


Abstract
241537
Introduction: Deep inspiration breath hold (DIBH) acquisition is a straightforward approach to mitigate the respiratory motion artifacts in PET/CT imaging but challenging in upper abdomen. The study aims to explore the clinical feasibility and efficacy of a DIBH PET/CT using 18F-NOTA-LM3 on upper abdominal lesions in patients with neuroendocrine tumors (NETs).
Methods: Twenty-three patients (F/M: 8/15, age: 25-75 y) with confirmed or suspected NETs for (re)staging or treatment monitoring were prospectively enrolled. All patients underwent a free-breath (FB) whole-body PET/CT using a novel PET/CT scanner (uMI Panorama, United Imaging Healthcare) with high sensitivity and excellent time-of-flight resolution to acquire 10 min/bed for the upper abdomen and 2 min/bed for other regions. A vital signal monitoring (VSM) system was mounted to patients for respiratory gating (RG). Immediately after the routine scan, a DIBH PET/CT was performed covering the same axial range as the RG PET. Patients were asked to breathe hold for 20 s with a voice instruction. For the bed covering the upper abdomen, FB PET was reconstructed using the rebinned 2-min list mode data; RG PET was generated with 6 bins amplitude-based reconstruction using the VSM signal; a 20-s and 15-s BH PET (referred to as BH_20 and BH_15) were reconstructed from the DIBH acquired data.
Subjective analysis was performed by two nuclear medicine physicians to evaluate the respiratory motion artefacts and diagnostic confidence using a 5-point Likert scale. In the quantitative analysis, liver SUVmean, lesion SUVmax, metabolic tumor volume (MTV), and target-to-background ratio (TBR) were obtained on each PET series. Subgroup analysis was performed based on lesion location (organ-based) and MTV (L-group for large volume and S-group for small volume with a cut-off value of 1.0 cm3).
Statistical analysis was performed in the subjective analysis using Wilcoxon signed rank test. Using RG PET as a reference, paired t-test was performed to compare the quantitative metrics.
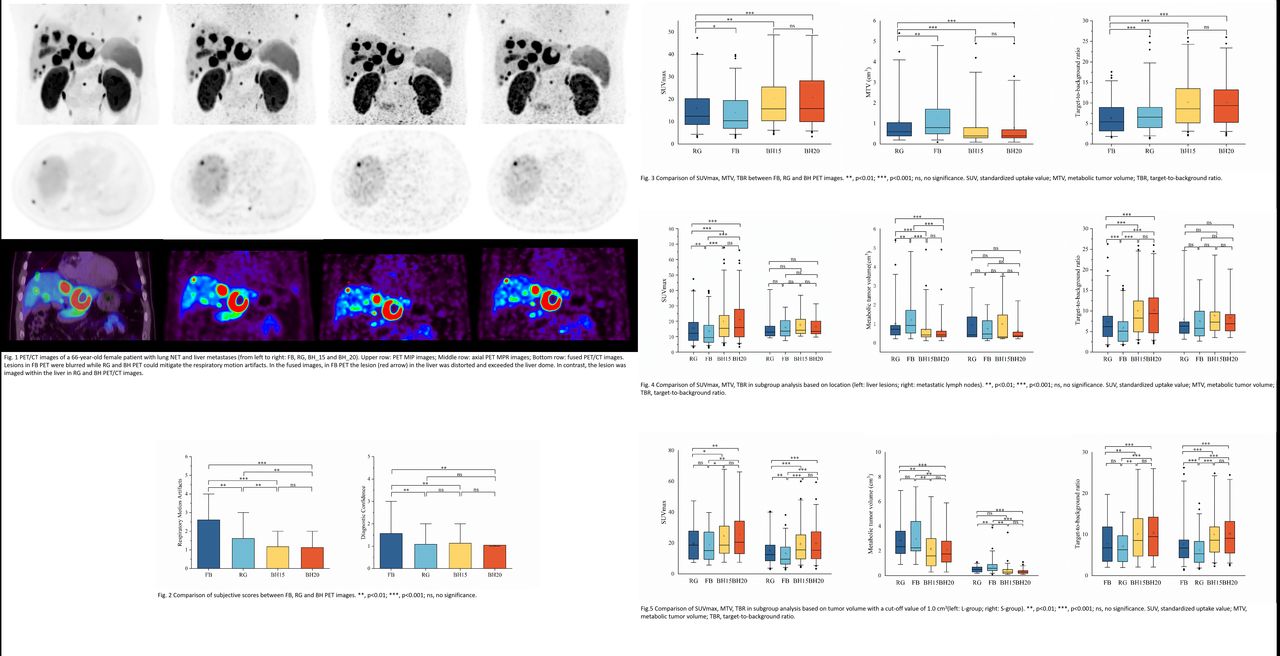
Results: In the subjective analysis, both BH PET showed significantly fewer respiratory motion artifacts than RG PET and FB PET (both p<0.01 and p<0.001, Fig. 1&2). Moreover, BH PET showed a comparable performance with RG PET regarding diagnostic confidence (both p=0.564), but significantly improve performance compared to FB PET (both p<0.05). No significant difference was observed between BH PET (Fig. 2).
In the quantitative analysis, concordance correlation coefficient of liver SUVmean between RG PET and BH PET are 0.953 and 0.956, respectively, suggesting a substantial agreement in PET quantitative accuracy in normal tissue. Both BH PET exhibited higher lesion SUVmax and TBR (n=78) than RG PET (all p<0.01, Fig. 3), and smaller MTV than RG PET (both p<0.001, Fig. 3). In the subgroup analysis, we analyzed liver lesions (n=60) and metastatic lymph nodes (MLN, n=8), and observed different significance (Fig. 4) in the three metrics. Noticeably, no significant difference in all the metrics was found in MLN. In subgroup analysis for the L-group, there was no significant difference in the three metrics between RG and BH PET (p=0.465, 0.976 and 0.203 for SUVmax, MTV and TBR, respectively, Fig. 5). However, BH PET can significantly further enhance SUVmax and TBR, and reduce MTV compared to RG and FB PET (all p<0.05). In contrast, in the S-group, RG and both BH PET significantly improved the lesion SUVmax and TBR, and reduced MTV (all p<0.01). Regarding the MTV, there was no significant difference between RG and BH_15 PET (p=0.087). Furthermore, no significant difference was observed between BH PET in any comparison in the quantitative analysis.
Conclusions: The DIBH PET/CT is effective in 18F-NOTA-LM3 imaging in detecting upper abdominal lesions as it can provide more accurate quantitative measurements. Using a novel PET/CT scanner, a 20-s even 15-s DIBH PET can provide comparable and better performance to RG PET, suggesting feasibility in the clinical routines.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.