


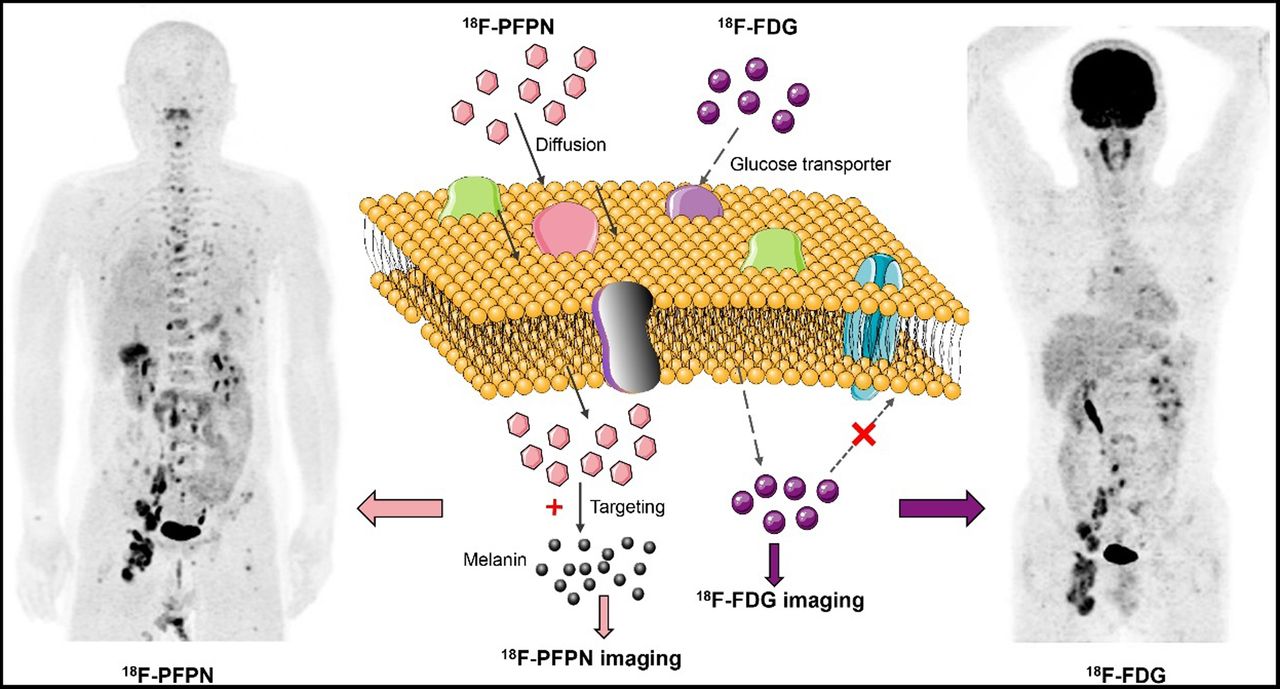
Visual Abstract
Abstract
18F-FDG PET has limited diagnostic applications in malignant melanoma (MM). 18F-N-(2-(diethylamino)ethyl)-5-(2-(2-(2-fluoroethoxy)ethoxy)ethoxy)picolinamide (18F-PFPN) is a novel PET probe with high affinity and selectivity for melanin. We conducted a clinical study with 2 aims, first to investigate the biodistribution and radiation dosimetry of 18F-PFPN in healthy volunteers, and second, to examine the diagnostic utility of 18F-PFPN PET imaging in patients with MM. Methods: 18F-PFPN was synthesized through a fluoro-for-tosyl exchange reaction. Five healthy volunteers were enrolled to investigate the biodistribution, pharmacokinetics, radiation dosimetry, and safety of the tracer. Subsequently, a total of 21 patients with clinically suspected or confirmed MM underwent both 18F-PFPN PET/MRI and 18F-FDG PET/CT scans. The normalized SUVmax of selected lesions was determined for both tracers and compared in patient- and lesion-based analyses. Results: 18F-PFPN has an elevated radiochemical yield and was highly stable in vivo. In healthy volunteers, 18F-PFPN was safe and well tolerated, and its effective absorbed dose was comparable to that of 18F-FDG. In patient-based analysis, 18F-PFPN uptake was higher than 18F-FDG for both primary tumors and nodal metastases. In lesion-based analysis,18F-PFPN PET imaging could detect 365 metastases that were missed on 18F-FDG PET. Additionally, 18F-PFPN PET imaging had clinical value in distinguishing false-positive lesions on 18F-FDG PET. Conclusion: 18F-PFPN is a safe and well-tolerated melanin PET tracer. In a pilot clinical study, 18F-PFPN PET imaging outperformed traditional 18F-FDG PET in identifying both primary MM and its distant spread.
Malignant melanoma (MM) is a highly aggressive tumor that poses a significant public health burden (1). The 5-y overall survival rates of patients with nodal and distant spread are as low as 65% and 25%, respectively. However, early surgical excision of localized MM portends favorable outcomes (5-y overall survival, 98%). In this scenario, both prompt diagnosis and accurate disease staging are paramount to reduce mortality.
Traditional 18F-FDG PET may be clinically useful for staging and therapeutic monitoring of advanced (stage III−IV) MM (2). However, the value of 18F-FDG PET imaging in this malignancy is limited by uptake in the liver and brain (3), which may ultimately compromise reliable detection of primary or metastatic melanoma lesions at these anatomic sites. Additionally, 18F-FDG PET does not have sufficient sensitivity to diagnose stage I−II MM (4) and is generally unable to identify small (<1 cm) metastases to the lung, liver, and brain (5).
Recent advances in specific PET tracers, including MM-selective antibodies (6,7), α-melanocyte–stimulating hormone receptor ligands (5,8), and peptides (9,10), have fostered our ability to identify MM lesions. Unfortunately, several caveats, including slow and limited tumor uptake, suboptimal in vivo stability, and elevated liver accumulation, still hamper their routine clinical application. One of the most promising molecular targets for the imaging of MM is melanin, which exists in most melanomas (>90%) (11). Several melanin-targeted radiopharmaceuticals, including 123I-MEL008 (12), 18F-FBZA (13), 18F-MEL050 (14), and 4-11C-MBZA (15), have been synthesized from benzamide, quinoxaline, or picolinamide and applied as PET and SPECT tracers. We have previously designed and synthesized an 18F-labeled benzamide analog as a melanin-imaging tracer, termed 18F-5-fluoro-N-(2-[diethylamino]ethyl)picolinamide (18F-5-FPN). This probe, characterized by high melanin affinity and favorable pharmacokinetic properties (16,17), has shown promising preclinical value for the identification of small (<2 mm) nodal and distant metastases from MM in mice (18). However, the relatively elevated hepatic tracer uptake of 18F-5-FPN hindered its clinical applications. Subsequently, we optimized this probe to have a higher tumor–to–normal-liver ratio and radiochemical yield, named 18F-N-(2-(diethylamino)ethyl)-5-(2-(2-(2-fluoroethoxy)ethoxy)ethoxy)picolinamide (18F-PFPN) (19).
To shed further light on the translational value of 18F-PFPN as a melanin-targeted PET probe for MM imaging, we designed the current study with 2 principal aims. First, we sought to investigate the biodistribution and radiation dosimetry of 18F-PFPN in healthy volunteers. Second, we examined, for the first time, the clinical utility of 18F-PFPN PET imaging in patients with suspected or pathologically confirmed MM.
MATERIALS AND METHODS
Healthy Volunteers and Patients
The institutional review board approved this study, and all subjects gave written informed consent. Five healthy volunteers (3 women and 2 men; age range, 28–48 y; Supplemental Table 1 [supplemental materials are available at http://jnm.snmjournals.org]) were enrolled to investigate the biodistribution, pharmacokinetics, radiation dosimetry, and safety of 18F-PFPN. Between January 19, 2021, and June 19, 2021, the patients with clinically suspected or confirmed MM were recruited. All patients underwent 18F-FDG PET/CT and 18F-PFPN PET/MRI within 1 wk. CT was performed when MRI was contraindicated (1 patient because of a metal implant). Patients with acute systemic diseases, electrolyte disorders, other known malignancies, an age of less than 18 y, or pregnancy or lactation were then excluded.
Biodistribution and Radiation Dosimetry of 18F-PFPN in Healthy Volunteers
18F-PFPN was synthesized using the procedural steps outlined in Supplemental Figure 1 (19). The procedures for determining the tracer biodistribution and the radiation dosimetry are described in Supplemental Figure 2. In healthy volunteers, serial whole-body PET/MRI scans were subsequently acquired on an integrated PET/MRI scanner (Signa; GE Healthcare) at 30, 60, 120, and 240 min after tracer injection. At each time point, images were acquired immediately after collection of biologic specimens (blood and urine). The tracer uptake in each major organ was determined by calculating the SUVmean. The pharmacokinetic profile of 18F-PFPN was investigated by determining the radioactive count of blood, plasma samples, and urine specimens collected at different time points using an automatic well-type automatic γ-counter (WIZARD 2470; PerkinElmer). The absorbed radiation dose for each major organ was calculated using the OLINDA/EXM software, version 2.1. The healthy volunteers were asked to report any subjective abnormality within 1 h from the completion of the study procedures. Vital signs were determined in the preprocedural phase and 4 h after tracer injection.
PET Imaging in Patients with Suspected or Pathologically Confirmed MM
18F-PFPN PET/MR images were acquired approximately 1 and 3 h after the intravenous injection of 18F-PFPN (dose, 3.0–5.4 MBq/kg). 18F-FDG PET/CT images were acquired approximately 60 min after the intravenous injection of 18F-FDG (dose, 3.7–5.4 MBq/kg). All scans were from the brain to the upper thigh (or the foot when required).
Image Interpretation
Images were uploaded on an Advantage Workstation (version AW4.6; GE Healthcare) for registration, fusion, and interpretation. 18F-PFPN and 18F-FDG PET images were independently reviewed by 2 experienced nuclear medicine physicians who were not aware of patient clinical data and conventional imaging results. All discrepancies were resolved by consensus.
Regions of interest were drawn on transaxial slices, and the raw SUVmax was automatically calculated to quantify 18F-FDG and 18F-PFPN uptake within each lesion. To improve the comparability of SUVmax, raw data were normalized using the following formula: where SUVbkgd indicates the SUVmean of the descending aorta.
where SUVbkgd indicates the SUVmean of the descending aorta.
Both patient- and lesion-based quantitative assessments were performed. Patient-based analysis included either the primary tumor or the single lesion showing the highest tracer uptake at each metastatic site. Lesion-based analysis for each site was performed either on all lesions (when their count was ≤10) or the 10 lesions that showed the highest tracer uptake (when their count was >10). A visual scoring system was also applied and is described in the supplemental materials.
Statistical Analysis
Continuous variables are presented as means ± SD. SUVmax was compared between groups using the Student t test. Categoric variables were compared using the χ2 test. All analyses were undertaken in SPSS, version 22 (IBM). Two-tailed P values of less than 0.05 were considered statistically significant.
RESULTS
Quality Control and Radiochemistry of the 18F-PFPN Tracer
18F-PFPN was successfully synthesized. The radiochemical purity and specific activity of 18F-PFPN (n = 5) was 97.38% ± 1.99% and 101–165 GBq/mmol, respectively. This probe’s in vivo stability measured at 4 h after injection was more than 95%. An illustrative high-performance liquid chromatography image of the tracer in the urine is shown in Supplemental Figure 3.
Biodistribution, Dosimetry, and Safety of 18F-PFPN in Healthy Volunteers
For healthy volunteers, the 18F-PFPN maximum-intensity-projection images are shown in Figure 1. 18F-PFPN uptake was visible in the renal pelvis and calices, ureters, gallbladder, urinary bladder, stomach, and liver. Hepatic SUVmean decreased over time, being 4.51 ± 0.75, 3.26 ± 0.62, 2.45 ± 0.40, and 1.74 ± 0.28 at 30, 60, 120, and 240 min after injection, respectively (Supplemental Fig. 4). A similar pattern was observed for blood uptake, which gradually decreased from (2.65 ± 0.20) × 10−3 percentage injected dose [%ID]/g at 30 min after injection to (1.35 ± 0.67) × 10−3 %ID/g at 240 min (Supplemental Fig. 5). Comparable results were evident for most organs, except the gallbladder, eyes, and urine. The tracer activity in the urine was 0.15 ± 0.05 %ID/g at 30 min after injection and reached a peak of 0.35 ± 0.14 %ID/g at 60 min, suggesting rapid renal clearance. Concerning the eyes, we observed an SUVmean increase from 0.79 ± 0.07 at 30 min after injection to 1.32 ± 0.30 at 240 min due to the presence of choroidal melanocytes and retinal pigment cells.

Maximum-intensity-projection PET images obtained from female and male volunteers at different time points after intravenous 18F-PFPN injection.
The estimated absorbed-radiation dosimetry for different organs is depicted in Supplemental Table. 2. The urinary bladder wall showed the highest dose activity (1.73 × 10−1 mSv/MBq), followed by the kidneys. A mean absorbed dose of 7.37 × 10−3 mSv/MBq was observed in the eyes. The total effective dose was 2.01 × 10−2 mSv/MBq.
Neither immediate adverse reactions nor significant changes in vital signs were observed after tracer injection. Similarly, follow-up laboratory examinations did not reveal any abnormal changes in liver and kidney function tests.
Characteristics of Patients with MM
In total, 21 patients (mean age, 54.86 ± 11.58 y) with clinically suspected or confirmed MM were included in the study (Table 1). Nine patients underwent imaging for initial disease staging, whereas investigations in the remaining 12 were aimed at detecting recurrences. Most primary MMs were in the skin, followed by choroid membranes. One patient had an occult primary MM located in the rectum.
General Characteristics of Patients with Clinically Suspected or Confirmed MM
Comparison of 18F-PFPN and 18F-FDG PET Imaging in Patients with MM
We subsequently compared 18F-PFPN and 18F-FDG PET imaging in MM patients (Table 2; Fig. 2). 18F-PFPN PET could clearly delineate lesions, with an excellent contrast due to low background uptake, especially in the brain and liver. On a patient-based analysis, both 18F-PFPN and 18F-FDG PET showed the same diagnostic performance (100%) for the detection of primary lesions; in addition, these 2 techniques performed similarly for identifying metastases (100.00% vs. 94.44% in lymph nodes, 100.00% vs. 87.50% in bone, 100.00% vs. 71.43% in liver, 100.00% vs. 66.67% in other sites, respectively). Significant differences were observed between SUVmax for 18F-PFPN and SUVmax for 18F-FDG measured at 1 and 3 h for both primary lesions (P = 0.022 and 0.008, respectively) and lymph node metastases (P = 0.043 and 0.005, respectively), with the former tracer showing the higher uptake.
Patient- and Lesion-Based Analyses of 18F-PFPN and 18F-FDG PET Imaging Findings

Representative images of patients with MM who underwent 18F-PFPN and 18F-FDG PET scans for disease staging. 18F-PFPN PET outperformed traditional 18F-FDG PET for identifying both primary tumors and distant metastases. Blue arrows indicate primary lesions, whereas yellow arrowheads denote lymph node metastases.
On a lesion-based analysis, 18F-PFPN PET/MRI detected a higher number of lesions than did 18F-FDG PET (365 additional lesions); the detection rates according to the anatomic distribution were as follows: lymph nodes (100.00% vs. 79.03%, respectively), bone (100.00% vs. 38.32%, respectively), liver (100.00% vs. 34.75%, respectively), and other sites (100.00% vs. 87.88%, respectively). The SUVmax for 18F-PFPN in the primary lesions, as well as in nodal, bone, and hepatic metastases, significantly increased from 1 to 3 h after injection (P < 0.05); conversely, a significant decrease was observed for most tissues and organs. A similar increase in normalized SUVmax for 18F-PFPN was evident between 1 and 3 h. Notably, normalized SUVmax for18F-PFPN at 3 h was higher than that for 18F-FDG for most lesions (P < 0.01). The original SUVmax data are shown in Supplemental Table 3.
On the visual scoring system (Fig. 3), 18F-PFPN outperformed 18F-FDG for the detection of distant metastases to the liver (10′ vs. 0′), bone (8′ vs. 0′), other distant sites (3′ vs. 0′) and lymph nodes (8′ vs. 0′). The total scores for 18F-PFPN and 18F-FDG PET were 29′ and 0′, respectively.

Comparative findings obtained from visual assessment of 18F-PFPN and 18F-FDG PET images. LM = liver metastases; BM = bone metastases; LNM = lymph node metastases. n (%) in each bar refers to patient number (patient number as a percentage of the total population).
Illustrative Case Reports
A 47-y-old man (patient 8, Fig. 4) underwent 18F-PFPN PET for the detection of MM recurrences. 18F-PFPN PET identified more lesions than 18F-FDG PET did (fold-change in lesion detection for 18F-PFPN PET: 2-fold higher for nodal metastases, 3-fold higher for hepatic metastases, and 2.5-fold higher for bone metastases). Notably, 18F-PFPN PET successfully detected lesions smaller than 2 mm.

A 47-y-old man who underwent surgical removal of choroidal MM 19 mo before imaging. On maximum-intensity-projection (MIP) images, 18F-PFPN PET (A) was able to identify higher number of lesions (blue arrowheads) than 18F-FDG PET could (B). 18F-PFPN PET/MRI identified hyperintense T1-weighted focus of increased tracer uptake in left arm (SUVmax, 8.4; red arrows) and left femur (SUVmax, 6.8; <2 mm, green arrows), which had normal uptake and density on 18F-FDG PET/CT images.
In patient 16 (Fig. 5), high background activity caused by elevated physiologic tracer uptake in the brain prevented the identification of cerebral metastases on 18F-FDG PET imaging; however, the lesions were clearly visible on 18F-PFPN PET images. Besides, MRI sequences provided diagnostic confirmation.

A 63-y-old man who underwent surgical removal of plantar melanoma 2 y before PET imaging. (A) Craniocerebral 18F-PFPN PET/MRI revealed avid tracer uptake in left parietal lobe (SUVmax, 1.8; red arrows) and right cerebellum (SUVmax, 4.3; green arrows). (B) Conversely, no malignant lesions were visible on 18F-FDG PET; notably, these images were characterized by high background activity caused by elevated physiologic tracer uptake in brain.
In patient 3 (Fig. 6), 18F-PFPN PET, but not 18F-FDG PET, correctly identified the primary lesion located in the left foot as an early-stage melanoma. Interestingly, the cervical lymph nodes showed intense 18F-FDG uptake, whereas there was no 18F-PFPN accumulation in these areas. The follow-up results suggested the findings to be inflammatory but not metastasis lesions and false-positive on 18F-FDG PET.

A 40-y-old man who sought medical attention for growing pigmented lesion on arch of left foot. 18F-FDG PET images (A and B) revealed mild tracer accumulations in left anterior arch (red circle and red arrows; SUVmax, 3.3) and lateral margin of right foot (blue circle and blue arrows; SUVmax, 2.7). 18F-PFPN PET clearly delineated left-foot lesion, which showed avid tracer uptake (SUVmax, 5.0), but 18F-PFPN PET did not identify any lesion in right foot. Results of pathologic examination identified left-foot lesion as nodular ulcerated MM (thickness, 1.2 mm; pathologic T stage, pT2b). Interestingly, there was intense 18F-FDG uptake in cervical lymph nodes (C, green arrows: SUVmax, 3.0–12.6), which, however, did not show significant 18F-PFPN uptake. Collectively, these findings ruled out possibility that these lesions were metastases from MM; 18F-FDG PET–positive nodes likely had reactive inflammatory nature.
Figure 7 shows an illustrative case of 18F-PFPN PET and 18F-FDG PET findings in a woman with distant amelanotic lesions from MM. Melanoma cells unable to produce melanin were missed on 18F-PFPN PET, which further confirmed the specificity of 18F-PFPN as a melanin PET tracer.

A 51-y-old woman who underwent partial excision of MM in left breast 1 y before PET imaging. She was regularly followed up; marked increase in serum CA 19-9 level (>1,200 U/mL; reference range, 0–35 U/mL) was evident over last 4 mo. (A) On 18F-FDG PET imaging, avid tracer uptake was evident in operated breast (SUVmax, 3.7–10.4), axillary lymph nodes (SUVmax, 3.8–9.6), and bone (SUVmax, 3.2–10.2), indicating recurrent disease. Unexpectedly, 18F-PFPN PET imaging findings were negative. (B) Visual examination of operated breast showed nonpigmented recurrent lesions. Pathology examination (hematoxylin and eosin [H&E] staining) of axillary lymph nodes identified metastases from MM; however, these metastatic cells were proven to be nonpigmented (unable to produce melanin). Red arrows indicate breast lesion.
DISCUSSION
There are 2 principal findings from this study. First, on analyzing the biodistribution, pharmacokinetics, radiation dosimetry, and safety of 18F-PFPN in 5 healthy volunteers, we found that this melanin PET tracer was safe and well tolerated; also, its absorbed radiation dose was comparable to 18F-FDG. Second, in a pilot clinical investigation on suspected or confirmed MM patients, 18F-PFPN showed higher uptake than 18F-FDG for both primary tumors and distant metastases. In a lesion-based analysis,18F-PFPN PET imaging could detect 365 metastases that were missed on 18F-FDG PET. Collectively, these data represent a promising step in understanding the clinical value of 18F-PFPN PET imaging for diagnosing and detecting disease recurrences in MM.
Although 18F-FDG PET imaging has extensive applications in patients with solid malignancies (20), its clinical value in MM is beset by high false-positive rates (100% in early-stage MM) (21). In this scenario, there have been increasing efforts to develop novel PET tracers capable of recognizing and binding to melanin with high affinity and specificity. The melanin PET tracer used in this study (18F-PFPN) was optimized and improved on the basis of our previous nicotinamide probe, 18F-5-FPN (17). Compared with the parent molecule, 18F-PFPN is characterized by a more favorable pharmacokinetic profile—importantly, the negligible hepatic accumulation and rapid renal clearance (19)—thus endowing this tracer with the capacity to be safely applied for clinical imaging studies.
However, partial excretion may occur through the hepatobiliary system, which may at least in part account for both gallbladder and intestinal wall uptake. On another note, the annular tracer accumulation in the eyes can be explained by the presence of choroidal melanocytes and retinal pigment cells. In terms of radiation safety, the total effective dose of 18F-PFPN was 0.020 mSv/MBq, which is comparable to the whole-body effective dose of 18F-FDG (0.019 mSv/MBq) (22). Collectively, these results prompted us to conduct the first clinical 18F-PFPN PET imaging study in patients with MM.
First, on analyzing diagnostic performance for the detection of primary MM, we found that 18F-PFPN PET could identify early T-stage lesions (e.g., T2b). Additionally, significant differences were observed between SUVmax for 18F-PFPN and SUVmax for 18F-FDG measured at 3 h for primary lesions, with the former tracer showing the highest uptake (3.92-fold higher uptake than that of 18F-FDG). In view of these findings, we subsequently examined the role of 18F-PFPN PET imaging to identify distant metastases. Although the results of 18F-PFPN PET imaging led to modifications in disease staging for one patient only (1/9), this may be related to the high proportion of patients with advanced disease stages. Interestingly, 18F-PFPN showed low background activity, ultimately allowing reliable delineation of a higher number of distant lesions from MM, including those at nodal, bone, and hepatic sites. Pigmented lesions can appear hyperintense on T1-weighted MR images because of the high number of negative melanin charges, which ultimately facilitate iron binding. In this scenario, the combination of 18F-PFPN PET with MRI can increase image interpretation accuracy. Immune checkpoint inhibitions could enhance immune cells to kill tumors, which had been one of the main treatments for metastatic melanoma (23). 18F-PFPN may provide an excellent possibility to distinguish between inflammatory processes and melanotic lesions through specific binding to melanin. Benefitting from this capacity, 18F-PFPN imaging could be a valuable tool to evaluate immune checkpoint inhibition efficacy by reflecting the changes in melanoma tumor cells. However, 18F-PFPN PET may underperform traditional 18F-FDG PET in less common amelanotic or hypomelanotic subtypes of MM, which comprise 2%−8% of all cases. These lesions, whose appearance can mimic several benign and malignant conditions, continue to pose significant diagnostic challenges (11).
Our findings need to be interpreted in the context of some limitations. First, it would have been interesting to include patients with early-stage (I−II) MM; more research is necessary to confirm our findings and to evaluate the role of 18F-PFPN PET imaging in this patient group. Second, our study focused on the clinical value of this imaging modality in patients with pigmented MM. One of the study patients had her distant amelanotic lesions missed on 18F-PFPN PET; therefore, the possibility of nonpigmented lesions in patients with MM should be based on a comprehensive consideration of thorough clinical and imaging investigations. Finally, the single-center design may have limited the external validity of our results. Despite these limitations, our data represent a promising step in understanding the potential utility of 18F-PFPN as a melanin tracer and may open new research directions. For example, labeling 18F-PFPN with therapeutic radioisotopes may warrant further scrutiny as a potential therapeutic strategy in metastatic MM (24).
CONCLUSION
18F-PFPN is a safe and well-tolerated melanin PET tracer. In a pilot clinical study, 18F-PFPN PET outperformed traditional 18F-FDG PET in identifying both primary MM and distant metastases. Further research is needed to verify these results in a larger sample and investigate the clinical value of 18F-PFPN PET imaging in early-stage MM.
DISCLOSURE
This work was financially supported by the National Natural Science Foundation of China (grants 81901783 and 82030052). Tzu-Chen Yen is an employee of Aprinoia Therapeutics Co., Ltd. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: 18F-PFPN is a novel PET probe with high affinity and selectivity for melanin; it may have clinical utility in patients with MM.
PERTINENT FINDINGS: In MM patients, uptake of 18F-PFPN was higher than that of 18F-FDG for both primary tumors and metastases, and 18F-PFPN PET could detect 365 metastases missed on 18F-FDG PET. Additionally, 18F-PFPN PET had clinical value in distinguishing false-positive lesions on 18F-FDG PET.
IMPLICATIONS FOR PATIENT CARE: 18F-PFPN PET may outperform traditional 18F-FDG PET in identifying both primary melanoma and its distant spread.
ACKNOWLEDGMENT
We thank Chunxia Qin for technical assistance.
Footnotes
Published online Feb. 3, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 8, 2021.
- Accepted for publication January 14, 2022.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}