR = 6.24; 95% CI = 1.99–19.61; P = 0.002) as independent prognostic factors (Table 3).
Clinical Features and Univariate Analyses of Prognostic Covariates in Study Subjects (n = 55)
Multivariate Analyses of OS in Recurrent Cervical Cancer Patients (n = 52)
Prognostic Scoring System
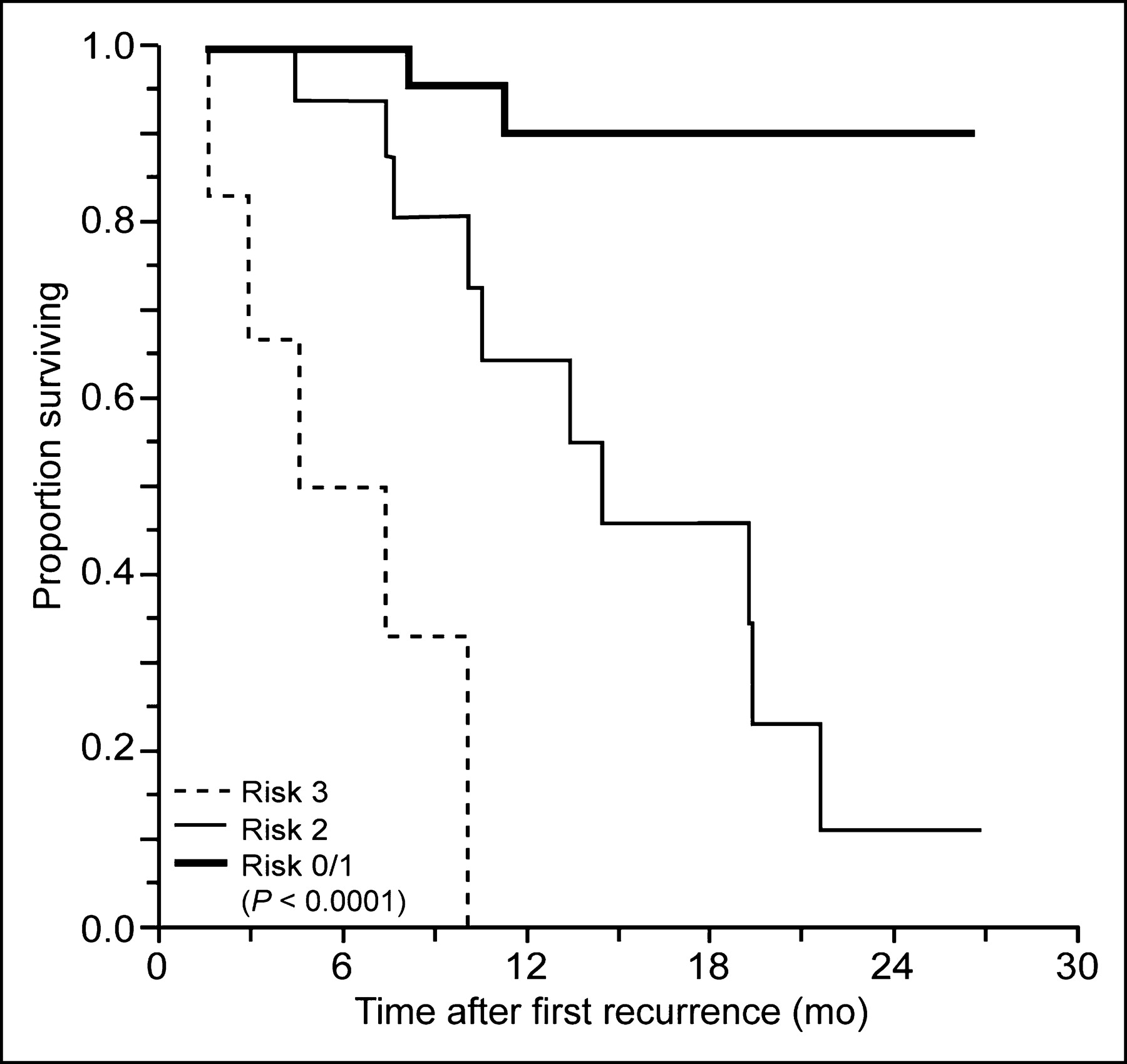
A prognostic scoring system was formulated by summing up the 3 significant covariates: 0 for SCC-Ag of ≤4 ng/mL, 1 for >4 ng/mL; 0 for the absence of symptoms and 1 for the presence of symptoms; 0 for primary treatment with radical surgery and 1 for primary treatment with RT (Table 4). The probability of dying in 2 y was the highest in the group with a score of 3 (high risk) (HR = 60.46; 95% CI = 9.68–378.09); this was followed by the group with a score of 2 (intermediate risk) (HR = 6.91; 95% CI = 1.49–32.14) compared with the group with a score of ≤1 (low risk) (P < 0.0001) (Fig. 3).
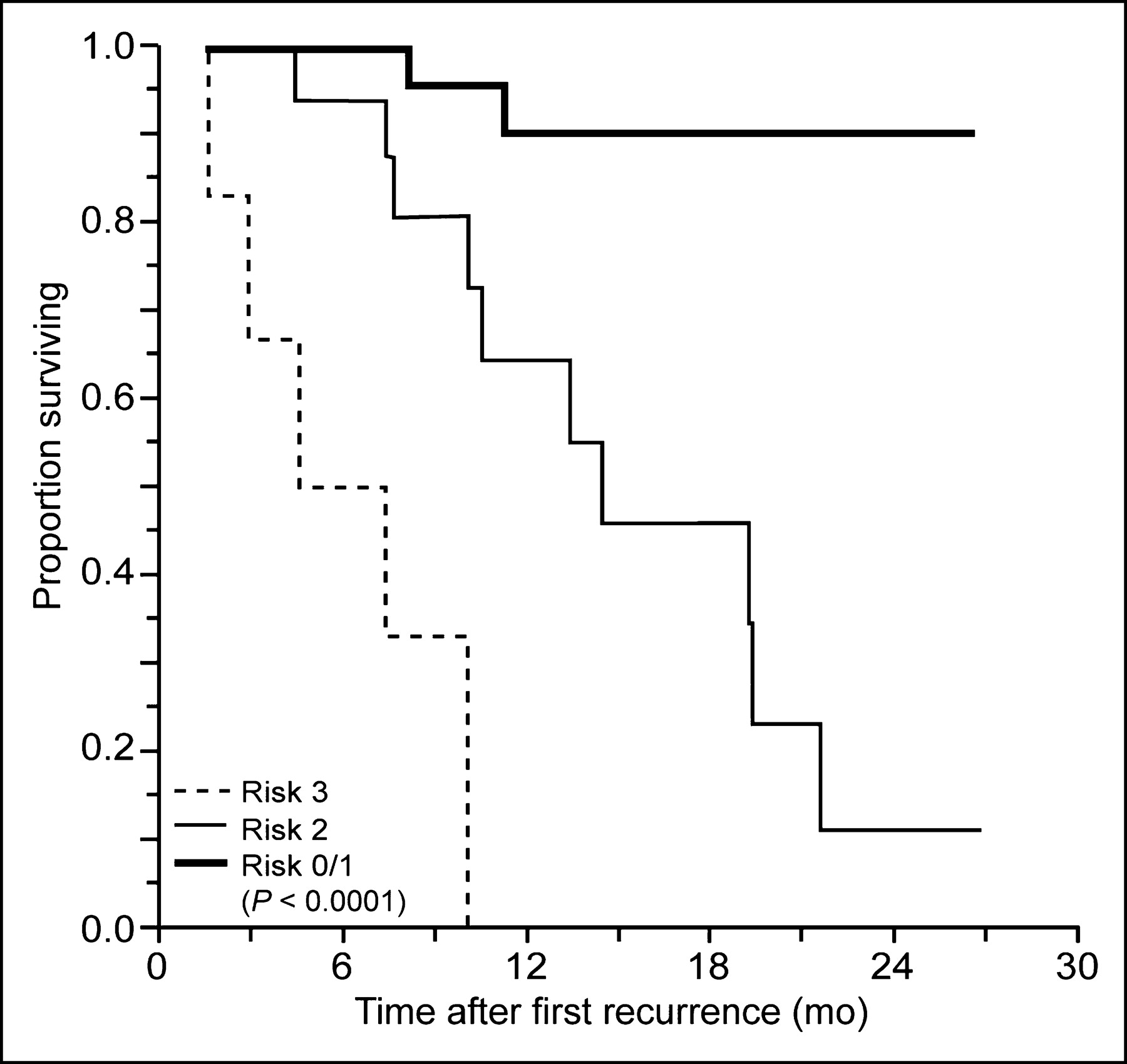
Kaplan–Meier curves for 2-y OS rates in patients with recurrent cervical cancer. Patients are categorized by risk score of ≤1 (bold solid line), 2 (thin solid line), and 3 (dashed line) (P < 0.0001).
HRs and Modification of Salvage Treatment Due to 18F-FDG PET According to Risk Score (n = 52)
In the low-risk group (n = 27), 10 patients were shifted to palliation and the other 17 remained with curative salvage therapy (7 with plan changed, 10 unchanged). Furthermore, in the intermediate-risk group (n = 19), 12 patients were switched to palliative treatment, whereas the other 7 patients stayed on curative treatment (2 with plan changed, 5 unchanged). Each of the 2 patients, who had changed treatment planning but still remained with a curative intent after PET, was alive at the time of analysis. Among the 6 patients in the high-risk group, 5 (83.3%) have changed treatment planning to palliation after PET, and 4 of these 5 (80%) were dead. The remaining 1 patient on curative therapy still died of disease (Table 4).
DISCUSSION
As a sensitive noninvasive approach and 3-dimensional visualization of the radiolabeled target molecules in the human or animal body, PET is well suited for both preclinical and clinical research on cancer biology (27). Owing to the limited health care resources in Taiwan and relatively high cost of PET, it is impractical to apply PET indiscriminately as a routine clinical practice in any kind of cancer. Therefore, a more realistic utilization of this new imaging technology should be determined by well-designed and well-conducted prospective studies targeting specific indications. Cost-effectiveness analysis is important and needs to be addressed in various clinical situations (28,29).
18F-FDG PET is a potentially useful diagnostic, staging, and restaging tool for cervical cancer (18–21,30–33). From our studies and those of others using PET in various indications for cervical cancer, PET has been noted to be sensitive in detecting metastatic lesions but the magnitude of benefit varies (18,20,21,30–33). In addition, dual-phase PET (adding delayed 3-h scans to 40-min scans) is also found to be more sensitive compared with only 40-min scans in the management of cervical cancer (21). In contrast to the developed countries, cervical cancer remained largely uncontrolled in the developing countries. The most important reason is the inability to find adequate financial resources and infrastructure that can provide effective screening programs for adult women. In such conditions, even with the emergence of PET from research into day-to-day practice in developed countries, a decision on the priority of using this high-cost test should be defined. The outcome of metastatic cancer tends to be better for those with the primary site controlled than for those presenting initially with the primary site untreated or uncontrolled (23). Tran et al. found that 8% (n = 14) of 186 patients with a new diagnosis of cervical cancer had supraclavicular LN metastasis (34). The median OS was 7.5 mo. All 14 patients developed metastasis or persistent primary tumor. Anderson et al. found that 2.1% (n = 1,025) of cervical cancer patient had metastases isolated to lung. The median OS for those with pulmonary resection was 26 mo (23). Thus, we conducted this study to summarize, from 2 independent prospective trials, the value of dual-phase PET in recurrent cervical cancer. Through analysis of prognostic variables, we aimed to define the priority of using PET in recurrent cervical cancer patients.
In this study, ROC curves demonstrated that PET was superior to CT/MRI for detecting metastatic lesions (P < 0.0001), with the resulting sensitivity of 85.0% as well as the therapeutic schema altered up to 65.5% (n = 36). Nine patients in this study who had their treatment field or modality changed but still with a curative intent are currently alive. The 2-y OS is better, but insignificant, between those with a modified/curative intent (n = 9) than those with an unchanged/curative intent (n = 19), due to the limitation of the sample size. In our previous study on recurrent cervical carcinoma (n = 177) after primary radical surgery, the median survival of patients with extravaginal relapse after primary radical surgery was only 7.7 mo (7). In this study, those with a superficial lesion on the cervix or vaginal cuff, who tend to have good prognosis and no additional finding after PET, were excluded. Therefore, the prognosis of the enrolled population would be worse than including those with a superficial lesion on the cervix or vaginal cuff. Nonetheless, the median survival of the 55 study patients was 19.4 mo.
In our previous study, survival after recurrence was significantly decreased in patients with pelvic node metastasis at primary surgery or adeno-adenosquamous carcinoma histology (7). Sommers et al. reported a large series of patients (n = 376) with recurrent cervical carcinoma after definitive RT (8). Salvage therapy after failure was surgery, RT, RT plus surgery, or chemotherapy. They noted no significant difference in survival after recurrence by the type of salvage treatment or the initial stage (4). Using the Cox proportional hazard model in multivariate analysis for forward selection, we clearly demonstrated that the serum SCC-Ag level at the time of recurrence (P = 0.010), the mode of previous definitive treatment (P = 0.002), and the presence of symptoms at the time of recurrence (P = 0.002) were independent prognostic factors for patients with recurrent cervical cancer, whereas pelvic node metastasis at primary treatment or the type of salvage therapy was not selected. The HR of 5.82 (95% CI = 1.53–22.04) for the SCC-Ag serum levels (>4 vs. ≤4 ng/mL), 6.24 (95% CI = 1.99–19.61) for the initial treatment mode (RT vs. surgery), and 14.62 (95% CI = 2.74–77.92) for the clinical presentation (symptomatic vs. asymptomatic) also confirmed that these 3 conditions were important independent prognostic factors for recurrent cervical cancer patients. This finding was compatible with our previous study on isolated paraaortic LN recurrence after definitive RT: A significantly better prognosis of the asymptomatic than the symptomatic and SCC[b]-Ag ≤ 4.0 ng/mL than > 4.0 ng/mL was noted (12). Around 70%–80% of recurrent cervical cancer patients had an elevation of the level of serum tumor markers before or at clinical evidence of tumor recurrence; however, the clinical value of SCC-Ag follow-up was in dispute (13–15,17,35,36). Theoretically, patients who had a better outcome may have an earlier detection of relapse than patients who did poorly. A shorter lead time from its elevation to the diagnosis of recurrence for the lower level of tumor markers than the higher level and restaging with PET than without PET could be anticipated.
Results of this study also indicated the influence of the previous treatment mode on prognosis. Data for the outcome of recurrent cervical cancer after primary definitive treatment remain limited (7–12). Besides, the study subjects of those reports were previously treated either with primary radical surgery with or without adjuvant RT (7,9,10) or with definitive RT only (8,12). Little attention has been paid to the impact of primary surgery or RT on the prognosis after relapse.
In this study, we classified the role of 18F-FDG PET into 3 prognostic scores with a decreasing priority in terms of survival. The benefits of PET are not only a reduction of mortality rates but also avoidance of unnecessary salvage attempts (futile suffering and unrewarded medical cost). The prognostic group classification was according to the sum of the 3 significant factors selected by multivariate analysis. Based on the modification of the treatment plan after PET and the overall outcome, we recommend that the priority use of PET in recurrent cervical cancer might be targeting those with a better prognosis (score ≤ 1) to achieve maximal benefits for those countries with limited health care resources and PET availability. For those with a score of 2, PET is valuable in modifying treatment for those with a curative intent treatment (prolong survival) and those on palliation (avoid unnecessary salvage therapy). PET could even be omitted to save costs in the case of a risk score of 3, because 83.3% (5/6) changed treatment to palliation due to PET findings. However, we must be very careful before making this conclusion, because of the limited number of patients (n = 55) enrolled in this study and only 6 patients had a risk score of 3; the impact in the group with a score of 3 needs to be confirmed by further studies. A cost-effectiveness analysis is ongoing by an independent study of our group, which is comparing the outcome and the cost for recurrent cervical cancer patients with (participants in this study) and without PET scans (historic control).
CONCLUSION
18F-FDG PET is useful in the management of recurrent or persistent cervical cancer because it allows more precise restaging than CT/MRI. In this prospective study, a prognostic scoring system taking into account the clinical presentation (symptomatic vs. asymptomatic), the primary treatment (surgery vs. radiation), and the SCC-Ag serum levels (>4 ng/mL vs. ≤4 ng/mL) identified 3 distinct prognostic groups. Using this risk scoring, 18F-FDG PET may offer maximal benefits by selecting appropriate recurrent cervical cancer patients for salvage therapy with precise restaging information. Larger controlled trials and cost-effectiveness analyses are still needed to confirm these preliminary results.
Acknowledgments
This research was supported by grants from the National Science Council-Taiwan (NSC 91-2314-B-182A-163), the Chang Gung Memorial Hospital (CTRP-018), and the Chang Gung Memorial Hospital (CTRP-016).
Footnotes
Received Feb. 12, 2004; revision accepted May 24, 2004.
For correspondence or reprints contact: Chyong-Huey Lai, MD, Department of Obstetrics and Gynecology, Chang Gung Memorial Hospital Linkou Medical Center, 5 Fu-Shin St., Kueishan, Taoyuan 333, Taiwan.
E-mail: sh46erry{at}ms6.hinet.net
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Para-aortic lymph node recurrence after curative radiotherapy for cervical cancer
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- Clarifying the Diagnosis of Clinically Suspected Recurrence of Cervical Cancer: Impact of 18F-FDG PET
- PET in Cervical Cancer -- Implications for `Staging,' Treatment Planning, Assessment of Prognosis, and Prediction of Response
- Expanding Role of Positron Emission Tomography in Cancer of the Uterine Cervix
- Oncologic Imaging in Gynecologic Malignancies
- MR imaging in cervical cancer: seeing is believing: The 2004 Mackenzie Davidson Memorial Lecture
- 18F-FDG PET Imaging in Posttherapy Monitoring of Cervical Cancers: From Diagnosis to Prognosis