


Abstract
Internal radiation therapy using intrahepatic arterial injection of 90Y-labeled glass microspheres (90Y-microspheres) has proven to be a promising therapeutic modality for inoperative liver tumor. Recently, direct intratumoral injection of 90Y-microspheres has been performed with even more encouraging results. The purpose of this study was to compare the treatment efficacy of these 2 methods using 90Y-microspheres. Methods: Forty-eight male rats, each bearing a hepatic tumor, were divided into 4 groups (12 rats in each group) to evaluate the efficacy of treatment. Group 1 received an intratumoral injection of 37 MBq (1 mCi) 90Y-microspheres. Group 2 received an intratumoral injection of 0.1 mL normal saline as the control group. Group 3 received an intra-arterial injection of 37 MBq (1 mCi) 90Y-microspheres. Group 4 received an intra-arterial injection of 0.1 mL normal saline as the control group. Tumor size was measured by liver sonography before injection as well as at 2 and 4 wk after injection. Survival time was calculated from the day of treatment to 2 mo after treatment by Kaplan-Meier survival analysis. The response rate was evaluated by the change in tumor size and survival time. Fisher's exact, 2-tailed test was used to compare response rates. Results: In the rats treated by intratumoral injection of 90Y-microspheres, 83.3% (10/12) showed a good response. In contrast, all 12 rats in the control group showed a poor response. The difference was significant (P < 0.00001). Eighty-three percent (10/12) of the rats survived >60 d after intratumoral injection of 90Y-microspheres, whereas only 25% (3/12) of the control rats survived >60 d. The difference was significant (P = 0.0068). In the rats treated by intra-arterial injection of 90Y-microspheres, 58.3% (7/12) showed a good response to the treatment. All rats in the control group showed a poor response. The difference was significant (P = 0.0023). Sixty-six percent (8/12) of the rats survived >60 d after intra-arterial injection of 90Y-microspheres, whereas only 16.7% (2/12) of the control rats survived >60 d. The difference was significant (P = 0.0385). However, the response rate and survival time between the intratumoral treatment group and the intra-arterial treatment group showed no significant difference (P = 0.3707 and 0.3988, respectively). Conclusion: Both methods (intratumoral treatment and intra-arterial treatment) showed a significantly good response rate and prolonged survival time compared with those of the control groups. However, no significant difference was found in the response rate or survival time between intratumoral treatment and intra-arterial treatment.
The treatment of liver tumors remains unsatisfactory. Hepatocellular carcinoma is almost always lethal because the disease is inoperable in most patients at the time of diagnosis, as a result of either extensive bilobar involvement or advanced hepatic cirrhosis (1,2). Intrahepatic arterial injection of 90Y-labeled glass microspheres (90Y-microspheres) has been introduced as an encouraging treatment modality for inoperable liver tumor, especially for hepatocellular carcinoma (3–7). Intra-arterial administration of 90Y-microspheres can deliver a tumorcidal dose of radiation to a liver tumor without jeopardizing nontumorous liver tissue (4). Nevertheless, selective catheterization that is highly dependent on operator skill and equipment is needed for intra-arterial infusion. In an attempt to obtain better therapeutic results and to simplify the procedure, Tian et al. (8) directly injected 90Y-microspheres into liver tumors under real-time sonographic guidance in 1996. They reported that intratumoral 90Y-microsphere injection showed better results than both traditional treatment and intra-arterial 90Y-microsphere injection. However, whether this technique is better than the intra-arterial injection technique for the treatment of liver tumors remains controversial (9).
The purpose of this study was to evaluate the effectiveness of 90Y-microspheres administered by direct intratumoral injection or intrahepatic arterial injection. We compared the change in tumor size and the survival in rats after treatment by each of these methods. In addition, we discuss the advantages and disadvantages of these 2 methods of 90Y-microsphere administration in the treatment of hepatic tumors.
MATERIALS AND METHODS
Animals and Tumor Cell Line
Male rats (Sprague-Dawley rats; National Laboratory Animal Breeding and Research Center, Taiwan) weighing 200–250 g were fed a standard chow diet and given water ad libitum. An N1-S1 hepatoma cell line (American Type Culture Collection, Rockville, MD) was used for tumor implantation. The tumor cells were routinely cultured in a mixture of Dulbecco's Modified Eagle Medium (GIBCO, Paisley, UK), 5% fetal bovine serum, 1% l-glutamine, and 20% horse serum. After growing exponentially for 1 wk, a concentration of ∼106 to 107 cells/mL was established. The cell viability was >90% as determined by trypan blue exclusion.
Inoculation
A subxyphoid laparotomy, 1.5–2 cm in length, was performed to expose the left and right lobes of the liver. Using a 27-gauge needle, a tumor cell suspension containing 4 × 106 cells/0.05 mL was slowly injected into 1 of the hepatic lobes under the liver capsule, raising a visible pale wheal. The puncture site was gently compressed with cotton gauze for 15 s to prevent bleeding. The wound was then closed in layers. Ten days after inoculation, sonography was performed to check tumor growth. Injection of 90Y-microspheres was performed the day after sonography.
90Y-Microspheres
The 90Y-microspheres (TheraSphere; Nordion International, Vancouver, BC, Canada) were supplied in 0.05 mL sterile, pyrogen-free water in a 0.3-mL V-bottom vial secured within a 12-mm clear acrylic vial shield. The mean sphere diameter of the 90Y-microspheres ranged from 20 to 30 μm. Each milligram contained 22,000–73,000 microspheres. The number of microspheres in 37 MBq (1 mCi) is changing continuously because of the decay effect of 90Y. However, the number is about 15,000 microspheres in 37 MBq at the calibration time.
Intrahepatic Arterial Injection of 90Y-Microspheres
A midline laparotomy was performed under anesthesia by intraperitoneal injection of ketamine. The hepatic artery and the gastroduodenal branch were identified and isolated. A temporary sling was placed around the hepatic artery proximal to the gastroduodenal branch to prevent back flow. After ligation of the distal end of the gastroduodenal branch, this artery was cannulated with fine (number 10) polyethylene tubing (Clay Adams Dickinson, Parsippany, NJ) that was secured with a fine silk tie and connected to a syringe. After injection of 37 MBq (1 mCi) 90Y-microspheres or normal saline in a volume of 0.1 mL, the cannula was flushed with 0.2 mL saline and removed. The proximal end of the gastroduodenal branch was then ligated. The sling around the hepatic artery was removed, and hepatic arterial circulation was restored.
Direct Intratumoral Injection of 90Y-Microspheres
A subxyphoid laparotomy, 3–4 cm in length, was performed under anesthesia by intraperitoneal injection of ketamine. After exposing the hepatic tumor, 37 MBq (1 mCi) 90Y-microspheres or normal saline in a volume of 0.1 mL were injected slowly into the center of the tumor. The puncture site was gently compressed with cotton gauze for 60 s to prevent bleeding.
Monitoring and Follow-Up
Forty-eight male rats, each bearing a liver tumor, were divided into 4 groups (12 rats in each group) to evaluate the efficacy of treatment. Group 1 received an intratumoral injection of 37 MBq (1 mCi) 90Y-microspheres. Group 2 received an intratumoral injection of 0.1 mL normal saline as the control group for group 1. Group 3 received an intra-arterial injection of 37 MBq (1 mCi) 90Y-microspheres. Group 4 received an intra-arterial injection of 0.1 mL normal saline as the control group for group 3. Tumor size was measured by liver sonography (128 × P computed sonography; Acuson Corp., Mountain View, CA) before injection and at 2 and 4 wk after injection. The maximum length and width of each lesion were measured by the same experienced sonography physician using the same machine. Survival time was calculated, using a computer program, from the day of treatment to 2 mo after treatment by Kaplan-Meier survival analysis. The response to treatment was classified according to the survival time and change in tumor size from before treatment to the fourth week after treatment: 1, good response (tumor size decreased); 2, poor response (any condition less than a good response or survival time <60 d). Fisher's exact, 2-tailed test was used to calculate the differences in response rate.
RESULTS
Table 1 shows the treatment effects and survival times of rats receiving intratumoral injection of 90Y-microspheres. Of the rats treated by intratumoral injection of 90Y-microspheres, 10 showed a good response to the treatment (Fig. 1). The complete disappearance of tumor was noted in 5 rats. Two rats showed a poor response to treatment. In the control group, the response to normal saline was poor in all 12 rats. The difference in the response rate was significant (P = <0.00001). Eighty-three percent (10/12) of the rats survived >60 d after intratumoral injection of 90Y-microspheres, whereas only 25% (3/12) of control animals survived >60 d (Fig. 2A). The difference was significant (P = 0.0068).
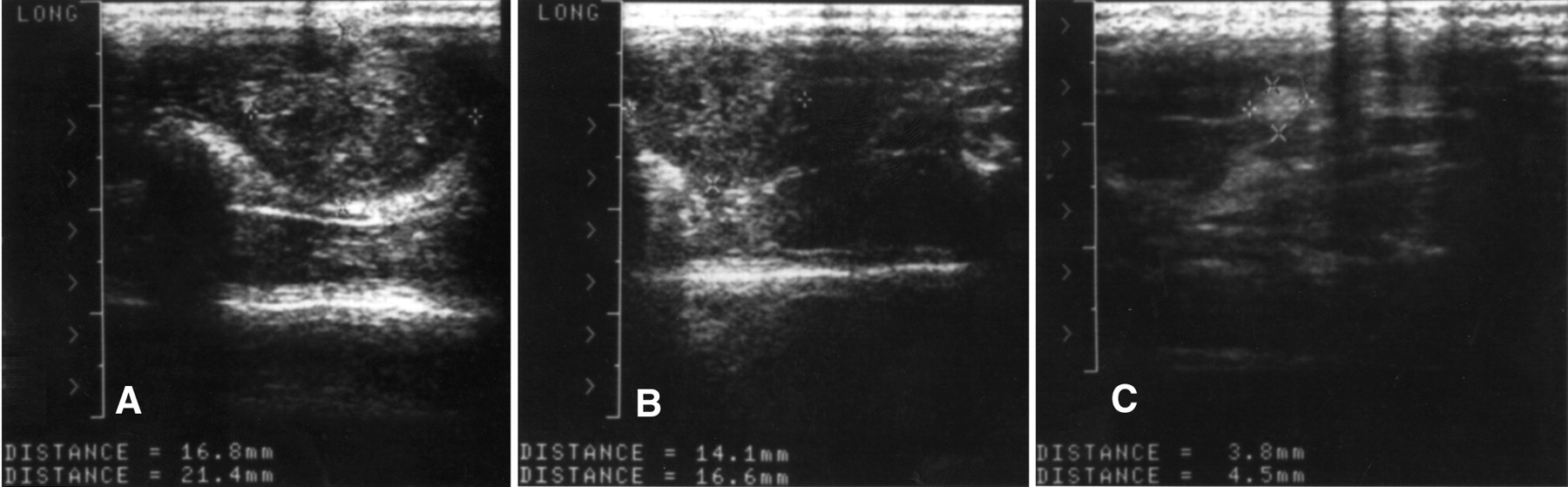
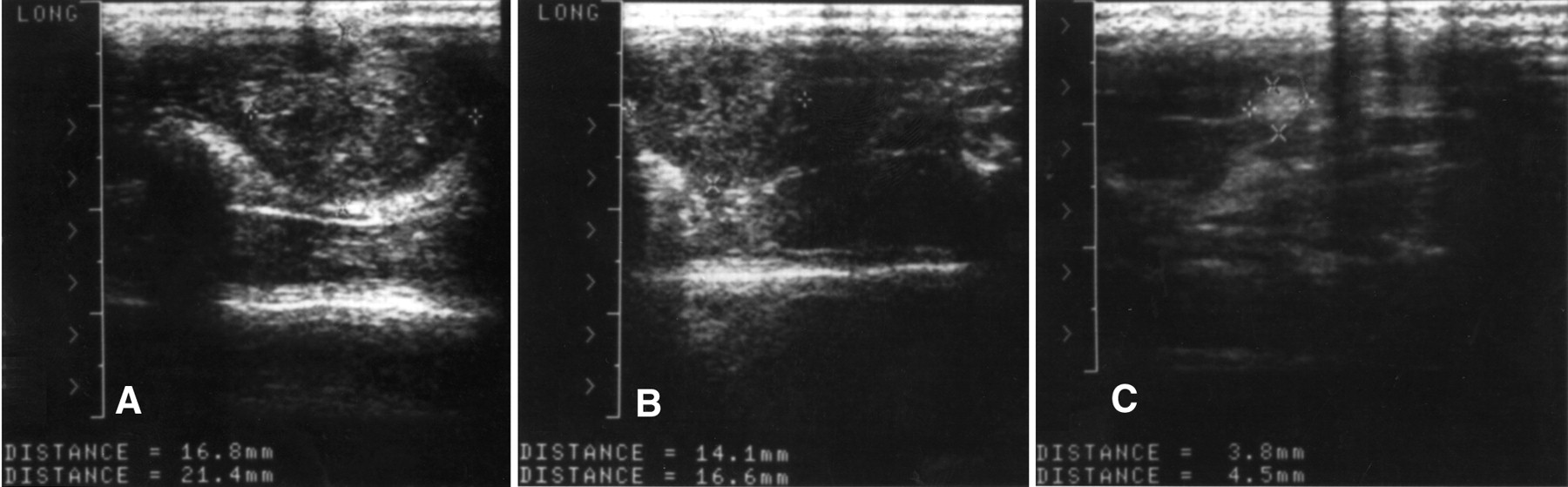
Change in tumor size of rat 1 in intratumoral group measured by sonography before treatment (A), in second week (B), and in fourth week (C) after intratumoral injection of 37 MBq 90Y-microspheres. Tumor size decreased significantly after treatment.

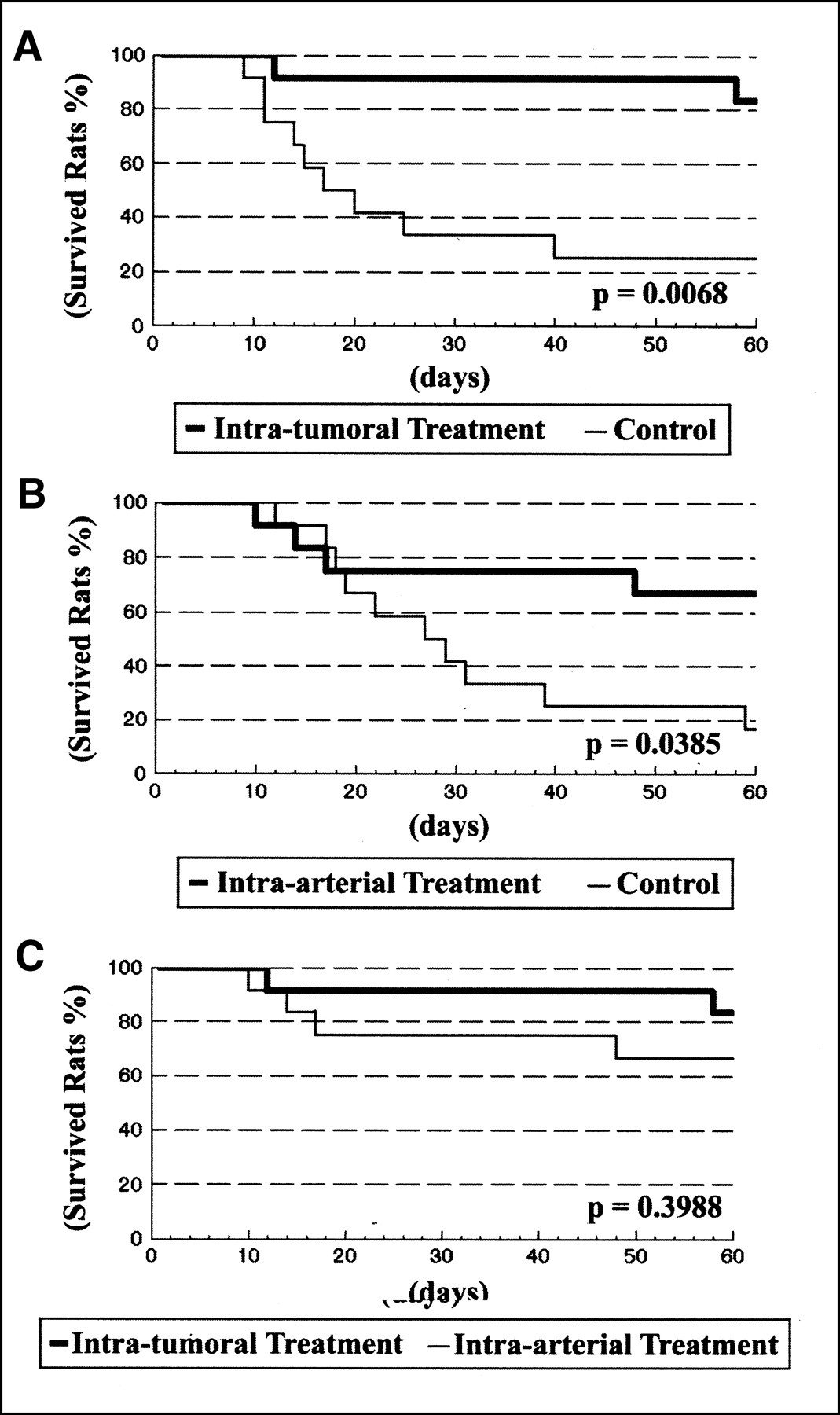
Survival curves for rats of 4 groups. (A) Comparison between rats treated by intratumoral injection of 90Y-microspheres and control rats that received only normal saline. Difference is significant (P = 0.0068). (B) Comparison between rats treated by intra-arterial injection of 90Y-microspheres and control rats that received only normal saline. Difference is significant (P = 0.0385). (C) Comparison between rats treated by intratumoral injection of 90Y-microspheres and rats treated by intra-arterial injection of 90Y-microspheres. Difference is not significant (P = 0.3988).
Detailed Data of Control Group and Rats with Liver Tumor After Intratumoral Injection of 90Y-Microspheres
Table 2 shows the treatment effects and survival times of rats receiving intra-arterial injection of 90Y-microspheres. Of the rats treated by intra-arterial injection of 90Y-microspheres, 7 showed a good response to the treatment. The complete disappearance of tumor was noted in 4 rats. Five rats showed a poor response to treatment, including 4 rats that died during this study and 1 rat with a good response in the second week but with tumor rebound in the fourth week. In the control group, the response to normal saline was poor in all 12 rats. The difference was significant (P = 0.023). Sixty-six percent (8/12) of the rats survived >60 d after intra-arterial injection of 90Y-microspheres, whereas only 16.7% (2/12) of control animals survived >60 d (Fig. 2B). The difference was significant (P = 0.0385).
Detailed Data of Control Group and Rats with Liver Tumor After Intra-Arterial Injection of 90Y-Microspheres
The response rate and survival time between the intratumoral treatment group and the intra-arterial treatment group showed no significant difference (P = 0.3707 and 0.3988, respectively) (Fig. 2C).
DISCUSSION
90Y is a pure β-particle emitter with a physical half-life of 64 h and a mean energy per disintegration of 0.973 MeV. The β particles have a mean tissue penetration of 2.5 mm, with a maximum penetration of about 10 mm. The physical characteristics of 90Y make it a suitable isotope for the administration of localized internal radiation therapy (10,11). Initial studies in this field used 90Y-labeled inert ceramic or resin microspheres. Although the response rates were encouraging, several patients died of myelosuppression from bone marrow uptake of free 90Y (12,13). In the late 1980s, 90Y-microspheres were developed by incorporating 89Y oxide into the glass matrix and activating the 89Y into 90Y by neutron bombardment before using the spheres as radiotherapeutic vehicles. The microspheres themselves are nondegradable and, therefore, infinitely stable, thus preventing leakage of 90Y into the bloodstream, decreasing the unnecessary radiation burden to systemic organs, and eliminating major complications such as myelosuppression (14,15).
90Y-microspheres have now become commercially available in unit doses. The technique of intra-arterial injection of 90Y-microspheres has been well established and has played a role in the treatment of hepatic tumors. Intra-arterial infusion of 90Y-microspheres possesses dual functions of internal radiation and embolization (radioembolization). Many studies have reported the effectiveness of intra-arterial infusion of 90Y-microspheres in the treatment of liver tumors (14–16). However, the intra-arterial injection method has some disadvantages (8,17). First, this technique requires extremely selective catheterization and is, therefore, highly dependent on operator skill and equipment. Second, the radionuclide reaches the tumor site by a nonspecific route. This means that normal tissue is irradiated in the same way as the tumor. Third, because of the nonspecific distribution, large quantities of radionuclides must be used.
Tian et al. (8) reported the novel use of sonographically guided, 90Y-microsphere interstitial radiotherapy in the treatment of hepatic malignancies. In their study, intratumoral 90Y-microsphere injection showed better results than intra-arterial 90Y-microsphere injection. According to our data, both methods (intratumoral treatment and intra-arterial treatment) showed good effectiveness in treating liver tumors compared with that of the control groups. Significant differences were found in both the response rate and the survival time between the treatment group and the control group. In most rats treated with 90Y-microspheres, the response was obvious in the second week and lasted to the fourth week after treatment. The complete disappearance of the tumor was noted in 5 rats treated by intratumoral injection and in 4 rats treated by intra-arterial injection. The good response rate of the intratumoral injection group was higher than that of the intra-arterial injection group (83% versus 58%). However, the difference was not significant (P = 0.3707 by Fisher's exact test, 2-tailed). In addition, the survival time of the rats treated by intratumoral injection was longer than that of the rats treated by intra-arterial injection, but this difference was also not significant (P = 0.3988 by Kaplan-Meier survival analysis).
The technique of direct intratumoral injection is attractive for the treatment of liver tumor because it is a relatively simple, less-painful, outpatient procedure. It is the most straightforward method of bringing the radioactivity into the tumor while avoiding a high radiation dose to the nontumorous tissue. In addition, our data indicate that the treatment results of intratumoral injection group are promising. However, this method also has some drawbacks (7). The radiation hazard to both the patient and the hospital personnel needs to be evaluated with this procedure. Extratumoral leakage of the 90Y-microspheres into the peritoneal cavity or shunting of the microspheres to the lungs and intestines may result in serious complications. According to the study by Tian et al. (8), leakage of 90Y-microspheres from the tumor can occur. In their study, 6 of 11 patients were found to have left lung radioactivity, and 4 were found to have intestinal radioactivity. In the case of a large tumor, multiple injections are needed, and the 90Y-microspheres may not be distributed evenly throughout the entire tumor. In patients with multiple nodular tumors, the effectiveness of this direct intratumoral injection method may be also limited. Moreover, it is difficult to reach a tumor that is deeply seated. Therefore, more research on this new technique is needed before it can be widely accepted.
According to previous reports, the radiation dose to the tumor varied between 88 and 305 Gy after intrahepatic arterial injection of 54–189 mCi 90Y-microspheres (18,19). In the study by Tian et al. (8), the radiation dose at 0.5–0.8 cm from the source was about 14–757 Gy after intratumoral injection of 2.5 mCi 90Y-microspheres. Because intratumoral injection is a straightforward method of bringing the radioactivity into the tumor, a small quantity of 90Y-microspheres supplied by intratumoral injection can deliver high radiation to the tumor cell compared with that of intra-arterial injection (8).
The radiation damage of 90Y-microspheres to the normal liver should be small because 90Y emits only β particles, which have a mean tissue penetration of 2.5 mm, with a maximum of only 10 mm. In a study by Andrew et al. (5), 24 patients with liver tumors received intrahepatic arterial injection of 1739–8436 90Y-microspheres. Only mild and transient elevations in the transaminase levels were evident after the treatment. No hepatic toxicity was noted. In a study by Yan et al. (18), 18 patients with liver tumors received intrahepatic arterial injection of 2442–5550 MBq 90Y-microspheres. Transient elevations of glutamic pyruvic transaminase levels were found in 8 patients after the treatment but the levels decreased within 2 wk. Bilirubin and alkaline phosphatase levels remained normal. In the study by Tian et al. (8), 33 patients with liver tumors received intratumoral injection of 740–4440 MBq 90Y-microspheres. No changes in liver function were detected in these patients after treatment.
CONCLUSION
Our data suggest that both the intratumoral method and the intra-arterial method have a good response and a long survival time in treating liver tumors compared with those of the control groups. The response rate and survival time of the intratumoral treatment group were better than those of the intra-arterial treatment group, but the difference was not significant.
Acknowledgments
This study was supported in part by a grant (TCVGH-896703C) from Taichung Veterans General Hospital, Taiwan.
Footnotes
Received Nov. 8, 1999; revision accepted Apr. 4, 2000.
For correspondence or reprints contact: Wan-Yu Lin, MD, Department of Nuclear Medicine, Taichung Veterans General Hospital, No. 160, Section 3, Taichung Harbor Rd., Taichung 407, Taiwan.




{kind=link}
{kind=link}