


Abstract
131I therapy is a widely accepted treatment for metastatic differentiated thyroid cancer. To investigate the feasibility of 131I therapy for breast cancer, we established breast cancer cells stably expressing Na+/I− symporter (NIS) gene that can be modulated and studied in vitro and in vivo. Methods: We transfected rat NIS genes into a human breast cancer cell line (MCF7) by electroporation. Iodide accumulation was evaluated under various extracellular concentrations of sodium and iodide, and iodide efflux was also assessed. Biodistribution and tumor imaging were studied using tumor-bearing mice. Results: A novel cell line (MCF3B), stably expressing the NIS gene, was established from MCF7. MCF3B took up 44 times more radioiodide in vitro than MCF7 did. Iodide uptake was completely inhibited by 1 mmol/L perchlorate and was dependent on external sodium and iodide concentrations. Iodide efflux from MCF3B cells was slower (half-life [T1/2] > 27 min) than from FRTL5 thyroid cells (T1/2 = 4 min). In the biodistribution study using MCF3B-xenografted mice, high tumor uptake of 125I was shown (16.73%) at 1 h after injection, and tumor-to-normal tissue ratios were also high (4.84–21.28), except in the stomach (0.47). However, the iodide accumulation in the tumor lessened with time, reaching less than 1% at 24 h after injection. Conclusion: Our preliminary data indicate that NIS-based gene therapy may be applied by concentrating a lethal dose of radiation in tumor cells in vivo, but further investigation is necessary to determine a method of maintaining radioiodine in the cells to allow greater therapeutic effects.
Radioiodide therapy using 131I is effective for patients who have metastatic disease from differentiated thyroid cancer (1,2). This therapy is based on uptake of radioactive iodide into cancer cells, as is observed in thyroid cells, to produce the thyroid hormones thyroxine and triiodothyronine, which are essential for the growth, development, and metabolism of most tissues (3).
Recently, the Na+/I− symporter (NIS) gene was cloned by Dai et al. (4), and some reports have described transfection of the NIS gene into several nonthyroidal cells as well as into thyroidal cells to express symporter protein (5–9). If the transfected cells take up and concentrate radioiodide, radiotherapy with 131I may be applicable to NIS-transfected cancer in the manner in which metastatic thyroid cancer is treated clinically. However, the characteristics of the transformed cells in vivo are still unclear, and the feasibility of radioiodine concentrator therapy is unknown.
Breast cancer is a common malignancy among women and often presents as a systemic disease that requires adjuvant therapy with hormones or cytotoxic drugs (10). As the first step of a novel strategy to use radioiodide concentrator gene therapy for metastases of malignant tumors, this preliminary study was designed to characterize transfected breast cancer cells both in vitro and in vivo.
MATERIALS AND METHODS
Cloning of Rat NIS Gene
The rat NIS gene was prepared as previously reported (5). Briefly, polyadenylate-positive RNA was extracted from FRTL5 functional rat thyroid cells cultured in 6H medium containing thyrotropin using a MicroFast Track kit (Invitrogen, Carlsbad, CA). Reverse transcription and polymerase chain reaction were performed using an oligo-(dT) primer and avian myeloblastosis virus reverse transcriptase and using Taq polymerase and the following primers according to the reported sequence (4): forward primer, 5′-PO4-TGCGAC TCTCCCACTGAC CGAGA-3′; reverse primer, 5′-CAACCATCCAGAG AGGAGGCTGC-3′. The polymerase chain reaction product that corresponded to nucleotide 40-2028 of rat NIS was directly subjected to TA cloning using the pCR3-Uni vector (Invitrogen) that contains the cytomegalovirus-promoter and neomycin-resistance gene. The complementary DNA (cDNA) clone obtained was confirmed by digestion with restriction enzymes (HindIII/BamHI/EcoRI/ApaI/NarI/PstI) and transfection into Cos-7 cells and by examination of 125I uptake.
Establishment of Breast Cancer Cell Lines Expressing NIS
Purified plasmid DNA was transfected into human breast cancer (MCF7) cells by electroporation (Bio-Rad, Hercules, CA). Selection was performed with 300 μg/mL Geneticin (true concentration; GIBCO BRL, Grand Island, NY) in RPMI1640 medium (Nissui, Tokyo, Japan) containing 10% fetal calf serum for 3 wk starting the day after transfection. Surviving well-isolated colonies were picked up by the cylinder technique and were subjected to screening for 125I− uptake. The cell line that accumulated the highest level of 125I− among 9 colonies screened was named MCF3B and was selected for further investigation.
Iodide Uptake
MCF3B cells were plated in 24-well plates and cultured with RPMI1640 medium containing 10% fetal calf serum. When the cells reached confluence (approximately 1 × 106 cells), 125I− uptake was examined. Unless otherwise noted, iodide uptake was determined by incubating cells with 500 μL Hank's balanced salt solution (HBSS) containing 0.5% bovine serum albumin and 10 mmol/L 2-[4-(2-hydroxyethyl)-1-piperazinyl]ethanesulfonic acid-NaOH, pH 7.4, with 3.7 kBq carrier-free Na125I and 10 μmol/L NaI, to yield a specific activity of 740 MBq/mmol (20 mCi/mmol) at 37°C for 5–120 min. After incubation, the cells were washed twice on ice as quickly as possible (<15 s) with 2 mL ice-cold HBSS incubation buffer, which does not contain iodide. The cells were detached with 1 mL Dulbecco's calcium- and magnesium-free phosphate-buffered saline (Nissui) containing 0.02% ethylenediaminetetraacetic acid, and the radioactivity was counted by an autowell γ counter. Cells from some wells were trypsinized for cell number counting. Iodide uptake was expressed as pmol/106 cells, unless otherwise noted. The same procedures were applied to FRTL5 cells in 24-well plates cultured in 6H medium (including thyroid-stimulating hormone) with 5% calf serum.
Iodide Efflux
Iodide efflux studies were performed at 37°C as described by Weiss et al. (11) using MCF3B cells cultured in RPMI1640 medium and FRTL5 cells cultured in 6H medium. After incubating the cells with 10 μmol/L NaI and 0.1 μCi Na125I in 500 μL HBSS incubation buffer at 37°C for 60 min, the cells were washed once and added to HBSS incubation buffer with 10 μmol/L nonradioactive NaI kept at 37°C and further incubated. Every 3 min (0–15 min) or 6 min (15–27 min), the buffer was replaced, and the radioactivity in the buffer was counted. After the last medium removal (27 min), the cells were made soluble for counting along with the previously collected medium samples. The total radioactivity present at the initiation of the efflux study (100%) was calculated by adding the counts in the final cells and the summation of the medium counts.
Preparation of Subcutaneous Xenografts in Athymic Nude Mice
The procedure used to establish human breast cancer tumors in athymic nude mice was similar to that described previously by Buchsbaum et al. (12) for B cell lymphoma xenografts. The MCF7 and MCF3B cell lines were cultured at 37°C in a humidified 5% CO2 atmosphere using RPMI1640 supplemented with 10% fetal calf serum (GIBCO BRL) and underwent passage every 2–3 d in RPMI1640 supplemented with 10% fetal calf serum. Cells to be injected into mice were taken from the culture during the log phase of growth. The human fibrosarcoma cell line HT1080 (supplied by Keiski Sasai, Department of Radiology, Kyoto University) was used as a feeder layer for in vivo growth of the breast cancer cell line. HT1080 cells were grown in monolayer culture in RPMI1640 supplemented with 10% fetal calf serum. The mice, placed in a holder made of paper, were exposed to 2 Gy irradiation (MI-201; Shimadzu Corporation, Kyoto, Japan) once a week during a 3-wk period. One day after the final irradiation, the animals were given subcutaneous injections in the left flank of an admixture of 1 × 107 MCF3B cells and 5 × 106 HT1080 fibrosarcoma cells. In the right flank was injected an admixture of 1 × 107 MCF7 cells and 5 × 106 HT1080 fibrosarcoma cells in 0.2 mL RPMI1640 containing 10% fetal calf serum. HT1080 cells were lethally irradiated with 60 Gy before injection. Tumors grew in a high percentage of animals and weighed as much as 200–500 mg within 2 wk after injection.
Analyses of Iodide Uptake in Vivo
Biodistribution studies were performed when the tumors weighed approximately 300 mg. At 1, 3, 6, 12, and 24 h after the intravenous administration of Na125I, the mice were killed and their organs were removed, weighed, and counted for radioactivity. Data were expressed as percentage of injected dose (%ID) per gram of tissue normalized to 20-g mice and also as tumor-to-normal tissue ratios. Plots of MCF3B–tumor activity over time were fitted with a monoexponential decay function. From these, the half-life (T1/2) of 125I− release was calculated.
Tumor Imaging
For the imaging of MCF3B-bearing nude mice, Na131I (11.1 MBq) was administered intravenously through the tail vein. Two hours after the injection of Na131I, the mice were anesthetized by an intraperitoneal injection of sodium pentobarbital, and scintigrams were obtained using a gamma camera (Pho/Gamma LFOV; Searle, Chicago, IL) equipped with a pinhole collimator (13).
The results were statistically analyzed using an unpaired t test for in vivo studies. Differences were considered significant when the probability value was less than 0.05. All animal experiments were performed in accordance with the regulations of the Kyoto University animal care facility.
RESULTS
Time Course of Iodide Uptake
As shown in Figure 1, the iodide uptake reached the half-maximal level within 10 min and reached a plateau at 30 min. The plateaued, steady state seems to reflect a balance of influx and efflux of iodide, as reported for FRTL5 cells. Iodide uptake was completely inhibited by 1 mmol/L ClO4−. In addition, the iodide uptake in MCF7 cells without transfection of the rat NIS gene was at the baseline level and was indistinguishable from that in MCF3B cells with 1 mmol/L ClO4−.

Time course of iodide uptake by MCF3B without perchlorate, MCF3B with 1 mmol/L perchlorate, and MCF7 without perchlorate. All data are expressed as means (pmol/106 cells) of duplicate wells. Iodide uptake by MCF3B was rapid and became maximal within 30 min, whereas uptake by MCF3B with perchlorate and by MCF7 remained low.
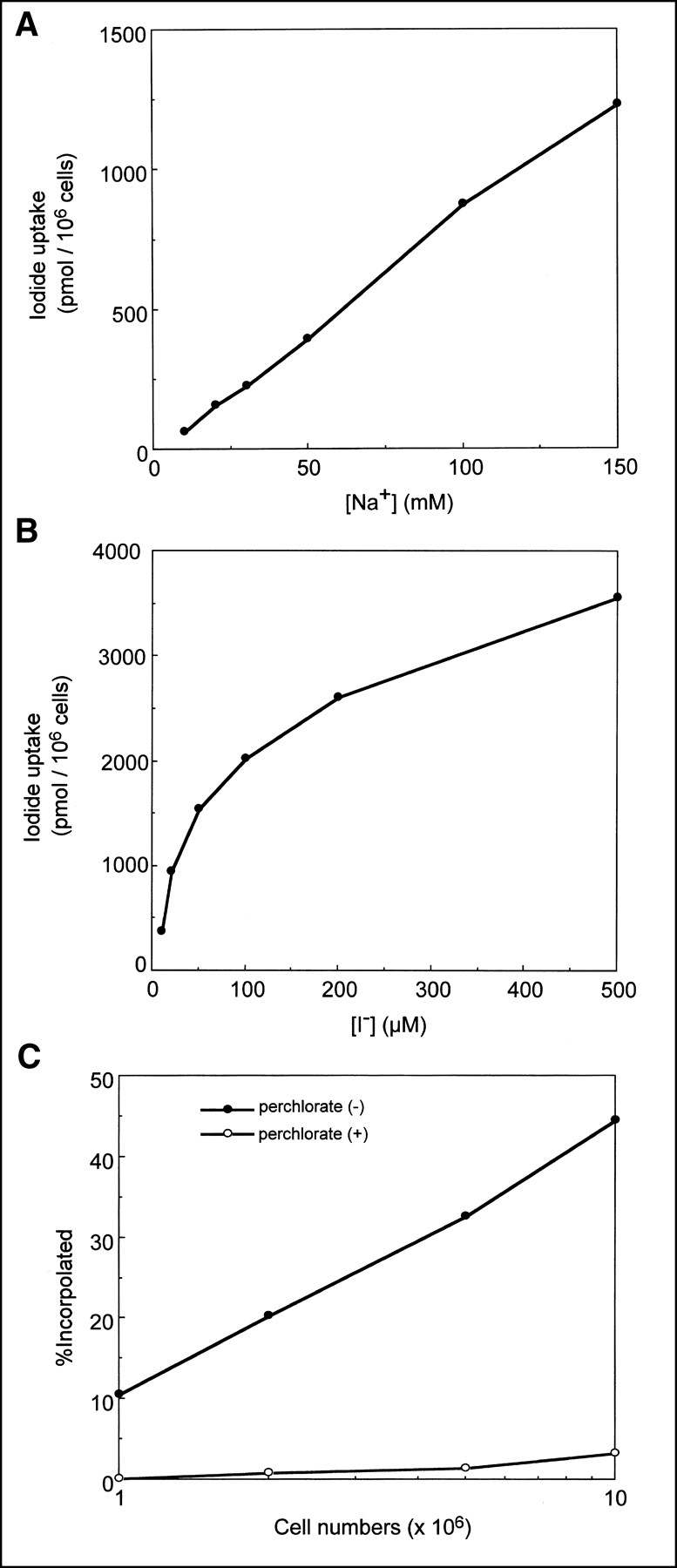
Na+, I−, and Cell Number Dependency of Iodide Uptake
By substituting choline chloride for NaCl in the incubation buffer, we could examine the effect of the Na+ concentration on iodide uptake in MCF3B cells. As shown in Figure 2A, a linear correlation was observed between iodide uptake and extracellular sodium concentration within a range of 10–150 mmol/L, as reported with FRTL5 (11). Also, an increase in iodide uptake was observed with the increase in iodine concentration within a range of 10–500 mmol/L (Fig. 2B). Moreover, iodide uptake was evaluated with increasing cell numbers (1 × 106, 2 × 106, 5 × 106, and 1 × 107) of MCF3B, and a cell number–dependent accumulation of iodide was observed (Fig. 2C).
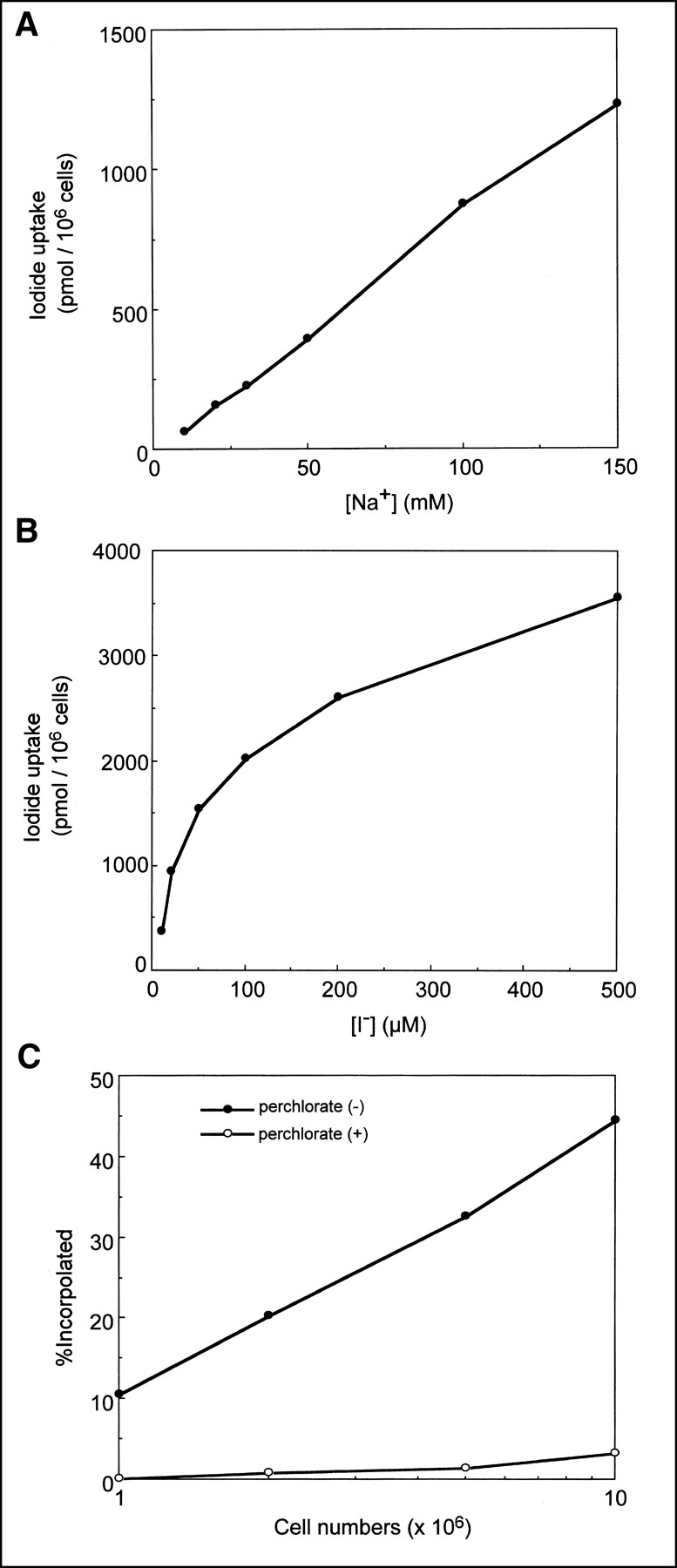
Iodide uptake plotted against Na+ concentration (A), I− concentration (B), and cell numbers (C).
Iodide Efflux
Iodide efflux was studied for both MCF3B cells and FRTL5 cells (Fig. 3). As previously reported (11), the radioiodide that had accumulated in FRTL5 cells was rapidly excreted, with a T1/2 of 4 min. MCF3B cells also showed an efflux of accumulated iodide, but the speed of efflux was slower (T1/2 > 27 min) than for FRTL5 cells.
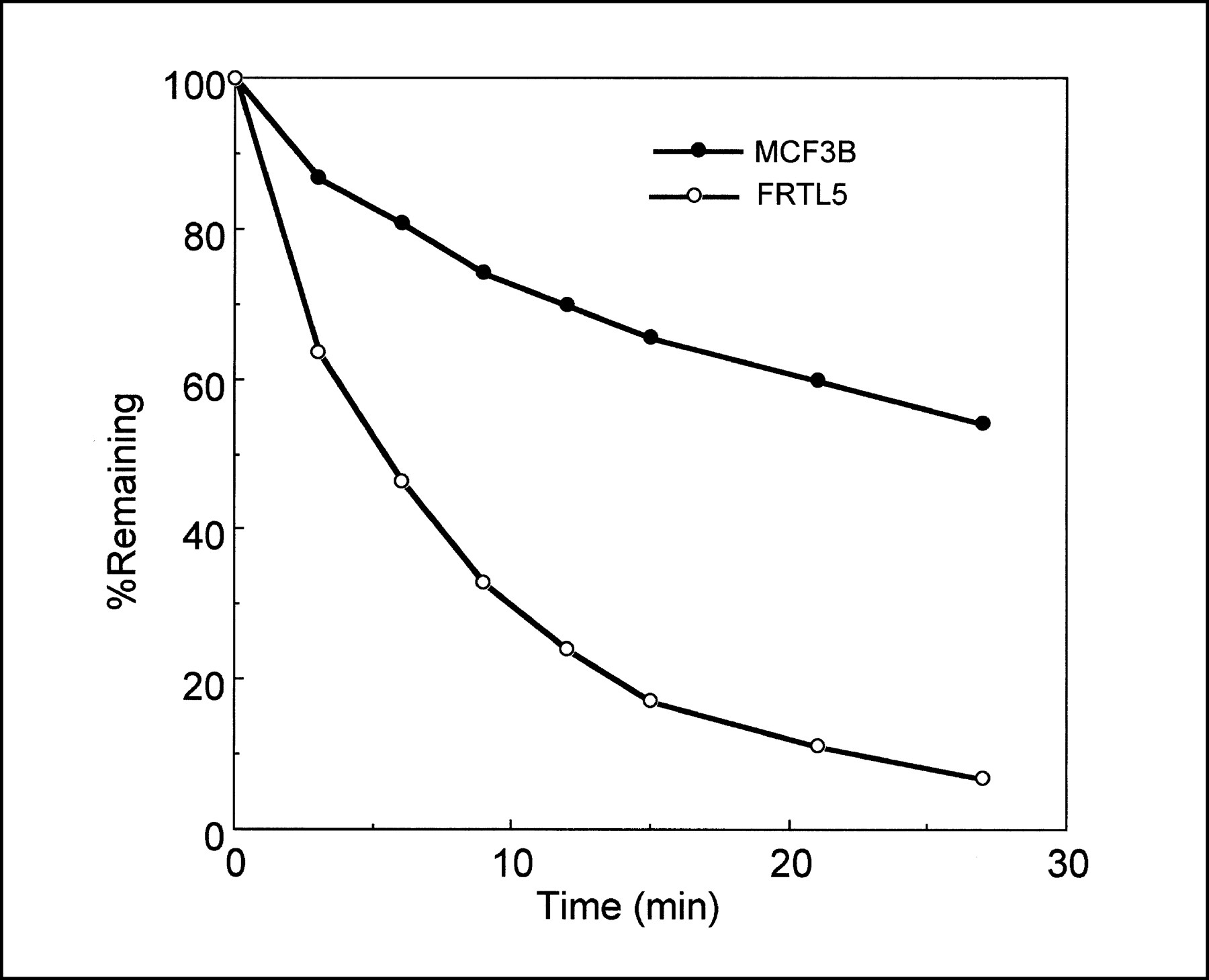
Iodide efflux from MCF3B and FRTL5 cells. All data are expressed as means (remaining percentage of 125I−) of duplicate wells. Although iodide that accumulated in FRTL5 cells was rapidly exchangeable, MCF3B cells released 125I− more slowly.
Biodistribution Study
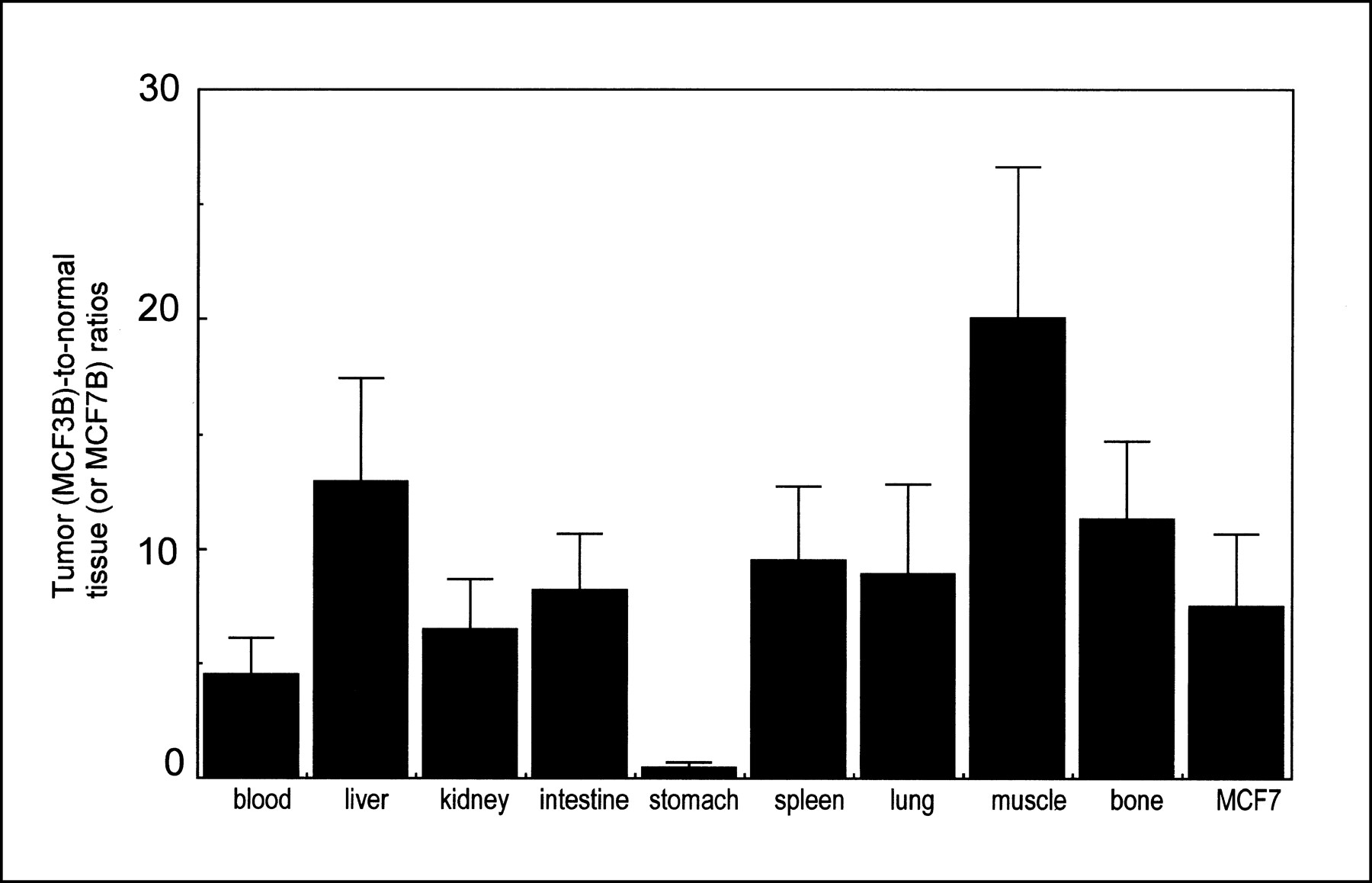
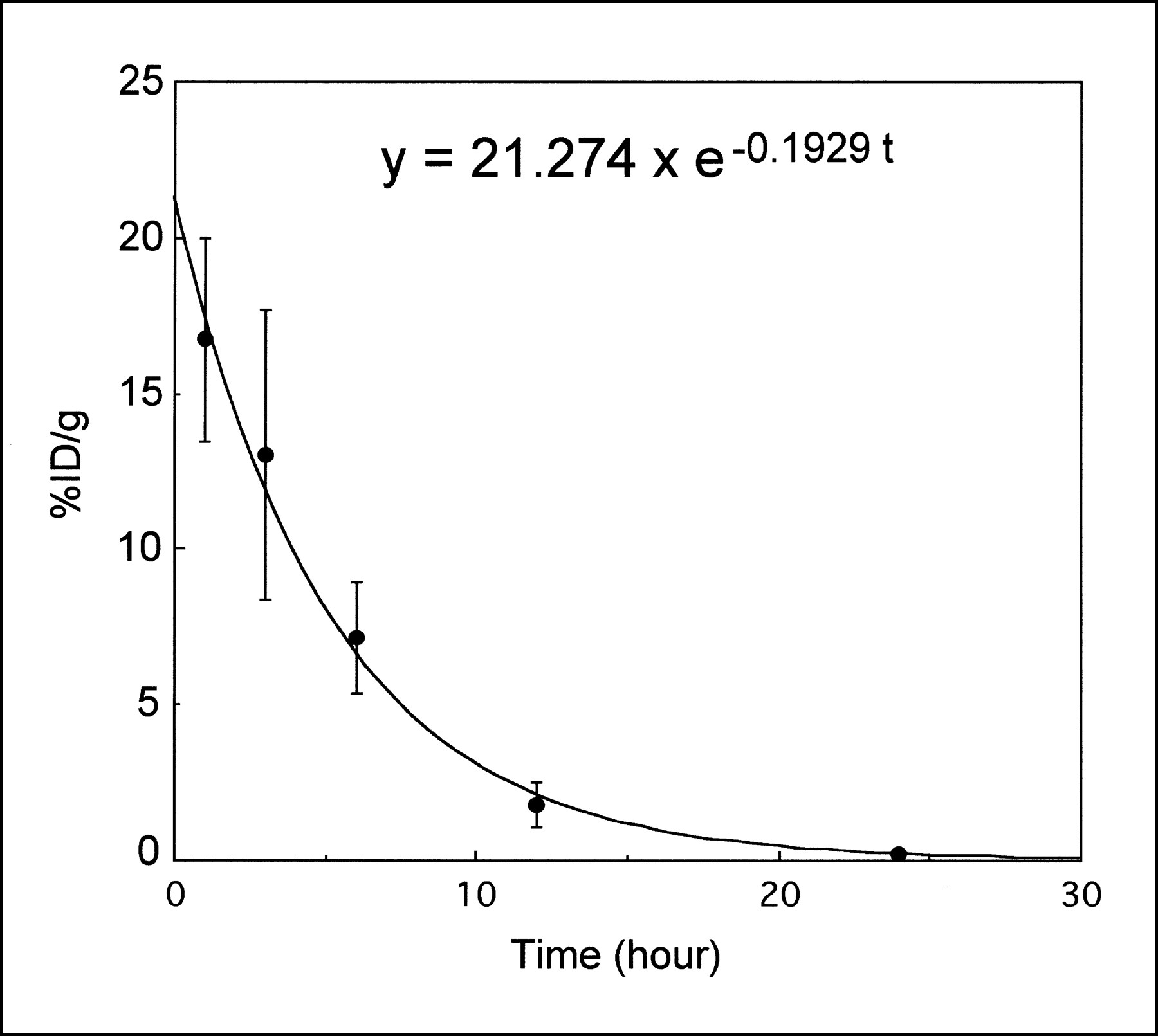
The biodistribution data for 125I− in MCF3B- and MCF7-bearing nude mice are summarized in Table 1. Figure 4 shows tumor (MCF3B)-to-normal tissue or tumor (MCF3B)-to-MCF7 tumor ratios at 1 h after the injection of 125I−. The %ID/g of MCF3B tumors at 1, 3, 6, 12, and 24 h after injection of 125I were 16.73%, 13.02%, 7.17%, 1.78%, and 0.22%, respectively, which were significantly higher percentages than those for MCF7 tumors (P < 0.01). The %ID/g in blood and most organs at 1 h after injection was less than 3.61%, but the %ID/g in the stomach was 39.25%. High tumor-to-normal tissue ratios, ranging from 4.84 (blood) to 21.28 (muscle), were obtained at 1 h after injection, except in the stomach (0.47). Figure 5 shows a time course of iodide accumulation in the tumors. The equation used was as follows: Y = 21.274 e−0.1929t, where t and Y refer to time (in hours) and %ID, respectively. The effective T1/2 in this model was 3.59 h.

Tumor-to-normal tissue ratios. High ratios were obtained as early as 1 h after injection, except in stomach.
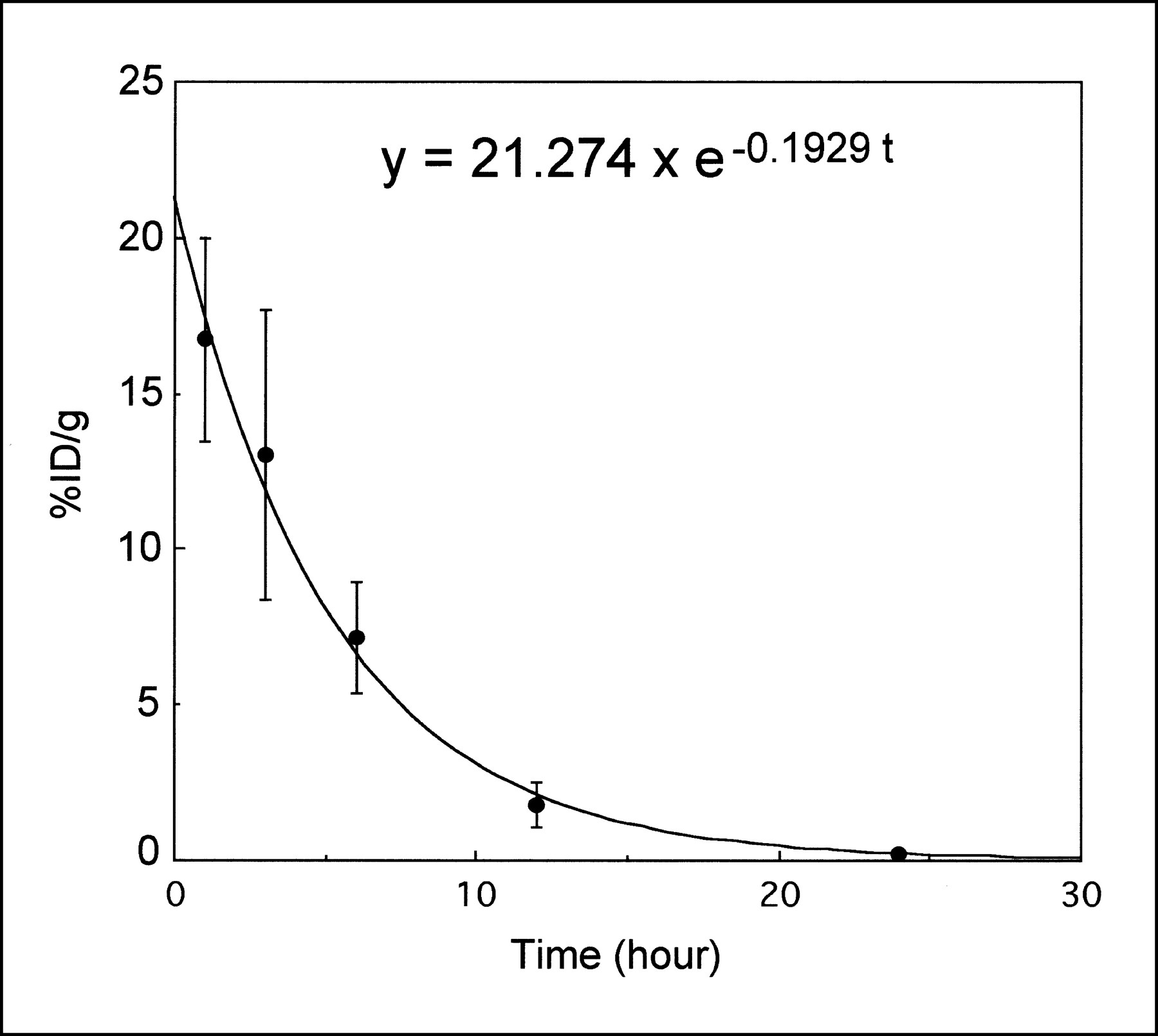
Time course of decay-corrected iodide accumulation in subcutaneous tumors. At 24 h after administration of 125I−, uptake in tumor was reduced to 0.2%. Monoexponential curve fitted for each point was also shown on identical graph. Calculated effective T1/2 was 3.59 h.
Biodistribution Data for Tumor-Bearing Nude Mice
Tumor Imaging
The images were consistent with the results of the biodistribution data (Fig. 6). A clear image with low background activity, including the kidneys, was obtained as early as 2 h after injection of 131I−, but physiologic uptake in the thyroid, stomach, and bladder was seen.

Imaging of MCF3B tumors by gamma camera. Two hours after injection of Na131I (11.1 MBq) intravenously, planar image (B) of mouse was obtained. Note visualized NIS-transduced MCF3B tumor (T). Thyroid, stomach, and bladder were also detected by physiologic uptake. Planar image is to scale with photograph (A).
DISCUSSION
NIS, first identified in FRTL5 cells, plays a critical role in iodide transport in the thyroid gland and in the production of the iodine-containing thyroid hormones. Thyroidal expression of NIS is responsible for highly effective treatment of thyroid cancer, even in advanced metastatic disease, by radioactive iodine administration. Shimura et al. (6) reported transfection of malignantly transformed rat thyroid cells (FRTL-Tc cells), which normally do not concentrate iodide, with a rat NIS–cDNA expression vector. The resulting rat NIS–expressing FRTL-Tc cell line accumulated 125I in vitro and in vivo. Additionally, expression of functionally active NIS was recently reported for human glioma cells using adenovirus-mediated gene delivery (7). Mandell et al. reported that various rat NIS–transfected cells could be selectively killed in vitro by the induced accumulation of 131I (8). These data suggest that NIS gene transfer can restore or newly induce radioiodide uptake in undifferentiated thyroid cancer as well as in malignant tumors derived from nonthyroid tissues.
To our knowledge, ours is the first report describing transfection into breast cancer, which is frequently seen clinically and is apt to metastasize to the lymph nodes, liver, lung, and bone. Our data indicate that transfection was successful and that iodine uptake was through the symporter. These transfected cells stably expressed the NIS gene, and high iodine accumulation in tumors was also confirmed in tumor-bearing mice, suggesting that this strategy may be feasible for a novel cancer treatment. Uptake in normal organs, except the stomach, was low, resulting in high tumor-to-normal tissue ratios ranging from 4.84 (blood) to 21.28 (muscle) at early times. These ratios are acceptable for clinical use, as has been shown for metastatic differentiated thyroid cancer. Macroscopically, the MCF3B tumor could not be distinguished from the MCF7 tumor xenografted at the opposite side with regard to tumor color, superficial vascularity, and degree of necrosis. Therefore, we think that the higher iodine uptake observed in MCF3B is not because of the difference in vascularity but because of the expression of the NIS gene. Possibly, the difference in vasculature between the 2 cells was not seen in the xenografted tumor model. Moreover, we could image tumors 2 h after administration, indicating a usefulness in diagnostic imaging for determining the management strategy. In other words, after transfection with the NIS gene, scintigraphy using a small amount of radioactive iodide would be available for assessment before therapy.
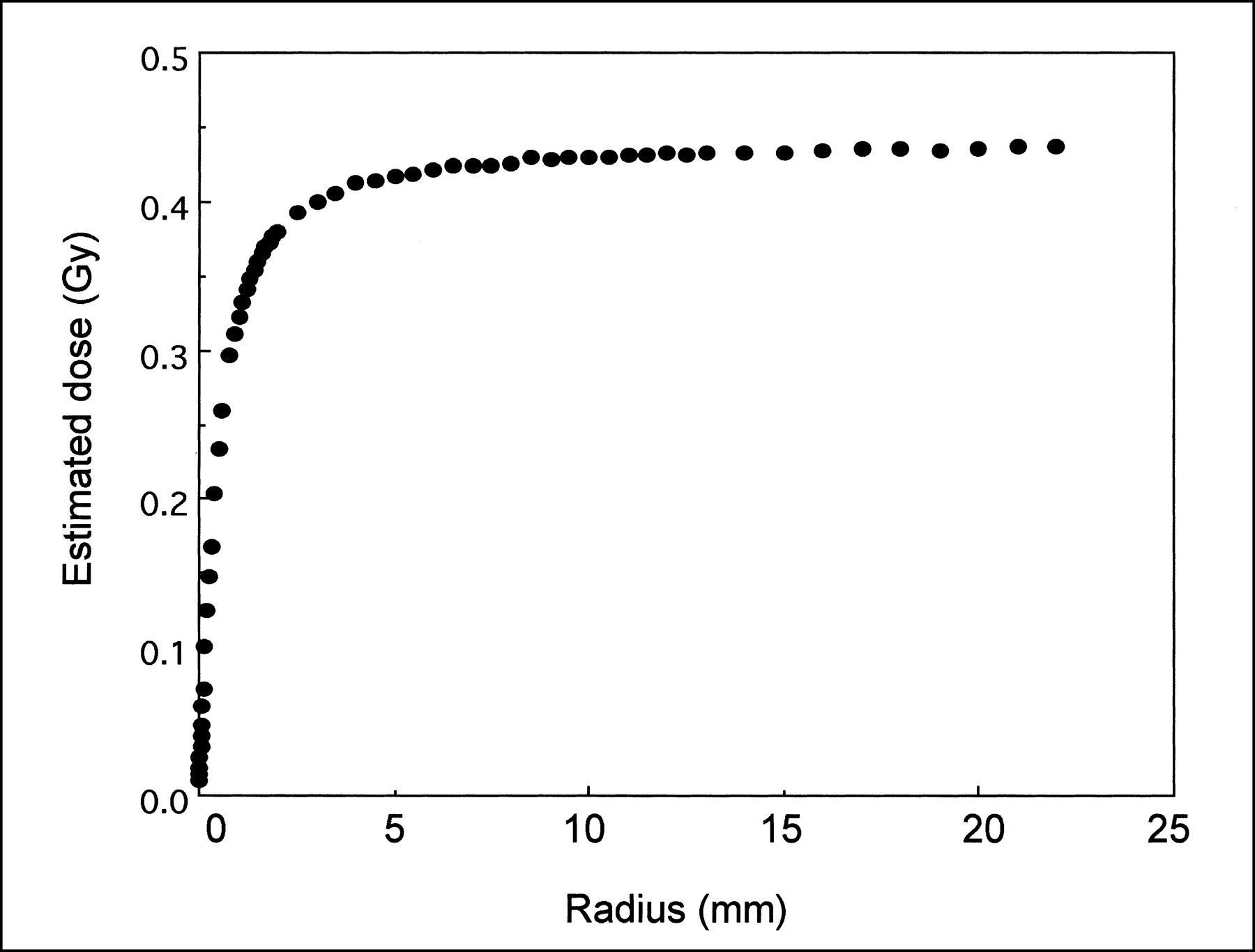
The efficacy of therapy depends not only on the amount of 131I that accumulates in the tumor but also on the time it remains there (14); that is, the biologic T1/2 should match the physiologic T1/2 of 131I (8 d). In the study of Maxon et al. (14), the effective T1/2 of tumors that responded to 131I averaged 78.7 h (equivalent to a biologic T1/2 of 5.5 d), whereas in nonresponders, the effective T1/2 was 45.8 h (equivalent to a biologic T1/2 of 2.5 d). Transfected cancer cells are unlike differentiated thyroid cells; accumulated iodide was apt to flow out extracellularly because the iodide that had been taken up was not involved in organic molecules, as occurs in native thyroid cells. Prompt excretion of iodide from the transfected cells was also shown previously (6). From our in vivo data, the calculated biologic T1/2 in this model is approximately 3.59 h (Fig. 5), whereas that in differentiated thyroid tumors is less than 10 d and that in the normal thyroid is approximately 60 d (15). The dose from accumulated 131I is affected by cell density, radius, and the stopping power of the β particle energy emitted by 131I (16,17). Mandell et al. (8) estimated, on the basis of the results of their in vitro studies, that the NIS-mediated radioiodide accumulation should be more effective in vivo. However, according to our in vivo study, the effective T1/2 is calculated at 3.52 h, considering the physical T1/2 of 131I. If we had administered 3.7 MBq (100 μCi) 131I by a single injection for a tumor with a radius of r mm, its estimated radiation dose should have been as follows: Radiation dose = 3.7 × 106 × ∫0∞ (0.21274 e−0.1969t/3600) × 4/3πr3dt × S, where S is the cumulated activity constant in Gy/Bq/s (18).
The relationship between tumor radius and estimated dose is shown in Figure 7. For a 5-mm radius, the estimated radiation dose was approximately only 0.4 Gy after injection of 3.7 MBq 131I−. Even 3 administrations of 11.1 MBq (300 μCi) would result in at most a therapeutically insufficient 4-Gy radiation dose to the tumor. To obtain therapeutic effects, the residence of radioiodide in the tumor should be prolonged to increase the radiation dose.
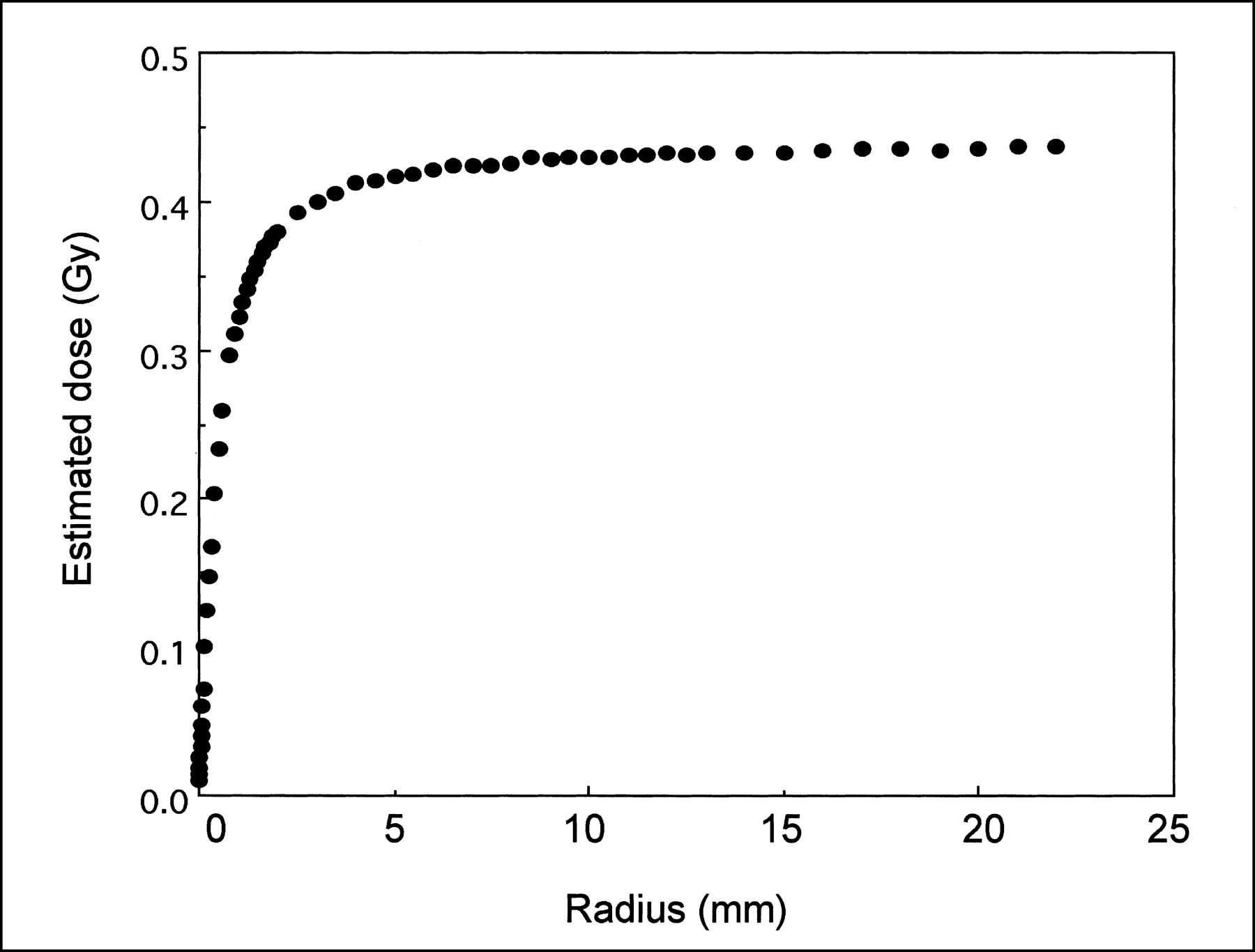
Relationship between radius of tumor and estimated dose for 3.7 MBq 131I administration. Dose increased with increase in radius of tumor but was considered to be therapeutically insufficient.
How can we maintain radionuclide in the cells? In normal thyroid tissue, organification of iodide to thyroid hormone causes retarded excretion. Thyroid peroxidase (TPO) gene is related to this function in thyroidal cells, and a way to overcome the rapid excretion of radioiodide from NIS-transfected tumor may be to transfer TPO gene to induce organification. However, a group reported that transfer of human TPO did not enhance iodide uptake in human anaplastic thyroid carcinoma cells (19), although the transfection of NIS gene was not performed in that group's system. However, lithium, which is used in the prophylaxis of bipolar depressive disorder, in augmentation treatment for depression, and sometimes in therapy for unipolar depression, was found to inhibit the release of iodine from the thyroid, whereas iodine uptake was unimpeded (20,21). Hence, lithium could theoretically increase the absorbed radiation dose to the tumor in radioiodide therapy. Some reports have mentioned lithium as a potential adjuvant to 131I therapy for thyroid carcinoma (22,23). In a report by Koong et al., (23) the largest fractional change in effective T1/2 with lithium occurred in lesions with a biologic T1/2 of less than 3 d. Therefore, lithium is also expected to suppress iodide excretion from transfected cells to allow therapeutic effects from radioiodide therapy.
Eskandari et al. (24) studied the substrate selectivity of NIS. According to their report, inward currents of bromine and fluorine through the symporter are low compared with iodine, although they belong to the halogen. No data were shown for astatine, but if astatine is confirmed to accumulate in the cells through the symporter as iodide accumulates, an α-particle emitter, 211At, may be valuable for delivering concentrated radiation doses of high radiobiologic effectiveness (25) because of its 7.2-h T1/2, 100% α emission, and chemical resemblance to iodine. Indeed, 211At has a relatively short T1/2, which can compensate for a short retention time.
Because this preliminary study focused on characterization of the symporter-transfected cells in vitro and in vivo, some problems remain to be solved. One problem is gene targeting, or how to transfer NIS genes specifically to the target tumors. Recently, Spitzweg et al. (9) succeeded in showing androgen-inducible expression of NIS in prostate cancer cells by coupling the NIS gene to prostate-specific antigen promoter. An effective method of transfection in vivo would also need to be found.
131I therapy for thyroid cancer is used in patients who have undergone total thyroidectomy. In our study, physiologic uptake in the thyroid and stomach was also very high and can be a limiting factor in clinical use. However, total thyroidectomy and supplementation of thyroidal hormone would be acceptable if the usefulness of radioiodide concentrator gene therapy for patients with multiple metastases could be guaranteed.
CONCLUSION
From our preliminary data, inducing cancer cells to express functionally active NIS will enable those cells to accumulate iodide from plasma in vivo and may lead to radioiodine cancer treatment. A method is needed of maintaining radioiodide in the cells to increase the therapeutic effects.
Footnotes
Received Dec. 28, 1999; revision accepted Apr. 10, 2000.
For correspondence or reprints contact: Yuji Nakamoto, MD, Department of Nuclear Medicine, Kyoto University Hospital, 54 Shogoin-kawahara-cho, Sakyo-Ku, Kyoto, 606-8507 Japan.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Transfection of the Human Sodium/Iodide Symporter (NIS) Gene with Liposomes and the Expression of the NIS Protein in Human Lung A549 Cancer Cells
- Radioiodide imaging and radiovirotherapy of multiple myeloma using VSV({Delta}51)-NIS, an attenuated vesicular stomatitis virus encoding the sodium iodide symporter gene
- Enhanced Expression of Adenovirus-Mediated Sodium Iodide Symporter Gene in MCF-7 Breast Cancer Cells with Retinoic Acid Treatment
- A perspective view of sodium iodide symporter research and its clinical implications.
- Development of a Sodium/Iodide Symporter (NIS)-Transgenic Mouse for Imaging of Cardiomyocyte-Specific Reporter Gene Expression
- In vivo Radioiodide Imaging and Treatment of Breast Cancer Xenografts after MUC1-Driven Expression of the Sodium Iodide Symporter
- Long-Term Radioiodine Retention and Regression of Liver Cancer after Sodium Iodide Symporter Gene Transfer in Wistar Rats
- Establishment of a Human Hepatocellular Carcinoma Cell Line Highly Expressing Sodium Iodide Symporter for Radionuclide Gene Therapy
- Iodide Kinetics and Dosimetry In Vivo After Transfer of the Human Sodium Iodide Symporter Gene in Rat Thyroid Carcinoma Cells
- Kinetics of Perrhenate Uptake and Comparative Biodistribution of Perrhenate, Pertechnetate, and Iodide by NaI Symporter-Expressing Tissues In Vivo
- Systemic Retinoic Acid Treatment Induces Sodium/Iodide Symporter Expression and Radioiodide Uptake in Mouse Breast Cancer Models
- In Vitro Cytotoxicity of 211At-Astatide and 131I-Iodide to Glioma Tumor Cells Expressing the Sodium/Iodide Symporter
- Radioiodide Treatment after Sodium Iodide Symporter Gene Transfer Is a Highly Effective Therapy in Neuroendocrine Tumor Cells
- Sodium Iodide Symporter: Its Role in Nuclear Medicine
- The Endogenous Mammary Gland Na+/I- Symporter May Mediate Effective Radioiodide Therapy in Breast Cancer