


Abstract
Many studies have pointed out the role of 18F-FDG PET/CT (or 18F-FDG PET) in patients with clinical stage III or II breast cancer. 18F-FDG PET/CT might advantageously replace other staging procedures, such as bone scanning and possibly contrast-enhanced CT of the thorax or abdomen–pelvis. We discuss the findings, locoregional or distant, that can be expected in different categories of breast cancer and their impact on prognosis and management. We also discuss the role of 18F-FDG PET/CT in restaging and how 18F-FDG PET/CT compares with conventional techniques in restaging for patients with suspected disease recurrence. We conclude with some recommendations for clinical practice and future research.
Accurate staging is important for management decisions in patients with newly diagnosed breast cancer. Several studies have pointed out the lack of utility of PET/CT with 18F-FDG in staging for patients with cancer detected early, that is, tumors of less than or equal to 2–3 cm and no palpable nodes—findings that represent most breast cancer cases (1–5). The lower sensitivity of 18F-FDG imaging than of the sentinel node technique in assessing axillary lymph node involvement is well known (1–3), and the risk of distant metastases in early-stage cases is low (4,5). These factors, combined with the good but finite specificity of 18F-FDG PET/CT, result in a relative abundance of false-positive findings and a paucity of true-positive findings; such findings lead to unwarranted patient anxiety and delay of care with the routine use of 18F-FDG PET/CT for breast cancer detected early.
In contrast, in such high-risk patients as those with inflammatory (T4d) or locally advanced breast cancer (LABC) (6,7), the role of 18F-FDG imaging in detecting distant lesions has been highlighted (8–12). Recently, several studies pointed out that staging with 18F-FDG PET/CT might be of value not only in patients with locally advanced disease but also in “intermediate-risk” patients (13–21)—that is, patients with clinical stage IIB disease (T2N1/T3N0) or higher—with significant diagnostic yield and prognostic information (18,19). PET/CT has also shown good performance in restaging for breast cancer patients (22–35).
This review assesses the advantages and limits of 18F-FDG PET/CT in initial staging and restaging for breast cancer patients.
REGIONAL AND DISTANT STAGING IN LOCALLY ADVANCED AND INFLAMMATORY BREAST CANCER
LABC is variably defined but usually refers to clinical N2, N3, or T4 disease and typically includes American Joint Committee on Cancer (AJCC) clinical stage IIIA (excluding T3N1), IIIB, and IIIC breast cancer (Table 1) (6,7). Within this entity, distinction is made between inflammatory carcinoma (T4d) and noninflammatory LABC. Patients without identified distant metastases usually receive neoadjuvant chemotherapy followed by surgery and radiation therapy as standard treatment.
TNM Clinical Stage Grouping for Breast Cancer*
Detection of Regional Node Involvement Outside Axillary Levels I and II
Axillary node clearance by axillary dissection is usually limited to levels I and II. 18F-FDG uptake suggesting involvement at level III (infraclavicular) or in extraaxillary locoregional nodes (supraclavicular or internal mammary) may have important implications in surgical management and the design of radiation therapy fields (7). Correlative CT information (from hybrid PET/CT imaging) is helpful in providing the anatomic location of 18F-FDG–avid lymph nodes (precise position relative to pectoralis minor muscle, clavicle, or intercostal space; Fig. 1) (36).

Invasive ductal carcinoma of right breast initially classified as T4cN0M0 (on basis of clinical examination, mammography, breast MRI, breast and axilla ultrasound, chest and abdominal CT scans, and bone scanning) in 63-y-old woman. PET/CT shows large breast tumor (SUVmax = 5.4) infiltrating skin and pectoral muscle (T4c) and depicts 18F-FDG–avid internal mammary node (SUVmax = 2.9) (final classification: T4cN2bM0).
Detection of Distant Metastases
LABC is associated with a high risk of distant metastases (Fig. 2 ). A pilot study by van der Hoeven et al. of 48 patients with LABC suggested that 18F-FDG PET was helpful in detecting distant metastases not seen with routine investigations (8). In a prospective cohort of 117 LABC patients (35 with inflammatory carcinoma and 82 with noninflammatory LABC), Groheux et al. compared a conventional staging approach routinely ordered by clinicians and including bone scanning, chest radiography (or dedicated CT), or liver ultrasound (or contrast-enhanced CT for abdomen–pelvis) with a single session of staging with 18F-FDG PET/CT (12). Distant metastases were detected on PET/CT in 43 patients (46% of patients with inflammatory LABC and 33% of those with noninflammatory LABC), whereas conventional imaging detected metastases in only 28 patients. 18F-FDG PET/CT outperformed conventional imaging for bone, distant lymph node, and liver metastases, whereas CT was more sensitive for lung metastases (12).

Invasive carcinoma of left breast classified as T3N2M0 (stage IIIA) before PET imaging in 62-y-old woman. PET/CT shows primary tumor (SUVmax = 7.3) and left axillary lymph node (SUVmax = 5.6), internal mammary lymph node (SUVmax = 2.1), and bone (SUVmax = 3.9) metastases. Classification after PET/CT was T3N3bM1 (stage IV).
PET efficiently detects supracentimetric pulmonary nodules. However, because of the partial-volume effect and respiratory movements, PET lacks sensitivity for smaller nodules. Careful scrutiny of CT images from PET/CT can reveal small nodules without 18F-FDG uptake. However, CT performed during free breathing is less efficient than standard diagnostic thoracic CT.
PET is more efficient than CT or bone scintigraphy for depicting lytic or mixed bone metastases and bone marrow lesions but can lack sensitivity for purely sclerotic bone metastases. However, although sclerotic metastases have no 18F-FDG uptake, they show osteocondensation on underlying CT images, so that they can be detected by hybrid PET/CT (36). A retrospective study comparing 18F-FDG PET/CT and bone scanning suggested a high concordance; it was rare for bone scintigraphy to diagnose bone involvement not identified by 18F-FDG PET/CT (37). These findings need confirmation in a prospective study but were significant enough to lead to the amendment of U.S. National Comprehensive Cancer Network (NCCN) guidelines to suggest that bone scintigraphy may not be necessary if both the PET and the CT components of 18F-FDG PET/CT that are used for staging are able to identify bony metastases (7).
In total, there is evidence that PET/CT can advantageously replace conventional imaging for examining extraaxillary nodes, chest, abdomen, and bone in a single session (12,17). PET/CT lacks sensitivity for brain metastases; patients at risk require dedicated imaging.
AT WHICH CLINICAL STAGE SHOULD 18F-FDG PET/CT BE INITIATED?
Between LABC and disease detected early (tumors of <2–3 cm; clinical N0), there are intermediate stages comprising large breast carcinomas or clinical N1 disease (stage IIA, stage IIB, and the T3N1 category of stage IIIA) (Table 2; Fig. 3). Early studies including both patients with stage II and patients with stage III breast carcinomas showed that PET/CT was helpful for detecting extraaxillary lymph node involvement and distant occult lesions (13–17). For example, Fuster et al. studied 60 consecutive patients with large breast cancers (>3 cm). Metastases missed by “conventional” work-up (chest contrast-enhanced CT, liver ultrasonography, and bone scans) were visualized by 18F-FDG PET/CT in 8 patients (14). However, the precise clinical stage at which PET/CT could be performed with favorably balanced cost-effectiveness remained unclear from these studies.
Studies Evaluating 18F-FDG PET/CT for Baseline Staging of Clinical Stage II or III Breast Cancer*

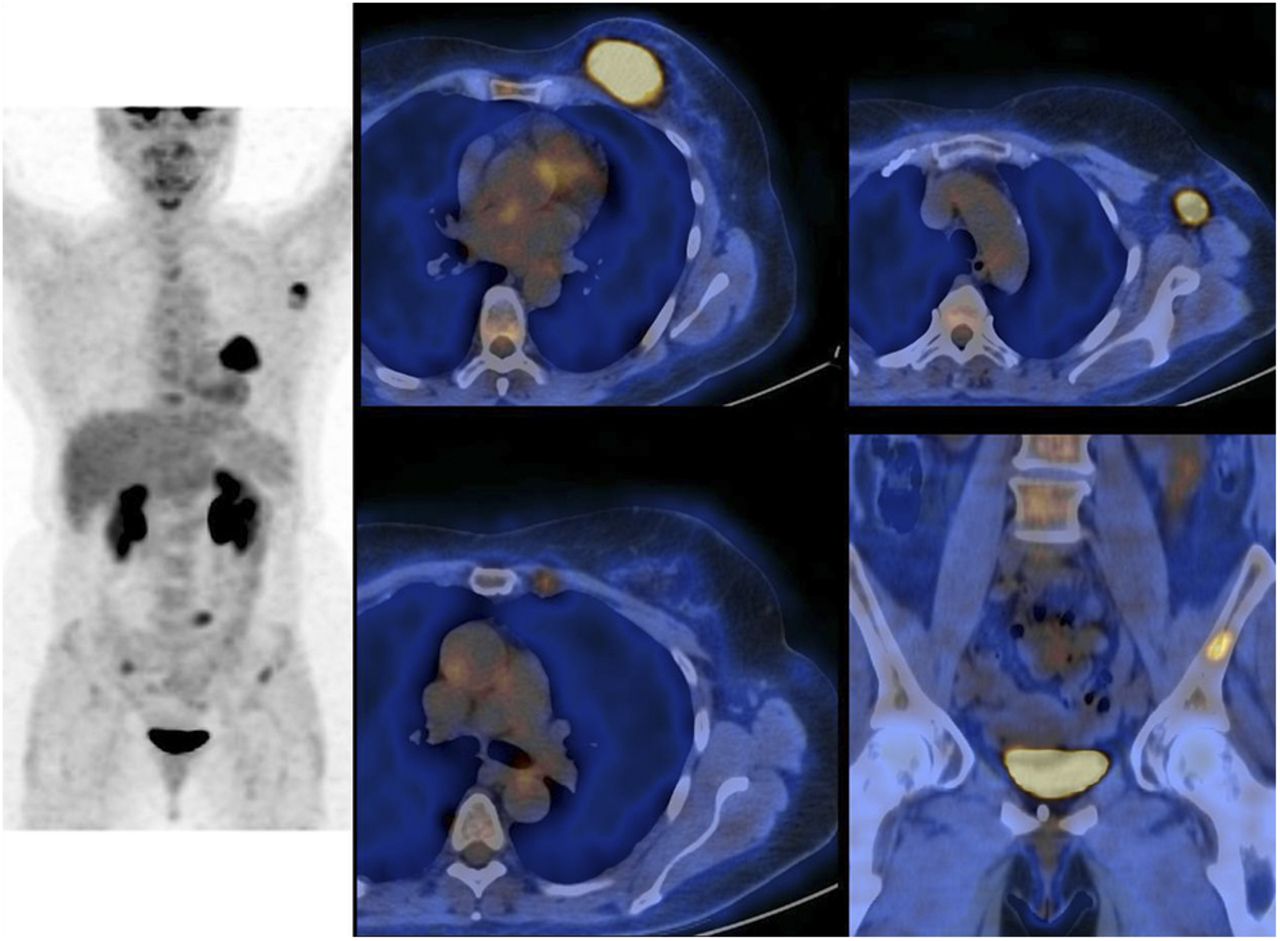
Bifocal invasive ductal carcinoma of left breast initially classified T3N0M0 (stage IIB) in 63-y-old woman. PET/CT shows 2 18F-FDG–avid foci in left breast (SUVmax = 9.6 and 6.4) and 3 18F-FDG–avid bone marrow foci in thoracic spine (T4, T5, and T6). Classification after PET/CT was T3N0M1 (stage IV).
More recently, Groheux et al. reported results from a prospective evaluation of 254 patients with breast cancers larger than 2 cm (18). The yield from 18F-FDG PET/CT imaging was examined in each of the specific subsets of patients with clinical stage IIA, IIB, IIIA, IIIB, or IIIC breast cancer (based on clinical examination, mammography, breast MRI, and locoregional ultrasonography). 18F-FDG PET/CT imaging changed the clinical stage in 77 patients (30.3%). It showed unsuspected N3 disease (infra- or supraclavicular or internal mammary nodes) in 40 patients and distant metastases in 53 patients. When the yield was examined by subsets, PET/CT revealed distant metastases in 2.3% of patients with clinical stage IIA disease (1/44), 10.7% of patients with stage IIB disease (6/56), 17.5% of patients with stage IIIA disease (11/63), 36.5% of patients with stage IIIB disease (27/74), and 47.1% of patients with stage IIIC disease (8/17). Stage IIIA was heterogeneous. The rate of distant metastases in patients with T3N1 disease (primary operable) was similar to that in patients with stage IIB disease (T2N1/T3N0). It was much higher in patients with N2 disease and was close to that found in patients with stage IIIB disease (18). Two other studies (1 including only breast cancer patients younger than 40 y) also showed that the yield from 18F-FDG PET/CT was high starting in patients with clinical stage IIB disease (16,20).
The results of these studies provide supportive evidence for a role of 18F-FDG PET/CT in determining the stage of disease for high- and intermediate-risk patients (clinical stage IIB or higher). Some breast oncology societies have changed their guideline recommendations to include these findings. However, practices differ according to countries. In the United States, current NCCN guidelines do not recommend the systematic use of 18F-FDG PET or PET/CT in breast cancer staging but state that “18F-FDG PET/CT may be helpful in identifying unsuspected regional nodal disease or distant metastases in LABC when used in addition to standard imaging studies” (7). In France, the National Cancer Institute recommends work-up for distant sites in the case of T3, T4, or N-positive disease (38); 18F-FDG PET/CT as a single procedure is an option (38).
PET/CT has no role in patients with clinical stage I breast cancer (clinically node-negative with breast tumors of ≤2 cm), which currently represents most newly diagnosed cases. These patients receive breast surgery with sentinel node biopsy (2). PET/CT cannot be used as a substitute for sentinel node biopsy because the spatial resolution of PET instruments precludes the detection of very small nodal metastases (1–5). The probability that 18F-FDG PET will detect extraaxillary regional node metastases or distant metastases in early-stage disease is low, and 18F-FDG imaging exposes women to false-positive findings. In a multicenter prospective study of 325 women with operable breast cancer, 18F-FDG PET (without the CT component) suggested distant metastases in 13 patients; metastatic disease was confirmed in 3 patients (0.9%), and the findings were false-positive in 10 patients (3.0%) (4). Therefore, the use of PET/CT in such patients is unjustified and exposes women to undue costs and additional anxiety and morbidity associated with false-positive diagnoses (39).
In the study by Groheux et al. (18), the overall yield from 18F-FDG PET/CT for stage IIA disease was only 4.5% unexpected findings (2.3% distant metastases and 2.3% extraaxillary nodes); these results challenge the use of 18F-FDG PET/CT for stage IIA disease. In that study, stage IIA was represented mainly by T2N0 disease (patients with T1N1 disease, as determined by positive sentinel node biopsy, were not included). These data require confirmation in larger studies.
SHOULD BREAST CANCER BIOLOGY, HISTOLOGY, AND PHENOTYPE BE CONSIDERED FOR BREAST CANCER STAGING?
18F-FDG uptake depends on the histologic and biologic characteristics of the breast tumor. Invasive ductal carcinoma exhibits higher uptake than invasive lobular carcinoma (40–42). Invasive tumors with Scarff-Bloom-Richardson grade 3 exhibit higher 18F-FDG uptake than lower-grade tumors (41,42). There is also a positive correlation between the tumor proliferation index (Ki-67 expression) and the intensity of 18F-FDG uptake (41). SUVs are higher in tumors that are negative for hormone receptors (41,42). Triple-negative breast cancer (TNBC; negative for estradiol and progesterone receptors and lacking human epidermal growth factor receptor 2 [HER2] overexpression) is usually highly 18F-FDG–avid (42,43).
Recent animal data showed that the molecular determinants of 18F-FDG uptake in breast cancer are complex and multifactorial (44). Awareness of the determinants of 18F-FDG uptake by oncologists and nuclear physicians is important because it may influence their clinical use of 18F-FDG PET/CT in breast cancer—based on the sensitivity with which they consider the modality to detect regional and distant disease spread—as well as their interpretation of the imaging results.
In the study by Riedl et al. (20), grade and receptor phenotype were found not to be related to distant metastases or extraaxillary lymphadenopathy. In the study by Groheux et al. (18), the rates of distant involvement did not differ according to grade or breast cancer phenotype. However, the sites of involvement differed. Patients with TNBC and HER2-positive disease had high proportions of extraskeletal metastases (18). N3 disease was more frequent in patients with grade 3 tumors, TNBC, or the HER2-positive phenotype.
Beyond the AJCC clinical stages, further studies are needed to evaluate the yield from PET/CT according to biomarkers of tumor aggressiveness. Given the high proportions of extraskeletal metastases in TNBC and HER2-positive breast cancer (18), the association of brain MRI with whole-body (WB) PET/CT should be evaluated for these subtypes. For lobular carcinoma, it is important that PET/CT interpretation be done with the knowledge that this histologic subtype has lower 18F-FDG uptake. Osteosclerotic bone lesions in a patient with lobular carcinoma should be considered suspect even when they are not 18F-FDG–avid (45).
PROGNOSTIC VALUE OF BASELINE 18F-FDG PET/CT
In the study by Groheux et al., among 189 patients with initial clinical stage IIB or higher and adequate follow-up, disease-specific survival was significantly shorter in the 47 patients found by 18F-FDG PET/CT to have M1 disease than in those with M0 disease (3-y disease-specific survival of 57% vs. 88%; P < 0.001) (18). In a recent publication, Cochet et al. also emphasized the prognostic value of 18F-FDG PET/CT for patients with clinical stage II or III disease (19).
Besides staging, the level of 18F-FDG uptake by a primary tumor also has prognostic value. High 18F-FDG uptake has been associated with a poorer outcome (10,46,47). Recently, high baseline tumor SUVmax and total lesion glycolysis were associated with shorter event-free survival in patients with estrogen receptor–positive/HER2-negative breast cancer (47).
PET/CT IN RESTAGING OF BREAST CARCINOMA
Early detection and precise characterization of the extent of recurrent disease are essential for guiding optimal therapy and prognostication. Locoregional recurrence may benefit from curative treatment based on surgery or radiation therapy, whereas distant metastases usually require palliative systemic therapy (31). Breast cancer recurrence can be suggested by clinical symptoms, radiologic findings, or rising levels of tumor markers (carcinoma antigen 15.3 or carcinoembryonic embryonic antigen). In all of these situations, the accuracy of PET/CT has been shown to be high (Table 3).
Studies Evaluating 18F-FDG PET/CT for Restaging
Because it allows better discrimination between posttreatment scar or fibrosis and viable tumor tissue, PET/CT is efficient for detecting locoregional recurrence (Fig. 4), especially in the chest wall, axilla, and extraaxillary lymph nodes basins, with better performance than CT or MRI (26–28). In the study by Schmidt et al., PET/CT was found to be more sensitive than WB MRI for the detection of lymph node involvement (n = 21 vs. n = 16); however, WB MRI was slightly more sensitive (n = 154 vs. n = 147) for the detection of distant metastases (26). Two metaanalyses compared 18F-FDG PET/CT, conventional imaging (ultrasonography, CT, and bone scintigraphy), and MRI for the detection of breast cancer recurrence (48,49). PET/CT outperformed PET alone and conventional imaging but not MRI. Compared with conventional imaging, PET/CT provides better prognostic stratification by discriminating patients with locoregional recurrence only from those with distant recurrence (30,34,35) and is helpful for downstaging suspected lesions in some situations (34,50).

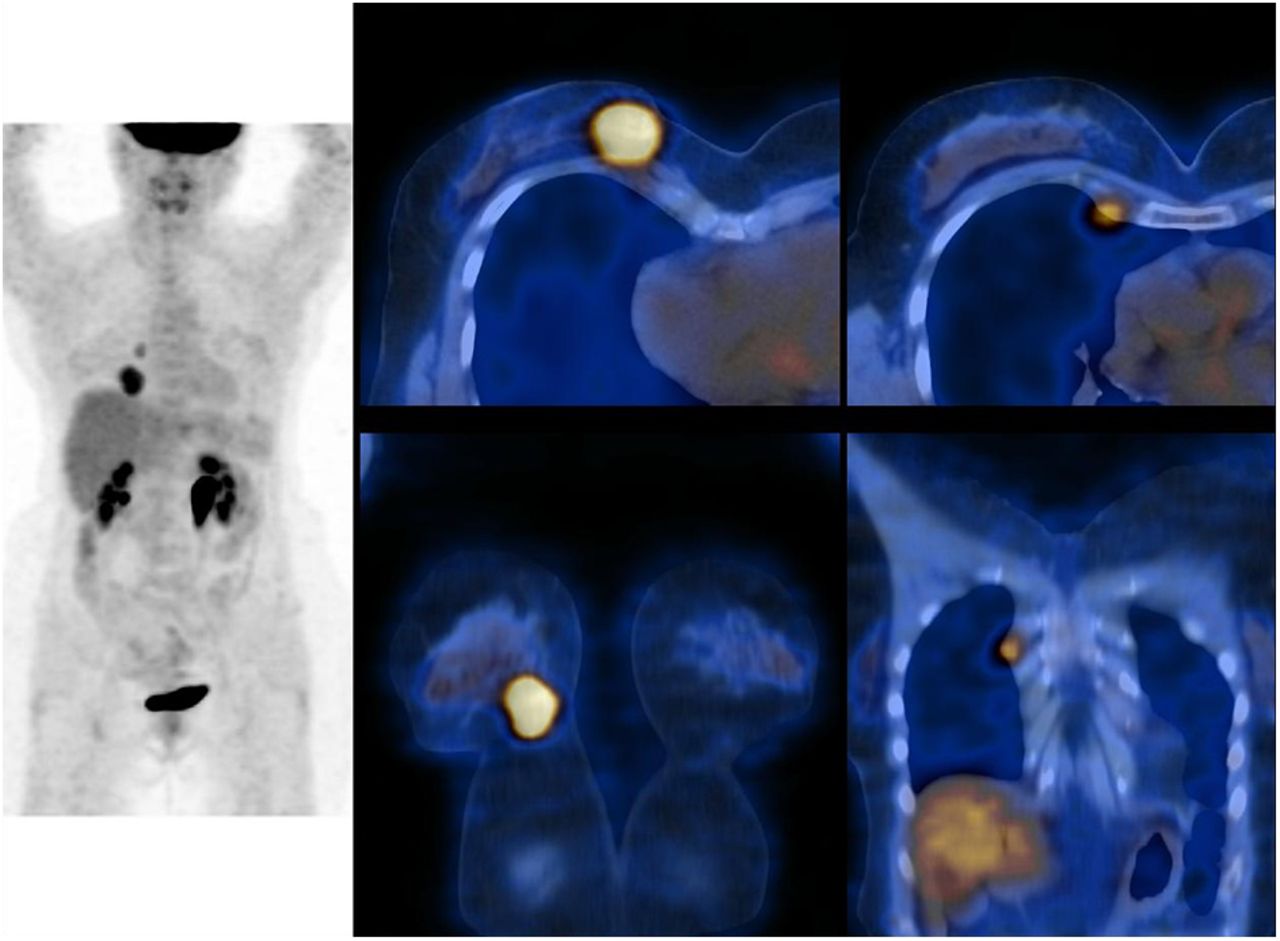
TNBC in left breast initially classified as T3N1M0 and treated with neoadjuvant chemotherapy, conservative surgery, and locoregional radiotherapy in 50-y-old woman. Eight months after end of radiotherapy, patient had moderate pain in left chest wall, and ultrasound of axilla showed suspected lesion. PET/CT revealed highly 18F-FDG–avid left interpectoral lymph node (11.2 mm; SUV = 9.4; arrow) but no other abnormal uptake. Biopsy confirmed this isolated locoregional recurrence of TNBC.
In the specific setting of asymptomatic patients with rising tumor marker levels and negative conventional imaging results, PET/CT has shown strength in detecting recurrence earlier than traditional imaging (29–31,35,51). In a metaanalysis of 13 studies, the sensitivity, specificity, and accuracy of PET were 87.8%, 69.3%, and 82.8%, respectively (51). PET/CT is also efficient in patients with suspected recurrence but negative tumor marker results (52).
Including 18F-FDG PET/CT in the diagnostic algorithm for breast cancer relapse has a major influence on management; after PET/CT, management was modified in 48%–57% of patients with suspected relapse (23,28–31,33,34). This impact could be even higher with the development of local control strategies for oligometastatic disease, such as surgery or stereotactic radiotherapy (53,54). Among patients with evidence of distant relapse, PET/CT may identify oligometastatic status in a significant proportion (35).
Most studies have retrospectively evaluated the incremental role of 18F-FDG PET/CT, in addition to conventional methods, in the diagnostic work-up of breast cancer relapse. Uncertainty remains about its utility as a replacement for conventional work-up rather than as an adjunct to conventional imaging (49). The potential roles of combined PET and whole-body MRI and contrast-enhanced PET/MRI are being investigated (55).
Although PET/CT offers the opportunity to provide an overview of disease in a single procedure (22–35), its use as a first-line method is not recommended in international guidelines. NCCN guidelines recommend that chest CT, abdominopelvic CT or MRI, and bone scanning be performed first; 18F-FDG PET/CT is considered optional and “most helpful in situations where standard staging studies are equivocal or suspicious” (7). The European Society for Medical Oncology recommends that “18F-FDG PET/CT can be useful for identifying the site of relapse when traditional methods are equivocal or conflicting” (56).
With regard to surveillance, American Society of Clinical Oncology and NCCN guidelines recommend only regular history, physical examination, and mammography for breast cancer routine follow-up (7,57). Systematic 18F-FDG PET/CT is not indicated. In a recent study, Chang et al. described a change in planned management in 10% of patients receiving PET/CT for routine follow-up without suspected relapse before imaging (33). The role of systematic PET/CT examination in subgroups of patients with a high risk of early relapse should be analyzed in a multicenter prospective study. One such subgroup could be patients who have TNBC but for whom a complete pathologic response was not achieved after neoadjuvant chemotherapy. Of 51 patients with TNBC who had no distant metastases at baseline PET but had residual disease after neoadjuvant chemotherapy, 21 experienced a relapse within a few years (17 developed distant metastases) (52).
CONCLUSION
18F-FDG PET/CT is useful for staging locally advanced and inflammatory breast cancer. One advantage of 18F-FDG PET/CT over conventional imaging is that it allows the examination of extraaxillary nodes as well as the chest, abdomen, and bone in a single session. The yield from PET/CT is also substantial in patients with clinical stage IIB (T2N1 and T3N0) and primary operable stage IIIA (T3N1) breast carcinomas; further studies with cost-effectiveness assessments would be helpful. PET is definitely not recommended for the initial assessment of patients with clinical T1N0 breast cancer.
18F-FDG PET/CT is also useful for detecting recurrence and for restaging in breast cancer patients by providing incremental information that can influence management and refine prognostic stratification. Randomized trials comparing 18F-FDG PET/CT and conventional imaging as initial restaging procedures are needed. The interest in 18F-FDG PET/CT will increase with the development of local control strategies for oligometastatic disease.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 29, 2015.
- Accepted for publication September 2, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- REGIONAL AND DISTANT STAGING IN LOCALLY ADVANCED AND INFLAMMATORY BREAST CANCER
- AT WHICH CLINICAL STAGE SHOULD 18F-FDG PET/CT BE INITIATED?
- SHOULD BREAST CANCER BIOLOGY, HISTOLOGY, AND PHENOTYPE BE CONSIDERED FOR BREAST CANCER STAGING?
- PROGNOSTIC VALUE OF BASELINE 18F-FDG PET/CT
- PET/CT IN RESTAGING OF BREAST CARCINOMA
- CONCLUSION
- DISCLOSURE
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Prognostic Implications of 68Ga-FAPI-46 PET/CT-Derived Parameters on Overall Survival in Various Types of Solid Tumors
- 18F-PFPN PET: A New and Attractive Imaging Modality for Patients with Malignant Melanoma
- Weight-Based Protocols Offer Significant Reduction in Radiation Dose Without Affecting PET-CT Image Quality
- PET-CT for Evaluating Breast Cancer Yields Incidental Finding in the Lung
- Assessing 18F-FDG Uptake in the Sentinel Lymph Node in Breast Cancer
- Interplay between ShcA Signaling and PGC-1{alpha} Triggers Targetable Metabolic Vulnerabilities in Breast Cancer
- Introduction and Overview