


Abstract
In the Western world, more than 90% of head and neck cancers are head and neck squamous cell carcinomas (HNSCCs). The most appropriate treatment approach for HNSCC varies with the disease stage and disease site in the head and neck. Concurrent chemoradiotherapy has become a widely used means for the definitive treatment of locoregionally advanced HNSCC. Although this multimodality treatment provides higher response rates than radiotherapy alone, the detection of residual viable tumor after the end of therapy remains an important issue and is one of the major applications of 18F-FDG PET. Studies have shown that negative 18F-FDG PET or PET/CT results after concurrent chemoradiotherapy have a high negative predictive value (>95%), whereas the positive predictive value is only about 50%. However, when applied properly, FDG PET/CT can exclude residual disease in most patients, particularly patients with residual enlarged lymph nodes who would otherwise undergo neck dissection. In contrast to other malignancies, data are limited on the utility of 18F-FDG PET for monitoring the response to induction chemotherapy in HNSCC or for assessing treatment response early during the course of definitive chemoradiotherapy. The proliferation marker 18F-3′-deoxy-3′fluorothymidine is currently under study for this purpose. Beyond standard chemotherapy, newer treatment regimens in HNSCC take advantage of our improved understanding of tumor biology. Two molecules important in the progression of HNSCC are the epidermal growth factor receptor and the vascular endothelial growth factor (VEGF) and its receptor VEGF-R. Drugs attacking these molecules are now under study for HNSCC. PET probes have been developed for imaging the presence of these molecules in HNSCC and their inhibition by specific drug interaction; the relevance of these probes for response assessment in HNSCC will be discussed. Hypoxia is a common phenomenon in HNSCC and renders cancers resistant to chemo- and radiotherapy. Imaging and quantification of hypoxia with PET probes is under study and may become a prerequisite for overcoming chemo- and radioresistance using radiosensitizing drugs or hypoxia-directed irradiation techniques and for monitoring the response to these techniques in selected groups of patients. Although 18F-FDG PET/CT will remain the major clinical tool for monitoring treatment in HNSCC, other PET probes may have a role in identifying patients who are likely to benefit from treatment strategies that include biologic agents such as epidermal growth factor receptor inhibitors or VEGF inhibitors.
Head and neck cancer is the sixth most common cancer worldwide. In the Western world, more than 90% of these malignancies are head and neck squamous cell carcinomas (HNSCCs). Approximately 47,000 new cases of HNSCC were diagnosed in the United States in 2008 (1). The worst prognosis is seen in patients with unresectable advanced disease, with a 5-y survival rate of less than 10%. Selection of the most appropriate treatment approach varies with disease stage and site in the head and neck.
CURRENT CLINICAL PRACTICE
Patients with early-stage disease are generally treated with unimodality therapy consisting of either surgery or radiotherapy, and nearly 80% are cured. Postoperative radiotherapy is recommended when the risk for locoregional recurrence in the head and neck exceeds 20%. For patients whose disease is not controlled with definitive radiotherapy, salvage surgery is recommended. In patients who undergo surgery for more advanced lesions, postoperative adjuvant radiotherapy is generally part of the treatment plan. Improvements in locoregional control rates, progression-free survival (2), and overall survival (3) can be achieved at the expense of an increased rate of acute treatment-related adverse events. The pooled analysis of these 2 randomized trials suggested that concurrent chemoradiotherapy should be offered when surgical margins are positive for tumor or when lymph nodes show extracapsular extension (4).
Patients with locoregionally advanced disease that is surgically unresectable, and patients in whom definitive treatment is administered with an attempt at organ preservation (e.g., oropharyngeal and laryngeal carcinomas), undergo treatment with concurrent chemoradiotherapy (5,6). Cisplatin is the drug with the most randomized clinical trial data to support its use as a drug enhancing the effects of radiotherapy in this setting. The larynx-preservation paradigm is supported by the results of a study that randomized 547 patients with stage 3 or 4 supraglottic and glottic laryngeal cancer into 3 treatment arms: concurrent chemoradiotherapy, induction chemotherapy consisting of cisplatin and 5-fluorouracil (5-FU) followed by radiotherapy, or radiotherapy alone. After a median follow-up of 3.5 y, the rates of locoregional control were 78%, 61%, and 56%, respectively. The fraction of patients who maintained an intact larynx at 2 y (and thus the ability to speak and swallow after the end of therapy) was also better with the concurrent regimen (88%, 75%, and 70%, respectively) (5). Overall survival rates were similar in all 3 groups. The utility of concurrent high-dose cisplatin for other subsites was established in a randomized study of 295 patients with unresectable head and neck cancer (7). Patients were randomized to radiotherapy alone, radiotherapy plus concurrent high-dose cisplatin, or radiotherapy (split course) plus cisplatin and 5-FU. With a median follow-up of 41 mo, 3-y overall survival results were 23%, 37%, and 27%, respectively. Improved locoregional control rates were also reported for concurrent chemoradiotherapy with a drug combination of carboplatin and 5-FU (6). In 226 patients with stage 3 or 4 oropharynx cancer, the 5-y rates of locoregional control were 48% for concurrent therapy, compared with 24% for radiotherapy alone. Concurrent chemoradiotherapy is therefore now widely applied as the definitive treatment of choice for locoregionally advanced HNSCC. If residual disease is detected after the end of therapy or during follow-up, salvage surgery (e.g., laryngectomy) may be offered.
The management of the neck when using an organ-preservation approach has remained somewhat controversial. Complete response rates in irradiated cervical lymph nodes vary between 59% and 83% and to some degree are related to nodal size, dose of radiotherapy, and time point when response is determined: complete response rates are almost 100% in N1 disease, higher in N2 than in N3 disease, and better when the largest metastatic node is smaller than 3 cm (8). In N2 or N3 disease, residual cancer in neck nodes has been reported in 16%−39% of patients achieving a clinical complete response (no overt residual neck mass) (8–11). Early studies (12) demonstrated better outcomes when radiotherapy was followed by neck dissection, leading to the practice of “planned neck dissection” for all patients with N2 or N3 disease on presentation (regardless of the response to treatment) and for patients with N1 disease and persistent palpable lymph nodes after irradiation (13–15). More recently, however, the improved locoregional control rates with concurrent chemoradiotherapy have prompted a debate on whether planned neck dissection is still appropriate or necessary in all patients with initial N2 or N3 disease. Proponents of this approach argue that because clinical examination and structural imaging cannot reliably identify residual viable tumor, neck dissection is the only means to eradicate all residual disease in the neck (9). In contrast, opponents suggest that neck dissection be performed only in high-risk patients, whereas close clinical follow-up and observation may be appropriate in most cases. Several recent studies have tried to define the utility of 18F-FDG PET in this patient population. These will be discussed later in this article.
Patients with recurrent or metastatic disease have a median survival of approximately 6–9 mo. Therapeutic options include chemotherapy alone, irradiation or reirradiation with or without chemotherapy, salvage surgery, or best supportive care for patients with a low performance status. Reirradiation with concurrent chemotherapy is feasible for recurrent unresectable HNSCC but is associated with considerable acute and long-term toxicity (16–19).
In summary, the suboptimal disease control rates and survival figures in HNSCC emphasize the need for early disease detection in the primary and recurrent settings and a need for better imaging tools for staging and response assessment. There is also a clear need to investigate new therapeutic regimens and drugs, such as biologic and molecular agents.
NEWER BIOLOGIC THERAPIES
Antiangiogenesis Therapies
The sprouting of new vessels (angiogenesis) is essential for tumor growth and metastasis (20). Tumor cell proliferation alone, in the absence of angiogenesis, may give rise to dormant, microscopic tumors of about 1 mm3 or less, but these in situ cancers are harmless to the host (21,22). The term angiogenic switch has been used to describe the step when tumors acquire the ability to recruit their own blood supply to support growth beyond microscopic size (23). Preclinical research from the past 20 y suggests that complete pharmacologic blockade of tumor angiogenesis will leave only residual microscopic lesions, which may be clinically harmless and manageable as a chronic condition (23). Of note, the newly formed tumor vessels are structurally abnormal (“leaky”) and dysfunctional, delivering less blood and oxygen and fewer nutrients than normal blood vessels of similar caliber. Their leakiness (hyperpermeability) also causes increased interstitial pressure. Ultimately, these properties limit the build-up of sufficient drug concentrations within the tumor (24) and promote the development of hypoxic tumor subregions. Hypoxia in turn is one of the strongest promoters of angiogenesis (25–31).
Antiangiogenic therapies are particularly directed against these newly formed tumor vessels and may thus reduce or eliminate the excess supply of nutrients that are needed for tumor growth (32). Paradoxically, these drugs may also improve drug distribution within the tumor and reduce levels of intratumoral hypoxia because they eliminate the dysfunctional, leaky tumor vessels and thereby reduce intratumoral interstitial pressure (24). Angiogenesis is tightly regulated by several molecules (33); the best known and studied of these is the vascular endothelial growth factor (VEGF). Increased levels of VEGF are found in many HNSCCs and in patient serum (34,35). High VEGF expression is a marker of poor prognosis, correlating with higher clinical stage (36), high rates of locoregional recurrence, and lower disease-free and overall survival (37,38). Accordingly, there is great interest in exploiting antiangiogenic therapies for the treatment of HNSCC.
Bevacizumab, a recombinant humanized, monoclonal IgG antibody against VEGF, has been studied in HNSCC in combination with chemotherapy (33). Trials testing the combination of bevacizumab with cisplatin and radiotherapy are ongoing (39). VEGF receptor tyrosine kinase inhibitors have been studied in smaller phase I trials (40), and combination therapies of bevacizumab with tyrosine kinase inhibitors are being developed (41). Experimentally, synergistic (supraadditive) effects have been observed for the combination of bevacizumab with the epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor erlotinib, as well as for the EGFR kinase inhibitor gefitinib and specific VEGF receptor tyrosine kinase inhibitors in conjunction with irradiation (42,43). The rationale for combining biologic agents with radiotherapy is based on evidence from experimental studies. Contrary to the concern that antiangiogenic therapy may cause or promote tumor hypoxia and hence radioresistance, it is indeed the newly formed tumor vessels that contribute to radioresistance. In tumor xenografts, external irradiation induces a 2- to 3-fold increase in VEGF expression and secretion that lasts for up to 14 d (44). This mechanism may contribute to protecting tumor blood vessels from radiation-mediated cytotoxicity and thus in fact promotes radioresistance (the tumor protecting itself). This radiation-induced angiogenesis can be suppressed by bevacizumab and erlotinib (43).
Therapies Targeting the EGFR
The EGFR is a member of the ErbB family of tyrosine kinase receptors. It is overexpressed or activated in most HNSCCs relative to normal tissue (45), and high expression is associated with poor disease control (46–49). EGFR copy number as determined by quantitative reverse-transcriptase polymerase chain reaction is inversely related to patient outcome: in a study of 134 patients with primary HNSCC, the 5-y survival in individuals with an increased EGFR copy number was only 9%, compared with 71% in individuals with a normal copy number (50). Although these data suggest that HNSCC is an ideal malignancy for treatment with EGFR inhibitors, the selection of appropriate patients for therapy with these agents remains challenging. In studies of anti-EGFR agents in patients with advanced HNSCC, the objective response rates have been approximately 10%, with the percentage depending on the specific agent (51).
Cetuximab, a chimeric IgG1 antibody against the extracellular domain of EGFR, is the most widely studied agent. Cetuximab receptor binding competes with the binding of the natural EGFR ligands and blocks the activation of the receptor tyrosine kinase (52). Cetuximab has been studied in recurrent HNSCC in combination with cisplatin (53) or in combination with platinum plus 5-FU (54) as a first-line treatment and also as a secondary treatment option in cases of platinum-refractory disease (55–57). In these trials including a total of almost 400 patients, the response rates based on CT or MRI assessment of target lesions were in the range of 10%−26%, although the disease control rates (a parameter that includes all patients with complete response, partial response, or stable disease) were as high as 46%−53% (55,57). In the largest trial to date (EXTREME trial), 442 patients with untreated metastatic or recurrent HNSCC were randomized to treatment with 5-FU plus either carboplatin or cisplatin, or the same chemotherapy regimen plus cetuximab. The addition of cetuximab increased the response rate from 20% to 36% (P < 0.001) and improved the median overall survival slightly but significantly from 7.4 to 10.1 mo (58).
Cetuximab also enhances the efficacy of radiation therapy. In a large, randomized study of 420 patients with locoregionally advanced HNSCC (59), the addition of cetuximab to radiotherapy improved locoregional tumor control and overall survival without increasing mucositis and dysphagia, when compared with radiotherapy alone. The corresponding median progression-free survival was 24 versus 15 mo, and the median overall survival was 49 versus 29 mo. Although this study did establish concurrent radiotherapy plus cetuximab as a viable treatment option in locoregionally advanced HNSCC, the study has also been criticized because the control group was treated with radiotherapy alone whereas the present standard regimen would be concurrent chemoradiotherapy. This issue is being addressed in ongoing clinical trials. One study is randomizing patients to induction chemotherapy followed by cisplatin plus radiotherapy versus induction chemotherapy followed by cetuximab with radiotherapy (60). Another randomized study is comparing standard concurrent chemoradiotherapy versus concurrent chemoradiotherapy plus cetuximab (61).
Other EGFR-inhibiting drugs include the small-molecule tyrosine kinase inhibitors gefitinib and erlotinib, which have been tested as single agents (62,63) or in combination with cisplatin (64). When used in combination with cisplatin, erlotinib seemed to have an additive effect, leading to an objective partial or complete response in 21% of patients and disease stabilization in 49%. However, the median progression-free survival was only 3 mo.
In summary, there is a sound scientific rationale for applying biologic agents against EGFR and VEGF in patients with locoregionally advanced or metastatic HNSCC. Unfortunately, major clinical responses are relatively rare. The selection of appropriate patients for therapy with these new and expensive drugs remains challenging.
RESPONSE ASSESSMENT WITH 18F-FDG PET
18F-FDG PET After Chemo- or Radiotherapy
Structural imaging with contrast-enhanced CT or MRI and functional imaging with 18F-FDG PET are now considered standard for assessing the response to therapy in HNSCC. In this section, we shall focus on studies in which 18F-FDG PET was used in patients treated with curative intent. Response rates at the site of primary disease are generally high with concurrent chemoradiotherapy. Therefore, the main focus of posttherapy PET is the detection of residual disease in neck lymph nodes. Tables 1 and 2, a summary of published data, show that most studies on posttherapy 18F-FDG PET in HNSCC included heterogeneous patient populations and that all the data come from retrospective analyses:
Patient selection criteria varied: Some studies included consecutive patients after chemo- or radiotherapy regardless of clinical or structural imaging findings. Some studies enrolled only patients with residual structural abnormality on clinical examination or CT/MRI. Some studies excluded patients with suspected or proven residual abnormality at the primary disease site and specifically addressed the role of PET for detecting residual cancer in neck lymph nodes.
Disease sites varied: Most studies focused on the utility of PET for response assessment after concurrent chemoradiotherapy (which is applied mostly for malignancies in the oropharynx and larynx), but some studies also included a large fraction of patients with other disease sites (nasopharynx, paranasal sinuses, skin). This difference is critical because tumor biology, clinical behavior, expected response rates, and the potential for false-positive findings differ between these latter cancers and tumors of the oropharynx and larynx.
Treatment strategies varied somewhat: One institution (65) reported on the utility of PET after induction chemotherapy (which is currently not considered a standard approach) and after subsequent definitive concurrent chemoradiotherapy, whereas all other studies focused on the outcome after definitive therapy.
Treatment protocols varied somewhat: Most but not all patients were treated with concurrent chemoradiotherapy. It is clear that greater posttreatment inflammation is expected after concurrent therapy than after irradiation alone. Chemotherapy acts as a radiation sensitizer in the irradiated tumor but also in the surrounding normal tissue that is included in the radiation field. Studies also differ in radiotherapy schedules, doses, and techniques. Only one study specifically addressed the role of PET after intensity-modulated radiotherapy (66).
Use of PET/CT versus only PET varied: Only a few recent studies specifically studied the role of combined PET/CT in this setting (67–70). In some other studies, a fraction of patients was imaged with PET/CT, but other patients were imaged with PET only. Earlier studies generally assessed the utility of PET only. This difference between studies is important because combined PET/CT reduces the number of equivocal findings and improves study accuracy (71,72).
Appropriate time for PET in response assessment varied: Perhaps most important, the time between the end of therapy and the PET scan varied considerably, ranging from 4 wk to almost 1 y. In a study of 26 patients, Goerres et al. (73) observed a sensitivity and specificity of 91% and 93%, respectively, for PET scans performed as early as 6 wk after chemoradiotherapy. We and others have not been able to reproduce these data (74,75) and instead suggest that posttherapy PET after chemoradiotherapy should not be performed before 10–12 wk after the end of treatment. By that time, most of the posttreatment inflammatory changes will have subsided, reducing the number of potentially false-positive interpretations. In general, the rate of false-positive cases declines with the interval between end of therapy and PET (76). Therefore, it is not surprising that studies that include a large fraction of patients in whom PET was performed as late as 6 mo after the end of therapy will have a lower false-positive rate. Some studies also demonstrated a higher false-negative rate when PET was done less than 4–8 wk after the end of therapy (68,77). It is conceivable that small-volume residual disease at this early time escapes detection on PET. Of note, most irradiated cells do not die instantaneously but instead can still undergo several cycles of cell division (only cells irradiated in the mid to late S-phase show instantaneous cell cycle blockade). Their subsequent fate varies: some cells may remain dormant for a protracted time and die eventually, but some cells may recover and start dividing again (78,79). Indeed, experimental studies on irradiated cell cultures show a rapid decline in 18F-FDG uptake, but the tracer uptake is not instantaneously abolished. Dormant cancer cells maintain their capability for glucose uptake and retention as long as their cell membrane is intact and basic metabolic processes continue. Some of these cells eventually die, whereas other cells may recover their full metabolic and proliferative potential. With increasing volume, the residual viable tumor cell nests may eventually become detectable on 18F-FDG PET.
Summary of Published Data: Patients
Summary of Published Data: Results
We would like to highlight some of the studies listed in Tables 1 and 2 to demonstrate the utility of 18F-FDG PET in HNSCC after irradiation and chemoradiotherapy. Data are based on the number of patients or on the number of heminecks in which disease was initially diagnosed. The first study included 53 patients (70 heminecks) who were imaged with PET or PET/CT (75). The median interval between end of therapy and PET was 15 wk. Twenty-eight of the 70 heminecks harbored residual enlarged lymph nodes. Using neck dissection or clinical follow-up as the standard of reference, 18F-FDG PET showed a sensitivity of 100% and a specificity of 94%, with a positive predictive value (PPV) of 43% and a negative predictive value (NPV) of 100%. The second study evaluated 39 patients who achieved a complete response to concurrent chemoradiotherapy at the primary site but had a residual neck mass (74). 18F-FDG PET, performed at a median of 12 wk after the end of therapy, had a sensitivity of 83% and a specificity of 93%; the NPV was 97%. Residual nodal metastasis was eventually proven in 6 of the 39 individuals; hence the PPV of structural imaging was only 15%. Finally, Ong et al. (67) studied 65 patients (84 heminecks) after concurrent chemoradiotherapy. 18F-FDG PET/CT was performed on all patients at least 8 wk after the end of therapy. The standard of reference consisted of histopathology of neck dissection specimens or clinical and imaging follow-up. In this study, the sensitivity and specificity were 71% and 89%, respectively, with a PPV of 38% and an NPV of 97%. All false-positive lymph nodes in neck dissection specimens showed either inflammation or granulomatous disease, which are known causes of increased 18F-FDG uptake in lymph nodes. Nevertheless, the fraction of false-positive studies could be reduced from 27% to 10% when the neck was assessed by combined PET/CT rather than by structural imaging alone, while maintaining a high NPV of 97%. The true value of posttherapy 18F-FDG PET in patients treated with current radio- or chemoradiotherapy is the high NPV. Many patients who might otherwise proceed to biopsy or planned neck dissection can in fact be observed with clinical follow-up and periodic imaging studies. Although the PPV of PET after chemoradiotherapy is relatively low, most scans will in fact have negative findings when interpreted properly. However, true prolonged, intense 18F-FDG uptake after definitive therapy indicates a poor treatment outcome or treatment-related complications: In an interesting study on patients with laryngeal cancer treated with intensity-modulated radiotherapy, Dornfeld et al. (80) showed an inverse relationship between the intensity of (persistent) 18F-FDG uptake at 12 mo after treatment and quality of life, the ability to speak, and the ability to swallow solid foods. In other words, persistent 18F-FDG uptake indicates either persistent disease or persistent treatment-induced structural and functional damage to the larynx.
Suggested PET Interpretation Criteria
Combined PET/CT, rather than PET only, should be used because it is more accurate and avoids equivocal interpretations, can distinguish between 18F-FDG uptake in normal structures versus lymph nodes, can guide biopsies, and can potentially guide planning of the target for adjuvant radiotherapy (71,72,81,82). 18F-FDG uptake in the treated neck should decline within weeks, allowing an accurate reading to be rendered at approximately 10–12 wk after the end of chemoradiotherapy. However, as in other disease sites, tracer uptake may occasionally persist (usually at mild to moderate intensity) for several months. The underlying reasons include persistent cancer, inflammation, abscess formation, and radionecrosis.
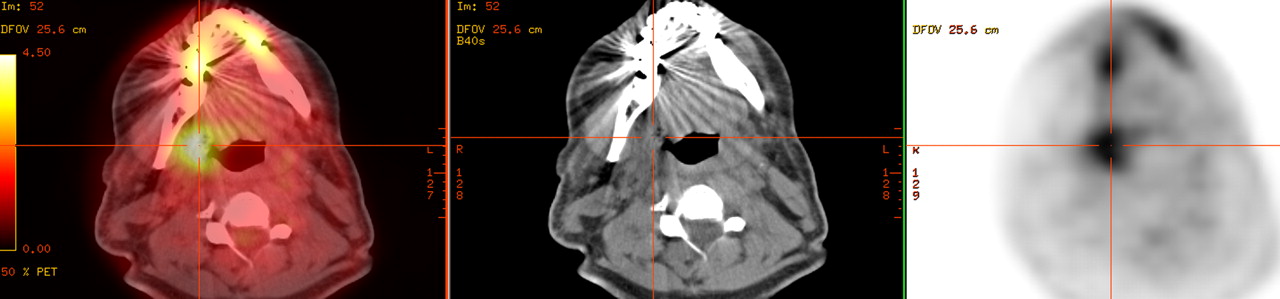
In general, focal and asymmetric 18F-FDG uptake with an intensity greater than that in surrounding normal tissues (in particular, muscle) and blood vessels should be considered suggestive of residual disease. On PET/CT, such abnormalities should fuse to the site of the primary disease or lymph nodes (rather than blood vessels, fat tissue, skeletal muscle, or other sites). In contrast, diffuse (nonfocal) 18F-FDG uptake within the radiation field is usually an indicator of postradiation inflammation. One of the initial trials that established concurrent chemoradiotherapy in locoregionally advanced HNSCC reported high-grade toxic effects in 82% of patients, including grade 3 or 4 mucositis in 41% of patients and laryngeal toxicity in 14% (5). This report has obvious implications for imaging studies: laryngeal edema and treatment-induced infiltrative changes in perilaryngeal soft tissues are commonly observed on posttreatment CT, along with nonspecific contrast enhancement patterns. Likewise, increased laryngeal or oropharyngeal 18F-FDG uptake may be observed for prolonged periods after chemoradiotherapy. In most cases, this uptake will be of mild to moderate intensity and will be diffuse throughout the larynx or along oropharyngeal walls. Again, focal uptake should raise suspicion about ulceration or persistent disease. In view of the relatively high response rates, the fact that persistent disease is uncommon should be considered when one is interpreting PET scans in this setting. Patient examples are shown in Figures 1–3⇓⇓.
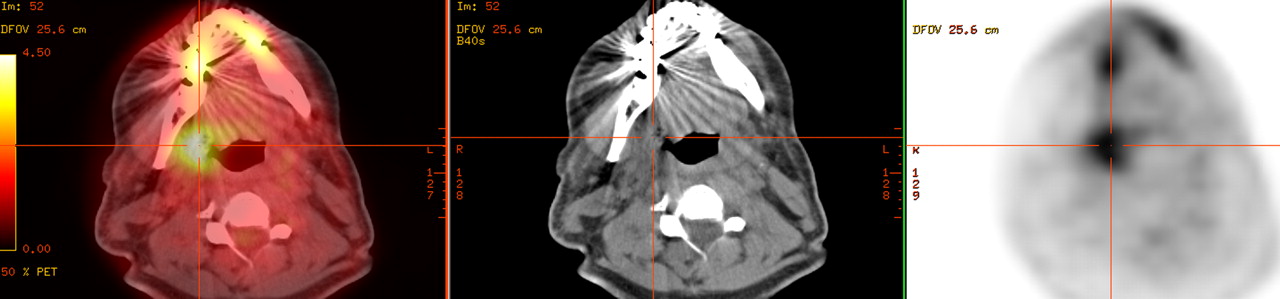
False-positive PET/CT findings for primary site, right tonsil cancer (T4N2c). PET/CT was performed 14 wk after chemoradiotherapy. Focally intense 18F-FDG uptake is seen in right tonsillar fossa, with SUV of 4.7; small ulceration was seen clinically. 18F-FDG uptake resolved on follow-up scan 3 mo later. However, this focal pattern of intense uptake is indeed the most characteristic finding in local residual disease.
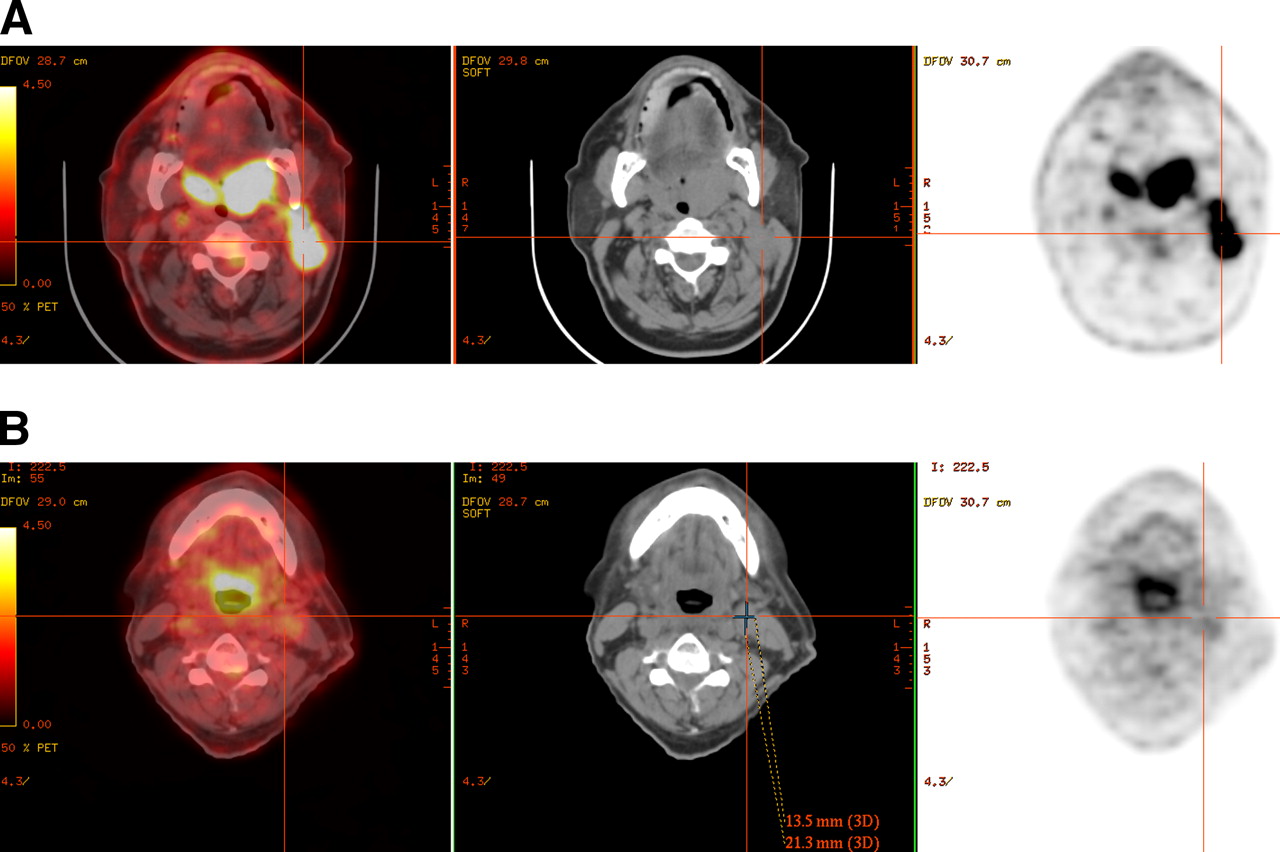
True-negative PET/CT findings for T2N2b cancer on left side of base of tongue. (A) Pretherapy scan shows intense 18F-FDG uptake in primary tumor and left neck lymphadenopathy. (B) Scan obtained 10 wk after end of chemoradiotherapy shows 13 × 21 mm lymph node in left neck, level 2, and mild, diffuse uptake (SUV 2.7) not strictly confined to node.

True-positive PET/CT findings for lymph node uptake in a case of T2N2a cancer on left side of base of tongue. PET/CT was performed 10 wk after end of chemoradiotherapy. A 7 × 17 mm lymph node in left neck, level 2, shows focal 18F-FDG uptake clearly higher than surrounding background activity, with SUV of 3.2.
Standardized uptake values (SUVs) cannot differentiate reliably between residual cancer and inflammation. In a retrospective analysis, Yao et al. (75) showed that an SUV of 2.9 identified residual disease in neck nodes with a sensitivity of 100% and a specificity of 97%. However, this finding could not be confirmed in subsequent studies. When applying the same SUV cutoff to a similar patient population, Ong et al. (67) reported a sensitivity of 57% and specificity of 84%, which were considerably worse than the 71% sensitivity and 89% specificity based on visual assessment using the aforementioned criteria. SUVs proposed as suitable cutoffs for the identification of residual cancer based on single-institution studies on a specific set of patients may not be applicable to other institutions with different equipment, patient populations, and clinical imaging protocols. It is also unlikely that any sharp cutoff truly exists between malignant and benign SUVs. Looking on the bright side, though, it is reassuring that clinical image interpretation skills and judgment, acquired over many years, cannot be replaced by a computer-generated number.
Impact on Patient Management
Because clinical parameters and structural imaging cannot reliably predict the presence of residual metastatic neck disease, some investigators still advocate planned neck dissection in all patients with initial N2 or N3 disease (8–10,83,84). Historically, the risk for residual cancer in such nodes has exceeded 20%, a number that has been accepted as the lower threshold for surgical intervention. In light of the high NPV of posttreatment 18F-FDG PET, this approach may no longer be justified. In one of the previously cited studies (67), planned neck dissection would have been considered in 51 patients because of the presence of residual enlarged lymph nodes, but disease was in fact present in only 7 of them. As shown in Tables 1 and 2, most posttreatment 18F-FDG PET scans even in this subset of patients with more advanced (N2 or N3) nodal disease will be negative with current treatment protocols. Implementing a treatment strategy based on posttherapy PET/CT findings in the study by Ong et al. (67) could have reduced the number of planned neck dissections by 75% (from 51 to 13) while missing disease in 2% (2/84 heminecks). Other investigators have suggested that negative 18F-FDG PET/CT results after chemoradiotherapy could reduce the number of planned neck dissections by more than 80% (70). Although clinical factors, including the initial nodal stage, remain an important consideration, it would appear that a PET/CT-based strategy might reduce the element of arbitrary decision making in patient management after chemoradiotherapy.
Whereas all of the aforementioned studies were retrospective, the currently ongoing Radiation Therapy Oncology Group Trial 0522 (85) is collecting these data prospectively. Patients with locoregionally advanced HNSCC will be randomized to treatment with cisplatin and radiotherapy, or cisplatin and radiotherapy plus cetuximab. This study primarily aims to determine whether disease-specific survival can be improved with the addition of cetuximab. However, a substudy will also investigate the prognostic and diagnostic utility of 18F-FDG PET before and after the end of therapy, and in particular the correlation between posttreatment 18F-FDG PET findings and nodal response or nodal relapse rates. The organizers hypothesize that negative posttreatment 18F-FDG PET results in patients with N2 or N3 disease indicates a pathologic complete response in more than 85% of treated necks and, conversely, a low overall nodal relapse rate of 10% or less. Study results will likely not become available before 2010.
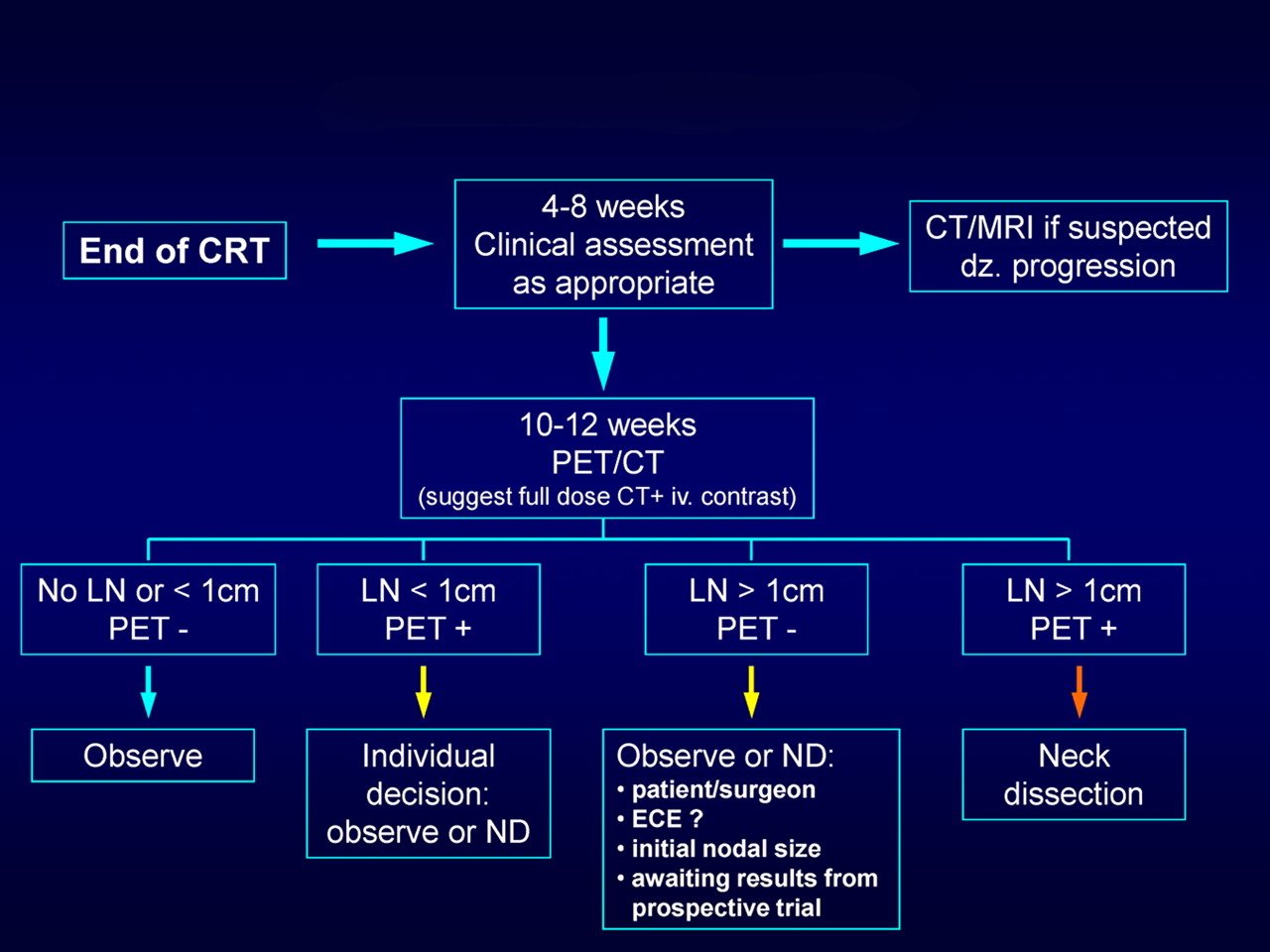
Several authors have proposed algorithms for patient management after chemoradiotherapy (67,74,75,86). These algorithms differ slightly in their proposed time points for early structural imaging and in the implications of PET findings for subsequent patient management. Some authors (75,86) have proposed the routine use of early (6–8 wk after the end of therapy) structural imaging to assess the treatment response, followed by a second set of PET and CT studies at 12 wk. We believe that a more measured approach can be taken and recommend early imaging of any kind only if there is a strong clinical suspicion of lack of response or progression (Fig. 4). In particular, it is the consensus opinion of the multidisciplinary head and neck cancer team at Memorial Sloan-Kettering Cancer Center that a dedicated neck CT scan with intravenous contrast material and 18F-FDG PET/CT (potentially in a single imaging session) should be performed about 10–12 wk after the end of therapy, unless clinical management requires imaging earlier. This time point strikes a balance between the clinical desire for early, yet accurate, response assessment and the surgeon's desire not to perform a neck dissection on tissues in which extensive fibrosis and scar tissue have developed as the result of chemoradiotherapy. Shrinkage of large nodal masses will take time; early imaging after the end of therapy only causes uncertainty and will rarely provide guidance for management. As shown in Figure 1, patients with no residual abnormal lymph nodes on CT (i.e., diameter < 1 cm) can generally be observed, because CT has a high NPV and 18F-FDG uptake in these normal-sized nodes is frequently false-positive. Patients with residual lymphadenopathy and abnormal PET findings should undergo neck dissection, possibly in the form of superselective neck dissection, which addresses only 1 or 2 neck levels of concern (87). Management of patients with residual enlarged nodes and negative PET findings should be individualized according to the following considerations: First, negative PET findings have a high NPV, and planned neck dissection is thus unnecessary in most of these cases. However, close follow-up of these patients is required. Second, if close clinical follow-up cannot be guaranteed, or if extenuating circumstances indicate a higher likelihood for local recurrence (e.g., extranodal tumor extension), a neck dissection may be indicated. Third, in any event, the rationale for the chosen approach should be discussed with the patient.
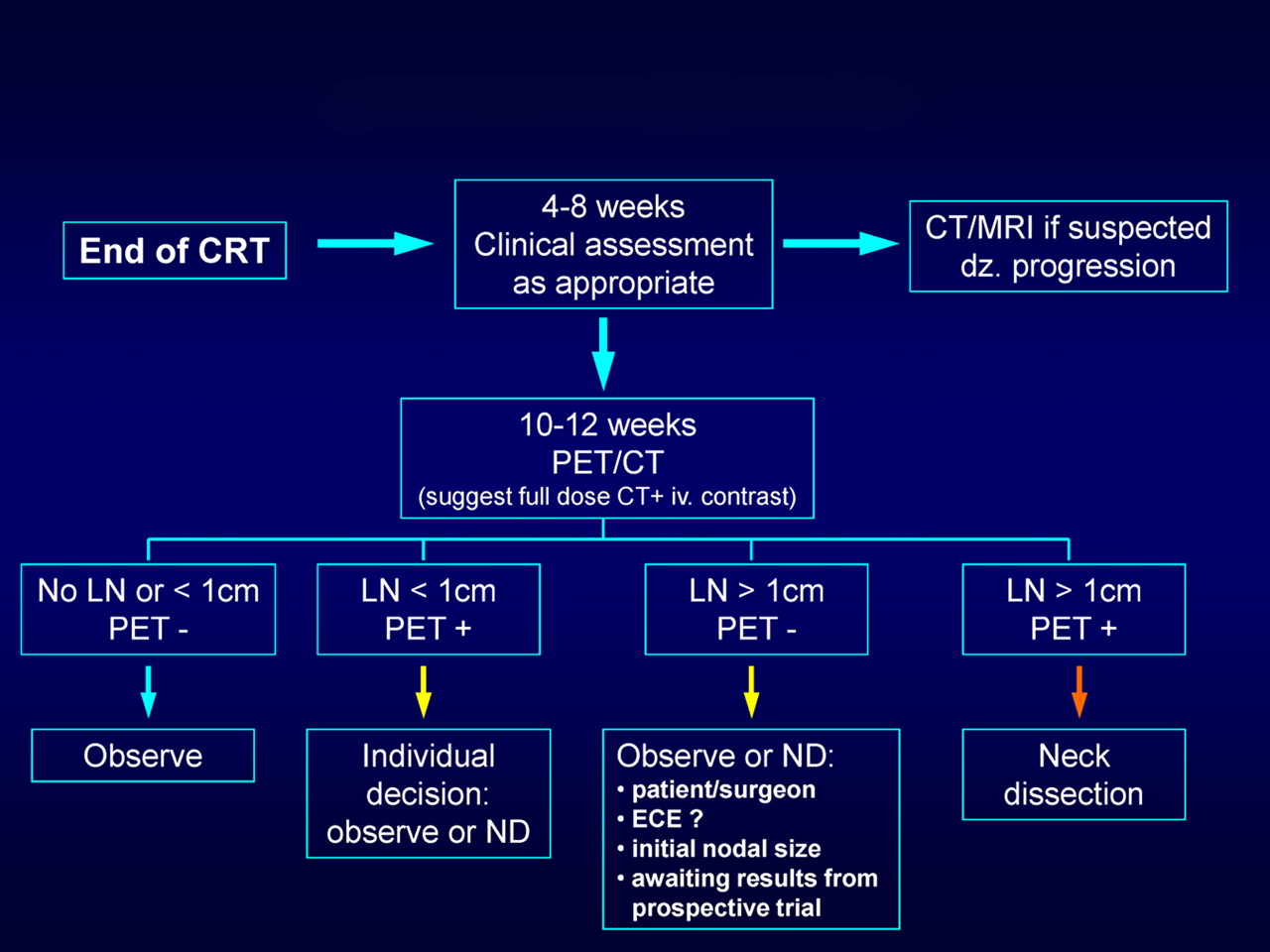
Suggested algorithm for management of HNSCC patients after chemoradiotherapy, based on PET and CT findings obtained approximately 10–12 wk after end of therapy. dz. = disease; ECE = extracapsular extension; iv. = intravenous; LN = lymph node; ND = neck dissection; PET - = PET-negative; PET + = PET-positive.
Regarding the optimal time point for follow-up imaging, we believe that PET scans done later than 12 wk after the end of therapy will not be helpful to surgeons attempting to judge the need for a neck dissection. Although these later scans may still provide clinically useful information (e.g., in the surveillance of high-risk patients or in the detection of early recurrence), they do not qualify as a tool for response assessment.
Ideally, the concept that patient management can be decided on the basis of posttherapy PET/CT findings would be tested in a randomized trial comparing outcome data in 2 groups of patients. In one group, planned neck dissection would be performed routinely, whereas in the other group, neck dissection would be performed only when the PET scan result was suggestive; all other patients would be followed clinically. Although a randomized trial may be preferred on scientific grounds, it is unlikely that this will happen, because the available evidence has already begun to shape clinical practice. A reasonable alternative approach would involve a medical team of head and neck cancer specialists (surgeons, oncologists, imaging physicians) that provide a structured plan for close follow-up based on one of the proposed algorithms.
18F-FDG PET During Chemoradiotherapy or After Induction Chemotherapy
The potential clinical utility of PET for early response assessment during chemoradiotherapy has not been studied systematically. Data from other malignancies (88,89) suggest that a significant decline in 18F-FDG uptake between baseline and interim PET after a few cycles of chemo- or chemoradiotherapy may indicate a better prognosis and high likelihood for achieving a complete response. Only a single small study has attempted to address this question in HNSCC (90). Using coincidence camera imaging, that study noted an early and significant decline in 18F-FDG uptake in 47 patients with locally advanced disease after a cycle of chemotherapy or 24 Gy of radiotherapy. When dichotomized by the median SUV, individuals with lower 18F-FDG uptake showed a better rate of locoregional control. However, a closer analysis of the study reveals that similar prognostic information could also be derived from the baseline scan alone. Although interesting, the study remains therefore largely inconclusive. In particular, it remains unclear at what interim time point during the course of therapy a PET scan should be performed and how interim PET findings might alter patient management (good local control rates with concurrent chemoradiotherapy, lack of an established alternate therapy).
There are also limited data on the role of PET in assessing the response to induction chemotherapy before subsequent concurrent chemoradiotherapy. This is a topic of growing interest to medical oncologists. Proponents of this approach believe that it may improve clinical outcome in locoregionally advanced HNSCC. For instance, in the DeCIDE trial, patients with N2 or N3 disease will be randomized to treatment with standard concurrent chemoradiotherapy or induction chemotherapy followed by chemoradiotherapy. The effect on overall and progression-free survival, rate of distant metastases, and quality of life will be compared (91). Other currently ongoing studies in the United States and Europe will apply induction chemotherapy followed by radiotherapy in combination with cisplatin or a biologic agent such as cetuximab (92,93). In the future, it will be important to identify patients who might benefit from this new treatment approach. It is conceivable that PET with either 18F-FDG or 18F-3′-deoxy-3′fluorothymidine (FLT) after induction chemotherapy might help in this decision. For instance, if a patient shows little or no metabolic response after induction chemotherapy, this might indicate a low likelihood for cure with subsequent chemoradiotherapy; perhaps such patients would benefit from immediate salvage surgery after induction therapy or should be enrolled in more aggressive chemoradiotherapy protocols.
18F-FDG PET After Surgery and Before Adjuvant Therapy
Shintani et al. (94) investigated the role of 18F-FDG PET/CT early after surgical resection and before planned adjuvant radiotherapy in a heterogeneous group of 91 patients (62 with squamous cell carcinoma). PET/CT approximately 28 d after surgery revealed findings suggestive of residual macroscopic tumor in 24 of the 91 individuals (26%). Subsequent biopsies proving residual cancer in 45% of these instances (PPV, 45%) led to a change in management in 14 patients (15%), including abandonment of adjuvant radiotherapy and a switch to palliative chemotherapy, as well as changes in radiation field or dose. Imaging early after surgery obviously causes a high rate of false-positive findings; the exact role of PET/CT, if any, remains to be defined. However, it is clear that combined PET/CT (rather than PET only) should be performed to enable precise target definition for radiotherapy in HNSCC (95).
A POTENTIAL ROLE FOR OTHER PET RADIOTRACERS
Amino Acid Transport and Protein Synthesis
PET with labeled amino acids has been applied to head and neck cancer. Despite the excitement generated by earlier studies, no tracer of amino acid transport or protein synthesis has been tested rigorously in HNSCC. 11C-methionine did not provide any clear benefits over imaging with 18F-FDG. The short half-life of 11C requires a nearby cyclotron, and the image quality is suboptimal. False-positive uptake at sites of inflammation can occur with this agent and with other amino acids. It is doubtful that any of these agents will have a future in the clinical response assessment of patients with HNSCC.
18F-FLT
18F-FLT uptake and retention require a functional nucleoside transporter in the plasma membrane and activity of the thymidine kinase-1 enzyme (96). In vitro, 18F-FLT retention correlates with the fraction of cells in the S-phase of the cell cycle and with thymidine kinase-1 activity (97,98). Thymidine kinase-1 is inhibited by many chemotherapeutic drugs and by external-beam irradiation (97). When tumor cells are irradiated, they do not enter the cell cycle but instead remain in the S-phase (97). In vitro, a radiation dose–dependent decrease in 18F-FLT uptake that paralleled the decline of the fraction of cells in the S-phase was shown (98). Decreases in 18F-FLT uptake and thymidine kinase-1 activity were observed within 24 h after irradiation.
The clinical utility of 18F-FLT in clinical response assessment in HNSCC is under investigation. From studies on other malignancies (99) it might be inferred that 18F-FLT imaging could potentially permit an earlier or more accurate response assessment in HNSCC than can imaging with 18F-FDG or CT/MRI. However, preliminary experimental studies have shown mixed results. When nude mice bearing the human squamous cell cancer graft (HNX-OE; nu/nu mice) were irradiated, both 18F-FDG and 18F-FLT uptake declined from baseline levels, but the decline in 18F-FDG uptake occurred mainly during the first week of treatment, whereas the greatest decline in 18F-FLT uptake was noted during the second treatment week (100). In another study, however, 18F-FLT PET showed promise in assessing the early response to cetuximab in a squamous cell cancer xenograft model (101). A significant decline in tumor SUV, tumor-to-muscle ratios, and thymidine kinase-1 activity occurred as early as 6 d after single-agent therapy had been initiated with cetuximab. In the clinic, these early changes might be helpful in assessing the response to cetuximab monotherapy during the induction phase for subsequent combination chemotherapy or chemoradiotherapy. Of note, false-positive 18F-FLT uptake can occur in reactive lymph nodes (102) and is a particular problem after concurrent chemoradiotherapy. The frequency of false-positive 18F-FLT uptake during or after chemoradiotherapy in patients with HNSCC has not been established. If this were indeed a common phenomenon, it would severely limit the utility of this tracer for response assessment.
Hypoxia Imaging
Tumor hypoxia is a common phenomenon in HNSCC (103–105). Hypoxic cells are resistant to the cytotoxic effects of chemotherapy and ionizing radiation (106–109) and require radiation doses up to 3 times higher than for the same level of cell inactivation relative to the same cells under normoxic conditions. A recent review of nearly 400 HNSCC patients who underwent tumor oxygenation measurement demonstrated that hypoxia was strongly associated with treatment failure (locoregional recurrence and distant metastasis) independently of stage and therapeutic modality (105). This observation has led to a growing interest in diagnosing hypoxic HNSCC before therapy in the hope of applying novel treatment strategies that may overcome the resistance to conventional chemoradiotherapy. Several compounds are available for the imaging of hypoxia (109,110). Currently, 18F-fluoromisonidazole (18F-FMISO) is still considered the standard PET tracer for hypoxia imaging. One goal of hypoxia imaging is the identification of patients with hypoxic tumors who may benefit from a combination therapy of irradiation with radiation sensitizers (111), vasodilators, or carbogen breathing, as was used in the ARCON (accelerated radiotherapy with carbogen and nicotinamide) trial in advanced head and neck cancer (112), or hypoxic cell cytotoxins such as tirapazamine. Whereas the nonselective addition of tirapazamine to standard chemoradiotherapy did not improve clinical outcome in a randomized phase III trial (HEADSTART) (113), an improvement in locoregional control rates could be shown in selected patients with evidence of tumor hypoxia on 18F-FMISO PET (114). However, some recent data suggest that hypoxia as shown on FMISO PET may be overcome in most patients even with standard chemoradiotherapy (115). Four weeks into treatment, only 2 of 20 patients showed imaging evidence of persistent hypoxia on the 18F-FMISO scan, and local recurrence did not develop in these 2 patients. With a median follow-up of 36 mo, the 3-y progression-free survival in this patient population was 95%. The frequency and time course at which tumor hypoxia persists after the initiation of chemoradiotherapy are unknown. It is conceivable that treatment outcome can be improved, despite the presence of hypoxia, with certain combinations of standard chemotherapy and irradiation. However, if interventions aimed at overcoming tumor hypoxia are used as part of the experimental protocol, they should probably center on the first 4 wk of therapy.
Imaging EGFR and Response to EGFR Inhibitors
Neither clinical presentation nor immunohistochemical analysis of tumor specimens can reliably predict the therapeutic response to EGFR inhibitors. A high EGFR gene copy in tumor specimens may identify patients with a increased likelihood of response, and a decline in phosphorylated EGFR levels in skin biopsies during therapy has been suggested as a potential surrogate marker for improved clinical outcome (116). However, the latter reflects only a systemic drug effect or toxicity and does not provide any information about local drug concentrations or about the effect on the tumor itself.
Clinical response can certainly be assessed nonspecifically with 18F-FDG PET (117,118). Downregulation of 18F-FDG uptake after treatment with small-molecule tyrosine kinase inhibitors, such as gefitinib, seems to be an early phenomenon (119) that precedes changes on structural imaging. More specific imaging tests based on the increasing recognition of the molecular structure of receptors and tumor pathways are being developed. Signal transduction through EGFR requires ligand binding to the receptor, dimerization of ligand–receptor complexes, and autophosphorylation of the receptor at the intracellular tyrosine kinase domain. In principle, at least 2 of these steps can be imaged, and such imaging might be helpful in predicting and monitoring treatment response. For instance, one radiolabeled ligand for EGFR, the chelate complex 64Cu–DOTA–cetuximab, has been tested in small-animal studies correlating tracer uptake on small-animal PET with EGFR expression in Western blot analysis (120). Another group of tracers, radiolabeled anilinoquinazolines, bind to the intracellular adenosine triphosphate binding pocket of the receptor kinase; agents that bind irreversibly at this site and are labeled with 11C or 124I appear suitable for PET (121,122). It is hoped that clinical PET studies with these or similar compounds may help in selecting patients who are likely to respond to EGFR inhibitors and in monitoring the drug response in a specific manner.
Imaging of Angiogenesis and Angiogenesis Inhibitors
It is currently unclear which patients may particularly benefit from treatment with angiogenesis-inhibiting drugs. Although elevated VEGF serum levels are a marker of poor prognosis in HNSCC, they cannot predict the clinical response to antiangiogenic therapies (123). First, VEGF is produced not only by tumor cells but also by normal platelets, cells in the tumor-surrounding stroma, and other cells in the body; second, VEGF receptors are found primarily on endothelial cells but also on various tumor cells; third, resistance to VEGF inhibitors can exist intrinsically or may develop during therapy (e.g., due to upregulation of other angiogenic receptors or an increase in circulating endothelial progenitor cells) (123). Because inhibition of angiogenesis per se may not cause cell death and tumor shrinkage (but instead “only” prevent further growth), it is also unclear how the efficacy of angiogenesis inhibitors could best be shown and monitored in the clinical setting (rather than inferring efficacy indirectly from achieving stable disease).
Changes in tumor hyperemia can be documented on contrast-enhanced CT and MRI or dedicated MRI perfusion sequences. However, more specific imaging tests documenting drug targeting and effect are available. One example is the radiotracer 18F-RGD peptide (124,125), which binds specifically to ανβ3 integrins expressed at the surface of activated endothelial cells during angiogenesis (126). The intensity of 18F-RGD peptide accumulation correlates with the presence of activated endothelial cells and, quantitatively, with microvessel density (124). 18F-RGD peptide imaging of HNSCC is feasible (127): In a pilot study of 11 patients, tracer uptake was detected in 10 of 12 primary lesions (SUV, 2.2–5.8) with reasonable contrast, based on a tumor-to-blood ratio of 2.8 ± 1.1. Two tumors that were smaller than 5 mm were missed. Immunohistochemistry confirmed αvβ3 expression on microvessels in all tumors. This or similar radiotracers might potentially be useful in identifying suitable patients for treatment with antiangiogenic drugs and in monitoring the response to such therapies in a drug-specific manner (instead of, or in addition to, tumor shrinkage or a decline in glucose metabolism).
Treatment Options on the Horizon
Cancer gene therapy, whereby replication-incompetent viral vectors are used to transfer a therapeutic gene into the cancer cell, is under study in many malignancies, including HNSCC (128). Another treatment option is the use of oncolytic viruses, which infect, multiply within, and subsequently lyse cancer cells. The attenuated adenovirus ONYX-015, which preferentially localizes in cells lacking the tumor suppressor gene p53, has been tested clinically. In a phase II trial, intratumoral ONYX-015 injection led to a complete or partial (<50% reduction in tumor diameter) response in 20% of cases (129). Other oncolytic viruses are under investigation. An attenuated, replication-competent, oncolytic herpes simplex virus (NV1023) has shown promise in experimental studies. NV 1023 delivery to the surgical bed after tumor resection caused viral infection of metastatic squamous cells in cervical lymph nodes and improved the rate of locoregional control and disease-free survival (130). Localization, distribution, and survival of this oncolytic virus was imaged with 18F-2′-fluoro-2′-deoxy-1-β-d-β-arabinofuranosyl-5-ethyluracil PET, taking advantage of viral thymidine kinase expression (131). One can envision similar imaging studies in the clinical environment, which may be particularly useful when the agent is to be administered intravenously rather than into the tumor site.
CONCLUSION
Concurrent chemoradiotherapy is widely used as the definitive treatment for locoregionally advanced HNSCC because it provides higher response rates than radiotherapy alone. Negative 18F-FDG PET or PET/CT findings after concurrent chemoradiotherapy have a high NPV (>95%). The PPV is lower, but few studies will be considered positive when interpreted as suggested in this review. On the basis of a patient's specific condition, neck dissection may be avoided in many cases. The role of PET with either 18F-FDG or 18F-FLT in assessing response during induction or definitive chemoradiotherapy is under investigation. Experimental therapy with EGFR and VEGF inhibitors is under study in HNSCC; several PET probes appear promising for measuring the response to these new drugs and potentially for selecting patients with suitable molecular targets for such experimental therapies. Hypoxia imaging may be helpful in designing alternate radiotherapy techniques that may overcome the radioresistance of hypoxic tumors. For most clinical purposes, however, 18F-FDG PET/CT will remain the major clinical tool for monitoring treatment in HNSCC in the near future.
Acknowledgments
We thank John Humm, for helpful discussions on radiation biology, and Richard Wong, for helpful discussions on oncolytic virus treatment for head and neck cancer.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.
- 15.↵
- 16.↵
- 17.
- 18.
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.
- 105.↵
- 106.↵
- 107.
- 108.
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- Received for publication January 27, 2009.
- Accepted for publication March 25, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 111In-Cetuximab-F(ab')2 SPECT and 18F-FDG PET for Prediction and Response Monitoring of Combined-Modality Treatment of Human Head and Neck Carcinomas in a Mouse Model
- The Value of PET Compared to MRI in Malignant Head and Neck Tumors
- Effect of Reconstruction Parameters in High-Definition PET/CT on Assessment of Lymph Node Metastases in Head and Neck Squamous Cell Carcinoma
- The role of positron emission tomography/CT imaging in head and neck cancer patients after radical chemoradiotherapy
- Usefulness of 3'-Deoxy-3'-18F-Fluorothymidine PET for Predicting Early Response to Chemoradiotherapy in Head and Neck Cancer
- Repeatability of 18F-FDG Uptake Measurements in Tumors: A Metaanalysis
- Treatment Evaluation of Metastatic Lymph Nodes after Concurrent Chemoradiotherapy in Patients with Head and Neck Squamous Cell Carcinoma
- FDG-PET as a Potential Tool for Selecting Patients with Advanced Non-Small Cell Lung Cancer Who May Be Spared Maintenance Therapy after First-Line Chemotherapy
- The physical basis and future of radiation therapy
- PET and PET/CT of the Neck Lymph Nodes Improves Risk Prediction in Patients with Squamous Cell Carcinoma of the Oral Cavity
- Assessing Tumor Response to Therapy