


Abstract
Since the approval of trastuzumab, a humanized monoclonal antibody against the extracellular domain of human epidermal growth factor receptor 2 (HER2), 3 other HER2-targeting agents have gained regulatory approval: lapatinib, pertuzumab, and trastuzumab–emtansine. These agents have revolutionized the management of HER2-positive breast cancer, highlighting the concept that targeted therapies are successful when patients exhibit tumor-selective expression of a molecular target—in this case, HER2. However, response prediction and innate or acquired resistance remain serious concerns. Predictive biomarkers of a response—which could help in the selection of patients who might benefit from a selected targeted therapy—are currently lacking. Molecular imaging with anti-HER2 probes allows the noninvasive, whole-body assessment of HER2 tumor burden and has the potential to improve patient selection, optimize the dose and schedule, and rationalize assessment of the response to anti-HER2 therapies. Furthermore, unlike biopsy-based HER2 assessment, this approach can reveal inter- or intratumoral heterogeneity as well as variations in HER2 expression over time. This review summarizes the available literature and the current status of molecular imaging as a tool for the assessment of HER2 (target) expression or the prediction of an early treatment response in early and advanced HER2-positive breast cancer.
Human epidermal growth factor receptor 2 (HER2) is overexpressed in several cancers, including breast, gastric, ovary, prostate, bladder, and lung cancers, and is a proven therapeutic target in the first 2 tumor types (1,2). In breast cancer (BC), in particular, HER2 overexpression is found in 15%–25% of patients and is associated with a clinically aggressive course. Successful targeting of HER2 with a range of anti-HER2 drugs has resulted in markedly improved patient outcomes in both advanced and early disease settings (3).
However, the presence of a target (in this case, HER2) does not always guarantee benefit from matched targeted therapies because downstream signaling resistance or escape can occur. In HER2-overexpressing BC, it has been estimated that about 50% of patients with metastases do not benefit from anti-HER2 therapies (4), and not a single biomarker for identifying nonresponding patients has yet been validated (5).
Furthermore, there is increasing evidence of temporal and spatial heterogeneity in BC HER2 overexpression. Patients with negative test results at diagnosis can have positive test results later in the disease course and vice versa, a fact that explains why biopsy of metastatic disease is a strong recommendation of many clinical treatment guidelines (6). Heterogeneity in biomarker expression at metastatic sites is only beginning to be recognized, with growing appreciation for molecular imaging.
This article focuses on HER2-positive BC and provides a comprehensive overview of the present and future roles of molecular imaging in improving target mapping, predicting benefit from chemotherapy with or without anti-HER2 drugs, and selecting patients for the targeted delivery of potent cytotoxic agents or therapeutic isotopes.
IMAGING OF HER2 (TARGET) EXPRESSION
In clinical practice, HER2 status is determined by immunohistochemistry (IHC) (usually with an antibody recognizing the intracellular domain of the receptor (7)) or fluorescence in situ hybridization (FISH), mostly from the primary tumor and sometimes from a metastatic lesion. HER2 positivity is defined as an IHC score of 3+ or an IHC score of 2+ with a FISH score of greater than or equal to 2.0 (8).
Bearing in mind the heterogeneity of HER2 expression and the resulting issues with macro- and microsampling of tumor samples, whole-body HER2 imaging could complement current standard approaches. Depending on the desired HER2 imaging technique—SPECT or PET—various isotopes can be used, with the latter modality offering images with higher resolution or sensitivity and allowing quantification.
Imaging can be performed with various targeting molecules, such as antibodies, peptides, small-molecule ligands, and aptamers. A full-length, high-molecular-weight monoclonal antibody (mAb) offers slow blood hepatobiliary clearance. In contrast, its bioengineered derived fragments [Fab fragments, F(ab′)2] and variants (scFv, diabodies, and minibodies) and nontraditional protein scaffolds (Affibody molecules, Nanobodies, and anticalins) result in faster pharmacokinetics with similar affinity and specificity (9). These low-molecular-weight probes can be radiolabeled with isotopes—such as 68Ga, 18F, 64Cu, and 76Br for PET imaging—that have a short half-life, allowing imaging on the day of injection with a low radiation burden. In contrast, when mAbs are radiolabeled with isotopes that have a longer half-life—such as 89Zr, 124I, and 86Y for PET imaging and 111In for SPECT imaging—images can be retrieved up to several days after tracer injection, allowing optimal uptake in tumor tissue.
Preclinical Setting
Since the introduction of trastuzumab (a humanized mAb against HER2) for the treatment of HER2-positive BC more than a decade ago (4), trastuzumab-based HER2 imaging has received increasing attention, with some modalities reaching a successful transition from the laboratory to the clinic.
111In-, 86Y-, and 225Ac-radiolabeled trastuzumab (10–12) was introduced first; 89Zr-trastuzumab (13) was introduced a few years later in human tumor–bearing mice. Specific tumor uptake in HER2 tumor–bearing mice was confirmed with higher resolution and better quantification on 89Zr-trastuzumab PET images. In addition to high stability and maintenance of affinity, this tracer had the immunoreactivity and internalization properties of trastuzumab, despite the radiolabeling modifications. Furthermore, it was recently demonstrated (14) that trastuzumab-based tracers, such as 89Zr-trastuzumab, can reveal more than the mere expression of HER2; they can reveal its accessibility. Steric hindrance of mucin MUC4, masking the trastuzumab-binding epitope on HER2, negatively affected 89Zr-trastuzumab tumor uptake. This effect could be counteracted by supplementation with a mucolytic agent, such as N-acetylcysteine, in patient-derived HER2- and MUC4-overexpressing tumors (JIMT1).
An anti-HER2 mAb introduced later—pertuzumab—was also radiolabeled with 111In or 89Zr and was used to successfully image HER2-positive tumor xenografts (15,16).
In addition to mAbs, several reports have demonstrated the usefulness of HER2 imaging with Affibody-based tracers. Interestingly, in a study directly comparing a 124I-trastuzumab mAb with Affibody 124I-ZHER2:342, the Affibody showed even higher tumor-to-organ ratios than the mAb because of rapid clearance of radioactivity from blood and normal organs (17).
Several anti-HER2 Affibody molecules have also been labeled with 68Ga, 18F, 64Cu, and 11C for PET and with 99mTc and 111In for SPECT (18–21). Affibody ABY-002 radiolabeled with 111In for SPECT as well as with 68Ga for PET was shown to specifically target HER2-expressing xenografts in vivo with both isotopes, but the pharmacokinetic profile for 68Ga-radiolabeled ABY-002 was favored (20). Both tracers were investigated further in BC patients (22); the findings were in agreement with the preclinical data.
Furthermore, to guarantee maintenance of the targeting abilities of low-molecular-weight Affibody molecules, Wållberg et al. proposed a Sel-tagging technique enabling site-specific 11C radiolabeling of anti-HER2 Affibody ZHER2:342, resulting in a molecule with lower kidney retention and an overall absorbed dose comparable to that of 68Ga-ZHER2:342 (21).
HER2 imaging has also been investigated with even smaller probes, namely Nanobodies (23,24). Many anti-HER2 Nanobodies for the noninvasive imaging of HER2 expression have been proposed (23). Studies with Nanobodies radiolabeled with 99mTc (2Rs15dHis6) in mice bearing HER2-positive tumors revealed fast blood clearance, low accumulation in nontarget organs (except the kidneys, which are responsible for tracer clearance), and high concomitant tumor-to-blood and tumor-to-muscle ratios at 1 h after injection (24). PET imaging of HER2 expression with 68Ga-radiolabeled Nanobodies is currently being evaluated by the same group of researchers (Fig. 1) (25).
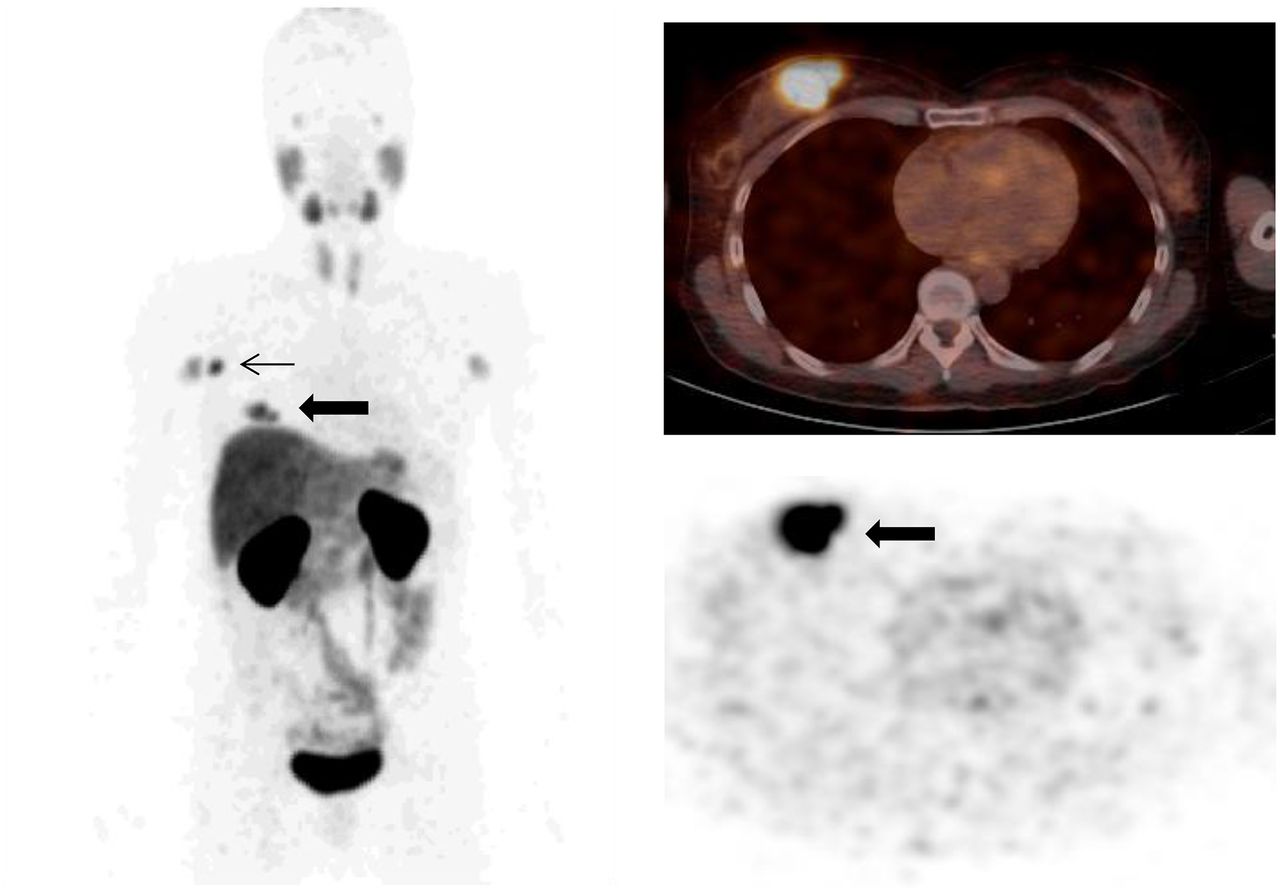
Uptake of 68Ga-HER2-Nanobody in primary breast carcinoma (thick arrow) and invaded lymph node (thin arrow) with high HER2 expression. (Left) Maximum-intensity-projection PET image. (Top right) PET/CT fusion image. (Bottom right) Corresponding PET image. (Courtesy of Marleen Keyaerts, UZ Brussel, Brussels, Belgium.)
In addition to the aforementioned probes, oligonucleotides, RNA, and DNA aptamers were recently introduced. A modified RNA aptamer with HER2-specific targeting was labeled with 99mTc and allowed SPECT imaging of HER2 expression (26,27). Another group used 64Cu-WT4340 for PET imaging of HER2 messenger RNA and also demonstrated its successful use for evaluating the therapeutic efficacy of doxorubicin therapy in immunocompromised mice carrying human HER2–positive BC xenografts (28). These new types of radiotracers have so far been investigated only in preclinical models.
Furthermore, various groups have also investigated the use of HER2 imaging for the evaluation of molecular responses to anti-HER2 therapy (heat shock protein 90 [HSP90] and trastuzumab) in vivo in human tumor xenografts with 68Ga-labeled F(ab′)2-trastuzumab (29), 89Zr-trastuzumab (30), and 18F–N-[2-(4-fluorobenzamido)ethyl]maleimide–ZHER2:342 PET/CT (31) and 111In-pertuzumab SPECT/CT (16). All of these modalities allowed the sensitive detection of HER2 downregulation.
Clinical Setting
Table 1 summarizes the results of 7 clinical studies of HER2 imaging in BC patients.
Molecular Imaging Studies Seeking to Confirm HER2 Overexpression in Early and Advanced HER2-Positive Breast Cancer
In 2000, a pilot study with 10 HER2-positive metastatic BC patients treated with trastuzumab concluded that 111In-trastuzumab immunoscintigraphy allowed diagnostic predictions with respect to therapeutic efficacy and cardiotoxicity (32). Others investigating this issue in HER2-positive advanced BC patients before treatment with trastuzumab and paclitaxel (33) reported different results. Indeed, of the 15 patients, only 1 showed myocardial uptake not translating into the development of heart failure.
Nonetheless, HER2-positive tumors were imaged, albeit with a low detection rate, probably because of the poor resolution of SPECT. Imaging quality was remarkably improved with the introduction of 89Zr-trastuzumab, allowing PET imaging (13). The best time for the assessment of tracer uptake in metastatic lesions was determined to be 4–5 d after tracer administration. Brain metastases, among other metastatic sites, were also successfully imaged. The study also highlighted the importance of the mass of administered protein, concluding that in trastuzumab-naive patients, a higher mass of (nonradiolabeled) trastuzumab (50 mg) enabled better distribution of the tracer into the metastatic lesions.
In addition, trastuzumab was also labeled with 64Cu in studies of both early and advanced HER2-positive BC (34,35). In both studies, the best time for imaging was 48 h after tracer injection. However, the results were different; the coinjection of 45 mg of trastuzumab enabled better visualization of liver metastases (35), whereas the results obtained with the administration of only the radiotracer were suboptimal because of a higher liver background (34). Interestingly, both studies compared 64Cu-trastuzumab PET/CT with 18F-FDG PET/CT, with a maximum of 13 d in between, and showed that some lesions could be detected only with 64Cu-trastuzumab PET/CT.
Apart from HER2-directed antibodies, 2 different Affibody molecules, ABY-002 (22) and ABY-025 (36,37), were labeled with 68Ga or 111In and injected into patients with advanced BC. In all of the studies, the radiolabeled Affibody molecules allowed imaging of HER2-positive lesions and even brain metastases (36). In the most recent study, increasing tracer uptake over time allowed discrimination between HER2-positive and HER2-negative lesions on the basis of radiotracer uptake and as confirmed by IHC (37). One issue was that because of the high background uptake of the radiolabeled Affibody molecules in the liver, the HER2 status of lesions in this organ could not be properly assessed.
Furthermore, successive HER2 imaging for different therapies was also studied. In one study, HER2 downregulation in the presence of an HSP90 inhibitor could be monitored through a decrease in 89Zr-trastuzumab uptake and was correlated with a response by RECIST 1.0 (38). In another study by the same group, trastuzumab combined with paclitaxel treatment led to a 20% decrease in 111In-trastuzumab tumor uptake. Interestingly, although tumor uptake decreased, HER2 imaging was still achievable, suggesting that sufficient HER2 is constantly available at the tumor cell membrane to bind trastuzumab (39).
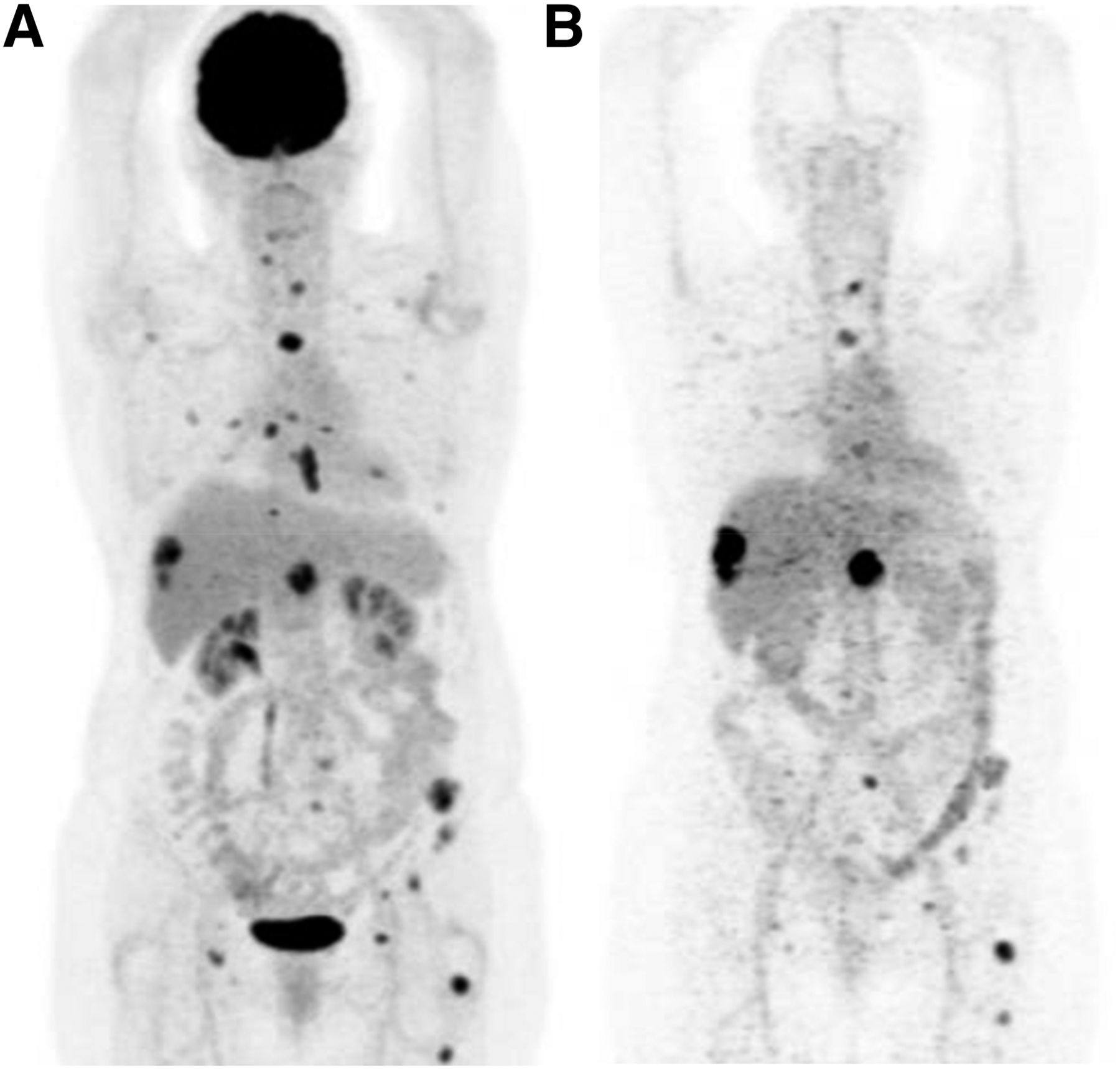
Regardless of the aforementioned findings, it is critical to demonstrate that assessing HER2 with molecular imaging in advanced BC has clinical utility. Three prospective clinical trials have been designed to address this important question: 1 study at Institut Jules Bordet (NCT01420146) and 2 studies at the University Medical Center Groningen (NCT01832051 and NCT01957332) (Fig. 2).
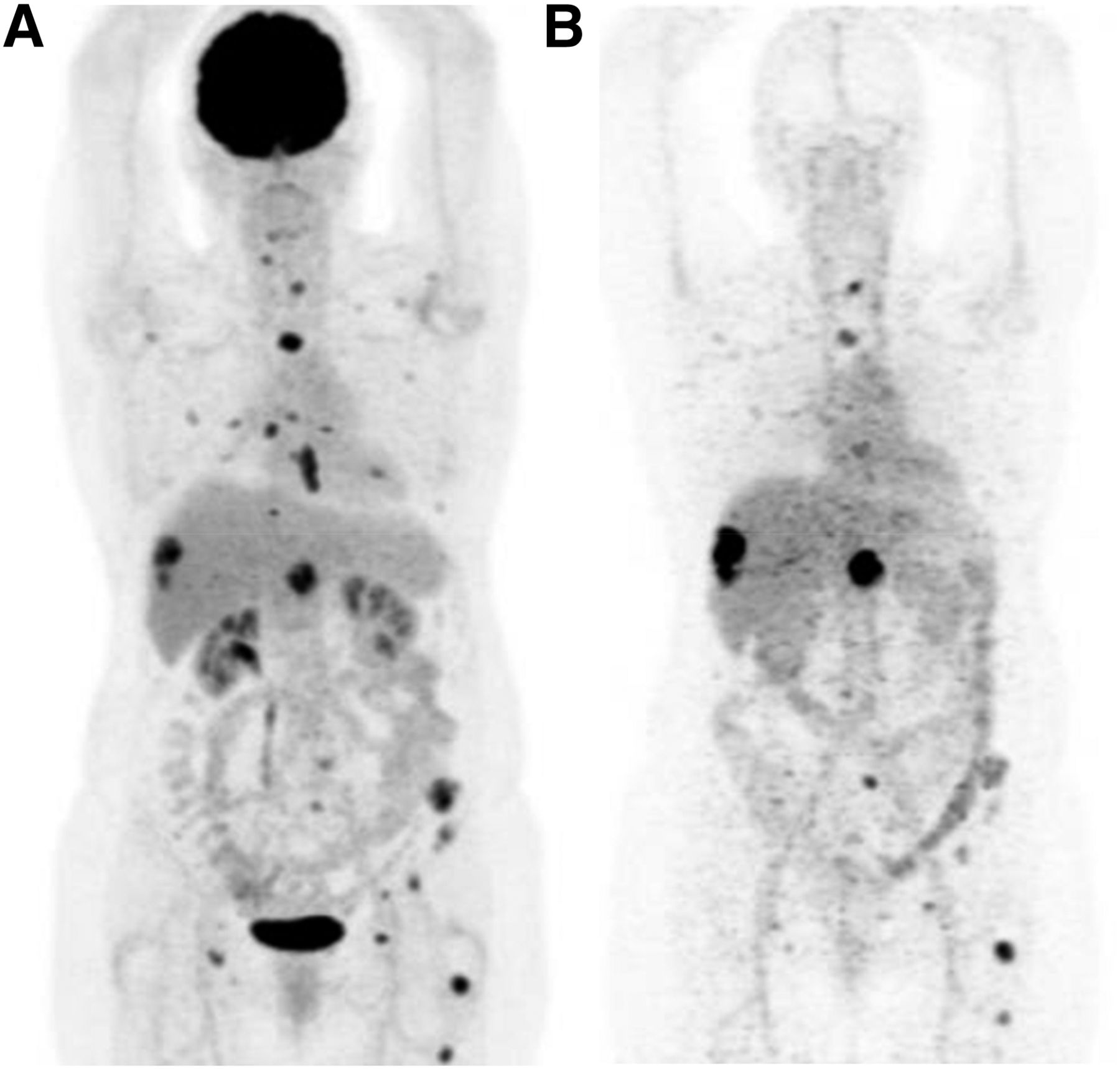
Representative molecular PET images of patient with HER2-positive breast cancer. Liver and bone metastases were visualized by 18F-FDG (A) and HER2 (B) imaging with 89Zr-trastuzumab, the latter illustrating high uptake in liver lesions and heterogeneous uptake in bone lesions.
NONSPECIFIC IMAGING (WITH 18F-FDG PET/CT) TO PREDICT PATHOLOGIC RESPONSE TO SYSTEMIC THERAPIES FOR EARLY HER2-POSITIVE BC
The use of 18F-FDG tumor uptake as a biomarker for predicting a pathologic response to neoadjuvant treatment has been explored in the preclinical and clinical settings, with conflicting results.
Preclinical Setting
Ex vivo results demonstrated that significant changes in 18F-FDG incorporation with trastuzumab therapy could be assessed (40). Furthermore, in vivo changes in 18F-FDG tumor uptake after therapy accurately differentiated responding and nonresponding human BC xenografts in athymic mice treated with trastuzumab (41). In contrast, in 2 other studies, 18F-FDG PET could not show an effect of trastuzumab treatment or of an HSP90 inhibitor in mice implanted with HER2-positive human BC tumors (40,42). Interestingly, Fleming et al. reported conflicting results in the same study and postulated that Akt inhibition and the glucose transport rate interfered with 18F-FDG incorporation and compromised the ability of 18F-FDG PET to measure treatment responses (43).
Clinical Setting
In women receiving systemic treatment for HER2-positive BC before surgery, the use of early 18F-FDG PET as a predictor of a pathologic complete response (pCR), a surrogate marker of disease-free survival and overall survival, was explored (44). Table 2 summarizes these studies, which were heterogeneous in terms of types of systemic therapies, timing of 18F-FDG PET, definition of pCR, and pCR rates. All studies but one (45) showed a correlation between early 18F-FDG PET/CT results and the probability of reaching a pCR. In the “negative” study, the cohort was small (only 25 patients), 18F-FDG PET/CT was performed 6–8 wk after the start of treatment with the chemotherapy–trastuzumab combination, and the axillary nodes were not evaluated.
18F-FDG PET/CT Studies Performed During Neoadjuvant Systemic Therapy to Predict pCR in HER2-Positive Breast Cancer
Among the “positive” studies, 2 studies opted for the evaluation of a metabolic response after 2 cycles of up-front anthracycline-based chemotherapy given as part of a sequential anthracycline–taxane–trastuzumab regimen (46,47). The other studies scheduled early 18F-FDG PET/CT up front after 1 or 2 cycles of a taxane- and trastuzumab-based combination (48–50).
Furthermore, the multicenter phase 3 Neoadjuvant Lapatinib or Trastuzumab Treatment Optimization (Neo-ALTTO) study was the only one that explored the predictive value of 18F-FDG PET/CT for dual anti-HER2 therapy given exclusively during a 6-wk “biologic window” and followed by the addition of paclitaxel (51).
The 18F-FDG PET/CT parameters found to correlate most strongly with a pCR were either the absolute residual SUVmax on early 18F-FDG PET/CT (46,49) or the change in the SUVmax threshold (47,48,50,51).
Of note, a multivariate analysis to assess the independent predictive value of early 18F-FDG PET/CT was performed in only 3 studies; the predictive value was confirmed in 2 studies (48,49). However, in the study conducted by our group (51), the hormone receptor status of the tumor was the most powerful predictor of a pCR. Furthermore, the study by Coudert et al. is of particular interest because it investigated the concept of a “response-adapted strategy”—escalating therapy with bevacizumab in patients showing a poor metabolic response on 18F-FDG PET/CT while receiving neoadjuvant trastuzumab and docetaxel (50). The authors demonstrated that the pCR rate was higher when bevacizumab was added than when the neoadjuvant therapy was unchanged.
Although the aforementioned studies reported encouraging results, the clinical utility of performing an early metabolic assessment during neoadjuvant therapy is far from being validated. The clinical utility of any biomarker assessment requires a demonstration that using the biomarker for treatment decision making improves clinical outcomes. Of note, such a demonstration is the last step of a challenging process of biomarker validation, which also comprises the demonstration of analytic and clinical validity (52).
Studies larger than the elegant study by Coudert et al. (50) will have to be performed and will involve the collaboration of several centers. Critical will be the use of common standardized PET imaging procedures like those developed by Boellaard et al. (53) for the validation of imaging biomarkers. Such multicenter prospective trials will need to explore and validate all or some of the different image-derived parameters extracted from sequential 18F-FDG PET and thought to be correlated with a pCR. Although a change in the SUVmax, a change in the SUVpeak, and the absolute residual SUVmax are the parameters most frequently used in studies of HER2-positive BC—mainly because of their reproducibility—other parameters, such as tumor lesion glycolysis, have also been assessed. A retrospective study (54) compared variations in the change in the SUVmax, the metabolically active tumor volume, and tumor lesion glycolysis at baseline and after 2 cycles of neoadjuvant chemotherapy (4 cycles of epirubicin plus cyclophosphamide followed by 4 cycles of docetaxel [plus trastuzumab in cases of HER2-positive BC]). The authors concluded that the change in tumor lesion glycolysis was the most accurate parameter for the prediction of a pCR, mainly in estrogen receptor–positive, HER2-negative tumors.
HER2 IMAGING TO PREDICT RESPONSE TO NEW ANTI-HER2 THERAPIES FOR ADVANCED HER2-POSITIVE BC
The first large prospective clinical study aimed at exploring HER2 imaging as a clinically useful predictive biomarker in advanced HER2-positive BC is the ZEPHIR study. This multicenter study of advanced HER2-positive BC (NCT01565200), which is a collaborative effort between Belgian and Dutch centers, aims to prospectively examine the role of pretreatment 89Zr-trastuzumab PET/CT (HER2 scan) and early 18F-FDG PET/CT (performed just before the second cycle of the antibody–drug conjugate [T-DM1]) in identifying lesions that will not respond to T-DM1. Preliminary data on the patient-based predictive abilities of these 2 PET scans, used alone or in combination, have been presented (55) and are promising. A high negative predictive value (100%) was found for 89Zr-trastuzumab PET results categorized as “negative” at baseline and an absence of a metabolic response on 18F-FDG PET/CT after one cycle of T-DM1. Furthermore, this study demonstrated that so-called advanced HER2-positive BC was a highly heterogeneous disease, with approximately one-third of patients showing the absence of HER2-specific targeting in all or most metastatic lesions.
Nonetheless, the determination of “negative” lesions must be made with great caution. False-negative results obtained for HER2 lesions by imaging have been described in patients with a high tumor load (56). This finding was seen in patients with 89Zr-trastuzumab uptake predominantly in the liver on the HER2 scan and subsequent rapid clearance of the tracer from the circulation. The reiteration of the HER2 scan in the presence of trastuzumab therapy resulted in improved pharmacokinetics and enabled better uptake of the tracer in bone lesions. The ZEPHIR study has been extended, with a requirement for biopsies for “HER2-negative” lesions, with the hope of confirming the initial encouraging results.
HER2-TARGETED THERAPY WITH RADIOACTIVE ANTI-HER2 PROBES
As previously mentioned, anti-HER2 probes have been successfully radiolabeled with various isotopes for diagnostic purposes—with SPECT and PET—as well as for targeted therapies.
Radioimmunotherapy (RIT) has been investigated predominantly and extensively with trastuzumab and therapeutic radionuclides, such as β-emitters 177Lu (57–60), 90Y (60,61), and 188Re (62,63); Auger electron emitter 111In (64); and even α-emitter actinium (12). All showed therapeutic efficacy in HER2-expressing xenografts. In addition, a combination of RIT and radiosensitizing chemotherapy was shown to potentiate the therapeutic effect of 212Pb-radiolabeled trastuzumab, resulting in prolonged median survival in HER2-positive xenograft models (65). RIT with 90Y-trastuzumab was even found to be applicable to BC expressing small amounts of HER2 (61). The results obtained with other candidates for RIT, such as the smaller Affibody molecules (66) and Nanobodies (177Lu (67) or 90Y (68)), have been encouraging. In addition, a first-in-human study assessing the safety of intraperitoneal α-RIT with 212Pb-TCMC-trastuzumab was presented recently. The latter approach showed an acceptable degree of early toxicity and absence of late toxicity (69).
CONCLUSION AND PERSPECTIVES
HER2 is an important target in the management of BC. Therefore, the assessment of HER2 is an essential step in the diagnostic workup and the selection of optimal treatments in both early-stage and metastatic settings. However, the heterogeneity of the disease, particularly in the metastatic setting, and the limited number of metastases that can be easily accessed for a biopsy remain issues of concern for the clinically available tests (IHC and FISH) with which HER2 status is determined.
Several anti-HER2 probes developed for both SPECT and PET have been proposed since the early 2000s as noninvasive approaches for assessing whole-body HER2 expression patterns, and some probes have successfully reached the clinical setting (Table 1). Small molecules—such as antibody fragments, Affibody molecules, and Nanobodies—offer the advantages of rapid uptake and clearance, uptake in tumors, and a low radiation burden for patients, thus enabling both early (1 h after administration) and serial HER2 imaging. In contrast, mAbs, with their slow clearance, allow for optimal imaging after several days at the cost of a higher radiation burden. Nonetheless, mAbs not only offer the advantage of identifying the presence of HER2 expression but also provide insight on mAb–target interactions, such as target availability or accessibility and complex internalization. These abilities are important for predicting responses to mAb-based treatments because accessibility is dependent on the size of the probe as well as the presence of the binding epitope on the target (14,70).
At present, predicting which type of HER2 tracer will be preferred in the clinical setting is difficult. We propose that the actual indication for HER2 imaging will dictate the choice of the imaging modality. For instance, low-molecular-weight probes could offer an alternative to IHC or FISH for diagnostic purposes or for the prediction of responses to treatment with small molecules (e.g., lapatinib, radiolabeled Nanobodies). In contrast, mAbs might be preferred when the intention is to treat with mAb-based therapies (e.g., trastuzumab, T-DM1, pertuzumab, radiolabeled mAbs). With regard to the recently introduced messenger RNA aptamers, further studies are needed, but these agents might be used to monitor treatment responses.
Of note is the fact that in preclinical models as well as in humans, the amount of protein or peptide influences the in vivo distribution pattern of the tracer (37,56,71). This fact was demonstrated in various studies in which increasing the nonradioactive probe content increased the contrast until a particular “threshold,” beyond which the contrast decreased, was reached. Therefore, the optimal amount of a probe, rather than the maximum obtainable specific activity, should be considered.
18F-FDG PET/CT has been used extensively in the neoadjuvant setting as an integrated biomarker to predict a pCR. Although the results have been encouraging, the next step is to establish its value as an integral biomarker that allows treatment deescalation or escalation on the basis of an early metabolic response/nonresponse or a poor response, respectively, as noted on 18F-FDG PET early after treatment initiation. Given the plethora of anti-HER2 agents that are currently clinically available and the lack of predictive tissue biomarkers beyond HER2, there is certainly a pressing need to demonstrate the clinical utility of noninvasive HER2 imaging or 18F-FDG PET/CT in advanced disease (e.g., helping to select a subset of patients who might most benefit or not benefit from a particular anti-HER2 therapy).
Molecular imaging has great potential to become a valuable tool in this new era of “personalized and precision medicine.” Important steps in adapting a new “image and treat” strategy in HER2-positive BC have already been accomplished. With additional prospective clinical studies and validation, molecular imaging in HER2-positive BC could allow patient-tailored dosage adaptation, with early cessation of futile (and expensive) therapies and deescalation of “aggressive” treatment, ultimately resulting in cost savings, lower morbidity, and improved patient outcomes.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 9, 2015.
- Accepted for publication October 9, 2015.





{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- IMAGING OF HER2 (TARGET) EXPRESSION
- NONSPECIFIC IMAGING (WITH 18F-FDG PET/CT) TO PREDICT PATHOLOGIC RESPONSE TO SYSTEMIC THERAPIES FOR EARLY HER2-POSITIVE BC
- HER2 IMAGING TO PREDICT RESPONSE TO NEW ANTI-HER2 THERAPIES FOR ADVANCED HER2-POSITIVE BC
- HER2-TARGETED THERAPY WITH RADIOACTIVE ANTI-HER2 PROBES
- CONCLUSION AND PERSPECTIVES
- DISCLOSURE
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Phase I Study of 99mTc-ADAPT6, a Scaffold Protein-Based Probe for Visualization of HER2 Expression in Breast Cancer
- Development of 64Cu-NOTA-Trastuzumab for HER2 Targeting: A Radiopharmaceutical with Improved Pharmacokinetics for Human Studies
- Radioiodinated Small-Molecule Tyrosine Kinase Inhibitor for HER2-Selective SPECT Imaging
- PET Imaging of Receptor Tyrosine Kinases in Cancer
- Preparation and In Vitro and In Vivo Characterization of the Tumor-specific Antigen-derived Peptide as a Potential Candidate for Targeting Human Epidermal Growth Factor Receptor 2-positive Breast Carcinomas
- SPECT/CT Imaging of the Novel HER2-Targeted Peptide Probe 99mTc-HYNIC-H6F in Breast Cancer Mouse Models
- Introduction and Overview